
Expectations and Concerns about the Use of Telemedicine for Autism Spectrum Disorder: A Cross-Sectional Survey of Parents and Healthcare Professionals

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
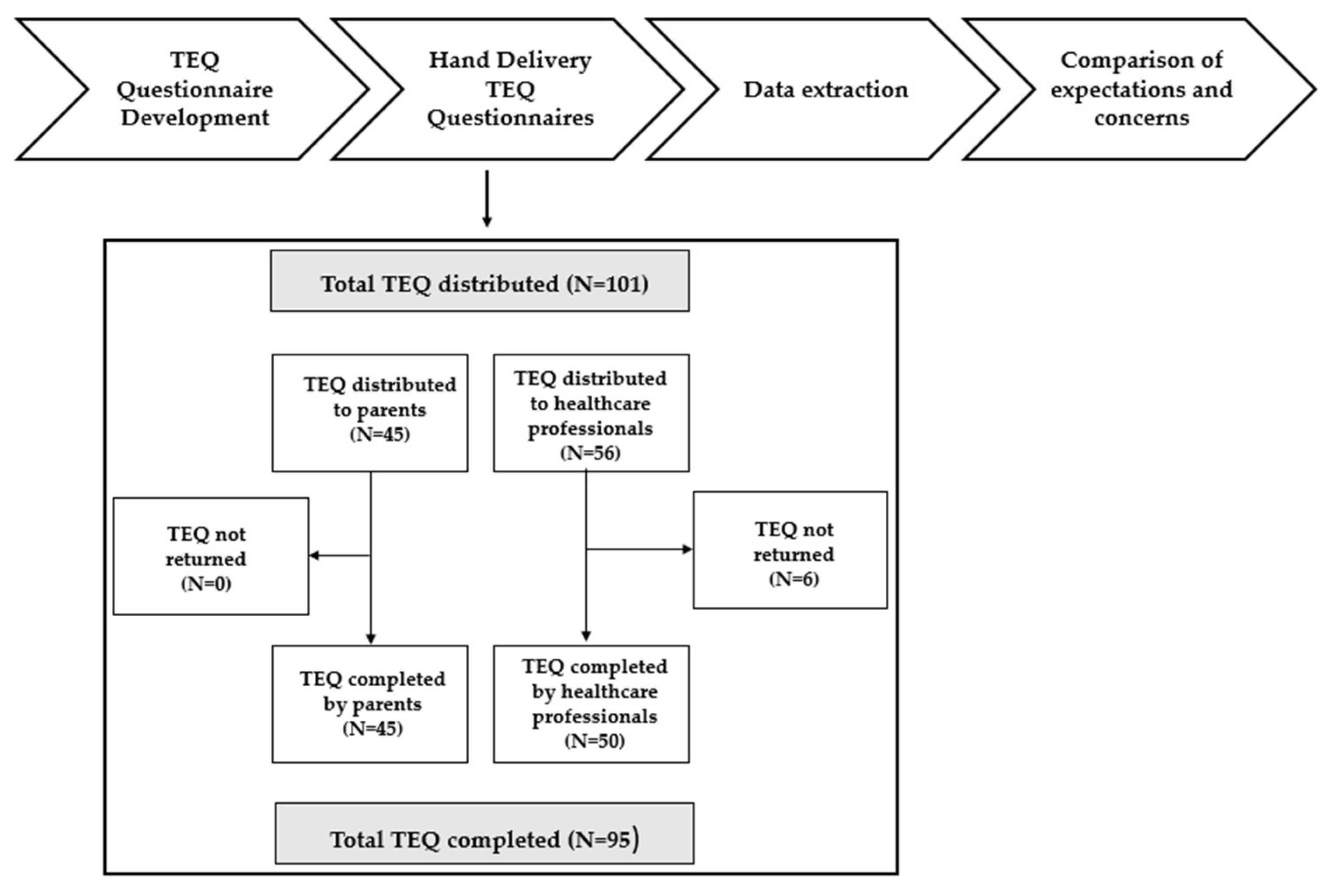
2.1. Participants
2.2. Measures
2.2.1. Socio-Demographic Information
2.2.2. Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Respondents’ Description
3.2. Expectations on the Uses and Potential Benefits of Telemedicine
3.3. Concerns about Objective and Subjective Barriers
4. Discussion
4.1. Expectations on the Uses and Potential Benefits of Telemedicine
4.2. Concerns about Objective and Subjective Barriers
4.3. Limits
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Maenner, M.J.; Shaw, K.A.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Esler, A.; Furnier, S.M.; Hallas, L.; Hall-Lande, J.; Hudson, A.; et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 sites, United States, 2018 MMWR. Surveill. Summ. 2021, 70, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Cardinal, D.N.; Griffiths, A.J.; Maupin, Z.D.; Fraumeni-McBride, J. An investigation of increased rates of autism in U.S. public schools. Psychol. Sch. 2020, 58, 124–140. [Google Scholar] [CrossRef]
- Hyman, S.L.; Levy, S.E.; Myers, S.M. Identification, evaluation, and management of children with autism spectrum disorder. Pediatrics 2020, 145, e20193447. [Google Scholar] [CrossRef]
- Bent, C.; Barbaro, J.; Dissanayake, C. Change in autism diagnoses prior to and following the introduction of DSM-5. J. Autism Dev. Disord. 2016, 47, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Styles, M.; Alsharshani, D.; Samara, M.; Alsharshani, M.; Khattab, A.; Qoronfleh, M.W.; Al-Dewik, N. Risk factors, diagnosis, prognosis, and treatment of autism. Front Biosci-Landmark 2020, 25, 1682–1717. [Google Scholar]
- Yoon, S.H.; Choi, J.; Lee, W.J.; Do, J.T. Genetic and epigenetic etiology underlying autism spectrum disorder. J. Clin. Med. 2020, 9, 966. [Google Scholar] [CrossRef]
- Howes, O.D.; Rogdaki, M.; Findon, J.; Wichers, R.H.; Charman, T.; King, B.H.; Loth, E.; McAlonan, G.; McCracken, J.T.; Parr, J.R.; et al. Autism spectrum disorder: Consensus guidelines on assessment, treatment and research from the British Association for Psychopharmacology. J. Psychopharmacol. 2017, 32, 3–29. [Google Scholar] [CrossRef]
- Murdaca, G.; Tonacci, A.; Negrini, S.; Greco, M.; Borro, M.; Puppo, F.; Gangemi, S. Emerging role of vitamin D in autoimmune diseases: An update on evidence and therapeutic implications. Autoimmun. Rev. 2019, 18, 102350. [Google Scholar] [CrossRef]
- Petruzzelli, M.G.; Marzulli, L.; Margari, F.; De Giacomo, A.; Gabellone, A.; Giannico, O.V.; Margari, L. Vitamin D deficiency in autism spectrum disorder: A cross-sectional study. Dis. Markers 2020, 2020, 9292560. [Google Scholar] [CrossRef]
- De Giacomo, A.; Gargano, C.D.; Simone, M.; Petruzzelli, M.G.; Pedaci, C.; Giambersio, D.; Margari, L.; Ruggieri, M. B and T Immunoregulation: A new insight of b regulatory lymphocytes in autism spectrum disorder. Front. Neurosci. 2021, 15, 732611. [Google Scholar] [CrossRef]
- Hughes, H.; Ko, E.M.; Rose, D.; Ashwood, P. Immune dysfunction and autoimmunity as pathological mechanisms in autism spectrum disorders. Front. Cell. Neurosci. 2018, 12, 405. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.C.; Lombardo, M.V.; Chakrabarti, B.; Baron-Cohen, S. Subgrouping the autism ‘spectrum’: Reflections on DSM-5. PLoS Biol. 2013, 11, e1001544. [Google Scholar] [CrossRef] [PubMed]
- Afif, I.Y.; Manik, A.R.; Munthe, K.; Maula, M.I.; Ammarullah, M.I.; Jamari, J.; Winarni, T.I. Physiological effect of deep pressure in reducing anxiety of children with ASD during traveling: A public transportation setting. Bioengineering 2022, 9, 157. [Google Scholar] [CrossRef] [PubMed]
- Penner, M.; Anagnostou, E.; Andoni, L.Y.; Ungar, W.J. Systematic review of clinical guidance documents for autism spectrum disorder diagnostic assessment in select regions. Autism 2017, 22, 517–527. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Rutter, M.; DLavore, P.C.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule-2 (ADOS-2), 2nd ed.; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism diagnostic interview-revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J. Autism Dev. Disord. 1994, 24, 659–685. [Google Scholar] [CrossRef] [PubMed]
- Simonoff, E.; Pickles, A.; Charman, T.; Chandler, S.; Loucas, T.; Baird, G. Psychiatric disorders in children with autism spectrum disorders: Prevalence, comorbidity, and associated factors in a population-derived sample. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 921–929. [Google Scholar] [CrossRef] [PubMed]
- CDC. Implementation of mitigation strategies for communities with local COVID-19 transmission. Centers Dis. Control Prev. 2020, 2019, 1–10. Available online: www.cdc.gov/COVID19 (accessed on 13 October 2021).
