
No Evidence for Classic Thrombotic Microangiopathy in COVID-19

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
3.2. COVID-19-Associated Laboratory Parameters and Organ Damage
3.3. COVID-19 Associated Haemostatic Alterations
3.3.1. Thromboembolic Events during COVID-19
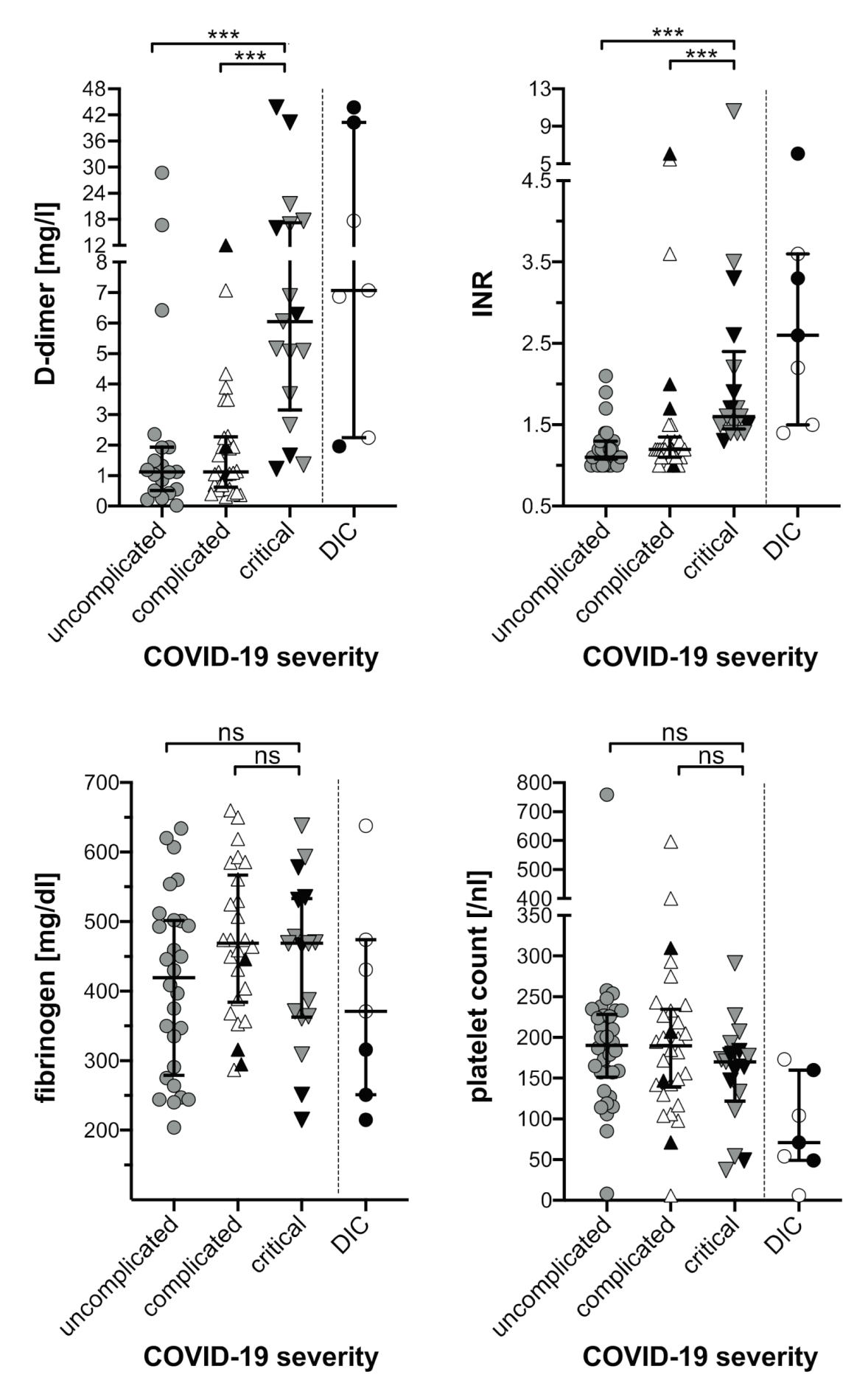
3.3.2. D-Dimers, Fibrinogen, INR, Platelet Count
3.3.3. Patients with DIC
3.3.4. Markers of Endothelial Damage and Thrombotic Microangiopathy
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and Clinical Characteristics of 99 Cases of 2019-Novel Coronavirus (2019-nCoV) Pneumonia in Wuhan, China. SSRN Electron. J. 2020, 395, 10223. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef]
- Yang, X.; Yang, Q.; Wang, Y.; Wu, Y.; Xu, J.; Yu, Y.; Shang, Y. Thrombocytopenia and its association with mortality in patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1469–1472. [Google Scholar] [CrossRef] [PubMed]
- Ranucci, M.; Ballotta, A.; Di Dedda, U.; Bayshnikova, E.; Poli, M.D.; Resta, M.; Falco, M.; Albano, G.; Menicanti, L. The procoagulant pattern of patients with COVID-19 acute respiratory distress syndrome. J. Thromb. Haemost. 2020, 18, 1747–1751. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Yan, X.; Fan, Q.; Liu, H.; Liu, X.; Liu, Z.; Zhang, Z. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19. J. Thromb Haemost. 2020, 18, 1324–1329. [Google Scholar] [CrossRef]
- Favaloro, E.J.; Lippi, G. Recommendations for Minimal Laboratory Testing Panels in Patients with COVID-19: Potential for Prognostic Monitoring. Semin. Thromb. Hemost. 2020, 46, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Cui, S.; Chen, S.; Li, X.; Liu, S.; Wang, F. Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 1421–1424. [Google Scholar] [CrossRef]
- Klok, F.A.; Kruip, M.; Van Der Meer, N.; Arbous, M.; Gommers, D.; Kant, K.; Kaptein, F.; Van Paassen, J.; Stals, M.; Huisman, M.; et al. Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-19: An updated analysis. Thromb. Res. 2020, 191, 148–150. [Google Scholar] [CrossRef]
- Lodigiani, C.; Iapichino, G.; Carenzo, L.; Cecconi, M.; Ferrazzi, P.; Sebastian, T.; Kucher, N.; Studt, J.-D.; Sacco, C.; Bertuzzi, A.; et al. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb. Res. 2020, 191, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Llitjos, J.-F.; Leclerc, M.; Chochois, C.; Monsallier, J.-M.; Ramakers, M.; Auvray, M.; Merouani, K. High incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. J. Thromb. Haemost. 2020, 18, 1743–1746. [Google Scholar] [CrossRef] [PubMed]
- Hasan, S.S.; Radford, S.; Kow, C.S.; Zaidi, S.T.R. Venous thromboembolism in critically ill COVID-19 patients receiving prophylactic or therapeutic anticoagulation: A systematic review and meta-analysis. J. Thromb. Thrombolysis 2020, 50, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Wichmann, D.; Sperhake, J.-P.; Lütgehetmann, M.; Steurer, S.; Edler, C.; Heinemann, A.; Heinrich, F.; Mushumba, H.; Kniep, I.; Schröder, A.S.; et al. Autopsy Findings and Venous Thromboembolism in Patients With COVID-19: A prospective cohort study. Ann. Intern. Med. 2020, 173, 268–277. [Google Scholar] [CrossRef]
