
Does Time-to-Chemotherapy after Primary Complete Macroscopic Cytoreductive Surgery Influence Prognosis for Patients with Epithelial Ovarian Cancer? A Study of the FRANCOGYN Group

 ,
,  , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Method
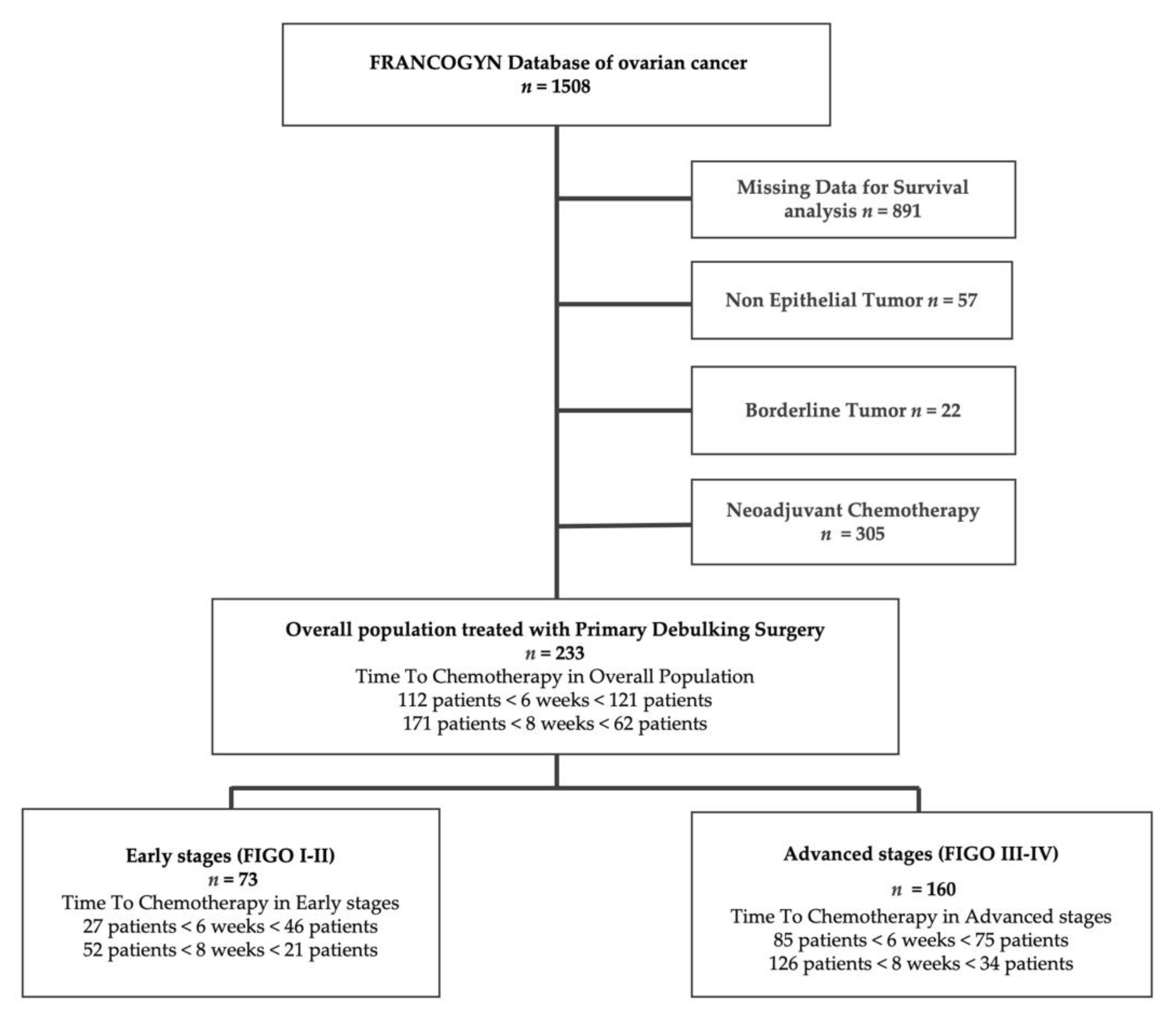
2.1. Study Population
2.2. Endpoints
2.3. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Survival Analysis
3.2.1. Whole Population
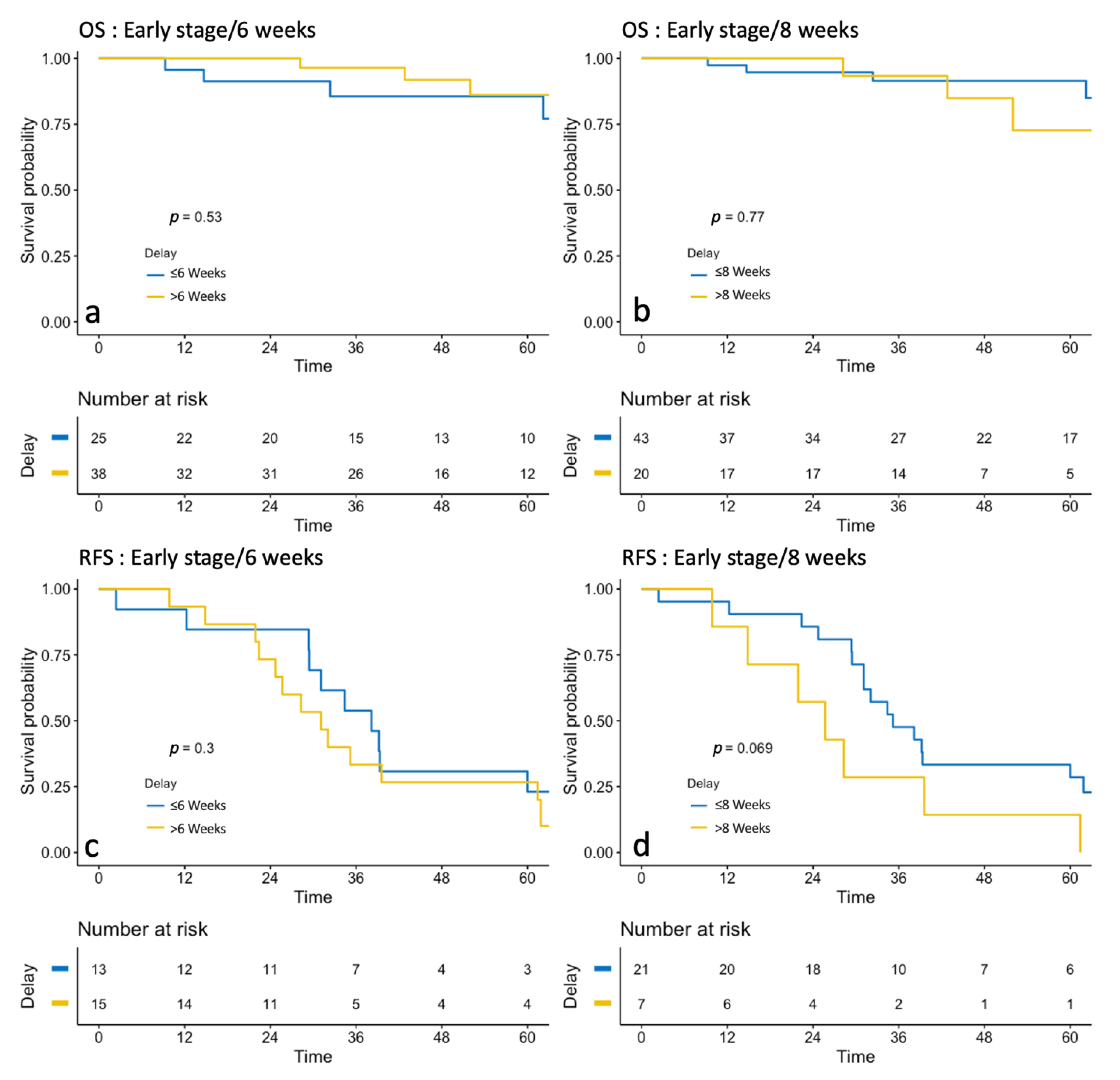
3.2.2. Early-Stage Group
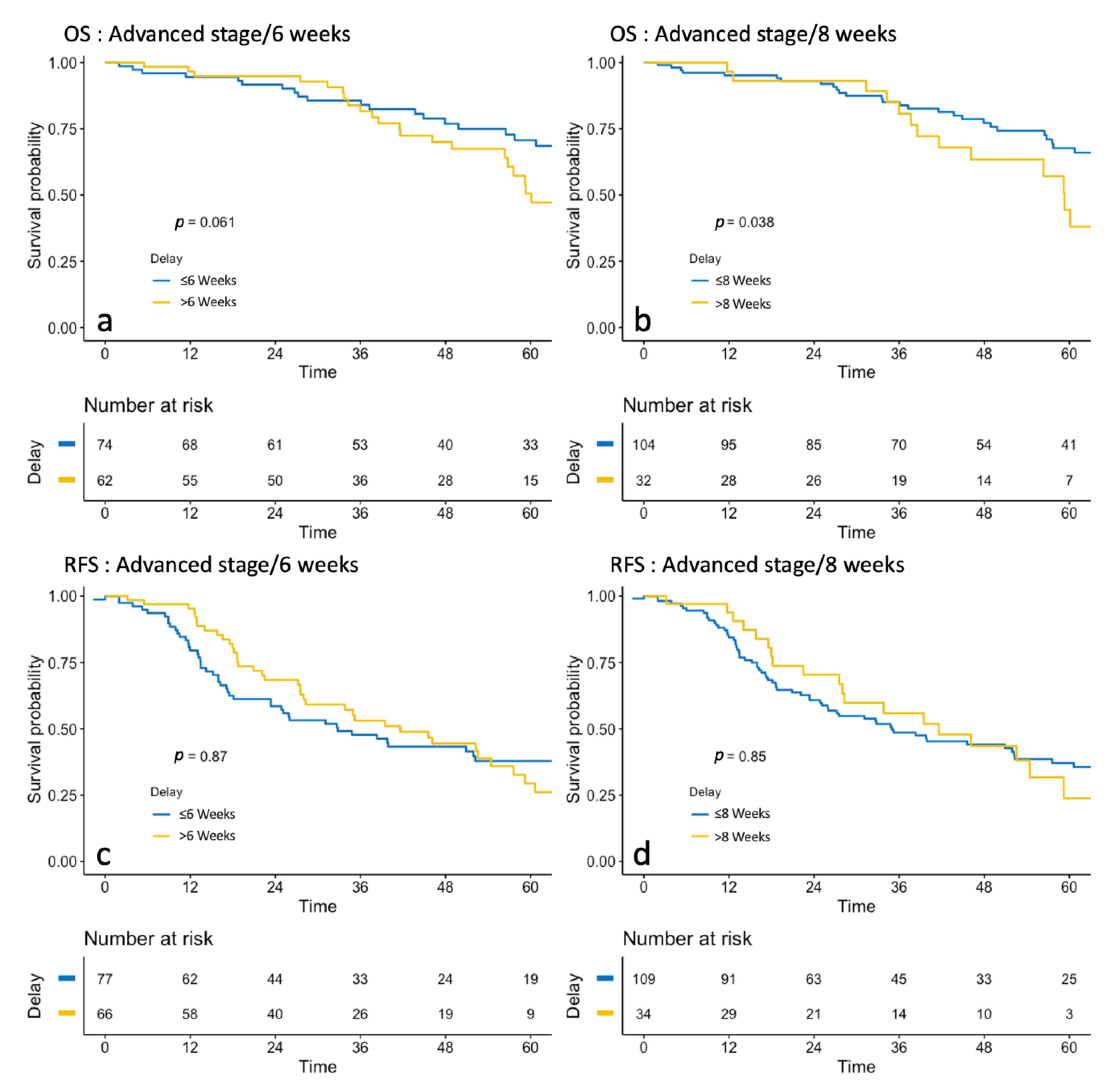
3.2.3. Advanced-Stage Group
3.3. Cox Univariate and Multivariate Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marszalek, A.; Alran, S.; Scholl, S.; Fourchotte, V.; Plancher, C.; Rosty, C.; Meyniel, J.P.; De Margerie, V.; Dorval, T.; De La Rochefordière, A.; et al. Outcome in Advanced Ovarian Cancer following an Appropriate and Comprehensive Effort at Upfront Cytoreduction: A Twenty-Year Experience in a Single Cancer Institute. Int. J. Surg. Oncol. 2010, 2010, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lavoue, V.; Huchon, C.; Akladios, C.; Alfonsi, P.; Bakrin, N.; Ballester, M.; Bendifallah, S.; Bolze, P.; Bonnet, F.; Bourgin, C.; et al. Management of epithelial cancer of the ovary, fallopian tube, and primary peritoneum. Long text of the Joint French Clinical Practice Guidelines issued by FRANCOGYN, CNGOF, SFOG, and GINECO-ARCAGY, and endorsed by INCa. Part 1: Diagnostic exploration and staging, surgery, perioperative care, and pathology. J. Gynecol. Obstet. Hum. Reprod. 2019, 48, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Defossez, G.; Le Guyader-Peyrou, S.; Uhry, Z.; Grosclaude, P.; Remontet, L.; Colonna, M.; Emmanuelle, D.; Patricia, D.; Florence, M.; Anne-Sophie, W.; et al. Estimations Nationales de L’incidence et de la Mortalité par Cancer en France Métropolitaine Entre 1990 et 2018. Etude à Partir des Registres des Cancers du Réseau Francim. Résultats préliminaires. Synthèse; Santé publique France: Saint-Maurice, France, 2019. [Google Scholar]