- Ellison, K.S.; Guidry, J.; Picou, P.; Adenuga, P.; Davis, T.E. Telehealth and autism prior to and in the age of COVID-19: A systematic and critical review of the last decade. Clin. Child Fam. Psychol. Rev. 2021, 24, 599–630. [Google Scholar] [CrossRef] [PubMed]
- Dahiya, A.V.; DeLucia, E.; McDonnell, C.G.; Scarpa, A. A systematic review of technological approaches for autism spectrum disorder assessment in children: Implications for the COVID-19 pandemic. Res. Dev. Disabil. 2021, 109, 103852. [Google Scholar] [CrossRef]
- Lim, T.; Tan, M.Y.; Aishworiya, R.; Kang, Y.Q. Autism spectrum disorder and COVID-19: Helping caregivers navigate the pandemic. Ann. Acad. Med. Singap. 2020, 49, 384–386. [Google Scholar] [CrossRef]
- Narzisi, A. Phase 2 and later of COVID-19 lockdown: Is it possible to perform remote diagnosis and intervention for autism spectrum disorder? An online-mediated approach. J. Clin. Med. 2020, 9, 1850. [Google Scholar] [CrossRef] [PubMed]
- Berger, N.I.; Wainer, A.L.; Kuhn, J.; Bearss, K.; Attar, S.; Carter, A.S.; Ibanez, L.V.; Ingersoll, B.R.; Neiderman, H.; Scott, S.; et al. Characterizing available tools for synchronous virtual assessment of toddlers with suspected autism spectrum disorder: A brief report. J. Autism Dev. Disord. 2021, 52, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Conti, E.; Chericoni, N.; Costanzo, V.; LaSala, R.; Mancini, A.; Prosperi, M.; Tancredi, R.; Muratori, F.; Calderoni, S.; Apicella, F. Moving toward telehealth surveillance services for toddlers at risk for autism during the COVID-19 pandemic. Front. Psychiatry 2020, 11, 565999. [Google Scholar] [CrossRef] [PubMed]
- Strehle, E.M.; Shabde, N. One hundred years of telemedicine: Does this new technology have a place in paediatrics? Arch. Dis. Child 2006, 91, 956–959. [Google Scholar] [CrossRef]
- Sood, S.; Mbarika, V.; Jugoo, S.; Dookhy, R.; Doarn, C.; Prakash, N.; Merrell, R.C. What is telemedicine? A collection of 104 peer-reviewed perspectives and theoretical underpinnings. Telemed. e-Health 2007, 13, 573–590. [Google Scholar] [CrossRef]
- WHO. A Health Telematics Policy in Support of WHO’s Health-for-All Strategy for Global Health Development: Report of the WHO Group Consultation on Health Telematics, Geneva, Switzerland, 11–16 December, 1997; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Doraiswamy, S.; Abraham, A.; Mamtani, R.; Cheema, S. Use of telehealth during the COVID-19 pandemic: Scoping review. J. Med. Internet Res. 2020, 22, e24087. [Google Scholar] [CrossRef]
- Rooks-Ellis, D.; Howorth, S.K.; Kunze, M.; Boulette, S.; Sulinski, E. Effects of a parent training using telehealth: Equity and access to early intervention for rural families. J. Child. Educ. Soc. 2020, 1, 141–166. [Google Scholar] [CrossRef]
- Alkhalifah, S.; Aldhalaan, H. Telehealth services for children with autism spectrum disorders in rural areas of the Kingdom of Saudi Arabia: Overview and recommendations. JMIR Pediatr. Parent. 2018, 1, e11402. [Google Scholar] [CrossRef]
- Antezana, L.; Scarpa, A.; Valdespino, A.; Albright, J.; Richey, J.A. rural trends in diagnosis and services for autism spectrum disorder. Front. Psychol. 2017, 8, 590. [Google Scholar] [CrossRef]
- Reese, R.M.; Jamison, T.R.; Braun, M.; Wendland, M.; Black, W.; Hadorn, M.; Nelson, E.L.; Prather, C. Brief report: Use of interactive television in identifying autism in young children: Methodology and preliminary data. J. Autism Dev. Disord. 2015, 45, 1474–1482. [Google Scholar] [CrossRef]
- Craig, J.; Patterson, V. Introduction to the practice of telemedicine. J. Telemed. Telecare 2005, 11, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Simacek, J.; Elmquist, M.; Dimian, A.F.; Reichle, J. Current trends in telehealth applications to deliver social communication interventions for young children with or at risk for autism spectrum disorder. Curr. Dev. Disord. Rep. 2020, 8, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Alfuraydan, M.; Croxall, J.; Hurt, L.; Kerr, M.; Brophy, S. Use of telehealth for facilitating the diagnostic assessment of Autism Spectrum Disorder (ASD): A scoping review. PLoS ONE 2020, 15, e0236415. [Google Scholar] [CrossRef] [PubMed]
- Reese, R.M.; Jamison, R.; Wendland, M.; Fleming, K.; Braun, M.J.; Schuttler, J.O.; Turek, J. Evaluating interactive videoconferencing for assessing symptoms of autism. Telemed. e-Health 2013, 19, 671–677. [Google Scholar] [CrossRef]
- Juárez, A.P.; Weitlauf, A.S.; Nicholson, A.; Pasternak, A.; Broderick, N.; Hine, J.; Stainbrook, J.A.; Warren, Z. Early identification of ASD through telemedicine: Potential value for underserved populations. J. Autism Dev. Disord. 2018, 48, 2601–2610. [Google Scholar] [CrossRef]