- Sadegh Beigee, F.; Pourabdollah Toutkaboni, M.; Khalili, N.; Nadji, S.A.; Dorudinia, A.; Rezaei, M.; Askari, E.; Farzanegan, B.; Marjani, M.; Rafiezadeh, A. Diffuse alveolar damage and thrombotic microangiopathy are the main histopathological findings in lung tissue biopsy samples of COVID-19 patients. Pathol Res. Pr. 2020, 216, 153228. [Google Scholar] [CrossRef]
- Escher, R.; Breakey, N.; Lammle, B. Severe COVID-19 infection associated with endothelial activation. Thromb Res. 2020, 190, 62. [Google Scholar] [CrossRef]
- Connors, J.M.; Levy, J.H. COVID-19 and its implications for thrombosis and anticoagulation. Blood 2020, 135, 2033–2040. [Google Scholar] [CrossRef]
- Makatsariya, A.D.; Slukhanchuk, E.V.; Bitsadze, V.O.; Khizroeva, J.K.; Tretyakova, M.V.; Tsibizova, V.I.; Elalamy, I.; Gris, J.-C.; Grandone, E.; Makatsariya, N.A.; et al. Thrombotic microangiopathy, DIC-syndrome and COVID-19: Link with pregnancy prothrombotic state. J. Matern. Neonatal Med. 2020, 2020, 1–9. [Google Scholar] [CrossRef]
- Levi, M.; Thachil, J. Coronavirus Disease 2019 Coagulopathy: Disseminated Intravascular Coagulation and Thrombotic Microangiopathy—Either, Neither, or Both. Semin. Thromb. Hemost. 2020, 46, 781–784. [Google Scholar] [CrossRef]
- Scully, M.; Cataland, S.; Coppo, P.; De La Rubia, J.; Friedman, K.D.; Hovinga, J.A.K.; Lämmle, B.; Matsumoto, M.; Pavenski, K.; Sadler, E.; et al. Consensus on the standardization of terminology in thrombotic thrombocytopenic purpura and related thrombotic microangiopathies. J. Thromb. Haemost. 2017, 15, 312–322. [Google Scholar] [CrossRef]
- George, J.N.; Nester, C.M. Syndromes of thrombotic microangiopathy. N. Engl. J. Med. 2014, 371, 654–666. [Google Scholar] [CrossRef]
- Kremer Hovinga, J.A.; Zeerleder, S.; Kessler, P.; Romani de Wit, T.; van Mourik, J.A.; Hack, C.E.; ten Cate, H.; Reitsma, P.H.; Wuillemin, W.A.; Lämmle, B. ADAMTS-13, von Willebrand factor and related parameters in severe sepsis and septic shock. J. Thromb. Haemost. 2007, 5, 2284–2290. [Google Scholar] [CrossRef]
- Lassnigg, A.; Schmid, E.R.; Hiesmayr, M.; Falk, C.; Druml, W.; Bauer, P.; Schmidlin, D. Impact of minimal increases in serum creatinine on outcome in patients after cardiothoracic surgery: Do we have to revise current definitions of acute renal failure? Crit. Care Med. 2008, 36, 1129–1137. [Google Scholar] [CrossRef]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; A Molitoris, B.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef]
- Taylor, F.B.; Toh, C.H.; Hoots, W.K.; Wada, H.; Levi, M. Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb. Haemost. 2001, 86, 1327–1330. [Google Scholar] [CrossRef]
