
Altered Plasma Proteins in Myogenous Temporomandibular Disorders


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. General Methodology
2.3. Pressure Pain Threshold
2.4. Questionnaire
2.4.1. Physical Activity Level
2.4.2. Symptom Questionnaire
2.4.3. Graded Chronic Pain Scale
2.4.4. Jaw Functional Limitation Scale
2.4.5. Patient Health Questionnaire
2.4.6. Generalized Anxiety Disorder
2.4.7. Pain Catastrophizing Scale
2.4.8. Perceived Stress Scale
2.4.9. Insomnia Severity Index
2.4.10. Quality of Life
2.5. Blood Sampling
2.6. Analyses
2.7. Statistics
3. Results
3.1. Background Data
3.2. Plasma Proteins
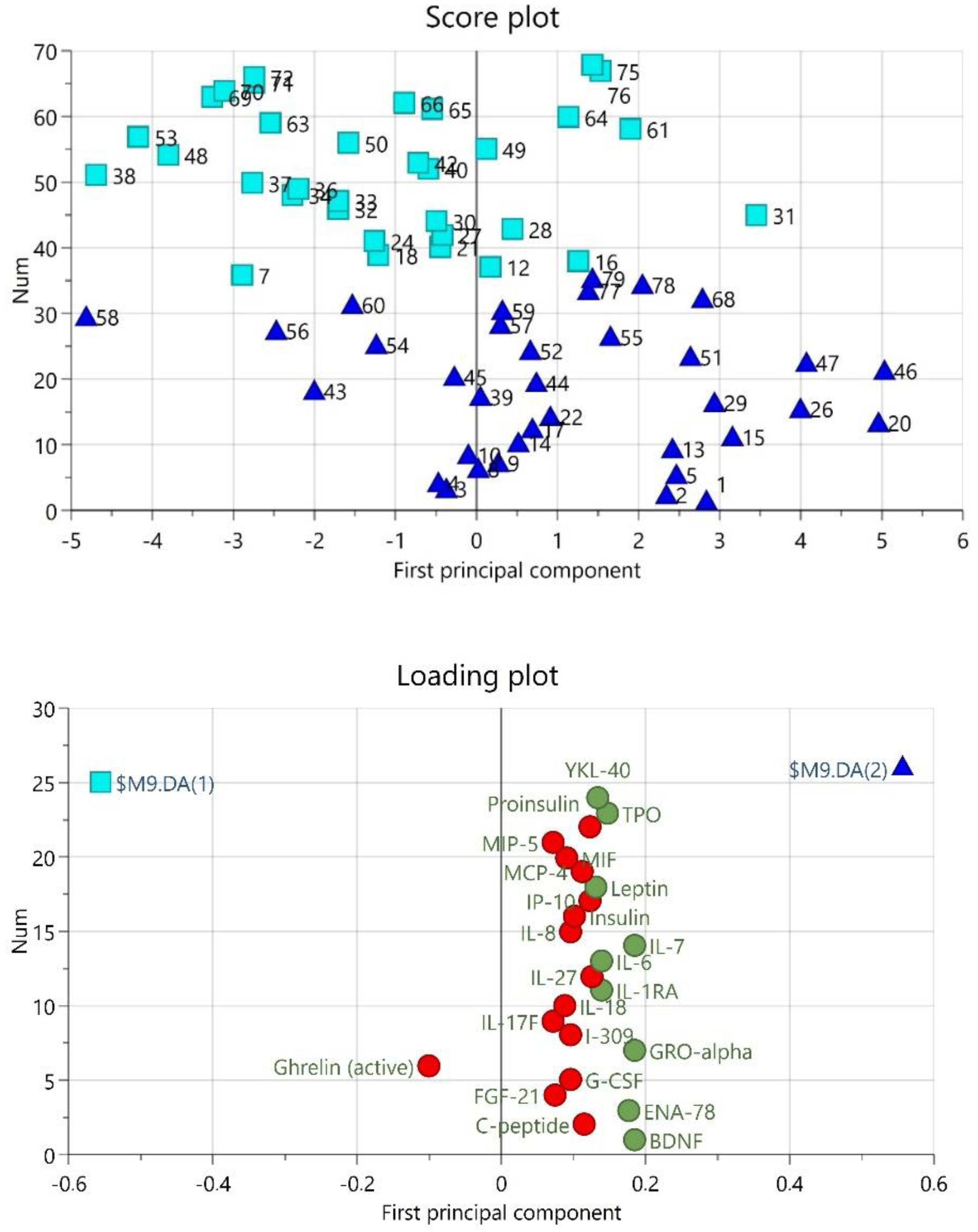
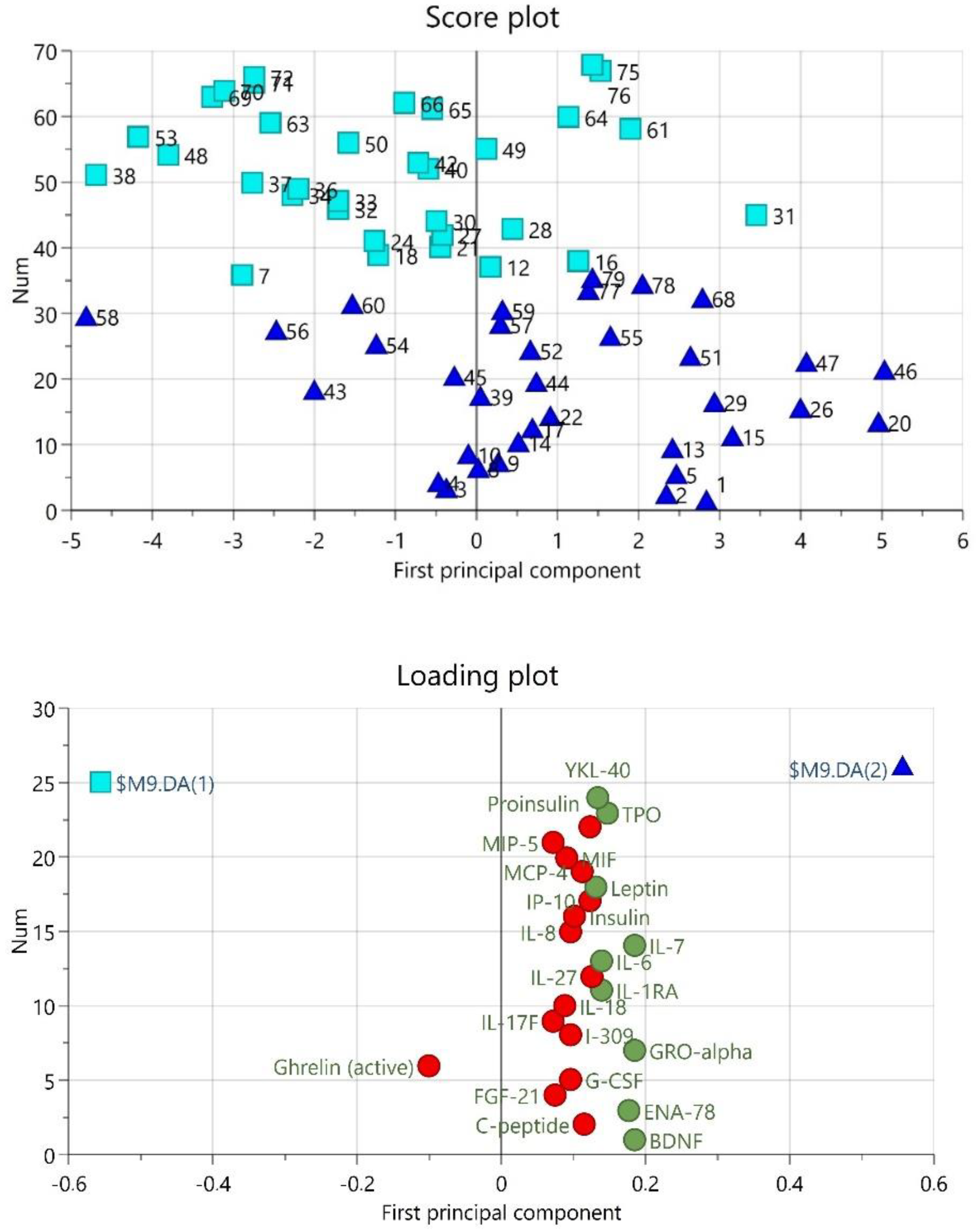
3.3. Multivariate Correlation between Markers and Clinical Parameters in TMD Patients
4. Discussion
4.1. Proteins Distinguishing TMDM from Controls
4.2. Differences between MYA and MFP
4.3. Correlation to Clinical Variables
4.4. Strengths and Limitations
4.5. Clinical Significance
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goldberg, D.S.; McGee, S.J. Pain as a global public health priority. BMC Public Health 2011, 11, 770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blyth, F.M.; Briggs, A.M.; Schneider, C.H.; Hoy, D.G.; March, L.M. The Global burden of musculoskeletal pain-where to from here? Am. J. Public Health 2019, 109, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: Recommendations of the international RDC/TMD consortium network and orofacial pain special interest groupdagger. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef] [PubMed]
- Wright, E.F. Referred craniofacial pain patterns in patients with temporomandibular disorder. J. Am. Dent. Assoc. 2000, 131, 1307–1315. [Google Scholar] [CrossRef] [PubMed]
- Fillingim, R.B.; Slade, G.D.; Greenspan, J.D.; Dubner, R.; Maixner, W.; Bair, E.; Ohrbach, R. Long-term changes in biopsychosocial characteristics related to temporomandibular disorder: Findings from the OPPERA study. Pain 2018, 159, 2403–2413. [Google Scholar] [CrossRef]