- Wagner, L.; Corona, L.L.; Weitlauf, A.S.; Marsh, K.L.; Berman, A.F.; Broderick, N.A.; Francis, S.; Hine, J.; Nicholson, A.; Stone, C.; et al. Use of the TELE-ASD-PEDS for autism evaluations in response to COVID-19: Preliminary Outcomes and clinician acceptability. J. Autism Dev. Disord. 2020, 51, 3063–3072. [Google Scholar] [CrossRef]
- Smith, C.J.; Rozga, A.; Matthews, N.; Oberleitner, R.; Nazneen, N.; Abowd, G. Investigating the accuracy of a novel telehealth diagnostic approach for autism spectrum disorder. Psychol. Assess. 2017, 29, 245–252. [Google Scholar] [CrossRef]
- Nazneen, N.; Rozga, A.; Smith, C.J.; Oberleitner, R.; Abowd, G.D.; Arriaga, R.I. A novel system for supporting autism diagnosis using home videos: Iterative development and evaluation of system design. JMIR mHealth uHealth 2015, 3, e68. [Google Scholar] [CrossRef]
- Fusaro, V.A.; Daniels, J.; Duda, M.; DeLuca, T.F.; D’Angelo, O.; Tamburello, J.; Maniscalco, J.; Wall, D.P. The potential of accelerating early detection of autism through content analysis of youtube videos. PLoS ONE 2014, 9, e93533. [Google Scholar] [CrossRef]
- Johnsson, G.; Kerslake, R.; Crook, S. Delivering allied health services to regional and remote participants on the autism spectrum via video-conferencing technology: Lessons learned. Rural Remote Health 2019, 19, 5358. [Google Scholar] [CrossRef]
- Sutherland, R.; Trembath, D.; Roberts, J. Telehealth and autism: A systematic search and review of the literature. Int. J. Speech-Language Pathol. 2018, 20, 324–336. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.S.; Messinger, D.S.; Stone, W.L.; Celimli, S.; Nahmias, A.S.; Yoder, P. Randomized controlled trial of Hanen’s ‘More Than Words’ in toddlers with early autism symptoms. J. Child Psychol. Psychiatry 2011, 52, 741–752. [Google Scholar] [CrossRef] [PubMed]
- Parsons, D.; Cordier, R.; Vaz, S.; Lee, H.C. Parent-mediated intervention training delivered remotely for children with autism spectrum disorder living outside of urban areas: Systematic review. J. Med. Internet Res. 2017, 19, e198. [Google Scholar] [CrossRef] [PubMed]
- Baer, D.M.; Wolf, M.M.; Risley, T.R. Some current dimensions of applied behavior analysis1. J. Appl. Behav. Anal. 1968, 1, 91–97. [Google Scholar] [CrossRef]
- Rogers, S.J.; Dawson, G. The Early Start Denver Model for Young Children with Autism: Promoting Language, Learning, and Engagement; Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- De Nocker, Y.L.; Toolan, C.K. Using telehealth to provide interventions for children with ASD: A systematic review. Rev. J. Autism Dev. Disord. 2021, 1–31. [Google Scholar] [CrossRef]
- Rogers, S.J.; Estes, A.; Lord, C.; Vismara, L.; Winter, J.; Fitzpatrick, A.; Guo, M.; Dawson, G. Effects of a brief early start Denver model (ESDM)–Based parent intervention on toddlers at risk for autism spectrum disorders: A randomized controlled trial. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 1052–1065. [Google Scholar] [CrossRef]
- Vismara, L.A.; Young, G.S.; Rogers, S.J. Telehealth for expanding the reach of early autism training to parents. Autism Res. Treat. 2012, 2012, 121878. [Google Scholar] [CrossRef]
- Bearss, K.; Burrell, T.L.; Challa, S.A.; Postorino, V.; Gillespie, S.E.; Crooks, C.; Scahill, L. Feasibility of parent training via telehealth for children with autism spectrum disorder and disruptive behavior: A demonstration pilot. J. Autism Dev. Disord. 2017, 48, 1020–1030. [Google Scholar] [CrossRef]
- Little, L.M.; Wallisch, A.; Pope, E.; Dunn, W. Acceptability and cost comparison of a telehealth intervention for families of children with autism. Infants Young Child. 2018, 31, 275–286. [Google Scholar] [CrossRef]
- Vismara, L.A.; McCormick, C.E.B.; Wagner, A.L.; Monlux, K.; Nadhan, A.; Young, G.S. Telehealth parent training in the early start Denver model: Results from a randomized controlled study. Focus Autism Other Dev. Disabil. 2016, 33, 67–79. [Google Scholar] [CrossRef]
- Solomon, D.; Soares, N. Telehealth approaches to care coordination in autism spectrum disorder. In Interprofessional Care Coordination for Pediatric Autism Spectrum Disorder; Springer: Cham, Switzerland, 2020; pp. 289–306. [Google Scholar] [CrossRef]
- Iacono, T.; Dissanayake, C.; Trembath, D.; Hudry, K.; Erickson, S.; Spong, J. Family and practitioner perspectives on telehealth for services to young children with autism. Stud. Health Technol. Inform. 2016, 231, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Corona, L.L.; Stainbrook, J.A.; Simcoe, K.; Wagner, L.; Fowler, B.; Weitlauf, A.S.; Juárez, A.P.; Warren, Z. Utilization of telemedicine to support caregivers of young children with ASD and their Part C service providers: A comparison of intervention outcomes across three models of service delivery. J. Neurodev. Disord. 2021, 13, 38. [Google Scholar] [CrossRef] [PubMed]
