
Walking the Line with Ticagrelor: Meta-Analysis Comparing the Safety and Efficacy of Ticagrelor Monotherapy after a Short Course of Ticagrelor-Based Dual Antiplatelet Therapy versus Standard Therapy in Complex Percutaneous Coronary Intervention

 , , , and
, , , and 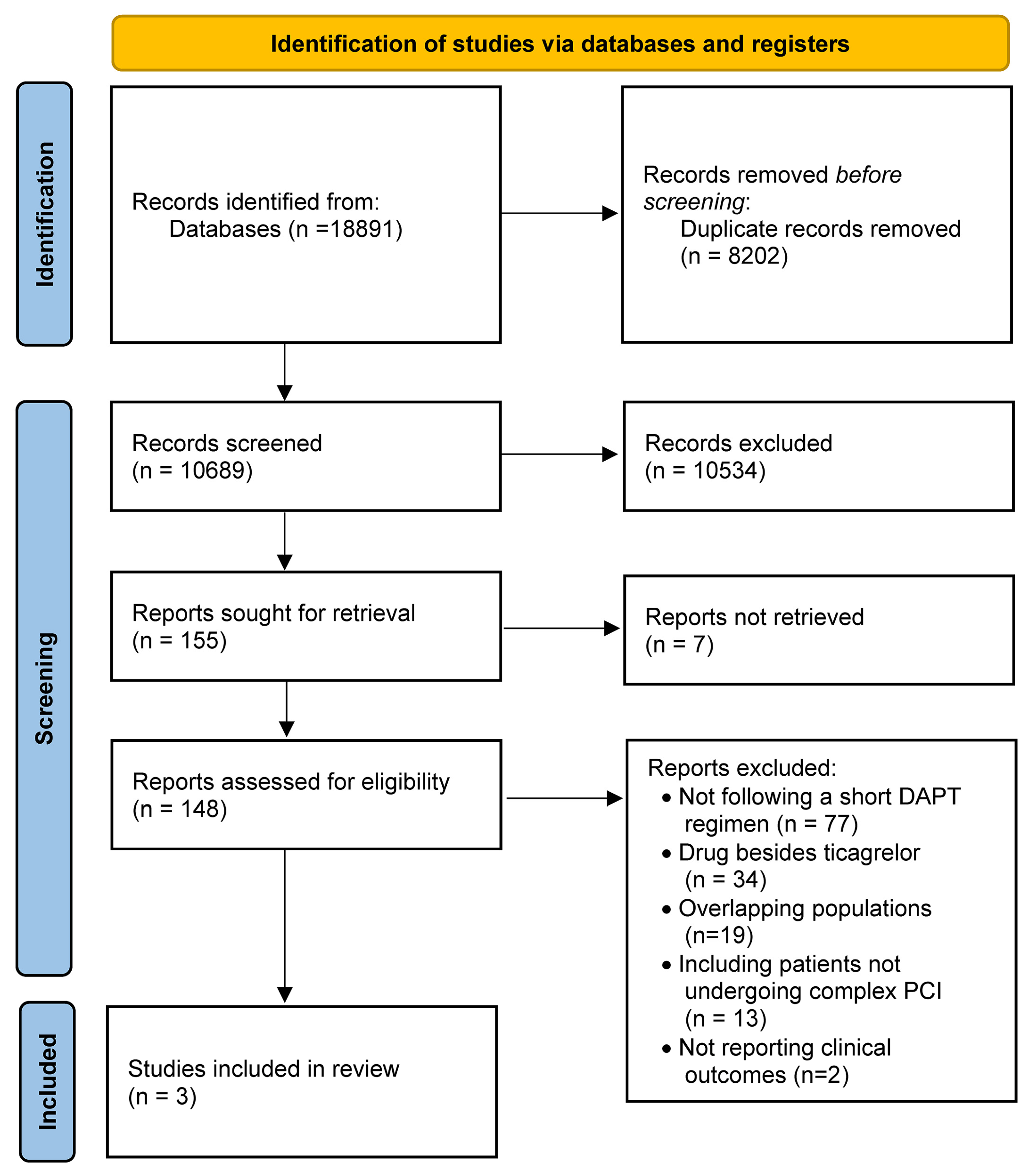{kind=link}
{kind=link}
Abstract
:1. Introduction
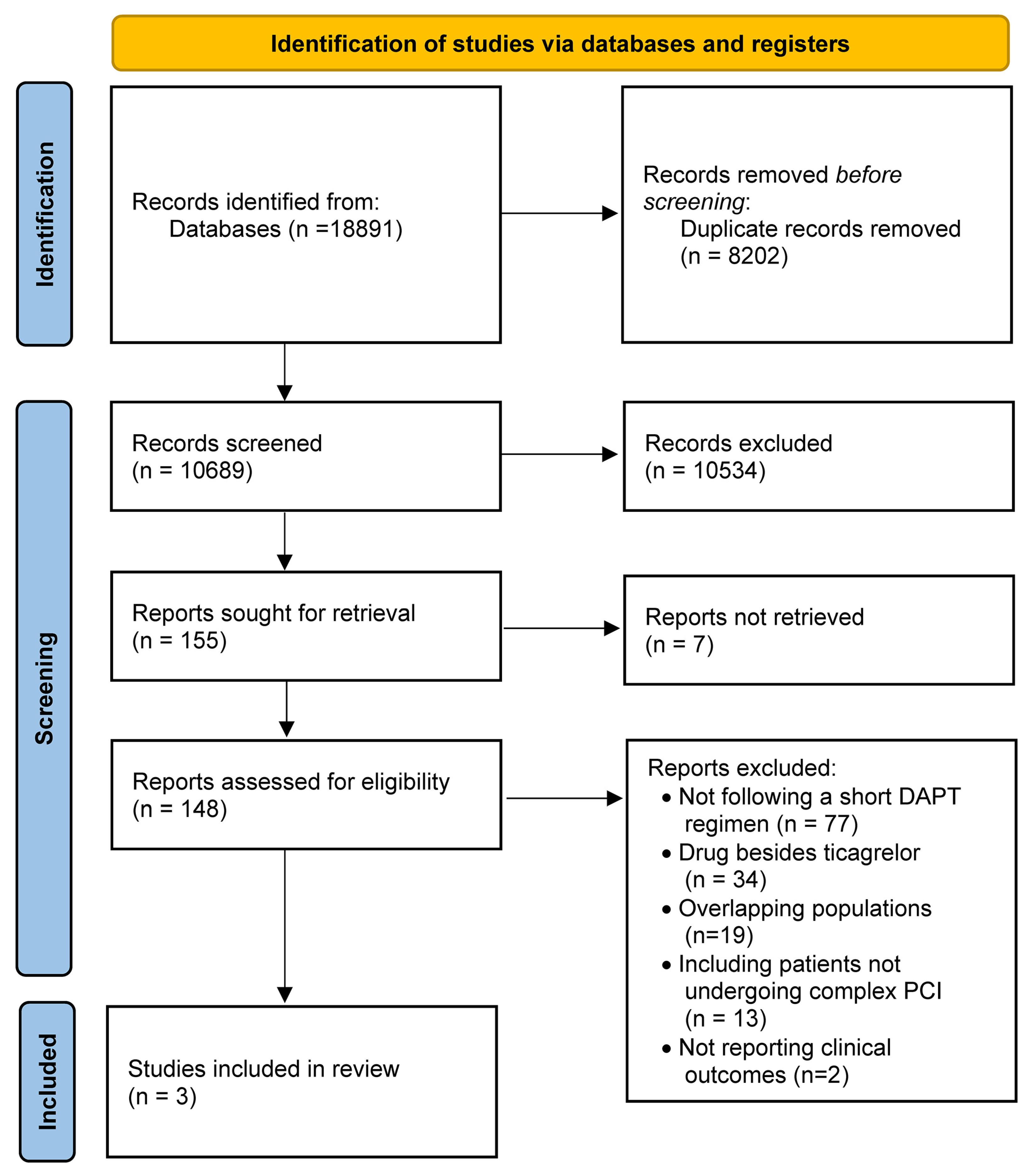
2. Materials and Methods
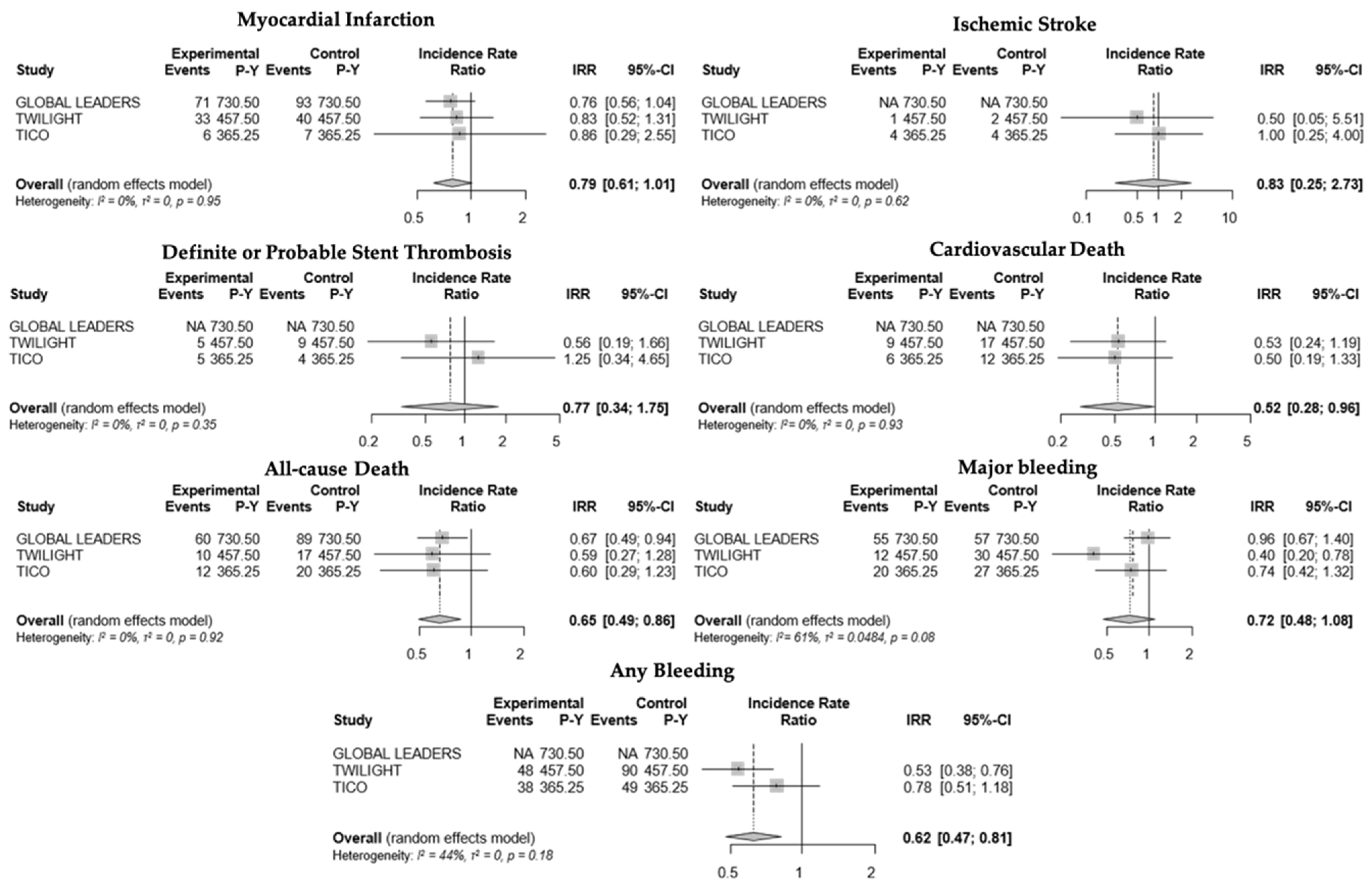
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.-P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC Focused Update on Dual Antiplatelet Therapy in Coronary Artery Disease Developed in Collaboration with EACTS. Eur. Heart J. 2018, 39, 213–260. [Google Scholar] [CrossRef] [PubMed]
- Giustino, G.; Chieffo, A.; Palmerini, T.; Valgimigli, M.; Feres, F.; Abizaid, A.; Costa, R.A.; Hong, M.-K.; Kim, B.-K.; Jang, Y.; et al. Efficacy and Safety of Dual Antiplatelet Therapy after Complex PCI. J. Am. Coll. Cardiol. 2016, 68, 1851–1864. [Google Scholar] [CrossRef] [PubMed]
- Brinza, C.; Burlacu, A.; Tinica, G.; Covic, A.; Macovei, L. A Systematic Review on Bleeding Risk Scores’ Accuracy after Percutaneous Coronary Interventions in Acute and Elective Settings. Healthcare 2021, 9, 148. [Google Scholar] [CrossRef]
- Valgimigli, M.; Mehran, R.; Franzone, A.; da Costa, B.R.; Baber, U.; Piccolo, R.; McFadden, E.P.; Vranckx, P.; Angiolillo, D.J.; Leonardi, S.; et al. Ticagrelor Monotherapy Versus Dual-Antiplatelet Therapy after PCI. JACC Cardiovasc. Interv. 2021, 14, 444–456. [Google Scholar] [CrossRef] [PubMed]