- Kokame, K.; Nobe, Y.; Kokubo, Y.; Okayama, A.; Miyata, T. FRETS-VWF73, a first fluorogenic substrate for ADAMTS13 assay. Br. J. Haematol. 2005, 129, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Kremer Hovinga, J.A.; Mottini, M.; Lammle, B. Measurement of ADAMTS-13 activity in plasma by the FRETS-VWF73 assay: Comparison with other assay methods. J. Thromb. Haemost. 2006, 4, 1146–1148. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; Thachil, J.; Iba, T.; Levy, J.H. Coagulation abnormalities and thrombosis in patients with COVID-19. Lancet Haematol. 2020, 7, e438–e440. [Google Scholar] [CrossRef]
- Jhaveri, K.D.; Meir, L.R.; Chang, B.S.F.; Parikh, R.; Wanchoo, R.; Barilla-LaBarca, M.L.; Bijol, V.; Hajizadeh, N. Thrombotic microangiopathy in a patient with COVID-19. Kidney Int. 2020, 98, 509–512. [Google Scholar] [CrossRef]
- Sweeney, J.M.; Barouqa, M.; Krause, G.J.; Gonzalez-Lugo, J.D.; Rahman, S.; Gil, M.R. Evidence for secondary thrombotic microangiopathy in COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H.; Connors, J.M.; Warkentin, T.E.; Thachil, J.; Levi, M. The unique characteristics of COVID-19 coagulopathy. Crit. Care 2020, 24, 1–8. [Google Scholar] [CrossRef]
- Levi, M.; Hunt, B.J. Thrombosis and coagulopathy in COVID-19: An illustrated review. Res. Pr. Thromb. Haemost. 2020, 4, 744–751. [Google Scholar] [CrossRef]
- Kusadasi, N.; Sikma, M.; Huisman, A.; Westerink, J.; Maas, C.; Schutgens, R. A Pathophysiological Perspective on the SARS-CoV-2 Coagulopathy. Hemasphere 2020, 4, e457. [Google Scholar] [CrossRef]
- Iba, T.; Connors, J.M.; Levy, J.H. The coagulopathy, endotheliopathy, and vasculitis of COVID-19. Inflamm. Res. 2020, 69, 1181–1189. [Google Scholar] [CrossRef]
- Lippi, G.; Favaloro, E.J. D-dimer is Associated with Severity of Coronavirus Disease 2019: A Pooled Analysis. Thromb. Haemost. 2020, 120, 876–878. [Google Scholar] [CrossRef]
- Han, H.; Yang, L.; Liu, R.; Liu, F.; Wu, K.L.; Li, J.; Liu, X.; Zhu, C. Prominent changes in blood coagulation of patients with SARS-CoV-2 infection. Clin Chem Lab. Med. 2020, 58, 1116–1120. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Elalamy, I.; Kastritis, E.; Sergentanis, T.N.; Politou, M.; Psaltopoulou, T.; Gerotziafas, G.; Dimopoulos, M.-A. Hematological findings and complications of COVID-19. Am. J. Hematol. 2020, 95, 834–847. [Google Scholar] [CrossRef] [PubMed]
- Al-Samkari, H.; Karp Leaf, R.S.; Dzik, W.H.; Carlson, J.C.; Fogerty, A.E.; Waheed, A.; Goodarzi, K.; Bendapudi, P.K.; Bornikova, L.; Gupta, S.; et al. COVID and Coagulation: Bleeding and Thrombotic Manifestations of SARS-CoV2 Infection. Blood 2020, 136, 486–500. [Google Scholar] [CrossRef] [PubMed]