- Shrivastava, M.; Battaglino, R.; Ye, L. A comprehensive review on biomarkers associated with painful temporomandibular disorders. Int. J. Oral Sci. 2021, 13, 23. [Google Scholar] [CrossRef]
- Ceusters, W.; Nasri-Heir, C.; Alnaas, D.; Cairns, B.E.; Michelotti, A.; Ohrbach, R. Perspectives on next steps in classification of oro-facial pain-Part 3: Biomarkers of chronic oro-facial pain-from research to clinic. J. Oral Rehabil. 2015, 42, 956–966. [Google Scholar] [CrossRef] [Green Version]
- Ernberg, M.; Hedenberg-Magnusson, B.; Alstergren, P.; Kopp, S. The level of serotonin in the superficial masseter muscle in relation to local pain and allodynia. Life Sci. 1999, 65, 313–325. [Google Scholar] [CrossRef]
- Castrillon, E.E.; Ernberg, M.; Cairns, B.E.; Wang, K.; Sessle, B.J.; Arendt-Nielsen, L.; Svensson, P. Interstitial glutamate concentration is elevated in the masseter muscle of myofascial temporomandibular disorder patients. J. Orofac. Pain 2010, 24, 350–360. [Google Scholar]
- Dawson, A.; Ghafouri, B.; Gerdle, B.; List, T.; Svensson, P.; Ernberg, M. Effects of experimental tooth clenching on pain and intramuscular release of 5-HT and glutamate in patients with myofascial TMD. Clin. J. Pain 2015, 31, 740–749. [Google Scholar] [CrossRef]
- Dawson, A.; Stensson, N.; Ghafouri, B.; Gerdle, B.; List, T.; Svensson, P.; Ernberg, M. Dopamine in plasma-a biomarker for myofascial TMD pain? J. Headache Pain 2016, 17, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basi, D.L.; Velly, A.M.; Schiffman, E.L.; Lenton, P.A.; Besspiata, D.A.; Rankin, A.M.; Hughes, P.J.; Swift, J.Q.; Kehl, L.J. Human temporomandibular joint and myofascial pain biochemical profiles: A case-control study. J. Oral Rehabil. 2012, 39, 326–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madariaga, V.I.; Jasim, H.; Ghafouri, B.; Ernberg, M. Myogenous temporomandibular disorders and salivary markers of oxidative stress-A cross-sectional study. J. Oral Rehabil. 