- Wright, J.D.; Herzog, T.J.; Neugut, A.I.; Burke, W.M.; Lu, Y.-S.; Lewin, S.N.; Hershman, D.L. Effect of Radical Cytoreductive Surgery on Omission and Delay of Chemotherapy for Advanced-Stage Ovarian Cancer. Obstet. Gynecol. 2012, 120, 871–881. [Google Scholar] [CrossRef]
- Castro, B.G.R.; Dos Reis, R.; Cintra, G.F.; Sousa, M.M.D.A.; Vieira, M.D.A.; Andrade, C.E.M.D.C. Predictive Factors for Surgical Morbidities and Adjuvant Chemotherapy Delay for Advanced Ovarian Cancer Patients Treated by Primary Debulking Surgery or Interval Debulking Surgery. Int. J. Gynecol. Cancer 2018, 28, 1520–1528. [Google Scholar] [CrossRef]
- Feng, Z.; Wen, H.; Bi, R.; Yang, W.; Wu, X. Prognostic impact of the time interval from primary surgery to intravenous chemotherapy in high grade serous ovarian cancer. Gynecol. Oncol. 2016, 141, 466–470. [Google Scholar] [CrossRef]
- Cannistra, S.A. Cancer of the Ovary. N. Engl. J. Med. 2004, 351, 2519–2529. [Google Scholar] [CrossRef]
- Griffiths, C.T. Surgical resection of tumor bulk in the primary treatment of ovarian carcinoma. Natl. Cancer Inst. Monogr. 1975, 42, 101–104. [Google Scholar]
- Tewari, K.S.; Java, J.J.; Eskander, R.N.; Monk, B.J.; A Burger, R. Early initiation of chemotherapy following complete resection of advanced ovarian cancer associated with improved survival: NRG Oncology/Gynecologic Oncology Group study. Ann. Oncol. 2016, 27, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Hofstetter, G.; Concin, N.; Braicu, I.; Chekerov, R.; Sehouli, J.; Cadron, I.; Van Gorp, T.; Trillsch, F.; Mahner, S.; Ulmer, H.; et al. The time interval from surgery to start of chemotherapy significantly impacts prognosis in patients with advanced serous ovarian carcinoma—Analysis of patient data in the prospective OVCAD study. Gynecol. Oncol. 2013, 131, 15–20. [Google Scholar] [CrossRef]
