
Ultrasound-Guided Femoral Nerve Block in Geriatric Patients with Hip Fracture in the Emergency Department

 , , , ,
, , , , 
Abstract
1. Introduction
1.1. Importance
1.2. Goals of This Investigation
2. Materials and Methods
2.1. Study Design and Protocol
2.2. Study Population and Setting
2.3. Interventions
2.4. Measurements
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study Participants
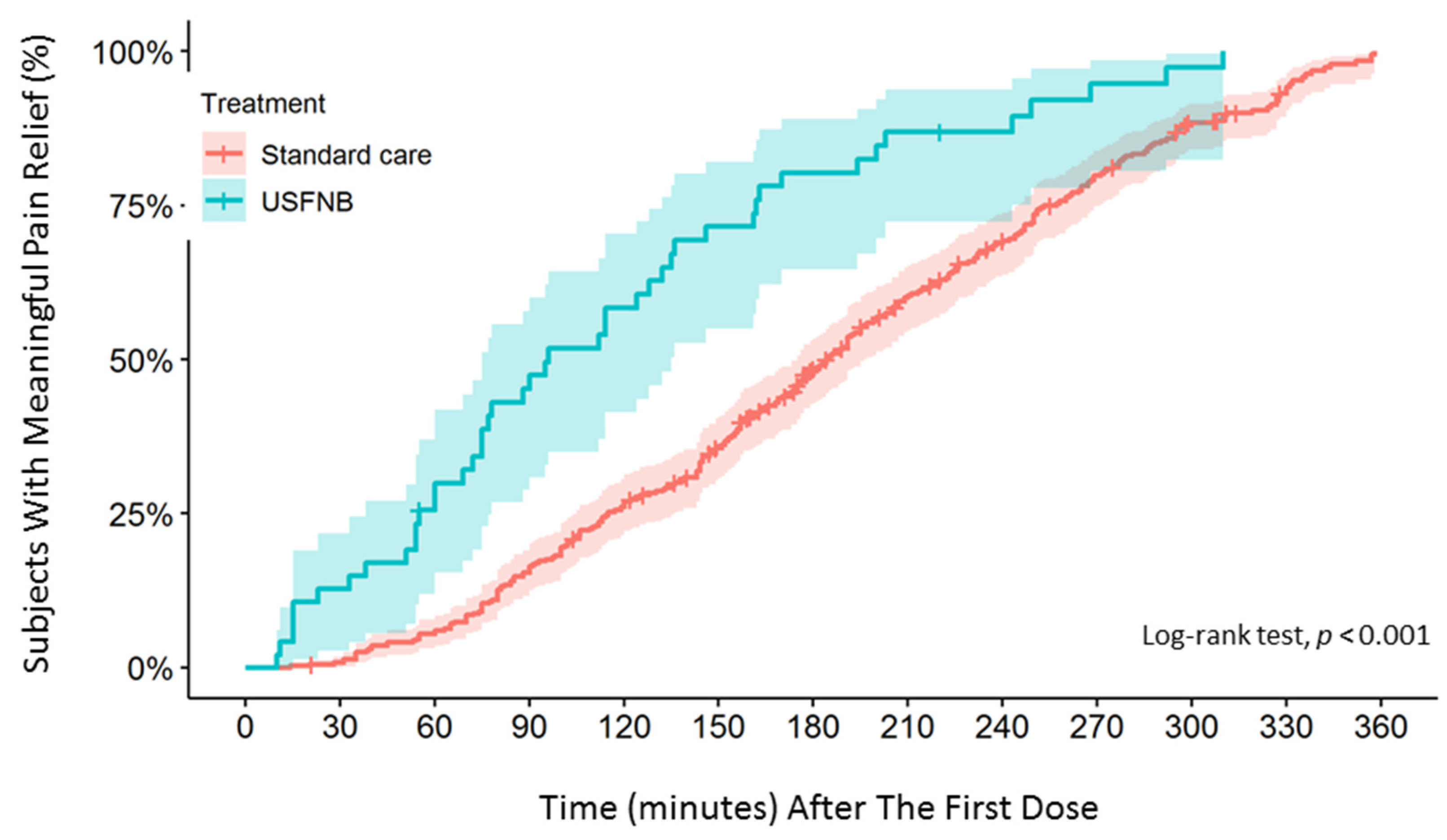
3.2. Main Results
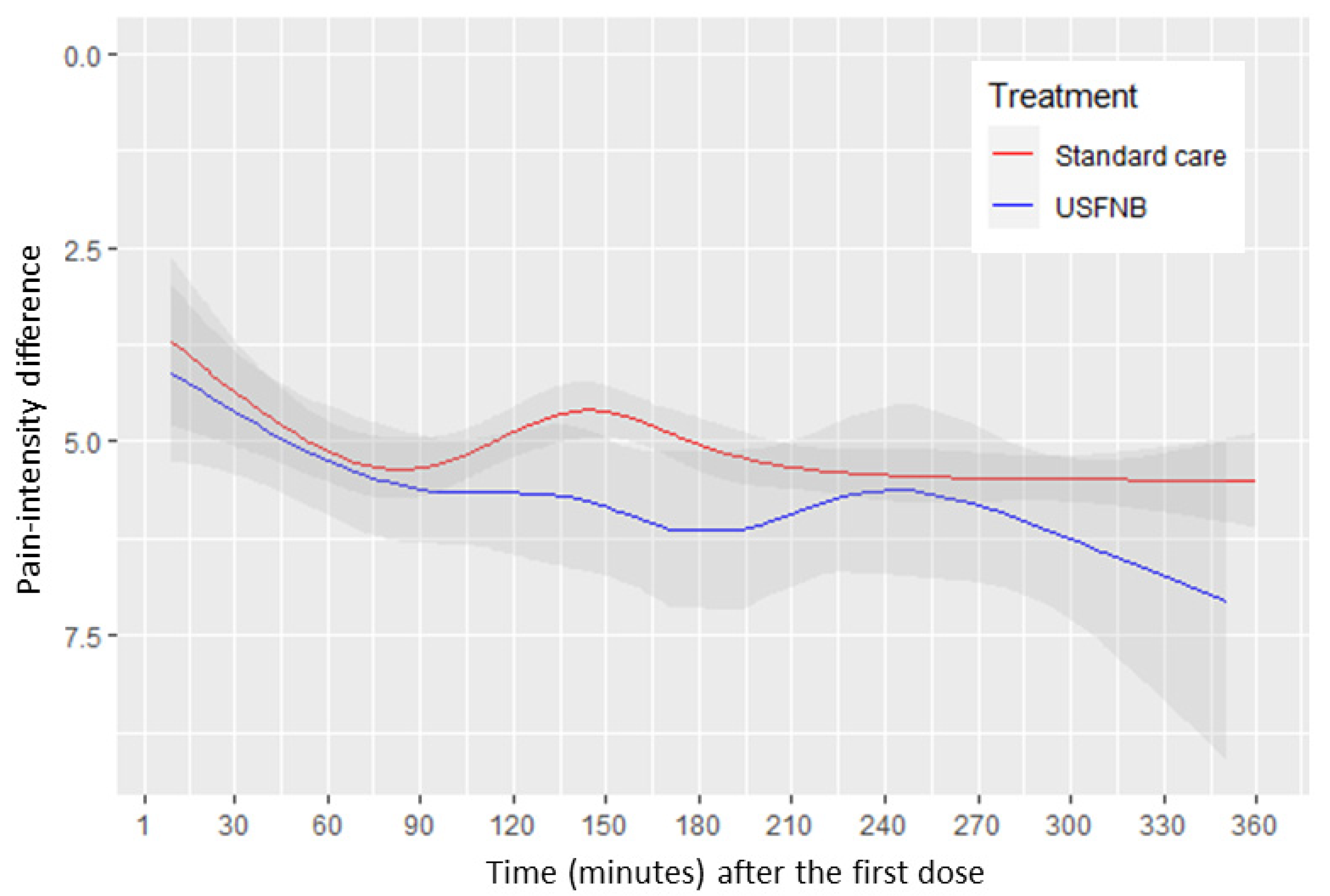
3.3. Comparison of Pain Scores between the USFNB and Standard Care Groups
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- White, S.M.; Griffiths, R. Projected incidence of proximal femoral fracture in England: A report from the NHS Hip Fracture Anaesthesia Network (HIPFAN). Injury 2011, 42, 1230–1233. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.-K.; Chen, Y.H.; Chen, H.-H.; Tsai, K.-W. A Study for the Elder Falls. Taiwan Geriatr. Gerontol. 2006, 1, 174–181. [Google Scholar] [CrossRef]
- Lin, S.-I. Risk of Falls in Community-dwelling Older Adults: A Review of Evidence and Taiwan Experiences. Taiwan Geriatr. Gerontol. 2013, 8, 239–251. [Google Scholar] [CrossRef]
- Lin, S.-M.; Yang, S.-H.; Cheng, H.-Y.; Liang, C.-C.; Huang, H.-K. Thiazide diuretics and the risk of hip fracture after stroke: A population-based propensity-matched cohort study using Taiwan’s National Health Insurance Research Database. BMJ Open 2017, 7, e016992. [Google Scholar] [CrossRef]
- Pei-Ju Huang, S.-H.L. Case-Control Study of Risk Factors for Hip fracture in the elderly. J. Nurs. 2012, 59, 10. [Google Scholar]
- Abou-Setta, A.M.; Beaupre, L.A.; Rashiq, S.; Dryden, D.M.; Hamm, M.P.; Sadowski, C.A.; Menon, M.R.; Majumdar, S.R.; Wilson, D.M.; Karkhaneh, M.; et al. Comparative effectiveness of pain management interventions for hip fracture: A systematic review. Ann. Intern. Med. 2011, 155, 234–245. [Google Scholar] [CrossRef]