- Giacoppo, D.; Matsuda, Y.; Fovino, L.N.; D’Amico, G.; Gargiulo, G.; Byrne, R.A.; Capodanno, D.; Valgimigli, M.; Mehran, R.; Tarantini, G. Short Dual Antiplatelet Therapy Followed by P2Y12 Inhibitor Monotherapy vs. Prolonged Dual Antiplatelet Therapy after Percutaneous Coronary Intervention with Second-Generation Drug-Eluting Stents: A Systematic Review and Meta-Analysis of Randomized Clinic. Eur. Heart J. 2021, 42, 308–319. [Google Scholar] [CrossRef]
- Généreux, P.; Giustino, G.; Redfors, B.; Palmerini, T.; Witzenbichler, B.; Weisz, G.; Stuckey, T.D.; Maehara, A.; Mehran, R.; Kirtane, A.J.; et al. Impact of Percutaneous Coronary Intervention Extent, Complexity and Platelet Reactivity on Outcomes after Drug-Eluting Stent Implantation. Int. J. Cardiol. 2018, 268, 61–67. [Google Scholar] [CrossRef]
- Costa, F.; Van Klaveren, D.; Feres, F.; James, S.; Räber, L.; Pilgrim, T.; Hong, M.-K.; Kim, H.-S.; Colombo, A.; Steg, P.G.; et al. Dual Antiplatelet Therapy Duration Based on Ischemic and Bleeding Risks after Coronary Stenting. J. Am. Coll. Cardiol. 2019, 73, 741–754. [Google Scholar] [CrossRef]
- Werner, N.; Nickenig, G.; Sinning, J.-M. Complex PCI Procedures: Challenges for the Interventional Cardiologist. Clin. Res. Cardiol. 2018, 107, 64–73. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 2019, l4898. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Serruys, P.W.; Takahashi, K.; Chichareon, P.; Kogame, N.; Tomaniak, M.; Modolo, R.; Chang, C.C.; Komiyama, H.; Soliman, O.; Wykrzykowska, J.J.; et al. Impact of Long-Term Ticagrelor Monotherapy Following 1-Month Dual Antiplatelet Therapy in Patients Who Underwent Complex Percutaneous Coronary Intervention: Insights from the Global Leaders Trial. Eur. Heart J. 2019, 40, 2595–2604. [Google Scholar] [CrossRef]