2021, 48, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Omidpanah, N.; Ebrahimi, S.; Raygani, A.V.; Mozafari, H.; Rezaei, M. Total antioxidant capacity, catalase activity and salivary oxidative parameters in patients with temporomandibular disorders. Front. Dent. 2020, 17, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Louca Jounger, S.; Christidis, N.; Svensson, P.; List, T.; Ernberg, M. Increased levels of intramuscular cytokines in patients with jaw muscle pain. J. Headache Pain 2017, 18, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slade, G.D.; Conrad, M.S.; Diatchenko, L.; Rashid, N.U.; Zhong, S.; Smith, S.; Rhodes, J.; Medvedev, A.; Makarov, S.; Maixner, W.; et al. Cytokine biomarkers and chronic pain: Association of genes, transcription, and circulating proteins with temporomandibular disorders and widespread palpation tenderness. Pain 2011, 152, 2802–2812. [Google Scholar] [CrossRef] [Green Version]
- Jasim, H.; Ernberg, M.; Carlsson, A.; Gerdle, B.; Ghafouri, B. Protein signature in saliva of temporomandibular disorders myalgia. Int. J. Mol. Sci. 2020, 21, 2569. [Google Scholar] [CrossRef] [Green Version]
- Dawes, C.; Wong, D.T.W. Role of saliva and salivary diagnostics in the advancement of oral health. J. Dent. Res. 2019, 98, 133–141. [Google Scholar] [CrossRef]
- Jasim, H.; Ghafouri, B.; Gerdle, B.; Hedenberg-Magnusson, B.; Ernberg, M. Altered levels of salivary and plasma pain related markers in temporomandibular disorders. J. Headache Pain 2020, 21, 105. [Google Scholar] [CrossRef]
- Ohrbach, R.; Gonzalez, Y.; List, T.; Michelotti, A.; Schiffman, E. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD). Clinical Examination Protocol: Version 2 June 2013. Available online: www.rdc-tmdinternational.org (accessed on 20 March 2022).
- Ohrbach, R. Diagnostic Criteria for Temporomandibular Disorders: Assessment Instruments. Version 15 May 2016. Available online: www.rdc-tmdinternational.org (accessed on 11 November 2021).
- Von Korff, M.; Ormel, J.; Keefe, F.J.; Dworkin, S.F. Grading the severity of chronic pain. Pain 1992, 50, 133–149. [Google Scholar] [CrossRef]
- Ohrbach, R.; Knibbe, W. Diagnostic Criteria for Temporomandibular Disorders: Scoring Manual for Self-Report Instruments. Version 29 May 2016. Available online: www.rdc-tmdinternational.org (accessed on 11 November 2021).