- Gando, S.; Levi, M.; Toh, C.H. Disseminated intravascular coagulation. Nat. Rev. Dis Primers 2016, 2, 16037. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H.; Wada, H.; Thachil, J.; Warkentin, T.E.; Levi, M.; The Subcommittee on Disseminated Intravascular Coagulation. Differential diagnoses for sepsis-induced disseminated intravascular coagulation: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2019, 17, 415–419. [Google Scholar] [CrossRef]
- Fogarty, H.; Townsend, L.; Ni Cheallaigh, C.; Bergin, C.; Martin-Loeches, I.; Browne, P.; Bacon, C.L.; Gaule, R.; Gillett, A.; Byrne, M.; et al. COVID19 coagulopathy in Caucasian patients. Br. J. Haematol. 2020, 189, 1044–1049. [Google Scholar] [CrossRef]
- Langer, F.; Kluge, S.; Klamroth, R.; Oldenburg, J. Coagulopathy in COVID-19 and Its Implication for Safe and Efficacious Thromboprophylaxis. Hämostaseologie 2020, 40, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Warkentin, T.E.; Thachil, J.; Levi, M.; Levy, J.H. Proposal of the Definition for COVID-19-Associated Coagulopathy. J. Clin. Med. 2021, 10, 191. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, N.; Montagnana, M.; Pizzolo, F.; Friso, S.; Salvagno, G.L.; Forni, G.L.; Gianesin, B.; Morandi, M.; Lunardi, C.; Lippi, G.; et al. A relative ADAMTS13 deficiency supports the presence of a secondary microangiopathy in COVID 19. Thromb. Res. 2020, 193, 170–172. [Google Scholar] [CrossRef] [PubMed]
- Airoldi, A.; Perricone, G.; De Nicola, S.; Molisano, C.; Tarsia, P.; Belli, L. COVID-19-related thrombotic microangiopathy in a cirrhotic patient. Dig. Liver Dis. 2020, 52, 946. [Google Scholar] [CrossRef] [PubMed]
- Diorio, C.; McNerney, K.O.; Lambert, M.; Paessler, M.; Anderson, E.M.; Henrickson, S.E. Evidence of thrombotic microangiopathy in children with SARS-CoV-2 across the spectrum of clinical presentations. Blood Adv. 2020, 4, 6051–6063. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M.; Benoit, S.W.; de Oliveira, M.H.S.; Lippi, G.; Favaloro, E.J.; Benoit, J.L. ADAMTS13 activity to von Willebrand factor antigen ratio predicts acute kidney injury in patients with COVID-19: Evidence of SARS-CoV-2 induced secondary thrombotic microangiopathy. Int J. Lab. Hematol. 2020. [Google Scholar] [CrossRef]
- Huisman, A.; Beun, R.; Sikma, M.; Westerink, J.; Kusadasi, N. Involvement of ADAMTS13 and von Willebrand factor in thromboembolic events in patients infected with SARS-CoV-2. Int J. Lab. Hematol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Escher, R.; Breakey, N.; Lämmle, B. ADAMTS13 activity, von Willebrand factor, factor VIII and D-dimers in COVID-19 inpatients. Thromb. Res. 2020, 192, 174–175. [Google Scholar] [CrossRef] [PubMed]
- Kremer Hovinga, J.A.; Coppo, P.; Lammle, B.; Moake, J.L.; Miyata, T.; Vanhoorelbeke, K. Thrombotic thrombocytopenic purpura. Nat. Rev. Dis. Primers 2017, 3, 17020. [Google Scholar] [CrossRef]
- Levi, M.; Scully, M.; Singer, M. The role of ADAMTS-13 in the coagulopathy of sepsis. J. Thromb. Haemost. 2018, 16, 646–651. [Google Scholar] [CrossRef]