- Earle, C.C.; Schrag, D.; Neville, B.A.; Yabroff, K.R.; Topor, M.; Fahey, A.; Trimble, E.L.; Bodurka, D.C.; Bristow, R.E.; Carney, M.; et al. Effect of Surgeon Specialty on Processes of Care and Outcomes for Ovarian Cancer Patients. J. Natl. Cancer Inst. 2006, 98, 172–180. [Google Scholar] [CrossRef]
- Schrag, D.; Earle, C.; Xu, F.; Panageas, K.S.; Yabroff, K.R.; Bristow, R.E.; Trimble, E.L.; Warren, J.L. Associations Between Hospital and Surgeon Procedure Volumes and Patient Outcomes After Ovarian Cancer Resection. J. Natl. Cancer Inst. 2006, 98, 163–171. [Google Scholar] [CrossRef]
- Joseph, N.; Clark, R.M.; Dizon, D.S.; Lee, M.S.; Goodman, A.; Boruta, D.; Schorge, J.O.; Del Carmen, M.G.; Growdon, W.B. Delay in chemotherapy administration impacts survival in elderly patients with epithelial ovarian cancer. Gynecol. Oncol. 2015, 137, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-Y.; Lee, J.-W.; Lu, L.; Xu, W.; Kollara, A.; Brown, T.; Heo, E.-J.; May, T. Impact of interval from primary cytoreductive surgery to initiation of adjuvant chemotherapy in advanced epithelial ovarian cancer. Int. J. Gynecol. Obstet. 2018, 143, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Seagle, B.-L.L.; Butler, S.K.; Strohl, A.E.; Nieves-Neira, W.; Shahabi, S. Chemotherapy delay after primary debulking surgery for ovarian cancer. Gynecol. Oncol. 2017, 144, 260–265. [Google Scholar] [CrossRef]
- Singh, S.; Guetzko, M.; Resnick, K. Preoperative predictors of delay in initiation of adjuvant chemotherapy in patients undergoing primary debulking surgery for ovarian cancer. Gynecol. Oncol. 2016, 143, 241–245. [Google Scholar] [CrossRef]
