Abstract
Sleep disorders and primary headaches are frequent health problems in childhood, and they are often comorbid in an individual, linked by a mutual and complex relationship. This comorbidity is frequent and well-documented, but the available literature is usually biased in favor of one aspect or another, mainly depending on the expertise of the authors. The aim of this paper is to review existing literature on the diagnostic assessment of comorbid primary headaches and sleep disorders, so as to propose practical suggestions to accurately investigate the presence of comorbid conditions in children evaluated for primary headaches or for sleep disorders.
1. Introduction
Sleep disorders and headaches are frequent health problems in childhood, with primary headaches occurring in 12% of the pediatric population [1] and with 24% of children experiencing at least one type of sleep problem [2]. Sleep disturbances and headaches are often comorbid in an individual, and they are linked by a mutual and complex relationship. Headaches might be a consequence of disrupted sleep, with sleep alterations acting as trigger factors for attacks, especially in subjects who suffer migraines. Sleep disorders might also increase the severity of attacks and favor chronicization [3]. Furthermore, the circadian phenotype and the quality of sleep can influence migraine characteristics [4,5]. Inversely, headaches can also cause sleep problems, especially when nocturnal attacks interrupt sleep [6]. The high comorbidity rate between sleep disorders and headaches might indicate different underlying reasons. First, the alteration of the serotoninergic system, involved both in nociception and sleep regulation, might play a role [7]. Furthermore, both disorders could represent an expression of a common pathogenic process, with common cerebral structures and signaling pathways (including the hypothalamus, raphe nuclei, and serotoninergic system) involved in both sleep and migraines [6,8,9,10]. This complex correlation between headache and sleep disturbances related to common neurophysiological processes has important implications for the treatment of both conditions. In fact, drugs used in the treatment of primary headache can influence the physiology of sleep, as well as the treatment of sleep disorders, either with behavioral or pharmacological approach, can significantly improve migraine [11,12]. Last, common risk factors such as mood and anxiety disorders, related to both headaches and sleep disturbances, might increase the risk of this comorbidity [13]. Due to this complex and mutual relationship, a correct assessment of both disorders is necessary for planning an individualized treatment strategy addressing sleep disorders and headaches at the same time, thus ameliorating the quality of life of patients. Although this comorbidity is frequent and well-documented, the available literature is usually biased in favor of one aspect or another, mainly depending on the expertise of the authors. Several studies rigorously assessed migraines by following the diagnostic criteria of the International Classification of Headache Disorders (ICHD), but sleep disorders are poorly documented. Conversely, there are some studies focused on sleep disorders that use standardized sleep questionnaires or neurophysiologic studies, but the diagnosis of migraine diagnosis is not accurate [14,15,16].
The aim of this paper is to review existing literature on the diagnostic assessment of comorbid primary headaches and sleep disorders, so as to make practical suggestions for accurately investigating the presence of comorbid conditions in children evaluated for primary headaches or for sleep disorders.
2. Materials and Methods
The results of this review are reported according to the preferred reporting items for reviews and meta-analyses (PRISMA) and adhere to a structured review protocol [17]. To establish the research question, the PICO-model PICOS [18] (Patient, Intervention, Comparison, Outcome), according to the PRISMA guidelines was used: Patient: children with sleep disorders and primary headache, Intervention: review existing literature on the diagnostic assessment of comorbid primary headache and sleep disorders, Comparison: n.a., Outcome: propose some practical suggestion to accurately investigate the presence of comorbid conditions in children evaluated for primary headache or for sleep disorders.
Search Strategy and Article Selection
Two authors (A.O. and E.T.) performed a comprehensive search of four databases, PubMed, Embase, Cochrane, and Web of Science, using the following search strategy: “primary headache” OR “migraine” OR, AND “sleep” OR “sleep disorders” OR “sleep disturbance” OR, AND “diagnosis”.