- Magro, C.; Mulvey, J.J.; Berlin, D.; Nuovo, G.; Salvatore, S.; Harp, J.; Baxter-Stoltzfus, A.; Laurence, J. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: A report of five cases. Transl. Res. 2020, 220, 1–13. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Dolhnikoff, M.; Duarte-Neto, A.N.; Monteiro, R.A.D.A.; Da Silva, L.F.F.; De Oliveira, E.P.; Saldiva, P.H.N.; Mauad, T.; Negri, E.M. Pathological evidence of pulmonary thrombotic phenomena in severe COVID-19. J. Thromb. Haemost. 2020, 18, 1517–1519. [Google Scholar] [CrossRef] [PubMed]
- Mastellos, D.C.; Da Silva, B.G.P.; Fonseca, B.A.; Fonseca, N.P.; Auxiliadora-Martins, M.; Mastaglio, S.; Ruggeri, A.; Sironi, M.; Radermacher, P.; Chrysanthopoulou, A.; et al. Complement C3 vs C5 inhibition in severe COVID-19: Early clinical findings reveal differential biological efficacy. Clin. Immunol. 2020, 220, 108598. [Google Scholar] [CrossRef] [PubMed]
- Slomka, A.; Kowalewski, M.; Żekanowska, E. Haemostasis in coronavirus disease 2019—lesson from viscoelastic methods: A systematic review. Thromb. Haemost. 2021. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total | Uncomplicated COVID-19 | Complicated COVID-19 | Critical COVID-19 | DIC a |
|---|---|---|---|---|---|
| Number | 65 | 19 | 29 | 17 | 7 |
| Age (years) (IQR) | 69 (57–79) | 64 (39–79) | 74 (60–81) | 66 (53–73) | 76 (55–80) |
| Sex (male/female) | 41/24 (63.1/36.9%) | 10/9 (52.6/47.4%) | 17/12 (58.6/41.4%) | 14/3 (82.4/17.6%) | 7/0 (100/0.0%) |
| BMI (kg/m2) (IQR) b | 27.2 (24.2–33.6) | 26.7 (22.5–32.6) | 29.4 (24.4–33.6) | 27.0 (25.7–33.5) | 27.0 (24.7–29.4) |
| Preexisting comorbidities | |||||
| Arterial Hypertension | 38 (58.5%) | 9 (47.4%) | 9 (31%) | 10 (58.8%) | 6 (85.6%) |
| Diabetes mellitus | 14 (21.5%) | 1 (5.3%) | 8 (27.6%) | 5 (29.4%) | 2 (28.6%) |
| Obesity (BMI ≥30 kg/m2) b | 23/62 (37.1%) | 5/16 (31.1%) | 13/29 (44.8%) | 5/17 (29.4%) | 1/7 (14.3%) |
| Chronic respiratory disease | 11 (16.9%) | 2 (10.5%) | 6 (20.7%) | 3 (17.6%) | 1 (14.3%) |
| Cardiovascular disease | 17 (26.2%) | 5 (26.3%) | 8 (27.6%) | 4 (23.5%) | 3 (42.9%) |
| Cerebrovascular disease | 11 (16.9%) | 2 (10.5%) | 3 (10.3%) | 6 (35.3%) | 1 (14.3%) |
| Terminal renal insufficiency | 2 (3.1%) | 1 (5.3%) | 1 (3.4%) | 0 (0.0%) | 0 (0.0%) |
| Venous thromboembolic history | 4 (6.2%) | 0 (0.0%) | 1 (3.4%) | 3 (17.6%) | 1 (14.3%) |
| Pulmonary Embolism | 1 (1.5%) | 0 (0.0%) | 1 (3.4%) | 0 (0.0%) | 0 (0.0%) |
| Deep vein thrombosis | 4 (6.2%) | 0 (0.0%) | 1 (3.4%) | 3 (17.6%) | 1 (14.3%) |
| Preexisting anticoagulation | |||||
| DOAC | 1 (1.5%) | 0 (0.0%) | 1 (3.4%) | 0 (0.0%) | 1(14.3%) |
| Vitamin K antagonist | 1 (1.5%) | 0 (0.0%) | 0 (0.0%) | 1 (5.9%) | 0 (0.0%) |
| Platelet aggregation inhibitors | 19 (29.2%) | 8 (42.1%) | 7 (24.1%) | 4 (23.5%) | 0 (0.0%) |