- E Garcia-Soto, A.; Java, J.J.; Neira, W.N.; Pearson, J.M.; Cohn, D.E.; Lele, S.B.; Tewari, K.S.; Walker, J.L.; Secord, A.A.; Armstrong, D.K.; et al. Does time interval between surgery and intraperitoneal chemotherapy administration in advanced ovarian cancer carry a prognostic impact? An NRG Oncology/Gynecologic Oncology Group study ancillary study. Gynecol. Oncol. 2016, 143, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Mahner, S.; Eulenburg, C.; Staehle, A.; Wegscheider, K.; Reuss, A.; Pujade-Lauraine, E.; Harter, P.; Ray-Coquard, I.; Pfisterer, J.; Du Bois, A. Prognostic impact of the time interval between surgery and chemotherapy in advanced ovarian cancer: Analysis of prospective randomised phase III trials. Eur. J. Cancer 2013, 49, 142–149. [Google Scholar] [CrossRef]
- Prat, J. FIGO Committee on Gynecologic Oncology Staging classification for cancer of the ovary, fallopian tube, and peritoneum. Int. J. Gynecol. Obstet. 2014, 124, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Javadi, S.; Ganeshan, D.M.; Qayyum, A.; Iyer, R.B.; Bhosale, P. Ovarian Cancer, the Revised FIGO Staging System, and the Role of Imaging. Am. J. Roentgenol. 2016, 206, 1351–1360. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.D.; Doan, T.; McBride, R.; Jacobson, J.S.; Hershman, D.L. Variability in chemotherapy delivery for elderly women with advanced stage ovarian cancer and its impact on survival. Br. J. Cancer 2008, 98, 1197–1203. [Google Scholar] [CrossRef]
- Flynn, P.M.; Paul, J.; Cruickshank, D.J. Does the Interval from Primary Surgery to Chemotherapy Influence Progression-Free Survival in Ovarian Cancer? Gynecol. Oncol. 2002, 86, 354–357. [Google Scholar] [CrossRef] [PubMed]