Studies were initially included if they:
- (1)
- Involved individuals with headaches and sleep disorders;
- (2)
- Involved children and adolescents up to 18 years of age;
- (3)
- Reported the diagnostic evaluation methods for headaches and sleep disorders;
- (4)
- Were written in English;
- (5)
- Were published within 10 years of the search date (January 2010–December 2020), which was considered a sufficient period to capture publications with the most reliable, appropriate, and up-to-date diagnostic procedures.
We excluded:
- (1)
- Review articles, case reports, letters, metanalysis, and books
- (2)
- Treatment studies (both pharmacological and non-pharmacological);
- (3)
- Studies in which subjects presented other neurological disorders, such as epilepsy, or wherein the presence of headaches was addressed chiefly as a symptom in the context of other general medical conditions, or that dealt with neurodevelopmental disorders such as children with intellectual disability, borderline intellectual disability, psychiatric disorders, attention deficit hyperactivity disorder (ADHD), and tics;
- (4)
- Sleep disorders secondary to nocturnal enuresis;
- (5)
- Studies that relied exclusively on neurophysiological methods, since these are recognized and valid methods to study sleep characteristics but represent second-step investigations, as they are not used in the daily clinical practices.
Two authors (A.O. and E.T.) independently screened all the titles and abstracts of studies identified by the initial search. The full text of an article was obtained when either reviewer thought that it might fulfill the inclusion criteria. When there was uncertainty regarding the inclusion of a publication, three additional authors were consulted (M.A.N.F., R.M., and M.V.).
Full articles were reviewed for relevance and articles were excluded if they did not include data relating to the diagnostic methods applied to evaluate the presence of sleep disorders and/or headaches.
3. Results
After the initial identification of 120 papers, for the final analysis, we selected 13 manuscripts that fulfilled our inclusion criteria (Figure 1).
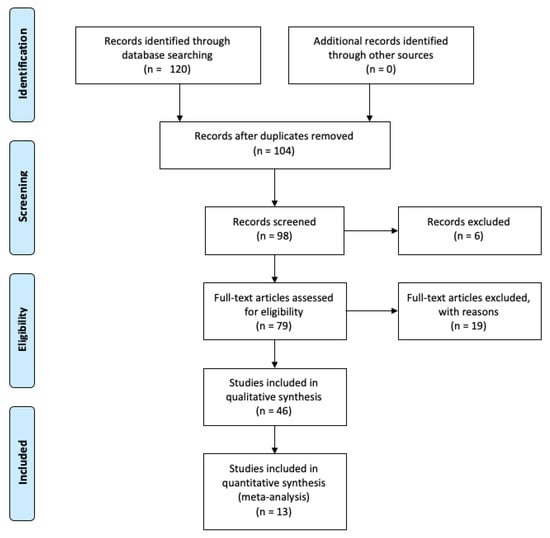
Figure 1.
PRISMA flow diagram.
Table 1 shows the main characteristics of all the studies selected for drafting this review.

Table 1.
Main characteristics of all studies selected for drafting this review.
Overall, these articles reported the results involving 14,674 subjects aged 5–18 years.
Of the 13 included studies of primary headaches, 11 diagnosed according to ICHD criteria, while the remaining 2 papers used self-diagnosis tools reports [19] or country-specific diagnostic criteria [10]. Included as primary headaches were migraines with (MwA) and without auras (MwoA), chronic migraines (CM), tension-type headaches (TTH), new daily persistent headaches (NDPH), and probable migraines (PM).
Several papers included the administration of specific tools used to evaluate the severity of headaches (Table 2), such as the Migraine Disabilities Assessment Scale (MIDAS) [19], Pediatric Migraine Disability Assessment Score (PedMIDAS) [20,21,25], and numerical rating scales (NRS) [10,22].
Table 2.
List of tools used to assess migraine severity in the considered papers, with a brief description.
