
A Cognitive Behavioral Therapy-Informed Self-Management Program for Acute Respiratory Failure Survivors: A Feasibility Study


Abstract
1. Introduction
2. Methods Section
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Lilly, C.M.; Swami, S.; Liu, X.; Riker, R.R.; Badawi, O. Five-Year Trends of Critical Care Practice and Outcomes. Chest 2017, 152, 723–735. [Google Scholar] [CrossRef] [PubMed]
- Needham, D.M.; Davidson, J.; Cohen, H.; Hopkins, R.O.; Weinert, C.; Wunsch, H.; Zawistowski, C.; Bemis-Dougherty, A.; Berney, S.C.; Bienvenu, O.J.; et al. Improving long-term outcomes after discharge from intensive care unit: Report from a stakeholders’ conference. Crit. Care Med. 2012, 40, 502–509. [Google Scholar] [CrossRef]
- Bienvenu, O.J.; Friedman, L.A.; Colantuoni, E.; Dinglas, V.D.; Sepulveda, K.A.; Mendez-Tellez, P.; Shanholz, C.; Pronovost, P.J.; Needham, D.M. Psychiatric symptoms after acute respiratory distress syndrome: A 5-year longitudinal study. Intensive Care Med. 2018, 44, 38–47. [Google Scholar] [CrossRef]
- Devlin, J.W.; Skrobik, Y.; Gélinas, C.; Needham, D.M.; Slooter, A.J.C.; Pandharipande, P.P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit. Care Med. 2018, 46, e825–e873. [Google Scholar] [CrossRef] [PubMed]
- Ely, E.W. The ABCDEF Bundle: Science and Philosophy of How ICU Liberation Serves Patients and Families. Crit. Care Med. 2017, 45, 321–330. [Google Scholar] [CrossRef]
- May, A.D.; Parker, A.M.; Caldwell, E.S.; Hough, C.L.; Jutte, J.E.; Gonzalez, M.S.; Needham, D.M.; Hosey, M.M. Provider-Documented Anxiety in the ICU: Prevalence, Risk Factors, and Associated Patient Outcomes. J. Intensive Care Med. 2020, 0885066620956564. [Google Scholar] [CrossRef]
- Chlan, L.; Savik, K. Patterns of anxiety in critically ill patients receiving mechanical ventilatory support. Nurs. Res. 2011, 60, S50. [Google Scholar] [CrossRef] [PubMed]
- Wade, D.M.; Mouncey, P.R.; Richards-Belle, A.; Wulff, J.; Harrison, D.A.; Sadique, M.Z.; Grieve, R.D.; Emerson, L.M.; Mason, A.J.; Aaronovitch, D.; et al. Effect of a Nurse-Led Preventive Psychological Intervention on Symptoms of Posttraumatic Stress Disorder Among Critically Ill Patients: A Randomized Clinical Trial. JAMA 2019, 321, 665–675. [Google Scholar] [CrossRef]
- Karnatovskaia, L.V.; Schulte, P.J.; Philbrick, K.L.; Johnson, M.M.; Anderson, B.K.; Gajic, O.; Clark, M.M. Psychocognitive sequelae of critical illness and correlation with 3 months follow up. J. Crit. Care 2019, 52, 166–171. [Google Scholar] [CrossRef]
- Wade, D.M.; Brewin, C.R.; Howell, D.C.J.; White, E.; Mythen, M.G.; Weinman, J.A. Intrusive memories of hallucinations and delusions in traumatized intensive care patients: An interview study. Br. J. Health Psychol. 2015, 20, 613–631. [Google Scholar] [CrossRef]
- Agard, A.S.; Egerod, I.; Tonnesen, E.; Lomborg, K. Struggling for independence: A grounded theory study on convalescence of ICU survivors 12 months post ICU discharge. Intensive Crit Care Nurs. 2012, 28, 105–113. [Google Scholar] [CrossRef]