- Ohrbach, R.; Larsson, P.; List, T. The jaw functional limitation scale: Development, reliability, and validity of 8-item and 20-item versions. J. Orofac. Pain 2008, 22, 219–230. [Google Scholar] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-15: Validity of a new measure for evaluating the severity of somatic symptoms. Psychosom. Med. 2002, 64, 258–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, M.J.L.; Bishop, S.R.; Pivik, J. The pain catastrophizing scale: Development and validation. Psychol. Assess. 1995, 7, 8. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Nordin, M.; Nordin, S. Psychometric evaluation and normative data of the Swedish version of the 10-item perceived stress scale. Scand. J. Psychol. 2013, 54, 502–507. [Google Scholar] [CrossRef]
- NH Department of Administrative Services Perceived Stress Scale. 2021. Available online: https://das.nh.gov/wellness/docs/percieved%20stress%20scale.pdf (accessed on 27 September 2021).
- Morin, C.M.; Belleville, G.; Belanger, L.; Ivers, H. The insomnia severity index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [Green Version]
- John, M.T.; Miglioretti, D.L.; LeResche, L.; Koepsell, T.D.; Hujoel, P.; Micheelis, W. German short forms of the Oral Health Impact Profile. Community Dent. Oral Epidemiol. 2006, 34, 277–288. [Google Scholar] [CrossRef]
- Larsson, P.; List, T.; Lundstrom, I.; Marcusson, A.; Ohrbach, R. Reliability and validity of a Swedish version of the Oral Health Impact Profile (OHIP-S). Acta Odontol. Scand. 2004, 62, 147–152. [Google Scholar] [CrossRef]
- Gerdle, B.; Ghafouri, B.; Ghafouri, N.; Backryd, E.; Gordh, T. Signs of ongoing inflammation in female patients with chronic widespread pain: A multivariate, explorative, cross-sectional study of blood samples. Med. (Baltim.) 2017, 96, e6130. [Google Scholar] [CrossRef]
- Wheelock, A.M.; Wheelock, C.E. Trials and tribulations of ‘omics data analysis: Assessing quality of SIMCA-based multivariate models using examples from pulmonary medicine. Mol. Biosyst. 2013, 9, 2589–2596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wåhlen, K.; Ghafouri, B.; Ghafouri, N.; Gerdle, B. Plasma Protein pattern correlates with pain intensity and psychological distress in women with chronic widespread pain. Front. Psychol. 2018, 9, 2400. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, L.; Byrne, T.; Johansson, E.; Trygg, J.; Vikström, C. Multi- and Megavariate Data Analysis: Basic Principles and Applications, 3rd ed.; MKS Umetrics AB: Malmö, Sweden, 2013. [Google Scholar]
- Nishimoto, N. Interleukin-6 in rheumatoid arthritis. Curr. Opin. Rheumatol. 2006, 18, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Dowlati, Y.; Herrmann, N.; Swardfager, W.; Liu, H.; Sham, L.; Reim, E.K.; Lanctot, K.L. A meta-analysis of cytokines in major depression. Biol. Psychiatry 2010, 67, 446–457. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.Q.; Liu, Z.; Liu, Z.H.; Chen, S.P.; Li, M.; Shahveranov, A.; Ye, D.W.; Tian, Y.K. Interleukin-6: An emerging regulator of pathological pain. J. Neuroinflamm. 2016, 13, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zwiri, A.; Al-Hatamleh, M.A.I.; WMA, W.A.; Ahmed Asif, J.; Khoo, S.P.; Husein, A.; Ab-Ghani, Z.; Kassim, N.K. Biomarkers for Temporomandibular Disorders: Current Status and Future Directions. Diagnostics 2020, 10, 303. [Google Scholar] [CrossRef]