- Usón, P.L.S.; Bugano, D.D.G.; França, M.S.; Antunes, Y.P.P.V.; Taranto, P.; Kaliks, R.A.; Del Giglio, A. Does Time-to-Chemotherapy Impact the Outcomes of Resected Ovarian Cancer? Meta-analysis of Randomized and Observational Data. Int. J. Gynecol. Cancer 2017, 27, 274–280. [Google Scholar] [CrossRef]
- Rosa, D.; Clamp, A.; Mullamitha, S.; Ton, N.; Lau, S.; Byrd, L.; Clayton, R.; Slade, R.; Kitchener, H.; Shanks, J.; et al. The interval from surgery to chemotherapy in the treatment of advanced epithelial ovarian carcinoma. Eur. J. Surg. Oncol. (EJSO) 2006, 32, 588–591. [Google Scholar] [CrossRef]
- Moore, K.; Colombo, N.; Scambia, G.; Kim, B.-G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.S.; et al. Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2018, 379, 2495–2505. [Google Scholar] [CrossRef]
- Ray-Coquard, I.; Pautier, P.; Pignata, S.; Pérol, D.; González-Martín, A.; Berger, R.; Fujiwara, K.; Vergote, I.; Colombo, N.; Mäenpää, J.; et al. Olaparib plus Bevacizumab as First-Line Maintenance in Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2416–2428. [Google Scholar] [CrossRef] [PubMed]
- Harter, P.; Sehouli, J.; Lorusso, D.; Reuss, A.; Vergote, I.; Marth, C.; Kim, J.W.; Raspagliesi, F.; Lampe, B.; Landoni, F.; et al. LION: Lymphadenectomy in ovarian neoplasms—A prospective randomized AGO study group led gynecologic cancer intergroup trial. J. Clin. Oncol. 2017, 35, 5500. [Google Scholar] [CrossRef]
- Quality Indicators. Society of Gynecologic Oncology. Available online: https://omssgo.wpengine.com/resources/quality-indicators/ (accessed on 15 February 2021).
- Querleu, D.; Planchamp, F.; Chiva, L.; Fotopoulou, C.; Barton, D.; Cibula, D.; Aletti, G.; Carinelli, S.; Creutzberg, C.; Davidson, B.; et al. European Society of Gynaecologic Oncology Quality Indicators for Advanced Ovarian Cancer Surgery. Int. J. Gynecol. Cancer 2016, 26, 1354–1363. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | ≤6 Weeks | >6 Weeks | p | ||