- Morrison, S.R.; Magaziner, J.; McLaughlin, M.A.; Orosz, G.; Silberzweig, S.B.; Koval, K.J.; Siu, A.L. The impact of post-operative pain on outcomes following hip fracture. Pain 2003, 103, 303–311. [Google Scholar] [CrossRef]
- Harirforoosh, S.; Asghar, W.; Jamali, F. Adverse effects of nonsteroidal antiinflammatory drugs: An update of gastrointestinal, cardiovascular and renal complications. J. Pharm. Pharm. Sci. 2013, 16, 821–847. [Google Scholar] [CrossRef]
- Barnett, M.L.; Olenski, A.R.; Jena, A.B. Opioid-Prescribing Patterns of Emergency Physicians and Risk of Long-Term Use. N. Eng. J. Med. 2017, 376, 663–673. [Google Scholar] [CrossRef]
- Hilliard, P.E.; Waljee, J.; Moser, S.; Metz, L.; Mathis, M.; Goesling, J.; Cron, D.; Clauw, D.J.; Englesbe, M.; Abecasis, G.; et al. Prevalence of Preoperative Opioid Use and Characteristics Associated with Opioid Use Among Patients Presenting for Surgery. JAMA Surg. 2018, 153, 929–937. [Google Scholar] [CrossRef]
- 2019 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr Soc. 2019, 67, 674–694. [Google Scholar] [CrossRef] [PubMed]
- Scurrah, A.; Shiner, C.T.; Stevens, J.A.; Faux, S.G. Regional nerve blockade for early analgesic management of elderly patients with hip fracture—A narrative review. Anaesthesia 2018, 73, 769–783. [Google Scholar] [CrossRef] [PubMed]
- McRae, P.J.; Bendall, J.C.; Madigan, V.; Middleton, P.M. Paramedic-performed Fascia Iliaca Compartment Block for Femoral Fractures: A Controlled Trial. J. Emerg Med. 2015, 48, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Beaudoin, F.L.; Haran, J.P.; Liebmann, O. A Comparison of Ultrasound-guided Three-in-one Femoral Nerve Block Versus Parenteral Opioids Alone for Analgesia in Emergency Department Patients with Hip Fractures: A Randomized Controlled Trial. Acad. Emerg. Med. 2013, 20, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, A.K.; Rigby, A.S.; Heyes, F.L. Three-in-one femoral nerve block as analgesia for fractured neck of femur in the emergency department: A randomized, controlled trial. Ann. Emerg Med. 2003, 41, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Unneby, A.; Svensson, O.; Gustafson, Y.; Olofsson, B. Femoral nerve block in a representative sample of elderly people with hip fracture: A randomised controlled trial. Injury 2017, 48, 1542–1549. [Google Scholar] [CrossRef] [PubMed]