- Park, J.W.; Chung, J.W. Inflammatory cytokines and sleep disturbance in patients with temporomandibular disorders. J. Oral Facial Pain Headache 2016, 30, 27–33. [Google Scholar] [CrossRef]
- Costello, N.L.; Bragdon, E.E.; Light, K.C.; Sigurdsson, A.; Bunting, S.; Grewen, K.; Maixner, W. Temporomandibular disorder and optimism: Relationships to ischemic pain sensitivity and interleukin-6. Pain 2002, 100, 99–110. [Google Scholar] [CrossRef]
- Hunt, C.; Mun, C.J.; Owens, M.; Lerman, S.; Kunatharaju, S.; Tennen, H.; Buenaver, L.; Campbell, C.; Haythornthwaite, J.; Smith, M.; et al. Sleep, positive affect and circulating interleukin-6 in women with temporomandibular joint disorder. Psychosom. Med. 2022, 22, 610. [Google Scholar] [CrossRef]
- Pal, M.; Febbraio, M.A.; Whitham, M. From cytokine to myokine: The emerging role of interleukin-6 in metabolic regulation. Immunol. Cell Biol. 2014, 92, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Barata, J.T.; Durum, S.K.; Seddon, B. Flip the coin: IL-7 and IL-7R in health and disease. Nat. Immunol. 2019, 20, 1584–1593. [Google Scholar] [CrossRef] [PubMed]
- Heitzer, E.; Sandner-Kiesling, A.; Schippinger, W.; Stohscheer, I.; Osprian, I.; Bitsche, S.; Eisner, F.; Verebes, J.; Hofmann, G.; Samonigg, H. IL-7, IL-18, MCP-1, MIP1-beta, and OPG as biomarkers for pain treatment response in patients with cancer. Pain Physician 2012, 15, 499–510. [Google Scholar] [PubMed]
- Jonsjo, M.A.; Olsson, G.L.; Wicksell, R.K.; Alving, K.; Holmstrom, L.; Andreasson, A. The role of low-grade inflammation in ME/CFS (Myalgic Encephalomyelitis/Chronic Fatigue Syndrome)-associations with symptoms. Psychoneuroendocrinology 2020, 113, 104578. [Google Scholar] [CrossRef]
- Lehto, S.M.; Huotari, A.; Niskanen, L.; Herzig, K.H.; Tolmunen, T.; Viinamaki, H.; Koivumaa-Honkanen, H.; Honkalampi, K.; Sinikallio, S.; Ruotsalainen, H.; et al. Serum IL-7 and G-CSF in major depressive disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2010, 34, 846–851. [Google Scholar] [CrossRef]
- Keeler, J.L.; Patsalos, O.; Chung, R.; Schmidt, U.; Breen, G.; Treasure, J.; Himmerich, H.; Dalton, B. Reduced MIP-1beta as a Trait marker and reduced IL-7 and IL-12 as state markers of anorexia nervosa. J. Pers. Med. 2021, 11, 814. [Google Scholar] [CrossRef]
- Arend, W.P.; Malyak, M.; Guthridge, C.J.; Gabay, C. Interleukin-1 receptor antagonist: Role in biology. Annu. Rev. Immunol. 1998, 16, 27–55. [Google Scholar] [CrossRef]
- Barjandi, G.; Kosek, E.; Hedenberg-Magnusson, B.; Velly, A.M.; Ernberg, M. Comorbid conditions in temporomandibular disorders myalgia and myofascial pain compared to fibromyalgia. J. Clin. Med. 2021, 10, 3138. [Google Scholar] [CrossRef]
- Tumer, M.K.; Nursal, A.F.; Tekcan, A.; Yerliyurt, K.; Geyko, A.; Yigit, S. The IL-1Ra gene variable number tandem repeat variant is associated with susceptibility to temporomandibular disorders in Turkish population. J. Clin. Lab. Anal. 2018, 32. [Google Scholar] [CrossRef] [Green Version]
- Fischer, M.; Wille, G.; Klien, S.; Shanib, H.; Holle, D.; Gaul, C.; Broessner, G. Brain-derived neurotrophic factor in primary headaches. J. Headache Pain 2012, 13, 469–475. [Google Scholar] [CrossRef] [Green Version]
