
Diagnostic Process Using Endoscopy for Biliary Strictures: A Narrative Review

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Noninvasive Evaluation
3. Endoscopic Retrograde Cholangiopancreatography with Cytology and Forceps Biopsy
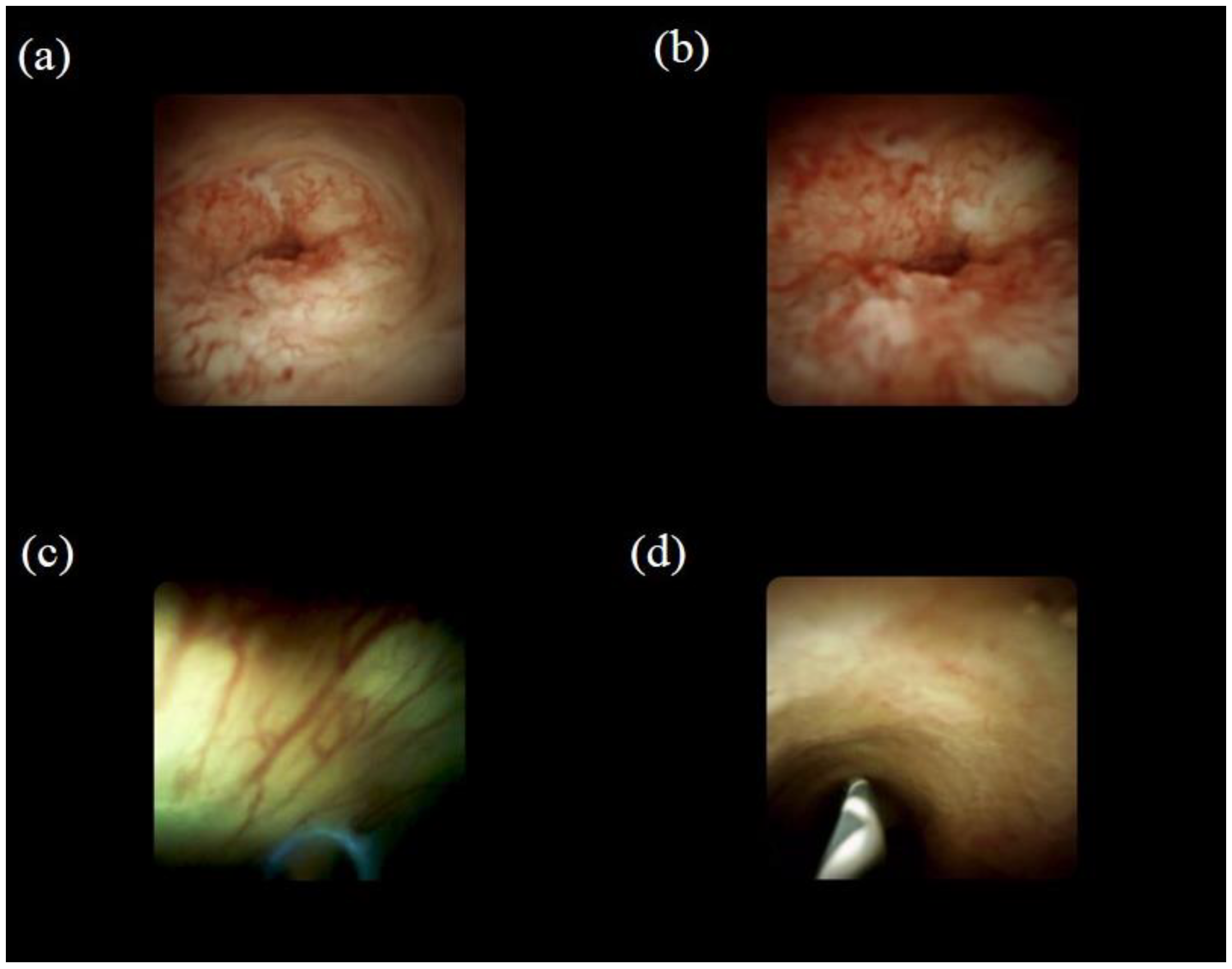
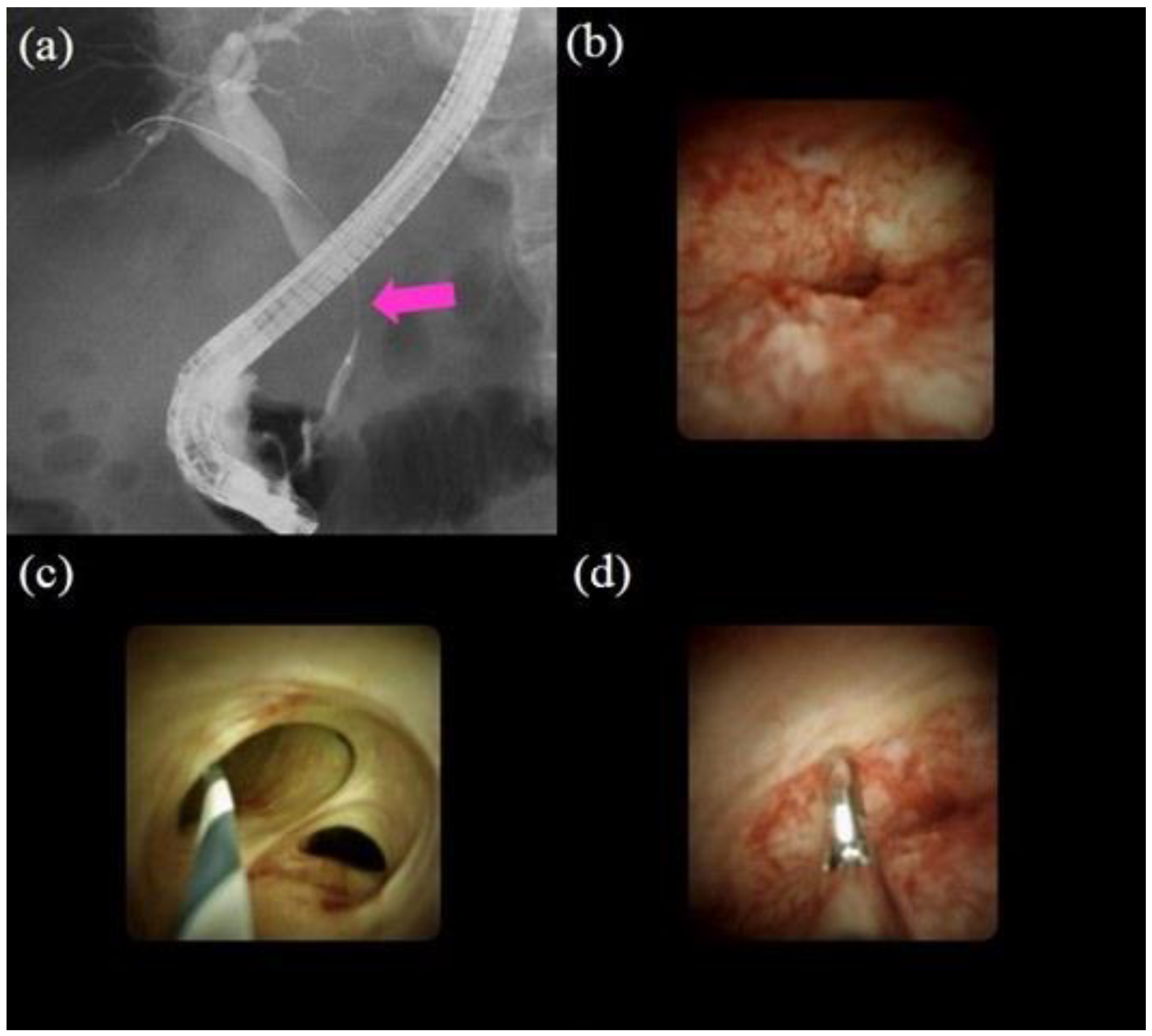
4. Cholangioscopy
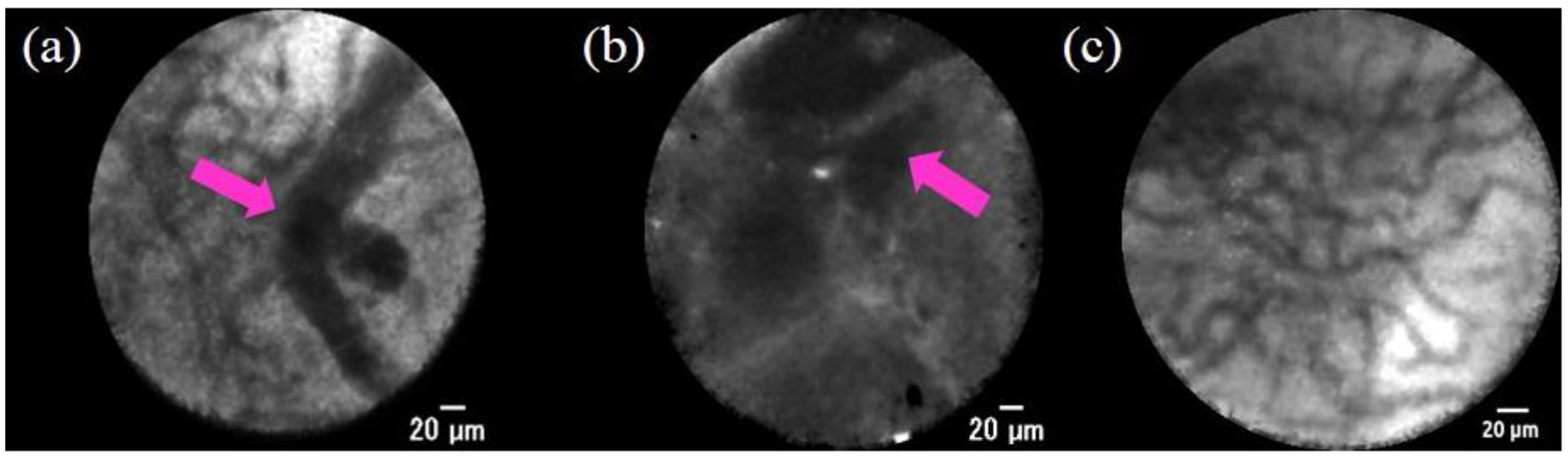
5. Confocal Laser Endomicroscopy
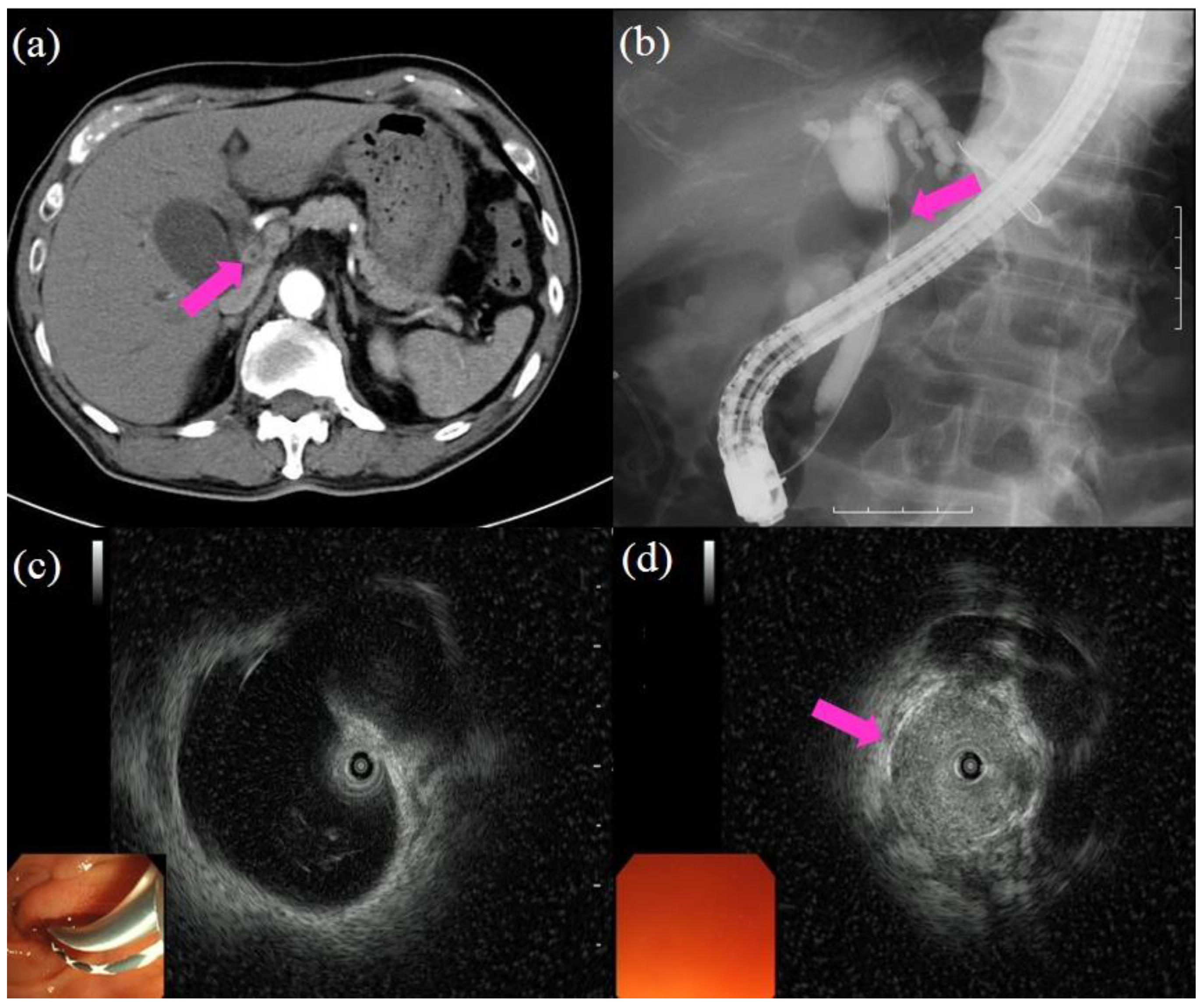
6. Endoscopic Ultrasound and Endoscopic Ultrasound-Guided Fine-Needle Aspiration
7. Molecular Diagnostics
8. Percutaneous Transhepatic Cholangiography
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Park, J.; Kim, M.H.; Kim, K.P.; Park, D.H.; Moon, S.H.; Song, T.J.; Eum, J.; Lee, S.S.; Seo, D.W.; Lee, S.K. Natural History and Prognostic Factors of Advanced Cholangiocarcinoma without Surgery, Chemotherapy, or Radiotherapy: A Large-Scale Observational Study. Gut Liver 2009, 3, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer. N. Engl. J. Med. 2010, 362, 1273–1281. [Google Scholar] [CrossRef]
- DeOliveira, M.L.; Cunningham, S.C.; Cameron, J.L.; Kamangar, F.; Winter, J.M.; Lillemoe, K.D.; Choti, M.A.; Yeo, C.J.; Schulick, R.D. Cholangiocarcinoma: Thirty-one-year experience with 564 patients at a single institution. Ann. Surg. 2007, 245, 755–762. [Google Scholar] [CrossRef]
- Sano, I.; Katanuma, A.; Kuwatani, M.; Kawakami, H.; Kato, H.; Itoi, T.; Ono, M.; Irisawa, A.; Okabe, Y.; Iwashita, T.; et al. Long-term outcomes after therapeutic endoscopic retrograde cholangiopancreatography using balloon-assisted enteroscopy for anastomotic stenosis of choledochojejunostomy/pancreaticojejunostomy. J. Gastroenterol. Hepatol. 2019, 34, 612–619. [Google Scholar] [CrossRef]
- Prokopič, M.; Beuers, U. Management of primary sclerosing cholangitis and its complications: An algorithmic approach. Hepatol. Int. 2021, 15, 6–20. [Google Scholar] [CrossRef]
- Garcea, G.; Ngu, W.; Neal, C.P.; Dennison, A.R.; Berry, D.P. Bilirubin levels predict malignancy in patients with obstructive jaundice. HPB 2011, 13, 426–430. [Google Scholar] [CrossRef]
- Bowlus, C.L.; Olson, K.A.; Gershwin, M.E. Evaluation of indeterminate biliary strictures. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Oseini, A.M.; Chaiteerakij, R.; Shire, A.M.; Ghazale, A.; Kaiya, J.; Moser, C.D.; Aderca, I.; Mettler, T.A.; Therneau, T.M.; Zhang, L.; et al. Utility of serum immunoglobulin G4 in distinguishing immunoglobulin G4-associated cholangitis from cholangiocarcinoma. Hepatology 2011, 54, 940–948. [Google Scholar] [CrossRef]
- Azeem, N.; Ajmera, V.; Hameed, B.; Mehta, N. Hilar cholangiocarcinoma associated with immunoglobulin G4-positive plasma cells and elevated serum immunoglobulin G4 levels. Hepatol. Commun. 2018, 2, 349–353. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Okusaka, T.; Shimizu, K.; Furuse, J.; Ito, Y.; Hanada, K.; Shimosegawa, T.; Okazaki, K. Committee for Revision of Clinical Guidelines for Pancreatic Cancer of the Japan Pancreas Society. Clinical Practice Guidelines for Pancreatic Cancer 2016 from the Japan Pancreas Society: A Synopsis. Pancreas 2017, 46, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, M.; Yoshitomi, H.; Miyakawa, S.; Uesaka, K.; Unno, M.; Endo, I.; Ota, T.; Ohtsuka, M.; Kinoshita, H.; Shimada, K.; et al. Clinical practice guidelines for the management of biliary tract cancers 2015: The 2nd English edition. J. Hepatobiliary Pancreat. Sci. 2015, 22, 249–273. [Google Scholar] [CrossRef]