- Skjold, C.; Møller, A.M.; Wildgaard, K. Pre-operative femoral nerve block for hip fracture—A systematic review with meta-analysis. Acta Anaesthesiol. Scand. 2020, 64, 23–33. [Google Scholar] [CrossRef]
- Worster, A.; Bledsoe, R.D.; Cleve, P.; Fernandes, C.M.; Upadhye, S.; Eva, K. Reassessing the methods of medical record review studies in emergency medicine research. Ann. Emerg. Med. 2005, 45, 448–451. [Google Scholar] [CrossRef]
- Taha, A.M.; Abd-Elmaksoud, A.M. Lidocaine use in ultrasound-guided femoral nerve block: What is the minimum effective anaesthetic concentration (MEAC90)? Br. J. Anaesth 2013, 110, 1040–1044. [Google Scholar] [CrossRef]
- Farrar, J.T.; Berlin, J.A.; Strom, B.L. Clinically Important Changes in Acute Pain Outcome Measures: A Validation Study. J. Pain Symptom Manag. 2003, 25, 406–411. [Google Scholar] [CrossRef]
- Harrell, F.E. (Ed.) Regression Modeling Strategies: With Applications to Linear Models, Logistic Regression, and Survival Analysis; Springer New York, Inc.: New York, NY, USA, 2015. [Google Scholar]
- Young, B.T.; Zolin, S.J.; Ferre, A.; Ho, V.P.; Harvey, A.R.; Beel, K.T.; Tseng, E.S.; Conrad-Schnetz, K.; Claridge, J.A. Effects of Ohio’s opioid prescribing limit for the geriatric minimally injured trauma patient. Am. J. Surg. 2020, 219, 400–403. [Google Scholar] [CrossRef]
- Santosa, K.B.; Lai, Y.-L.; Oliver, J.D.; Hu, H.-M.; Brummett, C.M.; Englesbe, M.J.; Waljee, J.F. Preoperative Opioid Use and Mortality After Minor Outpatient Surgery. JAMA Surg. 2020, 155, 1169–1171. [Google Scholar] [CrossRef] [PubMed]