- Camden, C.; Silva, M. Pediatric teleheath: Opportunities created by the COVID-19 and suggestions to sustain its use to support families of children with disabilities. Phys. Occup. Ther. Pediatr. 2020, 41, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Corona, L.L.; Weitlauf, A.S.; Hine, J.; Berman, A.; Miceli, A.; Nicholson, A.; Stone, C.; Broderick, N.; Francis, S.; Juárez, A.P.; et al. Parent perceptions of caregiver-mediated telemedicine tools for assessing autism risk in toddlers. J. Autism Dev. Disord. 2020, 51, 476–486. [Google Scholar] [CrossRef]
- Salomone, E.; Arduino, G.M. Parental attitudes to a telehealth parent coaching intervention for autism spectrum disorder. J. Telemed. Telecare 2016, 23, 416–420. [Google Scholar] [CrossRef]
- Hollingshead, A.H. Four-Factor Index of Social Status; Yale University Department of Sociology: New Haven, CA, USA, 1975. [Google Scholar]
- Rai, J.J.; Acharya, R.V. Evaluation of patient and doctor perception toward the use of telemedicine in Apollo Tele Health Services, India. J. Fam. Med. Prim. Care 2016, 5, 798–803. [Google Scholar] [CrossRef]
- Pickard, K.E.; Wainer, A.L.; Bailey, K.M.; Ingersoll, B.R. A mixed-method evaluation of the feasibility and acceptability of a telehealth-based parent-mediated intervention for children with autism spectrum disorder. Autism 2016, 20, 845–855. [Google Scholar] [CrossRef]
- Albarrak, A.I.; Mohammed, R.; Almarshoud, N.; Almujalli, L.; Aljaeed, R.; Altuwaijiri, S.; Albohairy, T. Assessment of physician’s knowledge, perception and willingness of telemedicine in Riyadh region, Saudi Arabia. J. Infect. Public Health 2019, 14, 97–102. [Google Scholar] [CrossRef]
- Gibbs, V.; Cai, R.Y.; Aldridge, F.; Wong, M. Autism assessment via telehealth during the COVID 19 pandemic: Experiences and perspectives of autistic adults, parents/carers and clinicians. Res. Autism Spectr. Disord. 2021, 88, 101859. [Google Scholar] [CrossRef]
- Healy, S.; Marchand, G.; Williams, E. “I’m not in this alone” the perspective of parents mediating a physical activity intervention for their children with autism spectrum disorder. Res. Dev. Disabil. 2018, 83, 160–167. [Google Scholar] [CrossRef]
- Hines, M.; Lincoln, M.; Ramsden, R.; Martinovich, J.; Fairweather, C. Speech pathologists’ perspectives on transitioning to telepractice: What factors promote acceptance? J. Telemed. Telecare 2015, 21, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Cowan, K.E.; McKean, A.J.; Gentry, M.T.; Hilty, D.M. Barriers to use of telepsychiatry: Clinicians as gatekeepers. Mayo Clin. Proc. 2019, 94, 2510–2523. [Google Scholar] [CrossRef] [PubMed]
- Dunkley, C.; Pattie, L.; Wilson, L.; McAllister, L. A comparison of rural speech-language pathologists’ and residents’ access to and attitudes towards the use of technology for speech-language pathology service delivery. Int. J. Speech-Language Pathol. 2010, 12, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Adams, L.; Adamo, N.; Hollocks, M.J.; Valmaggia, L.; Brewster, A.; Watson, J.; Krisson, M.; Simonoff, E. Examining clinicians’ concerns delivering telemental health interventions directly to autistic individuals during COVID-19. Res. Autism Spectr. Disord. 2022, 94, 101956. [Google Scholar] [CrossRef]
- Schreibman, L.; Dawson, G.; Stahmer, A.C.; Landa, R.; Rogers, S.J.; McGee, G.G.; Kasari, C.; Ingersoll, B.; Kaiser, A.P.; Bruinsma, Y.; et al. Naturalistic developmental behavioral interventions: Empirically validated treatments for autism spectrum disorder. J. Autism Dev. Disord. 2015, 45, 2411–2428. [Google Scholar] [CrossRef]
- Pickles, A.; Le Couteur, A.; Leadbitter, K.; Salomone, E.; Cole-Fletcher, R.; Tobin, H.; Gammer, I.; Lowry, J.; Vamvakas, G.; Byford, S.; et al. Parent-mediated social communication therapy for young children with autism (PACT): Long-term follow-up of a randomised controlled trial. Lancet 2016, 388, 2501–2509. [Google Scholar] [CrossRef]
- Nicolaidis, C.; Raymaker, D.M.; Ashkenazy, E.; McDonald, K.; Dern, S.; Baggs, W.A.E.; Kapp, S.; Weiner, M.; Boisclair, W.C. Respect the way I need to communicate with you: Healthcare experiences of adults on the autism spectrum. Autism 2015, 19, 824–831. [Google Scholar] [CrossRef]
- Saqr, Y.; Braun, E.; Porter, K.; Barnette, D.; Hanks, C. Addressing medical needs of adolescents and adults with autism spectrum disorders in a primary care setting. Autism 2017, 22, 51–61. [Google Scholar] [CrossRef]
- Stavropoulos, K.K.-M.; Bolourian, Y.; Blacher, J. A scoping review of telehealth diagnosis of autism spectrum disorder. PLoS ONE 2022, 17, e0263062. [Google Scholar] [CrossRef]
- Grady, B.; Myers, K.M.; Nelson, E.-L.; Belz, N.; Bennett, L.; Carnahan, L.; Decker, V.B.; Holden, D.; Perry, G.; American Telemedicine Association Telemental Health Standards and Guidelines Working Group; et al. Evidence-based practice for telemental health. Telemed. e-Health 2011, 17, 131–148. [Google Scholar] [CrossRef]