- Jablochkova, A.; Backryd, E.; Kosek, E.; Mannerkorpi, K.; Ernberg, M.; Gerdle, B.; Ghafouri, B. Unaltered low nerve growth factor and high brain-derived neurotrophic factor levels in plasma from patients with fibromyalgia after a 15-week progressive resistance exercise. J. Rehabil. Med. 2019, 51, 779–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, E.J.; Reichardt, L.F. Neurotrophins: Roles in neuronal development and function. Annu. Rev. Neurosci. 2001, 24, 677–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maciejewska-Szaniec, Z.; Kaczmarek-Rys, M.; Hryhorowicz, S.; Przystanska, A.; Gredes, T.; Maciejewska, B.; Hoppe-Golebiewska, J.; Slomski, R.; Plawski, A.; Czajka-Jakubowska, A. Polymorphic variants in genes related to stress coping are associated with the awake bruxism. BMC Oral. Health 2021, 21, 496. [Google Scholar] [CrossRef] [PubMed]
- Slade, G.D.; Ohrbach, R.; Greenspan, J.D.; Fillingim, R.B.; Bair, E.; Sanders, A.E.; Dubner, R.; Diatchenko, L.; Meloto, C.B.; Smith, S.; et al. Painful temporomandibular disorder: Decade of discovery from OPPERA studies. J. Dent. Res. 2016, 95, 1084–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawes, J.M.; Calvo, M.; Perkins, J.R.; Paterson, K.J.; Kiesewetter, H.; Hobbs, C.; Kaan, T.K.; Orengo, C.; Bennett, D.L.; McMahon, S.B. CXCL5 mediates UVB irradiation-induced pain. Sci. Transl. Med. 2011, 3, 90ra60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hysing, E.B.; Smith, L.; Thulin, M.; Karlsten, R.; Bothelius, K.; Gordh, T. Detection of systemic inflammation in severely impaired chronic pain patients and effects of a multimodal pain rehabilitation program. Scand. J. Pain 2019, 19, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Silva, R.L.; Lopes, A.H.; Guimaraes, R.M.; Cunha, T.M. CXCL1/CXCR2 signaling in pathological pain: Role in peripheral and central sensitization. Neurobiol. Dis. 2017, 105, 109–116. [Google Scholar] [CrossRef]
- Jonsson, M.; Gerdle, B.; Ghafouri, B.; Backryd, E. The inflammatory profile of cerebrospinal fluid, plasma, and saliva from patients with severe neuropathic pain and healthy controls-a pilot study. BMC Neurosci. 2021, 22, 6. [Google Scholar] [CrossRef]
- Kosek, E.; Clauw, D.; Nijs, J.; Baron, R.; Gilron, I.; Harris, R.E.; Mico, J.A.; Rice, A.S.C.; Sterling, M. Chronic nociplastic pain affecting the musculoskeletal system: Clinical criteria and grading system. Pain 2021, 162, 2629–2634. [Google Scholar] [CrossRef]
- Ye, Y.; Salvo, E.; Romero-Reyes, M.; Akerman, S.; Shimizu, E.; Kobayashi, Y.; Michot, B.; Gibbs, J. Glia and orofacial pain: Progress and future directions. Int. J. Mol. Sci. 2021, 22, 5345. [Google Scholar] [CrossRef]
- O’Mahony, L.F.; Srivastava, A.; Mehta, P.; Ciurtin, C. Is fibromyalgia associated with a unique cytokine profile? A systematic review and meta-analysis. Rheumatology (Oxford) 2021, 60, 2602–2614. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Waise, T.M.Z.; Toshinai, K.; Tsuchimochi, W.; Naznin, F.; Islam, M.N.; Tanida, R.; Sakoda, H.; Nakazato, M. Functional interaction between Ghrelin and GLP-1 regulates feeding through the vagal afferent system. Sci. Rep. 2020, 10, 18415. [Google Scholar] [CrossRef] [PubMed]
- Jasim, H.; Carlsson, A.; Gerdle, B.; Ernberg, M.; Ghafouri, B. Diurnal variation of inflammatory plasma proteins involved in pain. Pain Rep. 2019, 4, e776. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| TMDM n = 39 | CON n = 38 | p-Value | MYA n = 14 | MFP n = 25 | p-Value | |
|---|---|---|---|---|---|---|
| Age (yr) | 29.1 (7.4) | 29.0 (7.0) | 0.890 | 28.6 (7.9) | 29.3 (7.3) | 0.413 |
| Sex (n, %F) | 32 (82) | 31 (82) | NT | 10 (71) | 22 (88) | |
| BMI (kg/m2) | 23.7 (3.9) | 22.7 (3.3.) | 0.331 | 23.0 (2.6) | 24.3 (4.5) | 0.300 |
| Country | 0.174 | NT | ||||