Large variations were noted in the measures and criteria used to define sleep disorders. None of the manuscripts mentioned the diagnostic criteria of the International Classification of Sleep Disorders (ICSD). However, different studies used validated questionnaires, including the Children’s Sleep Habits Questionnaire (CSHQ) [10,26], Sleep Disturbances Scale for Children (SDSC) [24,28], Pediatric Daytime Sleepiness Scale (PDSS) [28], BEARS Sleep Screening Tool [21], and Sleep Hygiene Inventory for Pediatrics (SHIP) [22,23]. In some studies, other questionnaires, including the Patient-Reported Outcomes Measurement Information System (PROMIS) [19], general lifestyle questionnaire [20], and National Comorbidity Survey-Adolescent (NCS-A) [13], were used (Table 3).
Table 3.
List of tools used to assess sleep disorders in the considered papers, with a brief description.
Different types of sleep disorders emerged: insomnia, disturbances of the sleep–wake rhythm, obstructive sleep apnea syndrome, daytime sleepiness, parasomnia, sleep anxiety, hypersomnia, snoring, co-sleeping, and unspecified sleep disorders.
4. Discussion and Conclusions
This review highlights that most researchers applied the ICHD criteria to reach the diagnosis of primary headache, while none of them mentioned the ICSD criteria. As for sleep, only 7 out of 13 analyzed studies used standardized questionnaires, meaning that in almost half of these papers, sleep was investigated through non-validated methods or with general questionnaires not specifically designed for sleep disorders. Furthermore, even when validated, some sleep questionnaires could not be considered as “fully diagnostic”, since they offered only a screening of sleep problems to be studied in more detail. The BEARS is a rapid, yet not diagnostic, screening tool that is easy to use in everyday clinical practice. Similarly, the SHIP questionnaire was specifically developed to highlight clinical concerns about sleep in patients suffering from primary headaches [23]. Overall, we can conclude that most of the selected articles rigorously analyzed only one aspect of the comorbidity, with sleep often representing the “weak” side of the study.
A prompt and correct diagnosis of this comorbidity is of crucial importance. Only treating headaches in a child who is also presenting a sleep disorder cannot produce good results, leading to the classification of the patient as a “non-responder” to first-line treatments. On the other hand, targeting both disorders at the same time can significantly ameliorate the quality of life of patients (and their families) and reduce all symptoms. A recent study by our group (published after the period considered for this review article) aimed at analyzing the relationship between migraines and sleep in a wide sample of pediatric migraine patients [38]. The study was conducted by administering a standardized questionnaire (CSHQ) to patients presenting a definite diagnosis of migraine according to ICHD-3 criteria. The results confirmed that sleep disorders are a very common complaint in pediatric patients with migraines, affecting about 73% of patients.
Sleep disorders are also included in the “episodic syndromes that may be associated with migraine” and are considered early life expressions of migraine [9,39]. Sleep disorders, such as sleep walking, sleep talking, night terror, and bruxism, are now included in the ICHD-3 classification [40] and considered part of a “migraine syndrome of childhood” [41,42]. Therefore, a correct and precise assessment of symptoms is of crucial importance, and it is worth emphasizing that most sleep disorders are easily assessable through accurate clinical histories and specific questionnaires. In the pediatric age group, it was shown that parental reports are consistent with objective measurements such as actigraphy and polysomnography [43].
In conclusion, this review underlines the paucity of data correctly assessing both headache and sleep disorders, thus leaving this comorbidity often underdiagnosed and there-fore undertreated. These results support the need, in the daily clinical practice, for an ex-tensive clinical history and validated assessments, including validated questionnaires and possibly actigraphy and polysomnography, in children searching medical advice for migraine or sleep disorders in order to be able to detect this comorbidity early, thus de-signing the better treatment strategy for the patient.