- Ballehaninna, U.K.; Chamberlain, R.S. The clinical utility of serum CA 19-9 in the diagnosis, prognosis and management of pancreatic adenocarcinoma: An evidence based appraisal. J. Gastrointest. Oncol. 2012, 3, 105–119. [Google Scholar] [PubMed]
- Qin, X.-L.; Wang, Z.-R.; Shi, J.-S.; Lu, M.; Wang, L.; He, Q.-R. Utility of serum CA19-9 in diagnosis of cholangiocarcinoma: In comparison with CEA. World J. Gastroenterol. 2004, 10, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Albu, S.; Tantau, M.; Sparchez, Z.; Branda, H.; Suteu, T.; Badea, R.; Pascu, O. Diagnosis and treatment of extrahepatic cholangiocarcinoma: Results in a series of 124 patients. Rom. J. Gastroenterol. 2005, 14, 33–36. [Google Scholar]
- Takakura, K.; Sumiyama, K.; Munakata, K.; Ashida, H.; Arihiro, S.; Kakutani, H.; Tajiri, H. Clinical usefulness of diffusion-weighted MR imaging for detection of pancreatic cancer: Comparison with enhanced multidetector-row CT. Abdom. Imaging 2011, 36, 457–462. [Google Scholar] [CrossRef]
- Fusari, M.; Maurea, S.; Imbriaco, M.; Mollica, C.; Avitabile, G.; Soscia, F.; Camera, L.; Salvatore, M. Comparison between multislice CT and MR imaging in the diagnostic evaluation of patients with pancreatic masses. Radiol. Med. 2010, 115, 453–466. [Google Scholar] [CrossRef]
- Zhao, W.Y.; Luo, M.; Sun, Y.W.; Xu, Q.; Chen, W.; Zhao, G.; Wu, Z.Y. Computed tomography in diagnosing vascular invasion in pancreatic and periampullary cancers: A systematic review and meta-analysis. Hepatobiliary Pancreat. Dis. Int. 2009, 8, 457–464. [Google Scholar] [PubMed]
- Martinez, N.S.; Trindade, A.J.; Sejpal, D.V. Determining the Indeterminate Biliary Stricture: Cholangioscopy and Beyond. Curr. Gastroenterol. Rep. 2020, 22, 58. [Google Scholar] [CrossRef]
- Al-Dhuhli, H. Role of Magnetic Resonance Cholangiopancreatography in the Evaluation of Biliary Disease. Sultan Qaboos Univ. Med. J. 2009, 9, 341–352. [Google Scholar]
- Freeman, M.L.; Guda, N.M. ERCP cannulation: A review of reported techniques. Gastrointest. Endosc. 2005, 61, 112–125. [Google Scholar] [CrossRef]
- Suissa, A.; Yassin, K.; Lavy, A.; Lachter, J.; Chermech, I.; Karban, A.; Tamir, A.; Eliakim, R. Outcome and early complications of ERCP: A prospective single center study. Hepatogastroenterology 2005, 52, 352–355. [Google Scholar] [PubMed]
- Park, M.S.; Kim, T.K.; Kim, K.W.; Park, S.W.; Lee, J.K.; Kim, J.S.; Lee, J.H.; Kim, K.A.; Kim, A.Y.; Kim, P.N.; et al. Differentiation of extrahepatic bile duct cholangiocarcinoma from benign stricture: Findings at MRCP versus ERCP. Radiology 2004, 233, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Tamada, K.; Ushio, J.; Sugano, K. Endoscopic diagnosis of extrahepatic bile duct carcinoma: Advances and current limitations. World J. Clin. Oncol. 2011, 2, 203–216. [Google Scholar] [CrossRef]
- Farrell, R.J.; Agarwal, B.; Brandwein, S.L.; Underhill, J.; Chuttani, R.; Pleskow, D.K. Intraductal US is a useful adjunct to ERCP for distinguishing malignant from benign biliary strictures. Gastrointest. Endosc. 2002, 56, 681–687. [Google Scholar] [CrossRef]
- Sun, B.; Hu, B. The role of intraductal ultrasonography in pancreatobiliary diseases. Endosc. Ultrasound 2016, 5, 291–299. [Google Scholar] [CrossRef]
- Meister, T.; Heinzow, H.S.; Woestmeyer, C.; Lenz, P.; Menzel, J.; Kucharzik, T.; Domschke, W.; Domagk, D. Intraductal ultrasound substantiates diagnostics of bile duct strictures of uncertain etiology. World J. Gastroenterol. 2013, 19, 874–881. [Google Scholar] [CrossRef]
- Desa, L.A.; Akosa, A.B.; Lazzara, S.; Domizio, P.; Krausz, T.; Benjamin, I.S. Cytodiagnosis in the management of extrahepatic biliary stricture. Gut 1991, 32, 1188–1191. [Google Scholar] [CrossRef] [PubMed]