|---|---|---|---|---|---|
| n = 233 | n = 116 | n = 117 | |||
| Age (years) | 59 (±12) | 58 (±12) | 60 (±12) | 0.41 | |
| BMI (kg/m2) | 24.58 (±4.88) | 24.09 (±4.79) | 25.08 (±4.94) | 0.13 | |
| Parity | 1.64 (±1.42) | 1.798 (±1.52) | 1.482 (±1.3) | 0.1 | |
| Mutation | BRCA 1 | 12 (5.1%) | 8 (6.8%) | 13 (11.1%) | 0.14 |
| BRCA 2 | 5 (2.1%) | 1 (3.4%) | 0 | ||
| Hypertension | 42 (24.6%) | 20 (22.5%) | 22 (26.8%) | 0.51 | |
| Diabetes | 10 (6.2%) | 6 (7.1%) | 4 (5.2%) | 0.85 | |
| Smoking | 12 (8.5%) | 5 (6.8%) | 7 (10.1%) | 0.48 | |
| Histologic type | Serous | 155 (70.1%) | 77 (74.5%) | 80 (66.1%) | 0.71 |
| Endometrioid | 37 (16.7%) | 15 (14.2%) | 22 (19.1%) | ||
| Clear Cell | 23 (10.4%) | 10 (9.7%) | 13 (10.7%) | ||
| Mucinous | 6 (2.7%) | 2 (1.9%) | 4 (3.3%) | ||
| Grade | 1 | 21 (67.7%) | 9 (75%) | 12 (63.2%) | 0.23 |
| 2 | 7 (22.6%) | 1 (8.3%) | 6 (31.6%) | ||
| 3 | 3 (9.7%) | 2 (16.7%) | 1 (5.3%) | ||
| Lymphovascular space involvement | Yes | 35 (43.8%) | 22 (46.8%) | 13 (39.4%) | 0.51 |
| Stage | Early | 69 (29.6%) | 89 (76.7%) | 75 (64.1%) | 0.035 |
| Advanced | 164 (70.4%) | 27 (23.3%) | 42 (35.9%) | ||
| FIGO Stage | I | 56 (24%) | 18 (15.5%) | 38 (32.5%) | 0.0092 |
| II | 17 (7.2%) | 11 (9.5%) | 6 (5.1%) | ||
| III | 141 (60.5%) | 74 (63.8%) | 67 (57.3%) | ||
| IV | 19 (8.1%) | 13 (11.2%) | 6 (5.1%) | ||
| Type of recurrence | Lymph node | 16 (16.7%) | 9 (17%) | 7 (16.3%) | 0.22 |
| Peritoneal Carcinomatosis | 63 (65.6%) | 37 (69.8%) | 26 (60.5%) | ||
| Metastasis | 9 (9.4%) | 2 (3.8%) | 7 (16.3%) |
| Variables | ≤8 weeks | >8 weeks | p | ||
|---|---|---|---|---|---|
| n = 233 | n = 175 | n = 58 | |||
| Age (years) | 59 (±12) | 58 (±12) | 60 (±12) | 0.41 | |