Author Contributions
Study design, A.O., M.A.N.F., E.T., M.V., and R.M.; data acquisition, A.O., L.O., M.A.N.F., G.S., F.U., and R.M.; data curation, A.O., M.A.N.F., E.T., M.P.C., M.V., and R.M.; writing original draft preparation, A.O., M.A.N.F., and R.M.; writing review and editing, A.O., M.A.N.F., and R.M.; and supervision, E.T., M.V., and F.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
We received the Institutional Review Board Approval from Bambino Gesù Children’s Hospital.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Abu-Arefeh, I.; Russell, G. Prevalence of Headache and Migraine in Schoolchildren. BMJ 1994, 309, 765–769. [Google Scholar] [CrossRef] [PubMed]
- Owens, J.A.; Witmans, M. Sleep Problems. Curr. Probl. Pediatr. Adolesc. Health Care 2004, 34, 154–179. [Google Scholar] [CrossRef] [PubMed]
- Rains, J.C. Sleep and Migraine: Assessment and Treatment of Comorbid Sleep Disorders. Headache 2018, 58, 1074–1091. [Google Scholar] [CrossRef] [PubMed]
- Viticchi, G.; Falsetti, L.; Paolucci, M.; Altamura, C.; Buratti, L.; Salvemini, S.; Brunelli, N.; Bartolini, M.; Vernieri, F.; Silvestrini, M. Influence of Chronotype on Migraine Characteristics. Neurol. Sci. 2019, 40, 1841–1848. [Google Scholar] [CrossRef] [PubMed]
- Viticchi, G.; Altamura, C.; Falsetti, L.; Buratti, L.; Salvemini, S.; Polidoro, F.; Silvestrini, M.; Vernieri, F.; Bartolini, M. Poor Sleep Quality in Patients Affected by Migraine: A Population Study. Neurol. Sci. 2020, 41, 495–496. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.; Pavlović, J.M. Sleep Disorders and Migraine: Review of Literature and Potential Pathophysiology Mechanisms. Headache 2018, 58, 1030–1039. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, G.; Cevoli, S.; Colavito, D.; Leon, A. Biochemistry of Primary Headaches: Role of Tyrosine and Tryptophan Metabolism. Neurol. Sci. 2015, 36 Suppl 1, 17–22. [Google Scholar] [CrossRef]
- Esposito, M.; Parisi, P.; Miano, S.; Carotenuto, M. Migraine and Periodic Limb Movement Disorders in Sleep in Children: A Preliminary Case-Control Study. J. Headache Pain 2013, 14, 57. [Google Scholar] [CrossRef] [PubMed]
- Miller, V.A.; Palermo, T.M.; Powers, S.W.; Scher, M.S.; Hershey, A.D. Migraine Headaches and Sleep Disturbances in Children. Headache 2003, 43, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Cheraghi, F.; Shamsaei, F.; Fayyazi, A.; Molaaei Yeganeh, F.; Roshanaei, G. Comparison of the Quality of Sleep and Intensity of Headache between Migraine, Tension Headache, and Healthy Children. Iran. J. Child. Neurol. 2018, 12, 45–54. [Google Scholar] [PubMed]
- Guidetti, V.; Dosi, C.; Bruni, O. The Relationship between Sleep and Headache in Children: Implications for Treatment. Cephalalgia 2014, 34, 767–776. [Google Scholar] [CrossRef] [PubMed]
- Nesbitt, A.D.; Leschziner, G.D.; Peatfield, R.C. Headache, Drugs and Sleep. Cephalalgia 2014, 34, 756–766. [Google Scholar] [CrossRef] [PubMed]
- Lateef, T.; Witonsky, K.; He, J.; Ries Merikangas, K. Headaches and Sleep Problems in US Adolescents: Findings from the National Comorbidity Survey—Adolescent Supplement (NCS-A). Cephalalgia 2019, 39, 1226–1235. [Google Scholar] [CrossRef] [PubMed]