- Tang, R.; Santosa, K.B.; Vu, J.V.; Lin, L.A.; Lai, Y.-L.; Englesbe, M.J.; Brummett, C.M.; Waljee, J.F. Preoperative Opioid Use and Readmissions Following Surgery. Anna. Surg. 2022, 275, e99–e106. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.-H.; Ho, S.-T.; Lu, C.-C.; Wang, J.-O.; Lin, T.-C.; Wang, K.-Y. Trends in the Consumption of Opioid Analgesics in Taiwan from 2002 to 2007: A Population-Based Study. J. Pain Symptom Manag. 2012, 45, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.V.; Stucke, R.S.; McMahon, M.L.; Beeman, J.L.; Barth, R.J., Jr. An Educational Intervention Decreases Opioid Prescribing After General Surgical Operations. Ann. Surg 2018, 267, 468–472. [Google Scholar] [CrossRef]
- Duncan, R.W.; Smith, K.L.; Maguire, M.; Stader, D.E., 3rd. Alternatives to opioids for pain management in the emergency department decreases opioid usage and maintains patient satisfaction. Am. J. Emerg Med. 2019, 37, 38–44. [Google Scholar] [CrossRef]
- Riddell, M.; Ospina, M.; Holroyd-Leduc, J.M. Use of Femoral Nerve Blocks to Manage Hip Fracture Pain among Older Adults in the Emergency Department: A Systematic Review. Cjem 2016, 18, 245–252. [Google Scholar] [CrossRef]
- Vinycomb, T.I.; Sahhar, L.J. Comparison of local anesthetics for digital nerve blocks: A systematic review. J. Hand Surg. Am. 2014, 39, 744–751.e5. [Google Scholar] [CrossRef]
- Forouzan, A.; Masoumi, K.; Yadegar, N.; Rahim, F.; Feli, M.; Darian, A. Comparison of Femoral Nerve Block with Intravenous Morphine Sulfate for Pain Relief of Femoral Fracture. Asian J. Sci. Res. 2015, 8, 429–435. [Google Scholar] [CrossRef][Green Version]
- Hopkins, P.M. Ultrasound guidance as a gold standard in regional anaesthesia. Br. J. Anaesth. 2007, 98, 299–301. [Google Scholar] [CrossRef]
- Olsen, M.F.; Bjerre, E.; Hansen, M.D.; Hilden, J.; Landler, N.E.; Tendal, B.; Hróbjartsson, A. Pain relief that matters to patients: Systematic review of empirical studies assessing the minimum clinically important difference in acute pain. BMC Med. 2017, 15, 35. [Google Scholar] [CrossRef] [PubMed]
- Guay, J.; Kopp, S. Peripheral nerve blocks for hip fractures in adults. Cochrane Database Syst. Rev. 2020, CD001159. [Google Scholar] [CrossRef]