- Kurzawinski, T.; Deery, A.; Dooley, J.; Dick, R.; Hobbs, K.; Davidson, B. A prospective controlled study comparing brush and bile exfoliative cytology for diagnosing bile duct strictures. Gut 1992, 33, 1675–1677. [Google Scholar] [CrossRef] [PubMed]
- Foutch, P.G.; Kerr, D.M.; Harlan, J.R.; Kummet, T.D. A prospective, controlled analysis of endoscopic cytotechniques for diagnosis of malignant biliary strictures. Am. J. Gastroenterol. 1991, 86, 577–580. [Google Scholar] [PubMed]
- Ponchon, T.; Gagnon, P.; Berger, F.; Labadie, M.; Liaras, A.; Chavaillon, A.; Bory, R. Value of endobiliary brush cytology and biopsies for the diagnosis of malignant bile duct stenosis: Results of a prospective study. Gastrointest. Endosc. 1995, 42, 565–572. [Google Scholar] [CrossRef]
- Pugliese, V.; Conio, M.; Nicolò, G.; Saccomanno, S.; Gatteschi, B. Endoscopic retrograde forceps biopsy and brush cytology of biliary strictures: A prospective study. Gastrointest. Endosc. 1995, 42, 520–526. [Google Scholar] [CrossRef]
- Mansfield, J.C.; Griffin, S.M.; Wadehra, V.; Matthewson, K. A prospective evaluation of cytology from biliary strictures. Gut 1997, 40, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Jailwala, J.; Fogel, E.L.; Sherman, S.; Gottlieb, K.; Flueckiger, J.; Bucksot, L.G.; Lehman, G.A. Triple-tissue sampling at ERCP in malignant biliary obstruction. Gastrointest. Endosc. 2000, 51, 383–390. [Google Scholar] [CrossRef]
- Stewart, C.J.; Mills, P.R.; Carter, R.; O’Donohue, J.; Fullarton, G.; Imrie, C.W.; Murray, W.R. Brush cytology in the assessment of pancreatico-biliary strictures: A review of 406 cases. J. Clin. Pathol. 2001, 54, 449–455. [Google Scholar] [CrossRef]
- Kitajima, Y.; Ohara, H.; Nakazawa, T.; Ando, T.; Hayashi, K.; Takada, H.; Tanaka, H.; Ogawa, K.; Sano, H.; Togawa, S.; et al. Usefulness of transpapillary bile duct brushing cytology and forceps biopsy for improved diagnosis in patients with biliary strictures. J. Gastroenterol. Hepatol. 2007, 22, 1615–1620. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, T.; Tsuyuguchi, T.; Sakai, Y.; Sugiyama, H.; Tawada, K.; Mikata, R.; Tada, M.; Ishihara, T.; Miyazaki, M.; Yokosuka, O. Factors affecting the accuracy of endoscopic transpapillary sampling methods for bile duct cancer. Dig. Endosc. 2014, 26, 276–281. [Google Scholar] [CrossRef]
- Gerges, C.; Benya, T.; Tang, R.S.Y.; Bahin, F.; Lau, J.Y.W.; Geenen, E.V.; Neuhaus, H.; Reddy, D.N.; Ramchandani, M. Digital single-operator peroral cholangioscopy-guided biopsy sampling versus ERCP-guided brushing for indeterminate biliary strictures: A prospective, randomized, multicenter trial (with video). Gastrointest. Endosc. 2020, 91, 1105–1113. [Google Scholar] [CrossRef]
- Schoefl, R.; Haefner, M.; Wrba, F.; Pfeffel, F.; Stain, C.; Poetzi, R.; Gangl, A. Forceps biopsy and brush cytology during endoscopic retrograde cholangiopancreatography for the diagnosis of biliary stenoses. Scand. J. Gastroenterol. 1997, 32, 363–368. [Google Scholar] [CrossRef]
- Kubota, Y.; Takaoka, M.; Tani, K.; Ogura, M.; Kin, H.; Fujimura, K.; Mizuno, T.; Inoue, K. Endoscopic transpapillary biopsy for diagnosis of patients with pancreaticobiliary ductal strictures. Am. J. Gastroenterol. 1993, 88, 1700–1704. [Google Scholar] [PubMed]
- Sugiyama, M.; Atomi, Y.; Wada, N.; Kuroda, A.; Muto, T. Endoscopic transpapillary bile duct biopsy without sphincterotomy for diagnosing biliary strictures: A prospective comparative study with bile and brush cytology. Am. J. Gastroenterol. 1996, 91, 465–467. [Google Scholar]