- Dangas, G.; Baber, U.; Sharma, S.; Giustino, G.; Mehta, S.; Cohen, D.J.; Angiolillo, D.J.; Sartori, S.; Chandiramani, R.; Briguori, C.; et al. Ticagrelor with or without Aspirin after Complex PCI. J. Am. Coll. Cardiol. 2020, 75, 2414–2424. [Google Scholar] [CrossRef]
- Lee, S.-J.; Lee, Y.-J.; Kim, B.-K.; Hong, S.-J.; Ahn, C.-M.; Kim, J.-S.; Ko, Y.-G.; Choi, D.; Hong, M.-K.; Jang, Y. Ticagrelor Monotherapy Versus Ticagrelor with Aspirin in Acute Coronary Syndrome Patients with a High Risk of Ischemic Events. Circ. Cardiovasc. Interv. 2021, 14, e010812. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, R.; Oliva, A.; Avvedimento, M.; Franzone, A.; Windecker, S.; Valgimigli, M.; Esposito, G.; Jüni, P. Mortality after Bleeding versus Myocardial Infarction in Coronary Artery Disease: A Systematic Review and Meta-Analysis. EuroIntervention 2021, 17, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.W.; Baos, S.; Collett, L.; Hutchinson, J.L.; Nkau, M.; Molina, M.; Aungraheeta, R.; Reilly-Stitt, C.; Bowles, R.; Reeves, B.C.; et al. Pharmacodynamic Comparison of Ticagrelor Monotherapy Versus Ticagrelor and Aspirin in Patients After Percutaneous Coronary Intervention: The TEMPLATE (Ticagrelor Monotherapy and Platelet Reactivity) Randomized Controlled Trial. J. Am. Heart Assoc. 2020, 9, e016495. [Google Scholar] [CrossRef]