| Scandinavia | 28 (72) | 26 (68) | 12 (86) | 16 (64) | ||
| Europe | 0 | 3 (8) | 0 | 0 | ||
| Other | 11 (28) | 8 (21) | 2 (14) | 9 (36) | ||
| Education | 0.322 | 0.964 | ||||
| Elementary | 2 (5) | 1 (3) | 1 (7) | 1 (4) | ||
| High school | 13 (33) | 15 (39) | 5 (36) | 8 (32) | ||
| University | 21 (54) | 22 (58) | 7 (50) | 14 (56) | ||
| Other | 3 (8) | 0 | 1 (7) | 2 (8) | ||
| Occupation | 0.898 | 0.128 | ||||
| Employed | 17 (44) | 22 (58) | 3 (21) | 13 (52) | ||
| Student | 22 (56) | 16 (42) | 11 (89) | 12 (48) | ||
| Physical activity * | 0.994 | 0.235 | ||||
| 1–2 times/mo | 6 (17) | 6 (16) | 2 (17) | 4 (17) | ||
| 1–2 times/w | 15 (43) | 16 (43) | 3 (25) | 12 (52) | ||
| ≥3 times/w | 14 (40) | 15 (41) | 7 (58) | 7 (31) | ||
| JFLS tot | 1.2 (1.7) | 0 (0) | <0.001 | 0.5 (1.8) | 1.6 (1.4) | 0.009 |
| PHQ-9 | 6.0 (6.5) | 1.0 (3.8) | <0.001 | 5.0 (5.8) | 6.0 (6.0) | 0.140 |
| GAD-7 | 4.0 (5.0) | 1.5 (3.0) | <0.001 | 4.5 (6.5) | 4.0 (4.5) | 0.986 |
| PHQ-15 | 10.0 (6.5) | 3.0 (3.8) | <0.001 | 9.0 (3.0) | 11.0 (5.0) | 0.411 |
| PSS-10 | 17.0 (11.0) | 10.0 (8.5) | 0.005 | 14.5 (16.8) | 19.0 (7.0) | 0.062 |
| PCS | 14.0 (15.0) | 3.0 (10.0) | <0.001 | 13.0 (10.0) | 14.0 (13.0) | 0.837 |
| ISI | 10.0 (8.5) | 5.0 (5.3) | <0.001 | 9.0 (8.0) | 10.0 (10.0) | 0.093 |
| OHIP-5 | 6.0 (5.0) | 0.0 (0.1) | <0.001 | 4.0 (3.5) | 7.0 (5.0) | 0.047 |
| TMDM n = 39 | CON n = 38 | p-Value | MYA n = 14 | MFP n =25 | p-Value | |
|---|---|---|---|---|---|---|
| Headache (n (%)) | 32 (82) | 0 (0) | NT | 5 (26) | 23 (92) | <0.001 |
| IBS * (n (%)) | 9 (24) * | 0 (0) | NT | 5 (26) | 9 (38) | 0.741 |
| GCPS interference | NT | 1.000 | ||||
| Grade I-II | 30 (77) | 0 (0) | 11 (78) | 19 (76) | ||
| Grade III-IV | 9 (23) | 0 (0) | 3 (22) | 6 (24) | ||
| CPI (0–100) | 60.0 (20.0) | 0 (0) | <0.001 | 53.3 (18.3) | 63.3 (16.7) | 0.151 |
| MUO pain-free (mm) | 40.6 (9.9) | 56.3 (6.2) | <0.001 | 44.1 (11.0) | 38.7 (8.8) | |
| MUO with pain (mm) | 52.5 (6.4) | 57.7 (6.1) | <0.001 | 54.8 (7.6) | 51.2 (5.4) | |
| PPT (kPa) | ||||||
| Masseter | 180 (56) | 268 (72) | <0.001 | 227 (50) | 157 (45) | 0.001 |
| Thumb | 356 (121) | 439 (119) | 0.020 | 415 (136) | 328 (105) | 0.076 |
| Diagnoses (n (%)) | ||||||
| Arthralgia | 26 (67) | 0 | NT | 7 (50) | 19 (76) | 0.157 |
| HA-TMD | 28 (72) | 0 | NT | 5 (36) | 21 (84) | 0.004 |
| DDwR | 10 (26) | 2 (5) | 0.032 | 4 (29) | 6 (24) | 1.000 |
| DJD | 1 (3) | 1 (3) | NT | 1 (7) | 0 | NT |
| Protein Marker | VIP | p(corr) | TMDM n = 39 | CON n = 38 |
|---|---|---|---|---|
| IL-7 | 1.48 | 0.69 | 2.96 (1.93) | 1.78 (1.26) |
| GRO-alpha | 1.47 | 0.69 | 151.01 (127.82) | 98.97 (64.64) |
| BDNF | 1.46 | 0.68 | 263.33 (245.13) | 151.81 (125.90) |
| ENA-78 | 1.41 | 0.66 | 347.47 (288.73) | 214.51 (142.37) |
| TPO | 1.17 | 0.55 | 549.62 (135.06) | 529.32 (71.63) |
| IL-1ra | 1.10 | 0.51 | 197.28 (66.47) | 174.13 (48.12) |
| IL-6 | 1.10 | 0.51 | 0.89 (0.82) | 0.54 (0.28) |
| YKL-40 | 1.06 | 0.50 | 22,016.97 (5599.54) | 19,092.95 (5432.94) |
| Leptin | 1.04 | 0.48 | 61,085.78 (56,801.28) | 29,440.17 (28,577.29) |
| Protein Marker | VIP | p(corr) | MYA n = 14 | MFP n = 25 |
|---|---|---|---|---|
| TARC | 1.79 | 0.72 | 71.13 (34.04) | 42.87 (15.36) |
| MCP-4 | 1.65 | 0.66 | 64.07 (28.72) | 46.36 (21.27) |
| GRO-alpha | 1.59 | 0.63 | 225.42 (164.96) | 112.19 (93.86) |
| BDNF | 1.50 | 0.60 | 373.09 (300.70) | 206.06 (194.04) |
| IL-7 | 1.49 | 0.60 | 3.82 (2.52) | 2.52 (1.41) |
| GLP-1 (total) | 1.32 | −0.53 | 13.50 (4.29) | 17.32 (6.81) |