- Hartman, D.J.; Slivka, A.; Giusto, D.A.; Krasinskas, A.M. Tissue Yield and Diagnostic Efficacy of Fluoroscopic and Cholangioscopic Techniques to Assess Indeterminate Biliary Strictures. Clin. Gastroenterol. Hepatol. 2012, 10, 1042–1046. [Google Scholar] [CrossRef] [PubMed]
- Navaneethan, U.; Njei, B.; Venkatesh, P.G.; Lourdusamy, V.; Sanaka, M.R. Endoscopic ultrasound in the diagnosis of cholangiocarcinoma as the etiology of biliary strictures: A systematic review and meta-analysis. Gastroenterol. Rep. 2015, 3, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Dumonceau, J.-M.; Kapral, C.; Aabakken, L.; Papanikolaou, I.S.; Tringali, A.; Vanbiervliet, G.; Beyna, T.; Dinis-Ribeiro, M.; Hritz, I.; Mariani, A.; et al. ERCP-related adverse events: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2020, 52, 127–149. [Google Scholar] [CrossRef] [PubMed]
- Banks, P.A.; Bollen, T.L.; Dervenis, C.; Gooszen, H.G.; Johnson, C.D.; Sarr, M.G.; Tsiotos, G.G.; Vege, S.S. Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis--2012: Revision of the Atlanta classification and definitions by international consensus. Gut 2013, 62, 102–111. [Google Scholar] [CrossRef]
- Kiriyama, S.; Kozaka, K.; Takada, T.; Strasberg, S.M.; Pitt, H.A.; Gabata, T.; Hata, J.; Liau, K.-H.; Miura, F.; Horiguchi, A.; et al. Tokyo Guidelines 2018: Diagnostic criteria and severity grading of acute cholangitis (with videos). J. Hepato-Biliary-Pancreat. Sci. 2018, 25, 17–30. [Google Scholar] [CrossRef]
- Cotton, P.B.; Eisen, G.M.; Aabakken, L.; Baron, T.H.; Hutter, M.M.; Jacobson, B.C.; Mergener, K.; Nemcek, A., Jr.; Petersen, B.T.; Petrini, J.L.; et al. A lexicon for endoscopic adverse events: Report of an ASGE workshop. Gastrointest. Endosc. 2010, 71, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, M.; Akasaka, Y.; Yamaguchi, K.; Fujimoto, S.; Kawai, K. Direct endoscopic visualization of the bile and pancreatic duct systems by peroral cholangiopancreatoscopy (PCPS). Gastrointest. Endosc. 1978, 24, 141–145. [Google Scholar] [CrossRef]
- Chen, Y.K.; Pleskow, D.K. Preclinical characterization of the Spyglass peroral cholangiopancreatoscopy system for direct access, visualization, and biopsy. Gastrointest. Endosc. 2007, 65, 303–311. [Google Scholar] [CrossRef]
- Navaneethan, U.; Hasan, M.K.; Kommaraju, K.; Zhu, X.; Hebert-Magee, S.; Hawes, R.H.; Vargo, J.J.; Varadarajulu, S.; Parsi, M.A. Digital, single-operator cholangiopancreatoscopy in the diagnosis and management of pancreatobiliary disorders: A multicenter clinical experience (with video). Gastrointest. Endosc. 2016, 84, 649–655. [Google Scholar] [CrossRef]
- Seo, D.W.; Lee, S.K.; Yoo, K.S.; Kang, G.H.; Kim, M.H.; Suh, D.-J.; Min, Y.I. Cholangioscopic findings in bile duct tumors. Gastrointest. Endosc. 2000, 52, 630–634. [Google Scholar] [CrossRef]
- Itoi, T.; Neuhaus, H.; Chen, Y.K. Diagnostic Value of Image-Enhanced Video Cholangiopancreatoscopy. Gastrointest. Endosc. Clin. N. Am. 2009, 19, 557–566. [Google Scholar] [CrossRef]
- Itoi, T.; Sofuni, A.; Itokawa, F.; Tsuchiya, T.; Kurihara, T.; Ishii, K.; Tsuji, S.; Moriyasu, F.; Gotoda, T. Peroral cholangioscopic diagnosis of biliary-tract diseases by using narrow-band imaging (with videos). Gastrointest. Endosc. 2007, 66, 730–736. [Google Scholar] [CrossRef]
- Awadallah, N.S.; Chen, Y.K.; Piraka, C.; Antillon, M.R.; Shah, R.J. Is there a role for cholangioscopy in patients with primary sclerosing cholangitis? Am. J. Gastroenterol. 2006, 101, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Woo, Y.S.; Lee, J.K.; Oh, S.H.; Kim, M.J.; Jung, J.G.; Lee, K.H.; Lee, K.T. Role of SpyGlass peroral cholangioscopy in the evaluation of indeterminate biliary lesions. Dig. Dis. Sci. 2014, 59, 2565–2570. [Google Scholar] [CrossRef] [PubMed]
