
Epidemiology and Treatment of Distal Radius Fractures in Finland—A Nationwide Register Study


Abstract
:1. Introduction
2. Materials and Methods
- All registered DRFs with code 52.5 or 52.6 between 1 January 2015 and 31 December 2019;
- Date of registration;
- Age of the patient at the first registration date;
- Only patients with Finnish social security number;
- Procedure of treatment (cast or operation according to NOMESCO classification, Supplementary Table S1);
- If the patient was registered in both the Specialist Care Register and the Primary Care Register, only the Specialist Care Register was utilized.
Statistical Analysis
3. Results
3.1. Incidence Rate of DRF
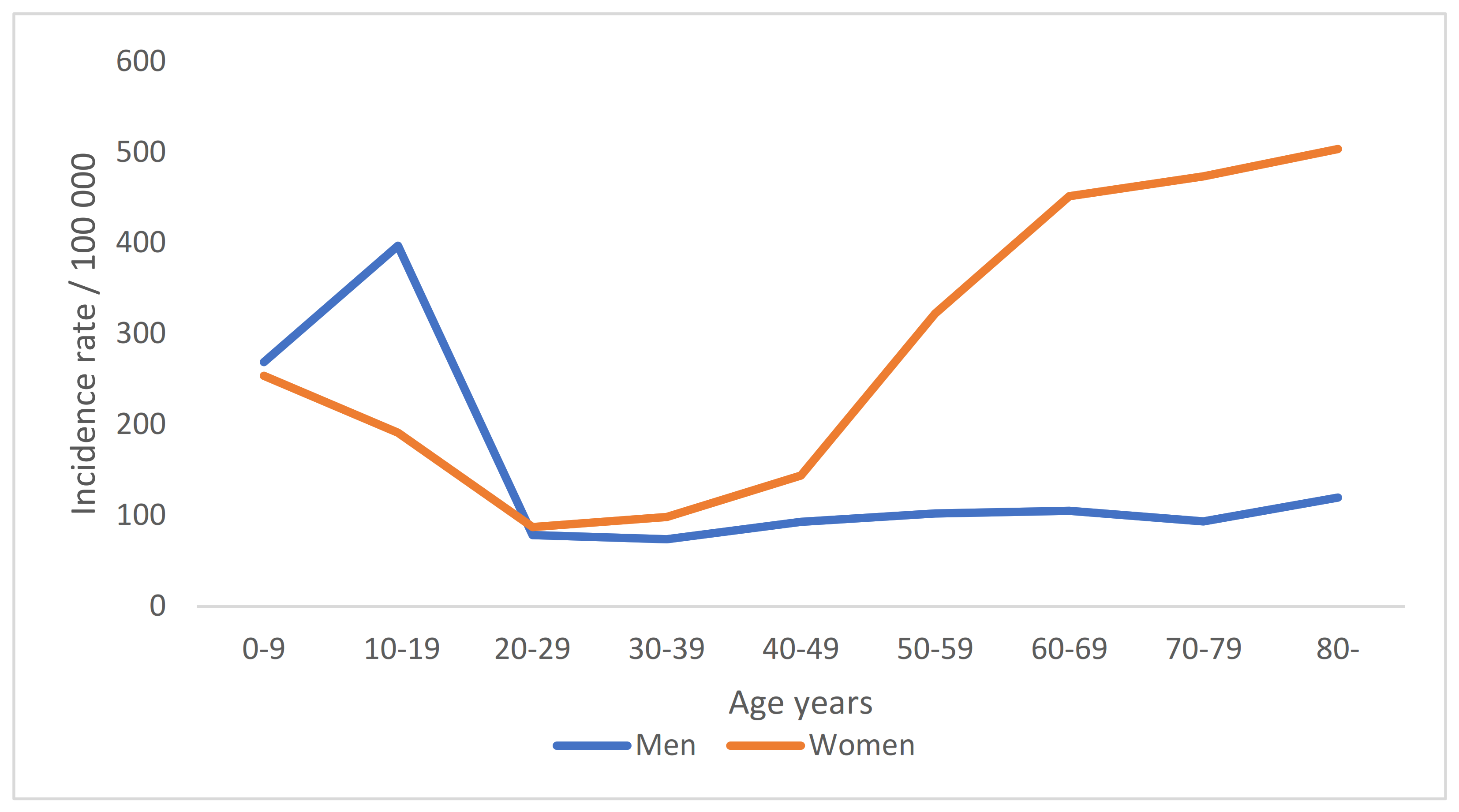
3.2. The Incidence of DRFs in Different Age Groups
3.3. The Annual Incidence of DRFs
3.4. Operative Treatment
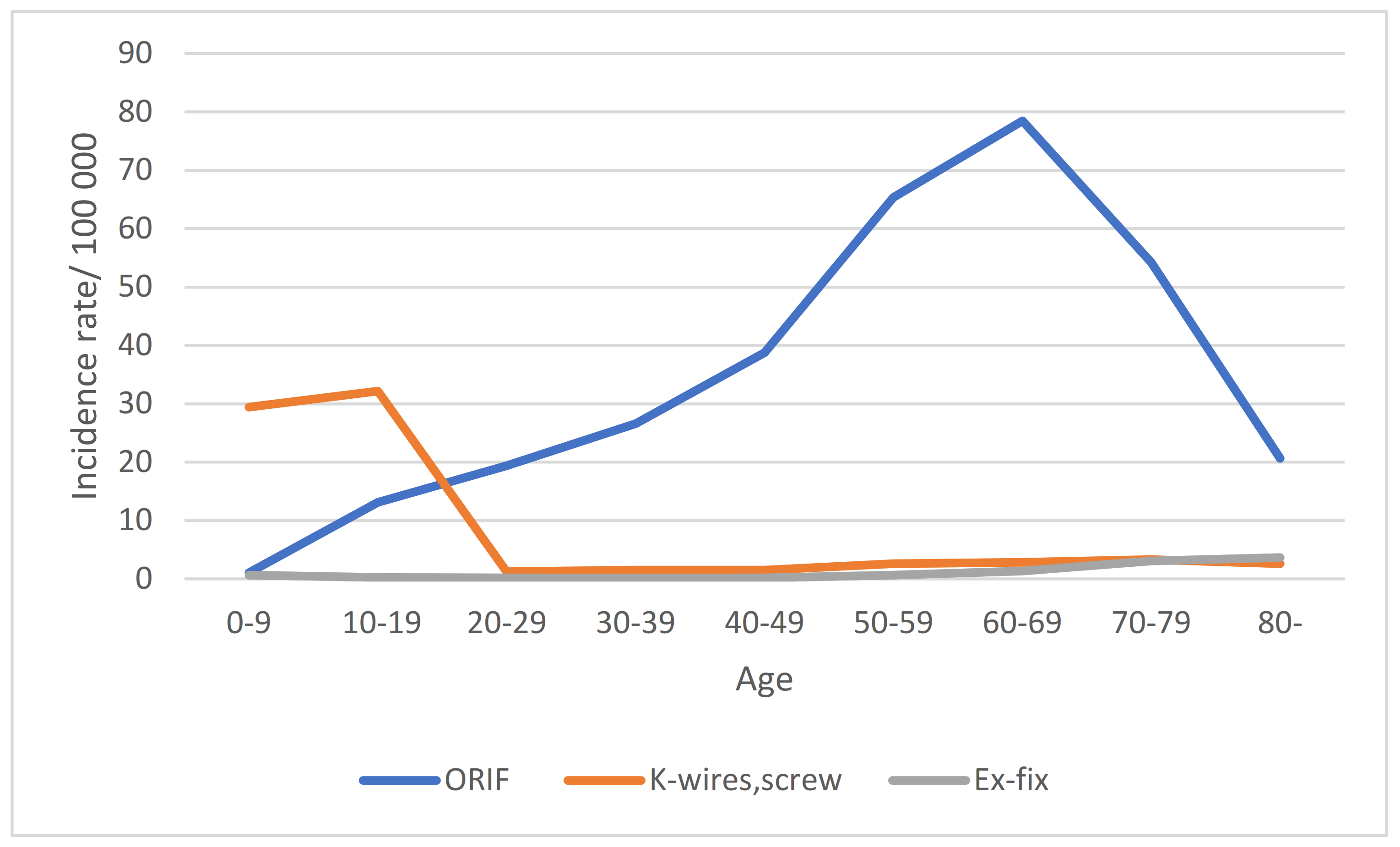
3.5. Operative Techniques
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Court-Brown, C.M.; Caesar, B. Epidemiology of Adult Fractures: A Review. Injury 2006, 37, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Stirling, E.R.B.; Johnson, N.A.; Dias, J.J. Epidemiology of Distal Radius Fractures in a Geographically Defined Adult Population. J. Hand Surg. Eur. Vol. 2018, 43, 974–982. [Google Scholar] [CrossRef] [PubMed]
- Azad, A.; Kang, H.P.; Alluri, R.K.; Vakhshori, V.; Kay, H.F.; Ghiassi, A. Epidemiological and Treatment Trends of Distal Radius Fractures across Multiple Age Groups. J. Wrist Surg. 2019, 8, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Wilcke, M.K.T.; Hammarberg, H.; Adolphson, P.Y. Epidemiology and Changed Surgical Treatment Methods for Fractures of the Distal Radius: A Registry Analysis of 42,583 Patients in Stockholm County, Sweden, 2004–2010. Acta Orthop. 2013, 84, 292–296. [Google Scholar] [CrossRef]
- Flinkkilä, T.; Sirniö, K.; Hippi, M.; Hartonen, S.; Ruuhela, R.; Ohtonen, P.; Hyvönen, P.; Leppilahti, J. Epidemiology and Seasonal Variation of Distal Radius Fractures in Oulu, Finland. Osteoporos. Int. 2011, 22, 2307–2312. [Google Scholar] [CrossRef]