- Dow, D.; Holbrook, A.; Toolan, C.; McDonald, N.; Sterrett, K.; Rosen, N.; Kim, S.H.; Lord, C. The Brief Observation of Symptoms of Autism (BOSA): Development of a new adapted assessment measure for remote telehealth administration through COVID-19 and beyond. J. Autism Dev. Disord. 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Boisvert, M.; Hall, N. The use of telehealth in early autism training for parents: A scoping review. Smart Homecare Technol. TeleHealth 2014, 2, 19–27. [Google Scholar] [CrossRef]
- Meadan, H.; Daczewitz, M.E. Internet-based intervention training for parents of young children with disabilities: A promising service-delivery model. Early Child Dev. Care 2014, 185, 155–169. [Google Scholar] [CrossRef]
- Thongseiratch, T.; Leijten, P.; Melendez-Torres, G.J. Online parent programs for children’s behavioral problems: A meta-analytic review. Eur. Child Adolesc. Psychiatry 2020, 29, 1555–1568. [Google Scholar] [CrossRef] [PubMed]
- Cleffi, C.; Su, W.-C.; Srinivasan, S.; Bhat, A. Using telehealth to conduct family-centered, movement intervention research in children with autism spectrum disorder during the COVID-19 pandemic. Pediatr. Phys. Ther. 2022, 34, 246–251. [Google Scholar] [CrossRef]
- Zwaigenbaum, L.; Bishop, S.; Stone, W.L.; Ibanez, L.; Halladay, A.; Goldman, S.; Kelly, A.; Klaiman, C.; Lai, M.; Miller, M.; et al. Rethinking autism spectrum disorder assessment for children during COVID-19 and beyond. Autism Res. 2021, 14, 2251–2259. [Google Scholar] [CrossRef]
- Johnsson, G.; Bulkeley, K. Practitioner and service user perspectives on the rapid shift to teletherapy for individuals on the autism spectrum as a result of COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 11812. [Google Scholar] [CrossRef]
- Boisvert, M.; Hall, N.; Andrianopoulos, M.; Chaclas, J. The multi-faceted implementation of telepractice to service individuals with autism. Int. J. Telerehabilitation 2012, 4, 11–24. [Google Scholar] [CrossRef]
- Nohelty, K.; Bradford, C.B.; Hirschfeld, L.; Miyake, C.; Novack, M.N. Effectiveness of telehealth direct therapy for individuals with autism spectrum disorder. Behav. Anal. Pract. 2021, 1–16. [Google Scholar] [CrossRef]
- Mazurek, M.O.; Shattuck, P.T.; Wagner, M.; Cooper, B.P. Prevalence and correlates of screen-based mediause among youths with autism spectrum disorders. J. Autism Dev. Disord. 2012, 42, 1757–1767. [Google Scholar] [CrossRef]
- Orsmond, G.I.; Kuo, H.Y. The daily lives of adolescents with an autism spectrum disorder: Discretionary time use andactivity partners. Autism 2011, 15, 579–599. [Google Scholar] [CrossRef] [PubMed]
- Sehlin, H.; Ahlström, B.H.; Andersson, G.; Wentz, E. Experiences of an internet-based support and coaching model for adolescents and young adults with ADHD and autism spectrum disorder—A qualitative study. BMC Psychiatry 2018, 18, 15. [Google Scholar] [CrossRef] [PubMed]
- Hamad, C.D.; Serna, R.W.; Morrison, L.; Fleming, R. Extending the reach of early intervention training for practitioners: A preliminary investigation of an online curriculum for teaching behavioral intervention knowledge in autism to families and service providers. Infants Young- Child. 2010, 23, 195–208. [Google Scholar] [CrossRef] [PubMed]
- Heitzman-Powell, L.S.; Buzhardt, J.; Rusinko, L.C.; Miller, T.M. Formative evaluation of an ABA outreach training program for parents of children with autism in remote areas. Focus Autism Other Dev. Disabil. 2013, 29, 23–38. [Google Scholar] [CrossRef]
- Ingersoll, B.; Berger, N.I. Parent engagement with a telehealth-based parent-mediated intervention program for children with autism spectrum disorders: Predictors of program use and parent outcomes. J. Med. Internet Res. 2015, 17, e227. [Google Scholar] [CrossRef]
- Vismara, L.A.; McCormick, C.; Young, G.S.; Nadhan, A.; Monlux, K. Preliminary findings of a telehealth approach to parent training in autism. J. Autism Dev. Disord. 2013, 43, 2953–2969. [Google Scholar] [CrossRef]
- Wacker, D.P.; Lee, J.F.; Dalmau, Y.C.P.; Kopelman, T.G.; Lindgren, S.D.; Kuhle, J.; Pelzel, K.E.; Dyson, S.; Schieltz, K.M.; Waldron, D.B. Conducting functional communication training via telehealth to reduce the problem behavior of young children with autism. J. Dev. Phys. Disabil. 2012, 25, 35–48. [Google Scholar] [CrossRef]
- Lindgren, S.; Wacker, D.; Suess, A.; Schieltz, K.; Pelzel, K.; Kopelman, T.; Lee, J.; Romani, P.; Waldron, D. Telehealth and autism: Treating challenging behavior at lower cost. Pediatrics 2016, 137, S167–S175. [Google Scholar] [CrossRef]
- Suess, A.N.; Wacker, D.P.; Schwartz, J.E.; Lustig, N.; Detrick, J. Preliminary evidence on the use of telehealth in an outpatient behavior clinic. J. Appl. Behav. Anal. 2016, 49, 686–692. [Google Scholar] [CrossRef]
- Baker-Ericzén, M.J.; Brookman-Frazee, L.; Stahmer, A. Stress levels and adaptability in parents of toddlers with and without autism spectrum disorders. Res. Pract. Pers. Sev. Disabil. 2005, 30, 194–204. [Google Scholar] [CrossRef]