- Kurihara, T.; Yasuda, I.; Isayama, H.; Tsuyuguchi, T.; Yamaguchi, T.; Kawabe, K.; Okabe, Y.; Hanada, K.; Hayashi, T.; Ohtsuka, T.; et al. Diagnostic and therapeutic single-operator cholangiopancreatoscopy in biliopancreatic diseases: Prospective multicenter study in Japan. World J. Gastroenterol. 2016, 22, 1891–1901. [Google Scholar] [CrossRef] [PubMed]
- Ogura, T.; Imanishi, M.; Kurisu, Y.; Onda, S.; Sano, T.; Takagi, W.; Okuda, A.; Miyano, A.; Amano, M.; Nishioka, N. Prospective evaluation of digital single-operator cholangioscope for diagnostic and therapeutic procedures (with videos). Dig. Endosc. 2017, 29, 782–789. [Google Scholar] [CrossRef]
- Shah, R.J.; Raijman, I.; Brauer, B.; Gumustop, B.; Pleskow, D.K. Performance of a fully disposable, digital, single-operator cholangiopancreatoscope. Endoscopy 2017, 49, 651–658. [Google Scholar] [CrossRef]
- Tanisaka, Y.; Ryozawa, S.; Nonaka, K.; Yasuda, M.; Fujita, A.; Ogawa, T.; Mizuide, M.; Tashima, T.; Araki, R. Diagnosis of Biliary Strictures Using Probe-Based Confocal Laser Endomicroscopy under the Direct View of Peroral Cholangioscopy: Results of a Prospective Study (with Video). Gastroenterol. Res. Pract. 2020, 2020, 1–9. [Google Scholar] [CrossRef]
- Navaneethan, U.; Hasan, M.K.; Lourdusamy, V.; Njei, B.; Varadarajulu, S.; Hawes, R.H. Single-operator cholangioscopy and targeted biopsies in the diagnosis of indeterminate biliary strictures: A systematic review. Gastrointest. Endosc. 2015, 82, 608–614. [Google Scholar] [CrossRef]
- Kawakami, H.; Kuwatani, M.; Etoh, K.; Haba, S.; Yamato, H.; Shinada, K.; Nakanishi, Y.; Tanaka, E.; Hirano, S.; Kondo, S.; et al. Endoscopic retrograde cholangiography versus peroral cholangioscopy to evaluate intraepithelial tumor spread in biliary cancer. Endoscopy 2009, 41, 959–964. [Google Scholar] [CrossRef]
- Draganov, P.V.; Chauhan, S.; Wagh, M.S.; Gupte, A.R.; Lin, T.; Hou, W.; Forsmark, C.E. Diagnostic accuracy of conventional and cholangioscopy-guided sampling of indeterminate biliary lesions at the time of ERCP: A prospective, long-term follow-up study. Gastrointest. Endosc. 2012, 75, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Korrapati, P.; Ciolino, J.; Wani, S.; Shah, J.; Watson, R.; Muthusamy, V.R.; Klapman, J.; Komanduri, S. The efficacy of peroral cholangioscopy for difficult bile duct stones and indeterminate strictures: A systematic review and meta-analysis. Endosc. Int. Open 2016, 4, E263–E275. [Google Scholar] [CrossRef] [PubMed]
- American Society for Gastrointestinal Endoscopy (ASGE) Standards of Practice Committee; Anderson, M.A.; Appalaneni, V.; Ben-Menachem, T.; Decker, G.A.; Early, D.S.; Evans, J.A.; Fanelli, R.D.; Fisher, D.A.; Fisher, L.R.; et al. The role of endoscopy in the evaluation and treatment of patients with biliary neoplasia. Gastrointest. Endosc. 2013, 77, 167–174. [Google Scholar] [CrossRef]
- Meining, A.; Chen, Y.K.; Pleskow, D.; Stevens, P.; Shah, R.J.; Chuttani, R.; Michalek, J.; Slivka, A. Direct visualization of indeterminate pancreaticobiliary strictures with probe-based confocal laser endomicroscopy: A multicenter experience. Gastrointest. Endosc. 2011, 74, 961–968. [Google Scholar] [CrossRef]
- Meining, A.; Shah, R.J.; Slivka, A.; Pleskow, D.; Chuttani, R.; Stevens, P.D.; Becker, V.; Chen, Y.K. Classification of probe-based confocal laser endomicroscopy findings in pancreaticobiliary strictures. Endoscopy 2012, 44, 251–257. [Google Scholar] [CrossRef]