- Hashem, M.D.; Nallagangula, A.; Nalamalapu, S.; Nunna, K.; Nausran, U.; Robinson, K.A.; Dinglas, V.D.; Needham, D.M.; Eakin, M.N. Patient outcomes after critical illness: A systematic review of qualitative studies following hospital discharge. Crit. Care 2016, 20. [Google Scholar] [CrossRef]
- Nikayin, S.; Rabiee, A.; Hashem, M.D.; Huang, M.; Bienvenu, O.J.; Turnbull, A.E.; Needham, D.M. Anxiety symptoms in survivors of critical illness: A systematic review and meta-analysis. Gen. Hosp. Psychiatry 2016, 43, 23–29. [Google Scholar] [CrossRef]
- Roberts, M.B.; Glaspey, L.J.; Mazzarelli, A.; Jones, C.W.; Kilgannon, H.J.; Trzeciak, S.; Roberts, B.W. Early Interventions for the Prevention of Posttraumatic Stress Symptoms in Survivors of Critical Illness: A Qualitative Systematic Review. Crit. Care Med. 2018, 46, 1328. [Google Scholar] [CrossRef] [PubMed]
- Peris, A.; Bonizzoli, M.; Iozzelli, D.; Migliaccio, M.L.; Zagli, G.; Bacchereti, A.; Debolini, M.; Vannini, E.; Solaro, M.; Balzi, I.; et al. Early intra-intensive care unit psychological intervention promotes recovery from post traumatic stress disorders, anxiety and depression symptoms in critically ill patients. Crit. Care 2011, 15, R41. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.; Gopal, A.; Roberts, K.J.; Anderson, E.; Siegel, A.M. Ventilator Dependent Patients Successfully Weaned with Cognitive Behavioral Therapy: A Case Series. Psychosomatics 2019. In Press. [Google Scholar] [CrossRef] [PubMed]
- Fauerbach, J.A.; Gehrke, A.K.; Mason, S.T.; Gould, N.F.; Milner, S.M.; Caffrey, J. Cognitive Behavioral Therapy for Acute Post-trauma Distress: A Randomized, Controlled, Proof-of-Concept Study among Hospitalized Adults with Burns. Arch. Phys. Med. Rehabil. 2019. [Google Scholar] [CrossRef]
- Czajkowski, S.M.; Powell, L.H.; Adler, N.; Naar-King, S.; Reynolds, K.D.; Hunter, C.M.; Laraia, B.; Olster, D.H.; Perna, F.M.; Peterson, J.C.; et al. From ideas to efficacy: The ORBIT model for developing behavioral treatments for chronic diseases. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2015, 34, 971–982. [Google Scholar] [CrossRef]
- Bradford, A.N.; Castillo, R.C.; Carlini, A.R.; Wegener, S.T.; Teter, H.J.; Mackenzie, E.J. The Trauma Survivors Network: Survive. Connect. Rebuild. J. Trauma Acute Care Surg. 2011, 70, 1557–1560. [Google Scholar] [CrossRef] [PubMed]
- Wegener, S.T.; Mackenzie, E.J.; Ephraim, P.; Ehde, D.; Williams, R. Self-Management Improves Outcomes in Persons With Limb Loss. Arch. Phys. Med. Rehabil. 2009, 90, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K.R.; Sobel, D.S.; Stewart, A.L.; Brown, B.W.J.; Bandura, A.; Ritter, P.; Gonzalez, V.M.; Laurent, D.D.; Holman, H.R. Evidence Suggesting That a Chronic Disease Self-Management Program Can Improve Health Status While Reducing Hospitalization: A Randomized Trial. Med. Care 1999, 37, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Cadel, L.; DeLuca, C.; Hitzig, S.L.; Packer, T.L.; Lofters, A.K.; Patel, T.; Guilcher, S.J.T. Self-management of pain and depression in adults with spinal cord injury: A scoping review. J. Spinal Cord Med. 2018, 1–18. [Google Scholar] [CrossRef]