| BMI (kg/m2) | 24.58 (±4.88) | 24.51 (±4.74) | 24.79 (±5.34) | 0.72 | |
| Parity | 1.64 (±1.42) | 1.758 (±1.48) | 1.278 (±1.17) | 0.031 | |
| Mutation | BRCA 1 | 12 (5.1%) | 17 (9.7%) | 4 (2.8%) | 0.8 |
| BRCA 2 | 5 (2.1%) | 1 (0.6%) | 0 | ||
| Hypertension | 42 (24.6%) | 32 (25%) | 10 (23.3%) | 0.82 | |
| Diabetes | 10 (6.2%) | 8 (6.7%) | 2 (4.8%) | 1 | |
| Smoking | 12 (8.5%) | 8 (7.6%) | 4 (10.8%) | 0.8 | |
| Histologic type | Serous | 155 (70.1%) | 116 (70.7%) | 39 (68.4%) | 0.94 |
| Endometrioid | 37 (16.7%) | 27 (16.5%) | 10 (17.5%) | ||
| Clear Cell | 23 (10.4%) | 17 (10.4%) | 6 (10.5%) | ||
| Mucinous | 6 (2.7%) | 4 (2.4%) | 2 (3.5%) | ||
| Grade | 1 | 21 (67.7%) | 16 (72.7%) | 5 (55.6%) | |
| 2 | 7 (22.6%) | 4 (18.2%) | 3 (33.3%) | ||
| 3 | 3 (9.7%) | 2 (9.1%) | 1 (11.1%) | ||
| Lymphovascular space involvement | Yes | 35 (43.8%) | 27 (45.8%) | 8 (38.1%) | 0.54 |
| Stage | Early | 69 (29.6%) | 127 (72.6%) | 37 (63.8%) | 0.2 |
| Advanced | 164 (70.4%) | 48 (27.4%) | 21 (36.2%) | ||
| FIGO Stage | I | 56 (24%) | 36 (20.6%) | 20 (34.5%) | 0.068 |
| II | 17 (7.2%) | 16 (9.1%) | 1 (1.7%) | ||
| III | 141 (60.5%) | 108 (61.7%) | 33 (56.9%) | ||
| IV | 19 (8.1%) | 15 (8.6%) | 4 (6.9%) | ||
| Type of recurrence | Lymph node | 16 (16.7%) | 12 (16.2%) | 4 (18.2%) | 0.84 |
| Peritoneal Carcinomatosis | 63 (65.6%) | 47 (63.5%) | 16 (72.7%) | ||
| Metastasis | 9 (9.4%) | 8 (10.8%) | 1 (4.5%) |
| Overall Survival. Median, Months | |||
|---|---|---|---|
| Time to Chemotherapy | TTC < 6 weeks | TTC > 6 Weeks | p |
| Whole population | 78.5 | 66.8 | 0.3 |
| Early-stage group | NA | NA | |
| Advanced-stage group | 77.2 | 60.1 | 0.06 |
| Time to Chemotherapy | TTC < 8 weeks | TTC > 8 weeks | |
| Whole population | 78.5 | 60.1 | 0.08 |
| Early-stage group | NA | NA | |