- Caillol, F.; Filoche, B.; Gaidhane, M.; Kahaleh, M. Refined Probe-Based Confocal Laser Endomicroscopy Classification for Biliary Strictures: The Paris Classification. Dig. Dis. Sci. 2013, 58, 1784–1789. [Google Scholar] [CrossRef] [PubMed]
- Slivka, A.; Gan, I.; Jamidar, P.; Costamagna, G.; Cesaro, P.; Giovannini, M.; Caillol, F.; Kahaleh, M. Validation of the diagnostic accuracy of probe-based confocal laser endomicroscopy for the characterization of indeterminate biliary strictures: Results of a prospective multicenter international study. Gastrointest. Endosc. 2015, 81, 282–290. [Google Scholar] [CrossRef]
- Dubow, M.; Tatman, P.D.; Shah, R.J. Individual probe based confocal laser endomicroscopy criteria in the analysis of indeterminate biliary strictures. Scand. J. Gastroenterol. 2018, 53, 1358–1363. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Lu, Y.; Sun, B.; Zhang, W.-M.; Zhang, Z.-Z.; He, Y.-P.; Yang, X.-J. Probe-based confocal laser endomicroscopy for the diagnosis of undetermined biliary stenoses: A meta-analysis. Clin. Res. Hepatol. Gastroenterol. 2016, 40, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Garrow, D.; Miller, S.; Sinha, D.; Conway, J.; Hoffman, B.J.; Hawes, R.H.; Romagnuolo, J. Endoscopic Ultrasound: A Meta-analysis of Test Performance in Suspected Biliary Obstruction. Clin. Gastroenterol. Hepatol. 2007, 5, 616–623.e1. [Google Scholar] [CrossRef] [PubMed]
- Mohamadnejad, M.; DeWitt, J.M.; Sherman, S.; LeBlanc, J.K.; Pitt, H.A.; House, M.G.; Jones, K.J.; Fogel, E.L.; McHenry, L.; Watkins, J.L.; et al. Role of EUS for preoperative evaluation of cholangiocarcinoma: A large single-center experience. Gastrointest. Endosc. 2011, 73, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Yamao, K.; Sawaki, A.; Mizuno, N.; Shimizu, Y.; Yatabe, Y.; Koshikawa, T. Endoscopic ultrasound-guided fine-needle aspiration biopsy (EUS-FNAB): Past, present, and future. J. Gastroenterol. 2005, 40, 1013–1023. [Google Scholar] [CrossRef] [PubMed]
- Hasan, M.K.; Hawes, R.H. EUS-Guided FNA of Solid Pancreas Tumors. Gastrointest. Endosc. Clin. N. Am. 2012, 22, 155–167. [Google Scholar] [CrossRef] [PubMed]
- Fritscherravens, A.; Broering, D.C.; Knoefel, W.T.; Rogiers, X.; Swain, P.; Thonke, F.; Bobrowski, C.; Topalidis, T.; Soehendra, N. EUS-Guided Fine-Needle Aspiration of Suspected Hilar Cholangiocarcinoma in Potentially Operable Patients with Negative Brush Cytology. Am. J. Gastroenterol. 2004, 99, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Rösch, T.; Hofrichter, K.; Frimberger, E.; Meining, A.; Born, P.; Weigert, N.; Allescher, H.-D.; Classen, M.; Barbur, M.; Schenck, U.; et al. ERCP or EUS for tissue diagnosis of biliary strictures? A prospective comparative study. Gastrointest. Endosc. 2004, 60, 390–396. [Google Scholar] [CrossRef]
- DeWitt, J.; Misra, V.L.; Leblanc, J.K.; McHenry, L.; Sherman, S. EUS-guided FNA of proximal biliary strictures after negative ERCP brush cytology results. Gastrointest. Endosc. 2006, 64, 325–333. [Google Scholar] [CrossRef]
- Weilert, F.; Bhat, Y.M.; Binmoeller, K.F.; Kane, S.; Jaffee, I.M.; Shaw, R.E.; Cameron, R.; Hashimoto, Y.; Shah, J.N. EUS-FNA is superior to ERCP-based tissue sampling in suspected malignant biliary obstruction: Results of a prospective, single-blind, comparative study. Gastrointest. Endosc. 2014, 80, 97–104. [Google Scholar] [CrossRef]
- Onda, S.; Ogura, T.; Kurisu, Y.; Masuda, D.; Sano, T.; Takagi, W.; Fukunishi, S.; Higuchi, K. EUS-guided FNA for biliary disease as first-line modality to obtain histological evidence. Ther. Adv. Gastroenterol. 2016, 9, 302–312. [Google Scholar] [CrossRef]