- Lamers, F.; Jonkers, C.C.M.; Bosma, H.; Chavannes, N.H.; Knottnerus, J.A.; van Eijk, J.T. Improving Quality of Life in Depressed COPD Patients: Effectiveness of a Minimal Psychological Intervention. COPD J. Chronic Obstr. Pulm. Dis. 2010, 7, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Heslop-Marshall, K.; Baker, C.; Carrick-Sen, D.; Newton, J.; Echevarria, C.; Stenton, C.; Jambon, M.; Gray, J.; Pearce, K.; Burns, G.; et al. Randomised controlled trial of cognitive behavioural therapy in COPD. ERJ Open Res. 2018, 4. [Google Scholar] [CrossRef]
- Howard, C.; Dupont, S. ‘The COPD breathlessness manual’: A randomised controlled trial to test a cognitive-behavioural manual versus information booklets on health service use, mood and health status, in patients with chronic obstructive pulmonary disease. NPJ Prim. Care Respir. Med. 2014, 24, 1–8. [Google Scholar] [CrossRef]
- Lorig, K.R.; Holman, H.R. Self-management education: History, definition, outcomes, and mechanisms. Ann. Behav. Med. 2003, 26, 7. [Google Scholar] [CrossRef]
- Archer, K.R.; Devin, C.J.; Vanston, S.W.; Koyama, T.; Phillips, S.E.; George, S.Z.; McGirt, M.J.; Spengler, D.M.; Aaronson, O.S.; Cheng, J.S.; et al. Cognitive-Behavioral–Based Physical Therapy for Patients With Chronic Pain Undergoing Lumbar Spine Surgery: A Randomized Controlled Trial. J. Pain 2016, 17, 76–89. [Google Scholar] [CrossRef]
- Lorig, K.R.; Hurwicz, M.-L.; Sobel, D.; Hobbs, M.; Ritter, P.L. A national dissemination of an evidence-based self-management program: A process evaluation study. Patient Educ. Couns. 2005, 59, 69–79. [Google Scholar] [CrossRef]
- Druss, B.G.; Zhao, L.; von Esenwein, S.A.; Bona, J.R.; Fricks, L.; Jenkins-Tucker, S.; Sterling, E.; DiClemente, R.; Lorig, K. The Health and Recovery Peer (HARP) Program: A peer-led intervention to improve medical self-management for persons with serious mental illness. Schizophr. Res. 2010, 118, 264–270. [Google Scholar] [CrossRef]
- Bodenheimer, T.; Lorig, K.; Holman, H.; Grumbach, K. Patient Self-management of Chronic Disease in Primary Care. JAMA 2002, 288, 2469–2475. [Google Scholar] [CrossRef] [PubMed]
- Hosey, M.M.; Ali, M.K.; Mantheiy, E.C.; Albert, K.; Wegener, S.T.; Needham, D.M. Psychology consultation patterns in a medical intensive care unit: A brief report. Rehabil. Psychol. 2019, 64, 360–365. [Google Scholar] [CrossRef]