| Clinical complications during COVID-19 infection | |||||
| Renal failure | 18 (27.7%) | 0 (0.0%) | 5 (17.2%) | 13 (76.5%) | 4 (57.1%) |
| AKIN 1 | 3 (4.6%) | 0 (0.0%) | 2 (6.9%) | 1 (5.9%) | 0 (0.0%) |
| AKIN 3 | 15 (23.1%) | 0 (0.0%) | 3 (10.3%) | 12 (70.6%) | 4 (57.1%) |
| Thromboembolic events | 4 (6.2%) | 1 (5.3%) | 0 (0.0%) | 3 (17.6%) | 1 (14.3%) |
| Acute coronary syndrome | 3 (4.6%) | 0 (0.0%) | 2 (6.9%) | 1 (5.9%) | 1 (14.3%) |
| Myocarditis | 2 (3.1%) | 2 (3.1%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Medical care during COVID-19 infection | |||||
| Hospitalized | 63 (96.9%) | 17 (89.5%) | 29 (100%) | 17 (100%) | 7 (100%) |
| Intensive care | 20 (30.8%) | 0 (0.0%) | 3 (10.3%) | 17 (100%) | 4 (57.1%) |
| Oxygen supplementation | 46 (70.8%) | - | 29 (100%) | 17 (100%) | 7 (100%) |
| Invasive ventilation | 17 (26.2%) | - | - | 17 (100%) | 4 (57.1%) |
| Renal replacement therapy | 10 (15.4%) | 0 (0.0%) | 0 (0.0%) | 10 (58.8%) | 3 (42.9%) |
| Anticoagulation during COVID-19 infection | |||||
| None | 7 (10.8%) | 5 (26.3%) | 2 (6.9%) | 0 (0.0%) | 1 (14.3%) |
| Prophylactic dose LMWH | 43 (66.2%) | 13 (68.4%) | 25 (86.2%) | 5 (29.4%) | 2 (28.6%) |
| Therapeutic dose LMWH | 14 (21.5%) | 1 (5.3%) | 1 (3.4%) | 12 (70.6%) | 3 (42.9%) |
| DOAC | 1 (1.5%) | 0 (0.0%) | 1 (3.4%) | 0 (0.0%) | 1 (14.3%) |
| Clinical outcome of COVID-19 infection | |||||
| Uncomplicated | 19 (29.2%) | 19 (100%) | - | - | 0 (0.0%) |
| Complicated | 29 (44.6%) | - | 29 (100%) | - | 3 (42.9%) |
| Critical | 17 (26.2%) | - | - | 17 (100%) | 4 (57.1%) |
| Deceased | 9 (13.8%) | 0 (0%) | 3 (10.3%) | 6 (35.3%) | 3 (42.9%) |
| Parameter | Total | Uncomplicated COVID-19 | Complicated COVID-19 | Critical COVID-19 | DIC a | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number of Patients | 65 | # | 19 | # | 29 | # | 17 | # | 7 | # |
| LDHmax (U/L) | 507 (381–705) | 63 | 421 (345–476) | 17 | 495 (367–593) | 29 | 705 (629–786) | 17 | 832 (641–1849) | 7 |
| ASTmax (U/L) | 76 (46–187) | 63 | 49 (35–76) | 19 | 69 (47–110) | 28 | 206 (103–394) | 16 | 188 (93–229) | 6 |
| ALTmax (U/L) | 51 (33–1429) | 64 | 41 (31–66) | 18 | 43 (28–69) | 29 | 156 (75–395) | 17 | 111 (22–927) | 7 |
| GGTmax (U/L) | 87 (43–180) | 63 | 58 (39–140) | 18 | 66 (3–113) | 28 | 526 (145–988) | 17 | 149 (44–988) | 7 |
| Total bilirubinmax (mg/dl) | 0.8 (0.6–1.4) | 64 | 0.7 (0.5–0.8) | 18 | 0.7 (0.6–0.9) | 29 | 2.5 (1.4–3.3) | 17 | 2.8 (1.5–7.0) | 7 |
| Albuminmin (g/L) | 26 (20–32) | 58 | 30 (25–35) | 17 | 28 (24–33) | 28 | 12 (11–16) | 13 | 16 (10–22) | 7 |
| CKmax (U/L) | 301 (97–798) | 62 | 161 (76–303) | 19 | 226 (77–490) | 26 | 1359 (768–2616) | 17 | 480 (154–2357) | 7 |
| TNImax (pg/mL) | 18.7 (10.6–89.3) | 61 | 16.8 (5.8–56.5) | 19 | 15.8 (6.6–21.2) | 25 | 89.3 (35.3–421) | 17 | 70.7 (15.8–421) | 7 |
| Creatininemax (mg/dL) | 1.2 (0.93–2.1) | 64 | 0.96 (0.74–1.18) | 19 | 1.21 (0.90–1.64) | 28 | 2.16 (1.64–3.33) | 17 | 2.16 (1.56–4.35) | 7 |