- Rivard, M.; Terroux, A.; Parent-Boursier, C.; Mercier, C. Determinants of stress in parents of children with autism spectrum disorders. J. Autism Dev. Disord. 2014, 44, 1609–1620. [Google Scholar] [CrossRef] [PubMed]
- Dąbrowska-Zimakowska, A.; Pisula, E. Parenting stress and coping styles in mothers and fathers of pre-school children with autism and Down syndrome. J. Intellect. Disabil. Res. 2010, 54, 266–280. [Google Scholar] [CrossRef]
- Jones, L.; Totsika, V.; Hastings, R.P.; Petalas, M.A. Gender differences when parenting children with autism spectrum disorders: A multilevel modeling approach. J. Autism Dev. Disord. 2013, 43, 2090–2098. [Google Scholar] [CrossRef]
- Herring, S.; Gray, K.; Taffe, J.; Tonge, B.; Sweeney, D.; Einfeld, S. Behaviour and emotional problems in toddlers with pervasive developmental disorders and developmental delay: Associations with parental mental health and family functioning. J. Intellect. Disabil. Res. 2006, 50, 874–882. [Google Scholar] [CrossRef]
- Tehee, E.; Honan, R.; Hevey, D. Factors contributing to stress in parents of individuals with autistic spectrum disorders. J. Appl. Res. Intellect. Disabil. 2009, 22, 34–42. [Google Scholar] [CrossRef]
- Zhai, Y. A call for addressing barriers to telemedicine: Health disparities during the COVID-19 pandemic. Psychother Psychosom. 2021, 90, 64–66. [Google Scholar] [CrossRef] [PubMed]
- Harris, L.; Gilmore, D.; Hanks, C.; Coury, D.; Moffatt-Bruce, S.; Garvin, J.H.; Hand, B.N. It was surprisingly equivalent to the appointment I had in person: Advantages and disadvantages of synchronous telehealth for delivering primary care for autistic adults. Autism 2021. [Google Scholar] [CrossRef]
- Chedid, R.J.; Dew, A.; Veitch, C. Barriers to the use of Information and communication technology by occupational therapists working in a rural area of New South Wales, Australia. Aust. Occup. Ther. J. 2012, 60, 197–205. [Google Scholar] [CrossRef]
- Wootton, A.R.; McCuistian, C.; Packard, D.A.L.; Gruber, V.A.; Saberi, P. Overcoming technological challenges: Lessons learned from a telehealth counseling study. Telemed. e-Health 2020, 26, 1278–1283. [Google Scholar] [CrossRef]
- Lee, J.F.; Schieltz, K.M.; Suess, A.N.; Wacker, D.P.; Romani, P.W.; Lindgren, S.D.; Kopelman, T.G.; Dalmau, Y.C.P. Guidelines for developing telehealth services and troubleshooting problems with telehealth technology when coaching parents to conduct functional analyses and functional communication training in their homes. Behav. Anal. Pract. 2014, 8, 190–200. [Google Scholar] [CrossRef]
- Bauerly, B.C.; McCord, R.F.; Hulkower, R.; Pepin, D. Broadband access as a public health issue: The role of law in expanding broadband access and connecting underserved communities for better health outcomes. J. Law Med. Ethics 2019, 47, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Rains, S.A. Health at high speed: Broadband internet access, health communication, and the digital divide. Commun. Res. 2008, 35, 283–297. [Google Scholar] [CrossRef]
- Stainbrook, J.A.; Weitlauf, A.S.; Juárez, A.P.; Taylor, J.L.; Hine, J.; Broderick, N.; Nicholson, A.; Warren, Z. Measuring the service system impact of a novel telediagnostic service program for young children with autism spectrum disorder. Autism 2018, 23, 1051–1056. [Google Scholar] [CrossRef]
- Zolyomi, A.; Begel, A.; Waldern, J.F.; Tang, J.; Barnett, M.; Cutrell, E.; McDuff, D.; Andrist, S.; Morris, M.R. Managing stress: The needs of autistic adults in video calling. Proc. ACM Human-Computer Interact. 2019, 3, 1–29. [Google Scholar] [CrossRef]
- Nazneen, N.; Matthews, N.; Smith, C.J.; Rozga, A.; Abowd, G.D.; Oberleitner, R.; Reischl, U.; Arriaga, R.I. Use of a novel imaging technology for remote autism diagnosis: A reflection on experience of stakeholders. In Proceedings of the 6th International Conference on Applied Human Factors and Ergonomics (AHFE 2015) and the Affiliated Conferences, Las Vegas, NV, USA, 26–30 July 2015; Volume 3, pp. 293–300. [Google Scholar] [CrossRef]
- Licoppe, C.; Relieu, M. Presentatio. Réseaux 2007, 5, 9–22. Available online: https://www.cairn-int.info/journal-reseaux-2007-5-page-9.htm (accessed on 8 April 2022). [CrossRef]
- Doyen, C.; Kaye, K. COVID-19: Pratique et éthique de l’évaluation par vidéoconsultation des enfants avec trouble du spectre de l’autisme. Ethique Sante 2021, 18, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Zwaigenbaum, L.; Bryson, S.E.; Lord, C.; Rogers, S.J.; Carter, A.S.; Carver, L.J.; Chawarska, K.; Constantino, J.N.; Dawson, G.; Dobkins, K.R.; et al. Clinical assessment and management of toddlers with suspected autism spectrum disorder: Insights from studies of high-risk infants. Pediatrics 2009, 123, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, W.; Wallis, K.; Bennett, A.; Brooks, E.; Dudley, J.; Gerdes, M.; Pandey, J.; Levy, S.E.; Schultz, R.T.; Miller, J.S. Accuracy of autism screening in a large pediatric Network. Pediatrics 2019, 144, e20183963. [Google Scholar] [CrossRef]