- Spathis, A.; Booth, S.; Moffat, C.; Hurst, R.; Ryan, R.; Chin, C.; Burkin, J. The Breathing, Thinking, Functioning clinical model: A proposal to facilitate evidence-based breathlessness management in chronic respiratory disease. NPJ Prim. Care Respir. Med. 2017, 27, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Sperry, L. Treatment of Chronic Medical Conditions: Cognitive-Behavioral Therapy Strategies and Integrative Treatment Protocols; American Psychological Association: Washington, DC, USA, 2009; ISBN 978-1-4338-0389-5. [Google Scholar]
- Happ, M.B.; Baumann, B.M.; Sawicki, J.; Tate, J.A.; George, E.L.; Barnato, A.E. SPEACS-2: Intensive Care Unit “Communication Rounds” with Speech Language Pathology. Geriatr. Nur. (Lond.) 2010, 31, 170–177. [Google Scholar] [CrossRef]
- Chlan, L.L.; Weinert, C.R.; Heiderscheit, A.; Tracy, M.F.; Skaar, D.J.; Guttormson, J.L.; Savik, K. Effects of patient-directed music intervention on anxiety and sedative exposure in critically ill patients receiving mechanical ventilatory support: A randomized clinical trial. JAMA 2013, 309, 2335–2344. [Google Scholar] [CrossRef]
- Bashar, F.R.; Vahedian-Azimi, A.; Hajiesmaeili, M.; Salesi, M.; Farzanegan, B.; Shojaei, S.; Goharani, R.; Madani, S.J.; Moghaddam, K.G.; Hatamian, S.; et al. Post-ICU psychological morbidity in very long ICU stay patients with ARDS and delirium. J. Crit. Care 2018, 43, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Girard, T.D.; Thompson, J.L.; Pandharipande, P.P.; Brummel, N.E.; Jackson, J.C.; Patel, M.B.; Hughes, C.G.; Chandrasekhar, R.; Pun, B.T.; Boehm, L.M.; et al. Clinical phenotypes of delirium during critical illness and severity of subsequent long-term cognitive impairment: A prospective cohort study. Lancet Respir. Med. 2018, 6, 213–222. [Google Scholar] [CrossRef]
- Williams, V.S.; Morlock, R.J.; Feltner, D. Psychhometric evaluation of a visual analog scale for the assessment of anxiety. Health Qual. Life Outcomes 2010, 8, 8. [Google Scholar] [CrossRef]
- Kok, L.; Slooter, A.J.; Hillegers, M.H.; van Dijk, D.; Veldhuijzen, D.S. Benzodiazepine Use and Neuropsychiatric Outcomes in the ICU: A Systematic Review*. Crit. Care Med. 2018, 46, 1673–1680. [Google Scholar] [CrossRef]
- Pisani, M.A.; Murphy, T.E.; Araujo, K.L.B.; Slattum, P.; Van Ness, P.H.; Inouye, S.K. Benzodiazepine and opioid use and the duration of ICU delirium in an older population. Crit. Care Med. 2009, 37, 177–183. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| SMARF Session | Session Description |
|---|---|
| 1. Education & Goal Setting | Learning the relationship between medical events and changes in anxiety level; education about structure and format of sessions; set goals for SMARF treatment |
| 2. Elicit Concerns & Problem Solving | Eliciting concerns about medical care (focusing on concerns within patient control); develop problem-solving skills & established approaches, including SMART (Specific, Measurable, Attainable, Relevant, Time-sensitive) goals |
| 3. Thought Restructuring | Identifying the relationship between thoughts and anxiety, identifying & challenging maladaptive thoughts and beliefs |