- De Moura, D.T.H.; Moura, E.G.H.; Bernardo, W.M.; De Moura, E.T.H.; Baraca, F.I.; Kondo, A.; Matuguma, S.E.; Almeida Artifon, E.L. Endoscopic retrograde cholangiopancreatography versus endoscopic ultrasound for tissue diagnosis of malignant biliary stricture: Systematic review and meta-analysis. Endosc. Ultrasound 2018, 7, 10–19. [Google Scholar] [CrossRef]
- Adler, D.G.; Witt, B.; Chadwick, B.; Wells, J.; Taylor, L.J.; Dimaio, C.; Schmidt, R. Pathologic evaluation of a new endoscopic ultrasound needle designed to obtain core tissue samples: A pilot study. Endosc. Ultrasound 2016, 5, 178–183. [Google Scholar] [CrossRef]
- Bang, J.Y.; Hebert-Magee, S.; Hasan, M.K.; Navaneethan, U.; Hawes, R.; Varadarajulu, S. Endoscopic ultrasonography-guided biopsy using a Franseen needle design: Initial assessment. Dig. Endosc. 2017, 29, 338–346. [Google Scholar] [CrossRef]
- Van Riet, P.A.; Erler, N.S.; Bruno, M.J.; Cahen, D.L. Comparison of fine-needle aspiration and fine-needle biopsy devices for endoscopic ultrasound-guided sampling of solid lesions: A systemic review and meta-analysis. Endoscopy 2020. [Google Scholar] [CrossRef] [PubMed]
- Gao, R.-Y.; Wu, B.-H.; Shen, X.-Y.; Peng, T.-L.; Li, D.-F.; Wei, C.; Yu, Z.-C.; Luo, M.-H.; Xiong, F.; Wang, L.-S.; et al. Overlooked risk for needle tract seeding following endoscopic ultrasound-guided minimally invasive tissue acquisition. World J. Gastroenterol. 2020, 26, 6182–6194. [Google Scholar] [CrossRef] [PubMed]
- Mizuide, M.; Ryozawa, S.; Fujita, A.; Ogawa, T.; Katsuda, H.; Suzuki, M.; Noguchi, T.; Tanisaka, Y. Complications of Endoscopic Ultrasound-Guided Fine Needle Aspiration: A Narrative Review. Diagnostics 2020, 10, 964. [Google Scholar] [CrossRef] [PubMed]
- Alekseyev, Y.O.; Fazeli, R.; Yang, S.; Basran, R.; Maher, T.; Miller, N.S.; Remic, D. A Next-Generation Sequencing Primer—How Does It Work and What Can It Do? Acad. Pathol. 2018, 5. [Google Scholar] [CrossRef] [PubMed]
- Singhi, A.D.; Nikiforova, M.N.; Chennat, J.; Papachristou, G.I.; Khalid, A.; Rabinovitz, M.; Das, R.; Sarkaria, S.; Ayasso, M.S.; Wald, A.I.; et al. Integrating next-generation sequencing to endoscopic retrograde cholangiopancreatography (ERCP)-obtained biliary specimens improves the detection and management of patients with malignant bile duct strictures. Gut 2020, 69, 52–61. [Google Scholar] [CrossRef]
- Kim, E.H.; Kim, H.J.; Oh, H.C.; Lee, K.H.; Jung, J.Y.; Kim, S.; Lee, S.S.; Seo, D.W.; Kim, M.H.; Lee, S.K. The usefulness of percutaneous transhepatic cholangioscopy for identifying malignancies in distal common [corrected] bile duct strictures. J. Korean Med. Sci. 2008, 23, 579–585. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wang, L.; Lin, N.; Xin, F.; Ke, Q.; Zeng, Y.; Liu, J. A systematic review of the comparison of the incidence of seeding metastasis between endoscopic biliary drainage and percutaneous transhepatic biliary drainage for resectable malignant biliary obstruction. World. J. Surg. Oncol. 2019, 17, 116. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Year | Number of Patients | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|
| Foutch et al. [29] | 1991 | 30 | 33 | 100 | 100 | 58 |
| Ponchon et al. [30] | 1995 | 204 | 35 | 97 | 96 | 44 |
| Pugliese et al. [31] | 1995 | 94 | 54 | 100 | 100 | 50 |
| Mansfield et al. [32] | 1997 | 43 | 42 | 100 | 100 | 8 |
| Jailwala et al. [33] | 2000 | 133 | 30 | 100 | 100 | 28 |
| Stewart et al. [34] | 2001 | 406 | 60 | 98 | 98 | 61 |
| Kitajima et al. [35] | 2007 | 60 | 72 | 100 | 100 | 32 |
| Nishikawa et al. [36] | 2014 | 123 | 51 | 98 | 97 | 63 |
| Gerges et al. [37] | 2020 | 27 | 21 | 100 | 100 | 65 |