- Yamamoto, K.; Watanabe, H.; Morimoto, T.; Domei, T.; Ohya, M.; Ogita, M.; Takagi, K.; Suzuki, H.; Nikaido, A.; Ishii, M.; et al. Very Short Dual Antiplatelet Therapy after Drug-Eluting Stent Implantation in Patients Who Underwent Complex Percutaneous Coronary Intervention: Insight from the STOPDAPT-2 Trial. Circ. Cardiovasc. Interv. 2021, 14, e010384. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, H. STOPDAPT-2 ACS: One-Month Dual Antiplatelet Therapy Followed by Clopidogrel Monotherapy in Acute Coronary Syn-Drome. In Proceedings of the ESC Congress 2021-The Digital Experience, London, UK, 27–30 August 2021. [Google Scholar]
- Condello, F. Uncertainties about Platelet Function and Genetic Testing for Guiding Dual Antiplatelet Therapy in Percutaneous Coronary Intervention. J. Thromb. Thrombolysis 2021, 2021, 1–3. [Google Scholar] [CrossRef]
- Gurbel, P.A.; Bliden, K.P.; Butler, K.; Tantry, U.S.; Gesheff, T.; Wei, C.; Teng, R.; Antonino, M.J.; Patil, S.B.; Karunakaran, A.; et al. Randomized Double-Blind Assessment of the ONSET and OFFSET of the Antiplatelet Effects of Ticagrelor Versus Clopidogrel in Patients with Stable Coronary Artery Disease. Circulation 2009, 120, 2577–2585. [Google Scholar] [CrossRef] [Green Version]
- Collet, J.P.; Thiele, H.; Barbato, E.; Bauersachs, J.; Dendale, P.; Edvardsen, T.; Gale, C.P.; Jobs, A.; Lambrinou, E.; Mehilli, J.; et al. 2020 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Valgimigli, M.; Frigoli, E.; Leonardi, S.; Vranckx, P.; Rothenbühler, M.; Tebaldi, M.; Varbella, F.; Calabrò, P.; Garducci, S.; Rubartelli, P.; et al. Radial