| Advanced-stage group | 70.5 | 59.3 | 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rocher, G.; Gaillard, T.; Uzan, C.; Collinet, P.; Bolze, P.-A.; Ballester, M.; Bendifallah, S.; Ouldamer, L.; Touboul, C.; Huchon, C.; et al. Does Time-to-Chemotherapy after Primary Complete Macroscopic Cytoreductive Surgery Influence Prognosis for Patients with Epithelial Ovarian Cancer? A Study of the FRANCOGYN Group. J. Clin. Med. 2021, 10, 1058. https://doi.org/10.3390/jcm10051058
Rocher G, Gaillard T, Uzan C, Collinet P, Bolze P-A, Ballester M, Bendifallah S, Ouldamer L, Touboul C, Huchon C, et al. Does Time-to-Chemotherapy after Primary Complete Macroscopic Cytoreductive Surgery Influence Prognosis for Patients with Epithelial Ovarian Cancer? A Study of the FRANCOGYN Group. Journal of Clinical Medicine. 2021; 10(5):1058. https://doi.org/10.3390/jcm10051058
Chicago/Turabian StyleRocher, Grégoire, Thomas Gaillard, Catherine Uzan, Pierre Collinet, Pierre-Adrien Bolze, Marcos Ballester, Sofiane Bendifallah, Lobna Ouldamer, Cyril Touboul, Cyrille Huchon, and et al. 2021. "Does Time-to-Chemotherapy after Primary Complete Macroscopic Cytoreductive Surgery Influence Prognosis for Patients with Epithelial Ovarian Cancer? A Study of the FRANCOGYN Group" Journal of Clinical Medicine 10, no. 5: 1058. https://doi.org/10.3390/jcm10051058
APA StyleRocher, G., Gaillard, T., Uzan, C., Collinet, P., Bolze, P.-A., Ballester, M., Bendifallah, S., Ouldamer, L., Touboul, C., Huchon, C., Lavoue, V., Dabi, Y., Akladios, C., Coutant, C., Raimond, E., Bricou, A., Canlorbe, G., & Azaïs, H. (2021). Does Time-to-Chemotherapy after Primary Complete Macroscopic Cytoreductive Surgery Influence Prognosis for Patients with Epithelial Ovarian Cancer? A Study of the FRANCOGYN Group. Journal of Clinical Medicine, 10(5), 1058. https://doi.org/10.3390/jcm10051058