- Hyman, S.L.; Johnson, J.K. Autism and pediatric practice: Toward a medical home. J. Autism Dev. Disord. 2012, 42, 1156–1164. [Google Scholar] [CrossRef]


{kind=link}
| Healthcare Professionals (n = 50) | |
| Male, n (%) | 3 (6%) |
| Race, n (%) | |
| White | 50 (100%) |
| Black | 0 (0%) |
| Others | 0 (0%) |
| Type of healthcare professionals | |
| Child neuropsychiatrist | 41 (82%) |
| Psychologists | 6 (12%) |
| Speech therapists | 2 (4%) |
| Professional educators | 1 (2%) |
| Years of professional experience, n (%) | |
| 1–5 | 27 (54%) |
| 6–10 | 12 (24%) |
| 11–20 | 7 (14%) |
| >20 | 4 (8%) |
| Parents (n = 45) | |
| Male, n (%) | 13 (29%) |
| Marital status, n (%) | |
| Married | 42 (94%) |
| Single | 0 (0%) |
| Divorced | 1 (2%) |
| Separeted | 2 (4%) |
| Race, n (%) | |
| White | 45 (100%) |
| Black | 0 (0%) |
| Others | 0 (0%) |
| ASD Children (n = 45) | |
| Age, years; n (%) | |
| <5 | 16 (36%) |
| 6–10 | 20 (44%) |
| 11–15 | 5 (11%) |
| 16–18 | 4 (9%) |
| Male, n (%) | 37 (82%) |
| Race, n (%) | |
| White | 45 (100%) |
| Black | 0 (0%) |
| Others | 0 (0%) |
| Severity level of ASD, n (%) | |
| 1 | 32(71%) |
| 2 | 7 (16%) |
| 3 | 6 (13%) |
| Pharmacological interventions, n (%) | |
| None | 35 (78%) |
| Antipsychotics | 7 (15%) |
| Antidepressants | 1 (2%) |
| Antiepileptics | 3 (7%) |
| Non-pharmacological interventions, n (%) | |
| None | 11 (24%) |
| Psychomotor therapy | 9 (20%) |
| Speech therapy | 11 (25%) |
| Cognitive–behavioural therapy | 17 (38%) |
| Psychotherapy | 4 (9%) |
| Statement | Parents (n = 45) | HP (n = 50) | ||||
|---|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | p-Value | ||
| USES AND WILLINGNESS |
| 2.98 (0.94) | 3 (2–4) * | 3.4 (0.76) | 3 (3–4) | 0.0223 |
| 3.09 (0.97) | 3 (2–4) | 3.32 (0.87) | 3 (3–4) | 0.2104 | |
| 1.93 (0.96) | 2 (1–3) | 2.26 (0.90) | 2 (2–3) | 0.0598 | |
| 2.11 (1.21) | 2 (1–3) * | 2.62 (0.83) | 3 (2–3) | 0.0061 | |
| 2.13 (1.10) | 2 (1–3) * | 2.84 (0.93) | 3 (2–4) | <0.0001 | |
| 2.98 (1.18) | 3 (2–4) | 2.98 (1.33) | 3 (2–4) | 0.9509 | |
| 3.09 (1.08) | 3 (2–4) | 2.36 (1.17) | 2 (1–3) * | 0.0026 | |
| 1.69 (1.18) | 1 (1–2) | 1.82 (1.22) | 1 (1–2) | 0.4588 | |
| Total a–h | 20 (7.41) | 19 (14–25) | 21.6 (6.21) | 22 (17–26) | 0.1445 | |
| POTENTIAL BENEFITS |
| 2.31 (1.26) | 2 (1–3) * | 2.82 (0.80) | 3 (2–3) | 0.0147 |
| 3.22 (1.22) | 3 (3–4) | 3.52 (0.76) | 4 (3–4) | 0.4219 | |
| 2.02 (1.25) | 2 (1–3) | 2.06 (0.79) | 2 (2–2) | 0.2262 | |
| 1.91 (1.18) | 1 (1–2) | 1.78 (0.76) | 2 (1–2) | 0.8223 | |
| 2.04 (1.22) | 2 (1–3) * | 2.62 (0.88) | 3 (2–3) | 0.0034 | |
| 1.93 (1.19) | 2 (1–2) * | 2.42 (0.90) | 2 (2–3) | 0.0034 | |
| 1.89 (1.13) | 2 (1–2) * | 2.16 (0.77) | 2 (2–3) | 0.0243 | |
| 1.89 (1.04) | 2 (1–3) | 2.16 (0.82) | 2 (2–3) | 0.0726 | |
| Total i–p | 17.22 (8.23) | 16 (11–23) * | 19.54 (4.63) | 20 (17–22) | 0.0207 | |
| Parents’s Data (n = 45) | Total a–h | Total a–e | Total i–p | ||||||
| Mean (sd) | Median (IQR) | p | Mean (sd) | Median (IQR) | p | Mean (sd) | Median (IQR) | p | |
| Respondent | 0.4066 | 0.3712 | 0.1913 | ||||||
| Mother | 19.44 (7.28) | 18.0 (9.5) | 11.91 (4.68) | 11.0 (6.3) | 16.44 (8.32) | 14.5 (9.5) | |||
| Father | 20.33 (6.55) | 20.0 (11.0) | 12.50 (4.13) | 12.0 (8.0) | 18.67 (7.40) | 19.0 (14.0) | |||
| Mother’s education level | 0.0432 | 0.0607 | 0.0531 | ||||||
| Primary school | 0 | 0 | 0 | 0 | 0 | 0 | |||
| Middle school | 24.38 (7.70) | 23.5 (10.0) | 15 (4.92) | 14.0 (6.0) | 23.00 (8.90) | 23.0 (12.8) | |||
| High school | 19.76 (7.34) | 18.0 (11.0) | 12.05 (4.56) | 11.0 (8.0) | 16.95 (8.36) | 16.0 (10.0) | |||
| Bachelor’s degree | 28.50 (5.50) | 28.5 (5.5) | 17.00 (3.00) | 17.0 (3.0) | 23.00 (2.00) | 23.0 (2.0) | |||
| Master’s degree/postgraduate course/PhD | 16.64 (4.59) | 16.0 (7.8) | 10.29 (3.39) | 10.0 (5.0) | 13.50 (4.94) | 11.0 (5.8) | |||
| Father’s education level | 0.1079 | 0.1347 | 0.0838 | ||||||
| Primary school | 24.00 (5.00) | 24.0 (5.0) | 15.00 (2.00) | 15.0 (2.0) | 20.00 (5.00) | 20.0 (5.0) | |||
| Middle school | 23.11(7.49) | 20.0 (10.0) | 14.11 (4.75) | 12.0 (6.0) | 20.44(9.50) | 17.0 (14.0) | |||
| High school | 21.00 (7.60) | 21.0 (12.0) | 12.88 (4.92) | 12.0 (8.0) | 19.06 (8.18) | 19.0 (14.0) | |||
| Bachelor’s degree | 0 | 0 | 0 | 0 | 0 | 0 | |||
| Master’s degree/postgraduate course/PhD | 16.88 (5.88) | 16.0 (8.0) | 10.29 (3.67) | 9.0 (5.0) | 13.35 (5.73) | 11.0 (7.0) | |||
| Family SES | 0.4510 | 0.4814 | 0.5982 | ||||||
| Low | 21.40 (5.54) | 19.0 (11.0) | 13.20 (3.37) | 13.0 (7.0) | 17.80 (4.83) | 17.0 (6.0) | |||
| Medium–low | 20.22 (5.75) | 20.0 (9.0) | 12.33 (3.86) | 12.0 (4.0) | 18.11 (7.89) | 18.0 (17.0) | |||
| Medium | 21.70 (7.75) | 21.0 (12.25) | 13.00 (4.45) | 13.0 (7.0) | 18.90 (7.67) | 18.5 (13.3) | |||