| Authors | Year | Number of Patients | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|
| Kubota et al. [39] | 1993 | 41 | 81 | 100 | 100 | 75 |
| Ponchon et al. [30] | 1995 | 128 | 43 | 97 | 97 | 41 |
| Sugiyama et al. [40] | 1996 | 45 | 81 | 100 | 100 | 67 |
| Jailwala et al. [33] | 2000 | 133 | 43 | 90 | 94 | 31 |
| Stewart et al. [34] | 2001 | 406 | 60 | 98 | 98 | 61 |
| Kitajima et al. [35] | 2007 | 60 | 65 | 100 | 100 | 22 |
| Hartman et al. [41] | 2012 | 81 | 76 | 100 | 100 | 81 |
| Nishikawa et al. [36] | 2014 | 87 | 50 | 96 | 97 | 41 |
| Authors | Year | Number of Patients | Visual Sensitivity (%) | Visual Specificity (%) | Visual Accuracy (%) | Biopsy Sensitivity (%) | Biopsy Specificity (%) | Biopsy Accuracy (%) |
|---|---|---|---|---|---|---|---|---|
| Chen et al. [48] | 2007 | 22 | 100 | 77 | 85 | 71 | 100 | 90 |
| Hartman et al. [41] | 2012 | 89 | 88 | 86 | 87 | 57 | 100 | 78 |
| Woo et al. [54] | 2014 | 32 | 100 | 90 | 96 | 64 | 100 | 73 |
| Kurihara et al. [55] | 2016 | 89 | 94 | 92 | 94 | 65 | 89 | 70 |
| Navaneethan et al. [49] | 2016 | 44 | 90 | 96 | N/A | 85 | 100 | N/A |
| Ogura et al. [56] | 2017 | 25 | 83 | 89 | 93 | 80 | 100 | 89 |
| Shah et al. [57] | 2017 | 58 | 97 | 93 | 94 | 86 | 100 | 91 |
| Gerges et al. [37] | 2020 | 31 | 96 | 67 | 87 | 68 | 100 | 77 |
| Tanisaka et al. [58] | 2020 | 30 | 100 | 77 | 90 | 82 | 100 | 90 |
| Authors | Year | Number of Patients | Sensitivity (%) | Specificity (%) | Accuracy (%) |
|---|---|---|---|---|---|
| Meining et al. [64] | 2011 | 89 | 98 | 67 | 81 |
| Meining et al. [65] | 2012 | 45 | 97 | 33 | N/A |
| Caillol et al. [66] | 2013 | 89 | 96 | 64 | 78 |
| Slivka et al. [67] | 2015 | 112 | 89 | 71 | 82 |
| Dubow et al. [68] | 2018 | 97 | 83 | 93 | 90 |
| Tanisaka et al. [58] | 2020 | 30 | 94 | 92 | 93 |
| Authors | Year | Number of Patients | Sensitivity (%) | Specificity (%) | Accuracy (%) | Adverse Events, n |
|---|---|---|---|---|---|---|
| Fritscher-Ravens et al. [74] | 2004 | 44 | 89 | 100 | 91 | None |
| Rösch et al. [75] | 2004 | 50 | 43 | 100 | 70 | N/A |
| DeWitt et al. [76] | 2006 | 24 | 77 | 100 | 79 | None |
| Mohamadnejad et al. [71] | 2011 | 81 | 73 | N/A | N/A | 1 (hemobilia) |
| Weilert et al. [77] | 2014 | 51 | 94 | 100 | 94 | None |
| Onda et al. [78] | 2016 | 47 | 84 | 100 | 87 | None |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanisaka, Y.; Mizuide, M.; Fujita, A.; Ogawa, T.; Suzuki, M.; Katsuda, H.; Saito, Y.; Miyaguchi, K.; Tashima, T.; Mashimo, Y.; et al. Diagnostic Process Using Endoscopy for Biliary Strictures: A Narrative Review. J. Clin. Med. 2021, 10, 1048. https://doi.org/10.3390/jcm10051048
Tanisaka Y, Mizuide M, Fujita A, Ogawa T, Suzuki M, Katsuda H, Saito Y, Miyaguchi K, Tashima T, Mashimo Y, et al. Diagnostic Process Using Endoscopy for Biliary Strictures: A Narrative Review. Journal of Clinical Medicine. 2021; 10(5):1048. https://doi.org/10.3390/jcm10051048
Chicago/Turabian StyleTanisaka, Yuki, Masafumi Mizuide, Akashi Fujita, Tomoya Ogawa, Masahiro Suzuki, Hiromune Katsuda, Youichi Saito, Kazuya Miyaguchi, Tomoaki Tashima, Yumi Mashimo, and et al. 2021. "Diagnostic Process Using Endoscopy for Biliary Strictures: A Narrative Review" Journal of Clinical Medicine 10, no. 5: 1048. https://doi.org/10.3390/jcm10051048
APA StyleTanisaka, Y., Mizuide, M., Fujita, A., Ogawa, T., Suzuki, M., Katsuda, H., Saito, Y., Miyaguchi, K., Tashima, T., Mashimo, Y., & Ryozawa, S. (2021). Diagnostic Process Using Endoscopy for Biliary Strictures: A Narrative Review. Journal of Clinical Medicine, 10(5), 1048. https://doi.org/10.3390/jcm10051048