- Armstrong, K.A.; von Schroeder, H.P.; Baxter, N.N.; Zhong, T.; Huang, A.; McCabe, S.J. Stable Rates of Operative Treatment of Distal Radius Fractures in Ontario, Canada: A Population-Based Retrospective Cohort Study (2004–2013). Can. J. Surg. 2019, 62, 386–392. [Google Scholar] [CrossRef] [Green Version]
- Solvang, H.W.; Nordheggen, R.A.; Clementsen, S.; Hammer, O.L.; Randsborg, P.H. Epidemiology of Distal Radius Fracture in Akershus, Norway, in 2010–2011. J. Orthop. Surg. Res. 2018, 13, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Lofthus, C.M.; Frihagen, F.; Meyer, H.E.; Nordsletten, L.; Melhuus, K.; Falch, J.A. Epidemiology of Distal Forearm Fractures in Oslo, Norway. Osteoporos. Int. 2008, 19, 781–786. [Google Scholar] [CrossRef]
- Mellstrand-Navarro, C.; Pettersson, H.J.; Tornqvist, H.; Ponzer, S. The Operative Treatment of Fractures of the Distal Radius Is Increasing. Bone Jt. J. 2014, 96-B, 963–969. [Google Scholar] [CrossRef] [Green Version]
- Rundgren, J.; Bojan, A.; Mellstrand Navarro, C.; Enocson, A. Epidemiology, Classification, Treatment and Mortality of Distal Radius Fractures in Adults: An Observational Study of 23,394 Fractures from the National Swedish Fracture Register. BMC Musculoskelet. Disord. 2020, 21, 88. [Google Scholar] [CrossRef]
- Südow, H.; Navarro, C.M. The Incidence of Distal Radius Fractures in a Swedish Pediatric Population-an Observational Cohort Study of 90 970 Individual Fractures. BMC Musculoskelet. Disord. 2021, 22, 1–8. [Google Scholar] [CrossRef]
- de Putter, C.E.; Selles, R.W.; Polinder, S.; Hartholt, K.A.; Looman, C.W.; Panneman, M.J.M.; Verhaar, J.A.N.; Hovius, S.E.R.; van Beeck, E.F. Epidemiology and Health-Care Utilisation of Wrist Fractures in Older Adults in The Netherlands, 1997–2009. Injury 2013, 44, 421–426. [Google Scholar] [CrossRef]
- Jo, Y.-H.; Lee, B.-G.; Kim, J.-H.; Lee, C.-H.; Kim, S.-J.; Choi, W.-S.; Koo, J.-W.; Lee, K.-H. National Surgical Trends for Distal Radius Fractures in Korea. J. Korean Med. Sci. 2017, 32, 1181. [Google Scholar] [CrossRef]
- Bergh Id, C.; Wennergren, D.; Mö Ller, M.; Brisby, H. Fracture Incidence in Adults in Relation to Age and Gender: A Study of 27,169 Fractures in the Swedish Fracture Register in a Well-Defined Catchment Area. PLoS ONE 2020, 15, e0244291. [Google Scholar] [CrossRef]