| Medium– high | 20.46 (9.01) | 17.0 (7.0) | 12.77 (5.77) | 12.0 (6.0) | 17.46 (10.20) | 13.0 (10.0) | |||
| High | 16.00 (4.21) | 14.5 (7.3) | 9.75 (3.27) | 8.5 (4.3) | 13.38 (5.07) | 11.0 (6.5) | |||
| ASD children’s data (n = 45) | Total a–h | Total a–e | Total i–p | ||||||
| Median (IQR) | p | Median (IQR) | p | Median (IQR) | p | ||||
| Age | 0.0711 | 0.0688 | 0.2219 | ||||||
| ≤6 year | 18.38 (6.88) | 16.0 (7.8) | 11.04 (4.15) | 10.5 (5.0) | 15.63 (7.04) | 12.0 (9.3) | |||
| >6 year | 21.86 (7.39) | 21.0 (10.0) | 13.62 (4.80) | 13.0 (6.0) | 19.05 (8.89) | 17.0 (10.0) | |||
| Gender | 0.4295 | 0.3783 | 0.3329 | ||||||
| Female | 21.75 (7.61) | 20.0 (3.0) | 13.75 (5.02) | 12.5 (3.8) | 19.88 (8.65) | 18.5 (5.0) | |||
| Male | 19.62 (7.21) | 17.0 (12.0) | 11.92 (4.49) | 11.0 (8.0) | 16.65 (7.91) | 14.0 (12.0) | |||
| Pharmacological therapy | 0.3656 | 0.3721 | 0.1623 | ||||||
| No | 19.81 (7.31) | 18.0 (10.0) | 11.97 (4.54) | 11.0 (7.0) | 16.59 (7.77) | 15.0 (10.0) | |||
| Yes | 21.90 (7.80) | 20.0 (10.0) | 13.60 (5.28) | 12.5 (7.0) | 20.70 (9.08) | 18.5 (11.8) | |||
| Severity level of ASD | 0.0261 | 0.0377 | 0.0327 | ||||||
| 1 | 18.1 (5.1) | 17.5 (7.5) | 11.21 (3.40) | 11.0 (5.5) | 15.36 (6.05) | 13.0 (8.3) | |||
| 2–3 | 24.4 (8.3) | 26.0 (12.0) | 14.69 (5.25) | 15.0 (10.0) | 21.54 (8.67) | 21.0 (10.0) | |||
| Healthcare professionals’ data | Total a–h | Total a–e | Total i–p | ||||||
| Median (IQR) | p | Median (IQR) | p | Median (IQR) | p | ||||
| Child neuropsychiatrist | 0.0193 | 0.0079 | 0.0510 | ||||||
| Not | 26.11 (5.63) | 26.0 (3.0) | 16.89 (2.88) | 17.0 (3.0) | 21.44 (4.78) | 22.0 (3.0) | |||
| Yes | 20.61 (5.81) | 19.0 (9.0) | 13.90 (3.06) | 14.0 (4.0) | 19.12 (4.49) | 19.0 (5.0) | |||
| Gender | 0.5529 | 0.5087 | 0.2958 | ||||||
| Female | 21.74 (6.19) | 22.0 (8.5) | 22.21 (8.7) | 16.0 (5.0) | 19.40 (4.66) | 19.0 (5.0) | |||
| Male | 19.33 (4.99) | 18.0 (6.0) | 18.00 (3.74) | 14.0 (3.0) | 21.67 (2.05) | 22.0 (2.5) | |||
| More than 5 years of professional experience | 0.0023 | 0.0018 | 0.0663 | ||||||
| Not | 19.04 (4.99) | 18.0 (6.5) | 16.26 (3.35) | 13.0 (4.0) | 18.33 (3.90) | 19.0 (6.0) | |||
| Yes | 24.61 (6.01) | 25.0 (7.0) | 28.65 (7.93) | 16.0 (4.0) | 20.96 (4.90) | 21.0 (6.0) | |||
| Barriers | Statement | Parents | Healthcare Professionals | Pearson’s Chi-Square Test | p |
|---|---|---|---|---|---|
| Objective | Lack of digital devices | 9% | 70% | 36.551 | 0.000 |
| Lack of knowledge of digital technology | 25% | 84% | 34.059 | 0.000 | |
| Poor-quality internet connection | 36% | 64% | 7.666 | 0.006 | |
| Active involvement/supervision of parents during telemedicine services | 20% | 4% | 5.922 | 0.015 | |
| Presence of at-home distractions | 42% | 34% | 0.680 | 0.409 | |
| Camera is unable to follow children as they moved around | 24% | 34% | 1.040 | 0.308 | |
| Subjective | Severity level of ASD | 22% | 30% | 12.418 | 0.000 |
| ASD child’s embarrassment during telemedicine services | 22% | 8% | 3.813 | 0.051 | |
| Changes in ASD child’s behaviour during telemedicine services | 33% | 16% | 3.878 | 0.049 | |
| Distraction of ASD child due to the use of digital devices | 58% | 48% | 0.908 | 0.341 | |
| ASD child’s compliance influenced by the home setting | 53% | 46% | 0.510 | 0.475 | |
| Changes in the traditional doctor-patient relationship | 49% | 54% | 0.480 | 0.488 | |
| Potential negative effects of digital devices | 9% | 26% | 3.419 | 0.064 | |
| No barrier | 6% | 2% | 1.279 | 0.258 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gabellone, A.; Marzulli, L.; Matera, E.; Petruzzelli, M.G.; Margari, A.; Giannico, O.V.; Margari, L. Expectations and Concerns about the Use of Telemedicine for Autism Spectrum Disorder: A Cross-Sectional Survey of Parents and Healthcare Professionals. J. Clin. Med. 2022, 11, 3294. https://doi.org/10.3390/jcm11123294
Gabellone A, Marzulli L, Matera E, Petruzzelli MG, Margari A, Giannico OV, Margari L. Expectations and Concerns about the Use of Telemedicine for Autism Spectrum Disorder: A Cross-Sectional Survey of Parents and Healthcare Professionals. Journal of Clinical Medicine. 2022; 11(12):3294. https://doi.org/10.3390/jcm11123294
Chicago/Turabian StyleGabellone, Alessandra, Lucia Marzulli, Emilia Matera, Maria Giuseppina Petruzzelli, Anna Margari, Orazio Valerio Giannico, and Lucia Margari. 2022. "Expectations and Concerns about the Use of Telemedicine for Autism Spectrum Disorder: A Cross-Sectional Survey of Parents and Healthcare Professionals" Journal of Clinical Medicine 11, no. 12: 3294. https://doi.org/10.3390/jcm11123294
APA StyleGabellone, A., Marzulli, L., Matera, E., Petruzzelli, M. G., Margari, A., Giannico, O. V., & Margari, L. (2022). Expectations and Concerns about the Use of Telemedicine for Autism Spectrum Disorder: A Cross-Sectional Survey of Parents and Healthcare Professionals. Journal of Clinical Medicine, 11(12), 3294. https://doi.org/10.3390/jcm11123294