- Carli, F.; Kehlet, H.; Baldini, G.; Steel, A.; McRae, K.; Slinger, P.; Hemmerling, T.; Salinas, F.; Neal, J.M. Evidence basis for regional anesthesia in multidisciplinary fast-track surgical care pathways. Reg. Anesth. Pain Med. 2011, 36, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.-Y.; Morrison, C.; Brown, B.; Saies, A.A.; Pawar, R.; Vermeulen, M.; Anderson, S.R.; Lee, T.S.; Doornberg, J.; Kroon, H.M.; et al. Pericapsular nerve group (PENG) block provides improved short-term analgesia compared with the femoral nerve block in hip fracture surgery: A single-center double-blinded randomized comparative trial. Reg. Anesth. Pain Med. 2021, 46, 398–403. [Google Scholar] [CrossRef]
- Thongkhamcharoen, R.; Phungrassami, T.; Atthakul, N. Regulation of Opioid Drugs in Thai Government Hospitals: Thailand National Survey 2012. Indian J. Palliat. Care 2014, 20, 6–11. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | USFNB (n = 66) | Standard Care (n = 541) | p-Value |
|---|---|---|---|
| Mean (SD) age (years) | 80.30 (8.62) | 79.69 (8.33) | 0.579 |
| Women, % (n) | 66.67 (44) | 65.99 (357) | 0.913 |
| Mean (SD) BMI | 22.84 (4.49) | 23.00 (4.20) | 0.784 |
| Fracture type | 0.160 | ||
| Extracapsular, % (n) | 63.64 (42) | 54.53 (295) | |
| Intracapsular, % (n) | 36.36 (24) | 45.47 (246) | |
| Mean (SD) of initial pain score | 7.86 (0.99) | 7.36 (1.60) | 0.013 |
| Triage *, % | 0.845 | ||
| Emergent | 28.79 | 27.73 | |
| Urgent | 71.21 | 72.27 | |
| Arrival (sent by EMT), % | 46.97 | 38.45 | 0.181 |
| Comorbidity | |||
| DM, % | 30.30 | 32.35 | 0.737 |
| Hypertension, % | 66.67 | 59.89 | 0.287 |
| Cardiovascular disease, % | 21.21 | 20.70 | 0.923 |
| CKD, % | 15.15 | 10.54 | 0.259 |
| Liver disease, % | 7.58 | 7.95 | 0.916 |
| Surgical history, % | 25.76 | 23.29 | 0.656 |
| Chronic arthritis, % | 13.64 | 6.10 | 0.023 |
| Malignancy, % | 13.64 | 8.69 | 0.190 |
| Mean (SD) of CCIS | 1.41 (1.26) | 1.26 (1.33) | 0.380 |