- Sebastin, S.J.; Chung, K.C. An Asian Perspective on the Management of Distal Radius Fractures. Hand Clin. 2012, 28, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Jerrhag, D.; Englund, M.; Karlsson, M.K.; Rosengren, B.E. Epidemiology and Time Trends of Distal Forearm Fractures in Adults—A Study of 11.2 Million Person-Years in Sweden. BMC Musculoskelet. Disord. 2017, 18, 240. [Google Scholar] [CrossRef] [Green Version]
- Thompson, P.W.; Taylor, J.; Dawson, A. The Annual Incidence and Seasonal Variation of Fractures of the Distal Radius in Men and Women over 25 Years in Dorset, UK. Injury 2004, 35, 462–466. [Google Scholar] [CrossRef]
- Mattila, V.M.; Huttunen, T.T.; Sillanpää, P.; Niemi, S.; Pihlajamäki, H.; Kannus, P. Significant Change in the Surgical Treatment of Distal Radius Fractures: A Nationwide Study between 1998 and 2008 in Finland. J. Trauma-Inj. Infect. Crit. Care 2011, 71, 939–942. [Google Scholar] [CrossRef]
- Hevonkorpi, T.P.; Launonen, A.P.; Huttunen, T.T.; Kannus, P.; Niemi, S.; Mattila, V.M. Incidence of Distal Radius Fracture Surgery in Finns Aged 50 Years or More between 1998 and 2016—Too Many Patients Are yet Operated On? BMC Musculoskelet. Disord. 2018, 19, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Saving, J.; Ponzer, S.; Enocson, A.; Navarro, C.M. Distal Radius Fractures—Regional Variation in Treatment Regimens. PLoS ONE 2018, 13, e0207702. [Google Scholar] [CrossRef]
- Huetteman, H.E.; Shauver, M.J.; Malay, S.; Chung, T.T.; Chung, K.C. Variation in the Treatment of Distal Radius Fractures in the United States: 2010 to 2015. Plast. Reconstr. Surg. 2019, 143, 159–167. [Google Scholar] [CrossRef]
- Sund, R. Quality of the Finnish Hospital Discharge Register: A Systematic Review. Scand. J. Public Health 2012, 40, 505–515. [Google Scholar] [CrossRef]
- Abrahamsen, B.; Jørgensen, N.R.; Schwarz, P. Epidemiology of Forearm Fractures in Adults in Denmark: National Age- and Gender-Specific Incidence Rates, Ratio of Forearm to Hip Fractures, and Extent of Surgical Fracture Repair in Inpatients and Outpatients. Osteoporos. Int. 2015, 26, 67–76. [Google Scholar] [CrossRef]
- Jo, Y.H.; Lee, B.G.; Kim, H.S.; Kim, J.H.; Lee, C.H.; Kim, S.J.; Choi, W.S.; Lee, J.H.; Lee, K.H. Incidence and Seasonal Variation of Distal Radius Fractures in Korea: A Population-Based Study. J. Korean Med. Sci. 2018, 33, e48. [Google Scholar] [CrossRef]