- Nita, S.A.; Teleanu, R.I.; Bajenaru, O.A. The Role of Polysomnography in Identifying Sleep Disorders in Children with Migraine. J. Med. Life 2020, 13, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Roccella, M.; Marotta, R.; Operto, F.F.; Smirni, D.; Precenzano, F.; Bitetti, I.; Messina, G.; Sessa, F.; Di Mizio, G.; Loreto, C.; et al. NREM Sleep Instability in Pediatric Migraine Without Aura. Front. Neurol. 2019, 10, 932. [Google Scholar] [CrossRef] [PubMed]
- Vendrame, M.; Kaleyias, J.; Valencia, I.; Legido, A.; Kothare, S.V. Polysomnographic Findings in Children with Headaches. Pediatr. Neurol. 2008, 39, 6–11. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A Comparison Study of Specificity and Sensitivity in Three Search Tools for Qualitative Systematic Reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed]
- Kemper, K.J.; Heyer, G.; Pakalnis, A.; Binkley, P.F. What Factors Contribute to Headache-Related Disability in Teens? Pediatr. Neurol. 2016, 56, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Torres-Ferrus, M.; Vila-Sala, C.; Quintana, M.; Ajanovic, S.; Gallardo, V.J.; Gomez, J.B.; Alvarez-Sabin, J.; Macaya, A.; Pozo-Rosich, P. Headache, Comorbidities and Lifestyle in an Adolescent Population (The TEENs Study). Cephalalgia 2019, 39, 91–99. [Google Scholar] [CrossRef]
- Fonseca, E.; Torres-Ferrús, M.; Gallardo, V.J.; Macaya, A.; Pozo-Rosich, P. Impact of Puberty in Pediatric Migraine: A Pilot Prospective Study. J. Clin. Neurol. 2020, 16, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Rabner, J.; Kaczynski, K.J.; Simons, L.E.; LeBel, A. Pediatric Headache and Sleep Disturbance: A Comparison of Diagnostic Groups. Headache 2018, 58, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Rabner, J.; Kaczynski, K.J.; Simons, L.E.; Lebel, A.A. The Sleep Hygiene Inventory for Pediatrics: Development and Validation of a New Measure of Sleep in a Sample of Children and Adolescents With Chronic Headache. J. Child. Neurol. 2017, 32, 1040–1046. [Google Scholar] [CrossRef]
- Maltese, A.; Salerno, M.; Tripi, G.; Romano, P.; Ricciardi, A.; Di Folco, A.; Di Filippo, T.; Parisi, L. Internalizing problems are related to sleep patterns disordered in children affected by primary headache. Acta Med. Mediterr. 2017, 33, 729–735. [Google Scholar]
- Heyer, G.L.; Rose, S.C.; Merison, K.; Perkins, S.Q.; Lee, J.E.M. Specific Headache Factors Predict Sleep Disturbances among Youth with Migraine. Pediatr. Neurol. 2014, 51, 489–493. [Google Scholar] [CrossRef]
- Abou-Khadra, M.K.; Kishk, N.A.; Shaker, O.G.; Hassan, A. Urinary 6-Sulphatoxymelatonin Levels and Sleep Disorders in Children with Migraine. J. Child. Neurol. 2014, 29, 947–951. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, M.; Pıçakçıefe, M.; Ozge, A.; Palalı, I. Migraine and tension-type headache in schoolchildren in western of turkey. Acta Med. Mediterr. 2013, 29, 419. [Google Scholar]
- Esposito, M.; Roccella, M.; Parisi, L.; Gallai, B.; Carotenuto, M. Hypersomnia in Children Affected by Migraine without Aura: A Questionnaire-Based Case-Control Study. Neuropsychiatr. Dis. Treat. 2013, 9, 289–294. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Carotenuto, M.; Esposito, M.; Precenzano, F.; Castaldo, L.; Roccella, M. Cosleeping in Childhood Migraine. Minerva Pediatr. 2011, 63, 105–109. [Google Scholar]