| Ghrelin (active) | 1.29 | −0.52 | 114.14 (55.92) | 206.54 (131.85) |
| IP-10 | 1.26 | 0.50 | 325.89 (126.79) | 265.16 (86.13) |
| Eotaxin-3 | 1.15 | 0.47 | 6.68 (1.58) | 5.69 (2.77) |
| Eotaxin | 1.09 | 0.44 | 129.87 (41.50) | 115.92 (34.31) |
| IL-5 | 1.04 | 0.42 | 0.52 (0.49) | 0.35 (0.44) |
| MCP-2 | 1.01 | 0.40 | 26.91 (4.01) | 24.60 (5.82) |
| Protein Marker | VIP | p(corr) | Model Statistics | |
|---|---|---|---|---|
| OPLS Pain duration | ||||
| G-CSF | 1.85 | 0.65 | Principle component | 1 |
| IL-6 | 1.73 | 0.61 | Orthogonal component | 0 |
| IL-29/IFN-L1 * | 1.61 | −0.56 | CV-ANOVA p-value | 0.0085 |
| IL-21 | 1.61 | −0.56 | R2 | 0.51 |
| IL-17A | 1.49 | 0.52 | Q2 | 0.26 |
| IL-16 | 1.31 | 0.46 | ||
| GM-CSF | 1.09 | −0.39 | ||
| MCP-1 | 1.08 | 0.38 | ||
| M-CSF | 1.02 | 0.36 | ||
| OPLS characteristics pain intensity (CPI) | ||||
| IL-4 | 2.10 | 0.70 | Principle component | 1 |
| FLT3L | 1.66 | −0.50 | Orthogonal component | 1 |
| TPO | 1.54 | −0.46 | CV-ANOVA p-value | 0.0007 |
| CTACK | 1.47 | −0.44 | R2 | 0.73 |
| TSLP | 1.41 | 0.41 | Q2 | 0.49 |
| IL-1RA | 1.26 | 0.36 | ||
| IL-29/IFN-L1 * | 1.23 | −0.41 | ||
| IL-12p70* | 1.22 | 0.36 | ||
| GRO-alpha * | 1.16 | −0.34 | ||
| IL-22 | 1.13 | 0.34 | ||
| IL-15 | 1.00 | −0.30 | ||
| OPLS Pain catastrophizing (PCS) | ||||
| BDNF | 1.67 | 0.80 | Principle component | 1 |
| ENA-78 * | 1.59 | 0.75 | Orthogonal component | 0 |
| GRO-alpha * | 1.59 | 0.75 | CV-ANOVA p-value | 0.0267 |
| IL-7 | 1.52 | 0.72 | R2 | 0.37 |
| VEGF-A | 1.28 | 0.61 | Q2 | 0.20 |
| IL-12p70 * | 1.21 | 0.58 | ||
| TNF-α | 1.21 | 0.57 | ||
| IL-8 | 1.06 | 0.50 | ||
| OPLS Perceived stress (PSS) | ||||
| PYY | 1.82 | 0.62 | Principle component | 1 |
| I-309 * | 1.78 | −0.60 | Orthogonal component | 0 |
| IL-27 | 1.61 | −0.55 | CV-ANOVA p-value | 0.0225 |
| GLP-1 (total) | 1.58 | 0.54 | R2 | 0.48 |
| ENA-78 * | 1.32 | 0.45 | Q2 | 0.22 |
| Eotaxin-3 | 1.22 | −0.41 | ||
| IL-17D | 1.19 | −0.41 | ||
| Proinsulin * | 1.17 | −0.40 | ||
| GLP-1 (inactive) | 1.13 | 0.38 | ||
| IFN-γ | 1.08 | −0.37 | ||
| Ghrelin (active) | 1.06 | 0.36 | ||
| IP-10 | 1.04 | −0.36 | ||
| Ghrelin (total) | 1.01 | 0.35 | ||
| OPLS Insomnia severity (ISI) | ||||
| BAFF | 1.85 | −0.68 | Principle component | 1 |
| Proinsulin * | 1.84 | −0.68 | Orthogonal component | 0 |
| GIP (Inactive) | 1.53 | −0.57 | CV-ANOVA p-value | 0.0032 |
| Total GIP | 1.51 | −0.56 | R2 | 0.57 |
| Insulin | 1.47 | −0.54 | Q2 | 0.31 |
| C-peptide | 1.34 | −0.49 | ||
| I-309 * | 1.31 | −0.49 | ||
| GIP (active) | 1.26 | −0.46 | ||
| IL-1α | 1.10 | 0.41 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ernberg, M.; Jasim, H.; Wåhlén, K.; Ghafouri, B. Altered Plasma Proteins in Myogenous Temporomandibular Disorders. J. Clin. Med. 2022, 11, 2777. https://doi.org/10.3390/jcm11102777
Ernberg M, Jasim H, Wåhlén K, Ghafouri B. Altered Plasma Proteins in Myogenous Temporomandibular Disorders. Journal of Clinical Medicine. 2022; 11(10):2777. https://doi.org/10.3390/jcm11102777
Chicago/Turabian StyleErnberg, Malin, Hajer Jasim, Karin Wåhlén, and Bijar Ghafouri. 2022. "Altered Plasma Proteins in Myogenous Temporomandibular Disorders" Journal of Clinical Medicine 11, no. 10: 2777. https://doi.org/10.3390/jcm11102777
APA StyleErnberg, M., Jasim, H., Wåhlén, K., & Ghafouri, B. (2022). Altered Plasma Proteins in Myogenous Temporomandibular Disorders. Journal of Clinical Medicine, 11(10), 2777. https://doi.org/10.3390/jcm11102777