- Hagino, H.; Yamamoto, K.; Ohshiro, H.; Nose, T. Increasing Incidence of Distal Radius Fractures in Japanese Children and Adolescents. J. Orthop. Sci. 2000, 5, 356–360. [Google Scholar] [CrossRef]
- Khosla, S.; Melton, L.J.; Dekutoski, M.B.; Achenbach, S.J.; Oberg, A.L.; Riggs, B.L. Incidence of Childhood Distal Forearm Fractures Over 30 Years A Population-Based Study. JAMA 2003, 290, 1479–1485. [Google Scholar] [CrossRef] [Green Version]
- Sinikumpu, J.J.; Lautamo, A.; Pokka, T.; Serlo, W. The Increasing Incidence of Paediatric Diaphyseal Both-Bone Forearm Fractures and Their Internal Fixation during the Last Decade. Injury 2012, 43, 362–366. [Google Scholar] [CrossRef]
- Chung, K.C.; Shauver, M.J.; Birkmeyer, J.D. Trends in the United States in the Treatment of Distal Radial Fractures in the Elderly. J. Bone Jt. Surg.-Ser. A 2009, 91, 1868–1873. [Google Scholar] [CrossRef] [Green Version]
- Mosenthal, W.P.; Boyajian, H.H.; Ham, S.A.; Conti Mica, M.A. Treatment Trends, Complications, and Effects of Comorbidities on Distal Radius Fractures. Hand 2019, 14, 534–539. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Population | Primary Care | Specialist Care | Incidence of Operations |
|---|---|---|---|
| Men | 44.81 (43.68–45.93) | 146.41 (144.37–148.40) | 31.14 (30.20–32.06) |
| Women | 90.31 (88.73–91.88 | 254.56 (251.92–257.21) | 58.58 (57.32–59.85) |
| All | 69.53 (68.55–70.52) | 204.90 (203.21–206.59) | 45.66 (45.66–45.66) |
| Age Group, Years | Incidence Rate of DRFs Men | Incidence Rate of DRFs Women |
|---|---|---|
| 0–9 | 269.06 | 253.97 |
| 10–19 | 397.23 | 191.32 |
| 20–29 | 78.9 | 87.5 |
| 30–39 | 74.1 | 98.39 |
| 40–49 | 93.12 | 144.27 |
| 50–59 | 102.53 | 322.62 |
| 60–69 | 105.23 | 451.81 |
| 70–79 | 93.63 | 473.66 |
| 80– | 119.95 | 503.68 |
| Year | 2015 | 2016 | 2017 | 2018 | 2019 |
|---|---|---|---|---|---|
| Any operation | 43.07 (41.33–44.80) | 43.69 (41.95–45.44) | 46.97 (45.17–48.78) | 47.35 (45.54–45.16) | 47.42 (45.60–49.23) |
| ORIF * | 32.70 (31.18–34.21) | 33.9 (32.39–35.47) | 38.16 (36.53–39.79) | 38.90 (37.25–40.54) | 39.43 (37.78–41.09) |