- Stewart, W.F.; Lipton, R.B.; Dowson, A.J.; Sawyer, J. Development and Testing of the Migraine Disability Assessment (MIDAS) Questionnaire to Assess Headache-Related Disability. Neurology 2001, 56, S20–S28. [Google Scholar] [CrossRef] [PubMed]
- Hershey, A.D.; Powers, S.W.; Vockell, A.L.; LeCates, S.; Kabbouche, M.A.; Maynard, M.K. PedMIDAS: Development of a Questionnaire to Assess Disability of Migraines in Children. Neurology 2001, 57, 2034–2039. [Google Scholar] [CrossRef] [PubMed]
- Walker, B.J.; Polaner, D.M.; Berde, C.B. Acute Pain. In A Practice of Anesthesia for Infants and Children (Sixth Edition); Elsevier, Inc.: Philadelphia, PA, USA, 2019; pp. 1023–1062.e15. [Google Scholar]
- Cella, D.; Riley, W.; Stone, A.; Rothrock, N.; Reeve, B.; Yount, S.; Amtmann, D.; Bode, R.; Buysse, D.; Choi, S.; et al. The Patient-Reported Outcomes Measurement Information System (PROMIS) Developed and Tested Its First Wave of Adult Self-Reported Health Outcome Item Banks: 2005-2008. J. Clin. Epidemiol. 2010, 63, 1179–1194. [Google Scholar] [CrossRef]
- Markovich, A.N.; Gendron, M.A.; Corkum, P.V. Validating the Children’s Sleep Habits Questionnaire Against Polysomnography and Actigraphy in School-Aged Children. Front. Psychiatry 2014, 5, 188. [Google Scholar] [CrossRef]
- Owens, J.A.; Dalzell, V. Use of the “BEARS” Sleep Screening Tool in a Pediatric Residents’ Continuity Clinic: A Pilot Study. Sleep Med. 2005, 6, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Bruni, O.; Ottaviano, S.; Guidetti, V.; Romoli, M.; Innocenzi, M.; Cortesi, F.; Giannotti, F. The Sleep Disturbance Scale for Children (SDSC). Construction and Validation of an Instrument to Evaluate Sleep Disturbances in Childhood and Adolescence. J. Sleep Res. 1996, 5, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Drake, C.; Nickel, C.; Burduvali, E.; Roth, T.; Jefferson, C.; Pietro, B. The Pediatric Daytime Sleepiness Scale (PDSS): Sleep Habits and School Outcomes in Middle-School Children. Sleep 2003, 26, 455–458. [Google Scholar] [PubMed]
- Voci, A.; Bruni, O.; Ferilli, M.A.N.; Papetti, L.; Tarantino, S.; Ursitti, F.; Sforza, G.; Vigevano, F.; Mazzone, L.; Valeriani, M.; et al. Sleep Disorders in Pediatric Migraine: A Questionnaire-Based Study. J. Clin. Med. 2021, 10, 3575. [Google Scholar] [CrossRef]
- Gelfand, A.A. Migraine and Childhood Periodic Syndromes in Children and Adolescents. Curr. Opin. Neurol. 2013, 26, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd Edition. Cephalalgia 2018, 38, 1–211. [CrossRef]
- Abu-Arafeh, I.; Gelfand, A.A. The Childhood Migraine Syndrome. Nat. Rev. Neurol. 2021, 17, 449–458. [Google Scholar] [CrossRef]
- Tarantino, S.; Capuano, A.; Torriero, R.; Citti, M.; Vollono, C.; Gentile, S.; Vigevano, F.; Valeriani, M. Migraine Equivalents as Part of Migraine Syndrome in Childhood. Pediatr. Neurol. 2014, 51, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Bruni, O.; Fabrizi, P.; Ottaviano, S.; Cortesi, F.; Giannotti, F.; Guidetti, V. Prevalence of Sleep Disorders in Childhood and Adolescence with Headache: A Case-Control Study. Cephalalgia 1997, 17, 492–498. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).