| Hemoglobinmin (g/dL) | 10.3 (8.0–12.5) | 65 | 11.8 (7.6–13.6) | 19 | 11.5 (10.3–12.6) | 29 | 7.4 (7.0–8.4) | 17 | 8.0 (6.7–11.4) | 7 |
| Platelet countmin/nL | 178 (134–227) | 65 | 184 (134–233) | 19 | 185 (142–233) | 29 | 170 (133–183) | 17 | 71 (49–160) | 7 |
| Absolute leukocytesmax/nL | 7.6 (5.4–9.7) | 62 | 6.72 (4.6–8.3) | 18 | 7.0 (5.6–9.5) | 29 | 9.2 (7.3–11.4) | 15 | 8.0 (6.0–17.3) | 7 |
| Absolute neutrophilesmax/nL | 5.7 (3.5–8.7) | 62 | 4.5 (3.0–6.9) | 18 | 5.4 (3.9–7.8) | 29 | 8.1 (5.1–10.0) | 15 | 5.8 (4.6–13.8) | 7 |
| Absolute lymphocytesmin/nL | 0.7 (0.5–1.0) | 62 | 0.9 (0.6–1.4) | 18 | 0.6 (0.5–1.0) | 29 | 0.6 (0.5–0.8) | 15 | 0.6 (0.4–0.9) | 7 |
| CRPmax (mg/lL) | 172 (83–285) | 65 | 118 (39–176) | 19 | 121 (48–184) | 29 | 385 (348–413) | 17 | 348 (176–458) | 7 |
| PCTmax (ng/mL) | 0.18 (0.05–1.20) | 65 | 0.05 (0.02–0.24) | 19 | 0.08 (0.05–0.24) | 29 | 4.30 (1.0–11.0) | 17 | 7.00.(0.77–17.0) | 7 |
| INRmax | 1.2 (1.1–1.5) | 65 | 1.2 (1.1–1.3) | 19 | 1.2 (1.1–1.3) | 29 | 1.6 (1.5–2.2) | 17 | 2.6 (1.5–3.6) | 7 |
| Fibrinogenmax (mg/dL) | 586 (476–759) | 58 | 518 (479–582) | 16 | 495 (442–610) | 25 | 855 (730–897) | 17 | 586 (517–890) | 7 |
| Fibrinogenmin (mg/dL) | 465 (358–531) | 58 | 428 (287–505) | 16 | 474 (389–561) | 25 | 469 (364–531) | 17 | 371 (284–453) | 7 |
| D-dimermax (mg/L) | 1.67 (0.86–5.08) | 65 | 1.12 (0.51–1.93) | 19 | 1.14 (0.69–2.27) | 29 | 6.16 (4.36–17.23) | 17 | 7.07 (2.24–40.24) | 7 |
| Parameters of DIC Score | Points | Number of Patients (%) | |
|---|---|---|---|
| Meeting the ISTH Criteria of Overt DIC (total points ≥5) a | 7 (100) | ||
| Platelets | >100/nL | 0 | 3 (42.8) |
| 50–100/nL | 1 | 2 (28.6) | |
| <50/nL | 2 | 2 (28.6) | |
| D-dimer | normal (<0.5 mg/L) | 0 | 0 (0) |
| moderately elevated (0.5–2.0 mg/L) | 2 | 1 (14.3) | |
| extremely elevated (>2.0 mg/L) | 3 | 6 (85.7) | |
| INR | <1.25 | 0 | 0 (0) |
| 1.25–1.7 | 1 | 2 (28.6) | |
| >1.7 | 2 | 5 (71.4) | |
| Fibrinogen | ≥100 mg/dL | 0 | 7 (100) |
| <100 mg/dL | 1 | 0 (0) | |
| PatID | Timepoint a | Schistocytes [‰] | Haptoglobin [g/L] | Platelet Count [/nL] | Lowest b Platelet Count [/nL] | VWF Activity [%] | VWF Antigen [%] | ADAMTS13 Activity [%] | Ratio VWF:AG/ADAMTS13 Act | PCT [ng/mL] | CRP [mg/L] | Severity of COVID-19 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| normal | Days | <5 | 0.14–2.73 | 150–360 | 150–360 | 40–170 | 42–176 | ≥ 50 | 0.5–2.0 c | <0.5 | <5.0 | |
| 13 | 24 | 3 | 0.22 | 309 | 173 | n.m. | n.m. | 48.0 | 1.1 | 89 | cr (+DIC) | |
| 29 | 2 | Negative | 2.22 | 208 | 184 | 170 | 209 | 64.0 | 3.3 | 0.03 | 7.3 | uc |
| 36 | 1 | Negative | 4.15 | 293 | 293 | 344 | 396 | 55.8 | 7.1 | 0.15 | 151 | co |
| 40 | 2 | Negative | 2.96 | 341 | 179 | >390 | 654 | 75.4 | 8.7 | 0.06 | 31 | uc |
| 41 | 1 | Negative | 1.52 | 437 | 401 | 170 | 218 | 75.1 | 2.9 | 0.03 | 26 | co |