| K-wires, screw ** | 9.07 (8.28–9.87) | 8.89 (8.10–9.68) | 7.91 (7.17–8.65) | 7.82 (7.08–8.55) | 7.72 (6.99–8.45) |
| Ex-fix *** | 1.30 (0.99–1.62) | 0.88 (0.63–1.12) | 0.9 (0.65–1.15) | 0.64 (0.43–0.85) | 0.26 (0.13–0.39) |
| Age | ORIF | K-Wires, Screw | Ex-Fix | Incidence Rate of Any Surgery Per Age Group |
|---|---|---|---|---|
| 0–9 | 1.06 (1.06–1.06) | 29.43 (29.43–29.43) | 0.68 (0.07–0.07) | 30.55 (30.55–30.55) |
| 10–19 | 13.15 (13.15–13.15) | 32.17 (32.17–32.17) | 0.23 (0.23–0.23) | 45.55 (45.55–45.55) |
| 20–29 | 19.37 (19.37–19.37) | 1.24 (1.24–1.24) | 0.15 (0.15–0.15) | 20.75 (20.75–20.75) |
| 30–39 | 26.57 (26.57–26.57) | 1.50 (1.50–1.50) | 0.14 (0.14–0.14) | 28.22 (28.21–28.22) |
| 40–49 | 38.79 (38.79–38.79) | 1.51 (1.51–1.51) | 0.15 (0.15–0.15) | 40.46 (40.45–40.46) |
| 50–59 | 65.32 (62.32–65.32) | 2.64 (2.64–2.64) | 0.65 (0.65–0.65) | 68.61 (68.61–68.61) |
| 60–69 | 78.46 (78.45–78.46) | 2.83 (2.83–2.83) | 1.33 (1.33–1.33) | 82.61 (82.61–82.61) |
| 70–79 | 54.19 (54.19–54.19) | 3.28 (3.28–3.28) | 3.05 (3.05–3.05) | 60.51 (60.51–60.51) |
| 80– | 20.66 (20.65–20.66) | 2.63 (2.63–2.63) | 3.65 (3.65–3.65) | 26.93 (26.93–26.93) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raudasoja, L.; Aspinen, S.; Vastamäki, H.; Ryhänen, J.; Hulkkonen, S. Epidemiology and Treatment of Distal Radius Fractures in Finland—A Nationwide Register Study. J. Clin. Med. 2022, 11, 2851. https://doi.org/10.3390/jcm11102851
Raudasoja L, Aspinen S, Vastamäki H, Ryhänen J, Hulkkonen S. Epidemiology and Treatment of Distal Radius Fractures in Finland—A Nationwide Register Study. Journal of Clinical Medicine. 2022; 11(10):2851. https://doi.org/10.3390/jcm11102851
Chicago/Turabian StyleRaudasoja, Leena, Samuli Aspinen, Heidi Vastamäki, Jorma Ryhänen, and Sina Hulkkonen. 2022. "Epidemiology and Treatment of Distal Radius Fractures in Finland—A Nationwide Register Study" Journal of Clinical Medicine 11, no. 10: 2851. https://doi.org/10.3390/jcm11102851
APA StyleRaudasoja, L., Aspinen, S., Vastamäki, H., Ryhänen, J., & Hulkkonen, S. (2022). Epidemiology and Treatment of Distal Radius Fractures in Finland—A Nationwide Register Study. Journal of Clinical Medicine, 11(10), 2851. https://doi.org/10.3390/jcm11102851