| 4. Relaxation training | Identifying the relation between anxiety and physiologic response, and acquiring relaxation skills (e.g., guided imagery, body scan, and breathing retraining) |
| 5. Exposure | Understanding fear-avoidance patterns; providing in-vivo exposure to anxiety provoking events |
| 6. Transition out of Hospital | Providing education about anxiety and discharge from hospital; identifying “red flags” about levels of anxiety; discussing how to find help in the next settings |
| Patient Characteristic | Statistic |
|---|---|
| Age, Median (IQR) Years | 48 (32, 69) |
| Female, N (%) | 6 (55) |
| Race/Ethnicity, N (%) | |
| White | 6 (55) |
| Black | 4 (36) |
| Hispanic Ethnicity | 1 (9) |
| ICU Admission Diagnosis Category, N (%) | |
| Acute Hypoxemia Respiratory Failure | 8 (73) |
| Chronic Obstructive Pulmonary Disease | 1 (9) |
| Sepsis | 1 (9) |
| Gastrointestinal Bleed | 1 (9) |
| ICU LOS, median (IQR) days | 47 (24, 58) 1 |
| Hospital LOS, median (IQR) days | 51 (30, 121) |
| ICU LOS prior to start of intervention, median (IQR) days | 19 (13, 21) |
| Hospital LOS prior to start of intervention, median (IQR) days | 25 (14, 49) |
| Intervention Result | Statistic |
|---|---|
| Agree to participate in intervention, N (%) | 11 (100) |
| Number of sessions completed per patient, median (IQR) | 6 (3, 6) |
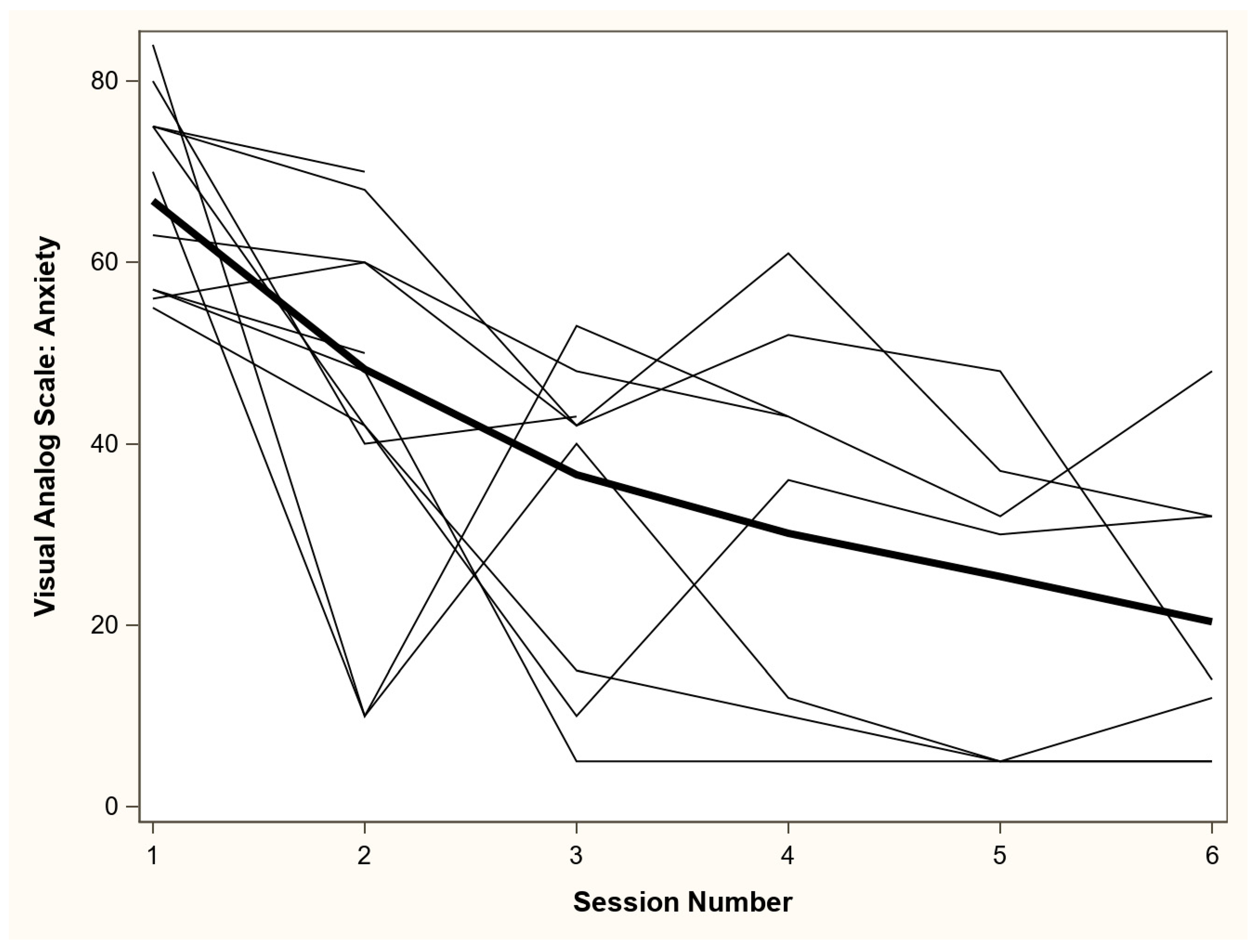
| Pre-intervention VAS-A 1 score, median (IQR) | 70 (57, 75) |
| Intervention sessions completed in ICU, N (%) | 42 (84%) |
| VAS-A 1 decrease from pre-intervention to final session for all patients, median (IQR) | 44 (21, 48) |
| VAS-A 1 decrease from pre-intervention to final session for patients receiving all 6 sessions, median (IQR) | 51 (44, 62) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosey, M.M.; Wegener, S.T.; Hinkle, C.; Needham, D.M. A Cognitive Behavioral Therapy-Informed Self-Management Program for Acute Respiratory Failure Survivors: A Feasibility Study. J. Clin. Med. 2021, 10, 872. https://doi.org/10.3390/jcm10040872
Hosey MM, Wegener ST, Hinkle C, Needham DM. A Cognitive Behavioral Therapy-Informed Self-Management Program for Acute Respiratory Failure Survivors: A Feasibility Study. Journal of Clinical Medicine. 2021; 10(4):872. https://doi.org/10.3390/jcm10040872
Chicago/Turabian StyleHosey, Megan M., Stephen T. Wegener, Caroline Hinkle, and Dale M. Needham. 2021. "A Cognitive Behavioral Therapy-Informed Self-Management Program for Acute Respiratory Failure Survivors: A Feasibility Study" Journal of Clinical Medicine 10, no. 4: 872. https://doi.org/10.3390/jcm10040872
APA StyleHosey, M. M., Wegener, S. T., Hinkle, C., & Needham, D. M. (2021). A Cognitive Behavioral Therapy-Informed Self-Management Program for Acute Respiratory Failure Survivors: A Feasibility Study. Journal of Clinical Medicine, 10(4), 872. https://doi.org/10.3390/jcm10040872