| 44 | 0 | 1 | 2.55 | 85 | 85 | >390 | 511 | 31.2 | 16.4 | 3.9 | 254 | uc |
| 44 | 1 | 5 | 2.44 | 106 | 85 | >390 | 458 | 40.7 | 11.3 | 2.9 | 156 | uc |
| 45 | 1 | Negative | 3.33 | 165 | 165 | 246 | 253 | 64.3 | 3.9 | 0.4 | 204 | uc |
| 48 | 2 | Negative | 4.25 | 305 | 275 | 328 | 409 | 71.6 | 5.7 | 0.12 | 186 | co |
| 52 | 1 | Negative | 3.51 | 682 | 597 | 158 | 218 | 63.5 | 3.4 | 0.04 | 37 | co |
| 55 | 14 | Negative | 2.96 | 224 | 193 | 329 | 221 | 85.4 | 2.6 | 0.12 | 46 | cr |
| 56 | 1 | Negative | 1.76 | 227 | 227 | 188 | 199 | 85.4 | 2.3 | 0.03 | 109 | uc |
| 58 | 1 | Negative | 1.79 | 250 | 200 | >390 | 782 | 46.0 | 17.0 | 3.5 | 184 | co |
| 59 | 0 | 9 | 3.31 | 240 | 213 | 336 | 226 | 88.5 | 2.6 | 0.02 | 32 | uc |
| 70 | 9 | Negative | 1.44 | 392 | 187 | 215 | 228 | 80.0 | 2.9 | 0.05 | 15 | uc |
| 73 | 0 | Negative | 1.71 | 254 | 254 | 178 | 202 | 97.8 | 2.1 | <0.02 | 0.79 | uc |
| 74 | 44 | Negative | 2.52 | 54 | 54 | >390 | 595 | 17.8 | 33.4 | 6.8 | 325 | cr (+DIC) |
| 77 | 15 | Negative | 3.81 | 245 | 119 | >390 | 613 | 90.9 | 6.7 | 0.12 | 32 | uc |
| 78 | 1 | Negative | 3.51 | 186 | 159 | 361 | 222 | 85.4 | 2.6 | 0.23 | 179 | uc |
| 79+ | 1 | Negative | 5.45 | 220 | 49 | >390 | 602 | 76.4 | 7.9 | 0.31 | 155 | cr (+DIC) |
| 81+ | 0 | n. m. | n.m. | 345 | 160 | 267 | 234 | 87.0 | 2.7 | 0.28 | 169 | cr (+DIC) |
| 84 | 0 | Negative | 4.21 | 759 | 759 | 263 | 231 | 71.8 | 3.2 | 0.24 | 138 | uc |
| 85 | 1 | Negative | 3.30 | 238 | 238 | 162 | 195 | 84.8 | 2.3 | 0.03 | 39 | Uc |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Falter, T.; Rossmann, H.; Menge, P.; Goetje, J.; Groenwoldt, S.; Weinmann, A.; Sivanathan, V.; Schulz, A.; Lemmermann, N.A.W.; Danckwardt, S.; et al. No Evidence for Classic Thrombotic Microangiopathy in COVID-19. J. Clin. Med. 2021, 10, 671. https://doi.org/10.3390/jcm10040671
Falter T, Rossmann H, Menge P, Goetje J, Groenwoldt S, Weinmann A, Sivanathan V, Schulz A, Lemmermann NAW, Danckwardt S, et al. No Evidence for Classic Thrombotic Microangiopathy in COVID-19. Journal of Clinical Medicine. 2021; 10(4):671. https://doi.org/10.3390/jcm10040671
Chicago/Turabian StyleFalter, Tanja, Heidi Rossmann, Philipp Menge, Jan Goetje, Steffen Groenwoldt, Arndt Weinmann, Visvakanth Sivanathan, Andreas Schulz, Niels A.W. Lemmermann, Sven Danckwardt, and et al. 2021. "No Evidence for Classic Thrombotic Microangiopathy in COVID-19" Journal of Clinical Medicine 10, no. 4: 671. https://doi.org/10.3390/jcm10040671
APA StyleFalter, T., Rossmann, H., Menge, P., Goetje, J., Groenwoldt, S., Weinmann, A., Sivanathan, V., Schulz, A., Lemmermann, N. A. W., Danckwardt, S., Lackner, K. J., Galle, P. R., Scharrer, I., Lämmle, B., & Sprinzl, M. F. (2021). No Evidence for Classic Thrombotic Microangiopathy in COVID-19. Journal of Clinical Medicine, 10(4), 671. https://doi.org/10.3390/jcm10040671