| Chronic opioid users, % | 6.06 | 5.91 | 0.962 |
| Mortality, % | 6.06 | 2.59 | 0.116 |
| Morphine Milligram Equivalents (mg) | Duration of ED Stay (Hours) | Duration of Hospital Stay (Days) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No | Unadjusted Mean | Adjusted Difference | p-Value | Unadjusted Mean | Adjusted Difference | p-Value | Unadjusted Mean | Adjusted Difference | p-Value | |
| USFNB | 66 | 0.52 ± 1.47 | −2.11 ± 0.32 † | <0.001 | 7.01 ± 6.49 | 0.93 ± 0.73 † | 0.203 | 7.98 ± 3.91 | −1.17 ± 0.91 † | 0.199 |
| Standard care | 541 | 2.57 ± 2.53 | Reference | 5.83 ± 5.43 | Reference | 9.28 ± 7.05 | Reference | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, T.-Y.; Cheong, K.M.; Su, Y.-C.; Shih, M.-C.; Chau, S.W.; Chen, M.-W.; Chen, C.-T.; Lee, Y.-K.; Sun, J.-T.; Chen, K.-F.; et al. Ultrasound-Guided Femoral Nerve Block in Geriatric Patients with Hip Fracture in the Emergency Department. J. Clin. Med. 2022, 11, 2778. https://doi.org/10.3390/jcm11102778
Tsai T-Y, Cheong KM, Su Y-C, Shih M-C, Chau SW, Chen M-W, Chen C-T, Lee Y-K, Sun J-T, Chen K-F, et al. Ultrasound-Guided Femoral Nerve Block in Geriatric Patients with Hip Fracture in the Emergency Department. Journal of Clinical Medicine. 2022; 11(10):2778. https://doi.org/10.3390/jcm11102778
Chicago/Turabian StyleTsai, Tou-Yuan, Kar Mun Cheong, Yung-Cheng Su, Ming-Chieh Shih, Su Weng Chau, Mei-Wen Chen, Chien-Ting Chen, Yi-Kung Lee, Jen-Tang Sun, Kuan-Fu Chen, and et al. 2022. "Ultrasound-Guided Femoral Nerve Block in Geriatric Patients with Hip Fracture in the Emergency Department" Journal of Clinical Medicine 11, no. 10: 2778. https://doi.org/10.3390/jcm11102778
APA StyleTsai, T.-Y., Cheong, K. M., Su, Y.-C., Shih, M.-C., Chau, S. W., Chen, M.-W., Chen, C.-T., Lee, Y.-K., Sun, J.-T., Chen, K.-F., Chen, K.-C., & Chou, E. H. (2022). Ultrasound-Guided Femoral Nerve Block in Geriatric Patients with Hip Fracture in the Emergency Department. Journal of Clinical Medicine, 11(10), 2778. https://doi.org/10.3390/jcm11102778