versus Femoral Access and Bivalirudin versus Unfractionated Heparin in Invasively Managed Patients with Acute Coronary Syndrome (MATRIX): Final 1-Year Results of a Multicentre, Randomised Controlled Trial. Lancet 2018, 392, 835–848. [Google Scholar] [CrossRef]
- Meijers, T.A.; Aminian, A.; van Wely, M.; Teeuwen, K.; Schmitz, T.; Dirksen, M.T.; Rathore, S.; van der Schaaf, R.J.; Knaapen, P.; Dens, J.; et al. Randomized Comparison between Radial and Femoral Large-Bore Access for Complex Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2021, 14, 1293–1303. [Google Scholar] [CrossRef] [PubMed]
- Räber, L.; Mintz, G.S.; Koskinas, K.C.; Johnson, T.W.; Holm, N.R.; Onuma, Y.; Radu, M.D.; Joner, M.; Yu, B.; Jia, H.; et al. Clinical Use of Intracoronary Imaging. Part 1: Guidance and Optimization of Coronary Interventions. An Expert Consensus Document of the European Association of Percutaneous Cardiovascular Interventions. Eur. Heart J. 2018, 39, 3281–3300. [Google Scholar] [CrossRef] [PubMed]
- Moulias, A.; Papageorgiou, A.; Alexopoulos, D. Platelet Function Testing and Genotyping for Tailoring Treatment in Complex PCI Patients. US Cardiol. Rev. 2021, 15, e14. [Google Scholar] [CrossRef]
- De Gregorio, M.G.; Marcucci, R.; Migliorini, A.; Gori, A.M.; Giusti, B.; Vergara, R.; Paniccia, R.; Carrabba, N.; Marchionni, N.; Valenti, R. Clinical Implications of “Tailored” Antiplatelet Therapy in Patients with Chronic Total Occlusion. J. Am. Heart Assoc. 2020, 9, e014676. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Condello, F.; Sturla, M.; Terzi, R.; Polimeni, A.; Stefanini, G.G. Walking the Line with Ticagrelor: Meta-Analysis Comparing the Safety and Efficacy of Ticagrelor Monotherapy after a Short Course of Ticagrelor-Based Dual Antiplatelet Therapy versus Standard Therapy in Complex Percutaneous Coronary Intervention. J. Clin. Med. 2021, 10, 5506. https://doi.org/10.3390/jcm10235506
Condello F, Sturla M, Terzi R, Polimeni A, Stefanini GG. Walking the Line with Ticagrelor: Meta-Analysis Comparing the Safety and Efficacy of Ticagrelor Monotherapy after a Short Course of Ticagrelor-Based Dual Antiplatelet Therapy versus Standard Therapy in Complex Percutaneous Coronary Intervention. Journal of Clinical Medicine. 2021; 10(23):5506. https://doi.org/10.3390/jcm10235506
Chicago/Turabian StyleCondello, Francesco, Matteo Sturla, Riccardo Terzi, Alberto Polimeni, and Giulio G. Stefanini. 2021. "Walking the Line with Ticagrelor: Meta-Analysis Comparing the Safety and Efficacy of Ticagrelor Monotherapy after a Short Course of Ticagrelor-Based Dual Antiplatelet Therapy versus Standard Therapy in Complex Percutaneous Coronary Intervention" Journal of Clinical Medicine 10, no. 23: 5506. https://doi.org/10.3390/jcm10235506
APA StyleCondello, F., Sturla, M., Terzi, R., Polimeni, A., & Stefanini, G. G. (2021). Walking the Line with Ticagrelor: Meta-Analysis Comparing the Safety and Efficacy of Ticagrelor Monotherapy after a Short Course of Ticagrelor-Based Dual Antiplatelet Therapy versus Standard Therapy in Complex Percutaneous Coronary Intervention. Journal of Clinical Medicine, 10(23), 5506. https://doi.org/10.3390/jcm10235506