The Prognostic Value of Eosinophil Recovery in COVID-19: A Multicentre, Retrospective Cohort Study on Patients Hospitalised in Spanish Hospitals

 , , , , , , , , , ,
, , , , , , , , , ,  , and add
Show full author list
, and add
Show full author list
Abstract
1. Introduction
Hypothesis and Objectives
2. Methods
2.1. Registry Design and Data Collection
2.2. Study Design
2.3. Statistical Analysis
3. Results
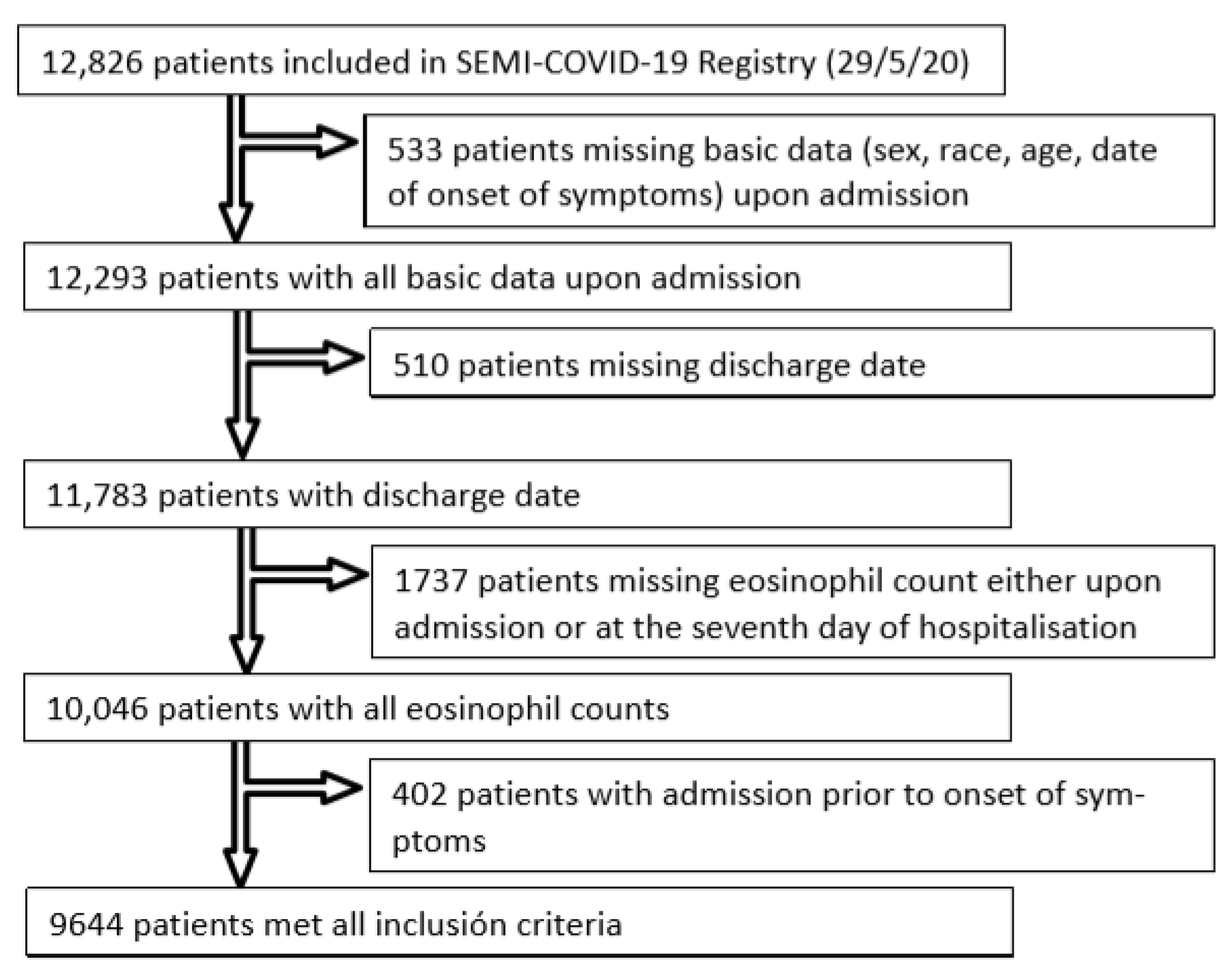
3.1. Sample Characteristics
3.2. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Stratton, C.W.; Tang, Y.W. Outbreak of pneumonia of unknown etiology in Wuhan, China: The mystery and the miracle. J. Med. Virol. 2020, 92, 401–402. [Google Scholar] [CrossRef] [PubMed]
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar]
- World Health Organization. Coronavirus Disease (COVID-19) Weekly Epidemiological Update-8 December 2020. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 9 December 2020).
- Ciotti, M.; Angeletti, S.; Minieri, M.; Giovannetti, M.; Benvenuto, D.; Pascarella, S.; Sagnelli, C.; Bianchi, M.; Bernardini, S.; Ciccozzi, M.; et al. COVID-19 Outbreak: An Overview. Chemotherapy 2020, 64, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases from the Chinese Center for Disease Control and Prevention. JAMA J. Am. Med. Assoc. 2020, 323, 1239–1242. Available online: https://jamanetwork.com/ (accessed on 9 December 2020). [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 2020, 81, e16–e25. [Google Scholar]
- Du, Y.; Tu, L.; Zhu, P.; Mu, M.; Wang, R.; Yang, P.; Wang, X.; Hu, C.; Ping, R.; Hu, P.; et al. Clinical Features of 85 Fatal Cases of COVID-19 from Wuhan. A Retrospective Observational Study. Am. J. Respir. Crit. Care Med. 2020, 201, 1372–1379. [Google Scholar] [CrossRef]
- Soni, M. Evaluation of eosinopenia as a diagnostic and prognostic indicator in COVID-19 infection. Int. J. Lab. Hematol. 2020, 1–5. [Google Scholar] [CrossRef]
- Tanni, F.; Akker, E.; Zaman, M.M.; Figueroa, N.; Pharm, B.T.; Hupart, K.H. Eosinopenia and COVID-19. JAOA 2020, 120, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Xia, Z. Eosinopenia as an early diagnostic marker of COVID-19 at the time of the epidemic. EClinicalMedicine 2020, 23, 100398. [Google Scholar] [CrossRef]
- Xie, G.; Ding, F.; Han, L.; Yin, D.; Lu, H.; Zhang, M. The role of peripheral blood eosinophil counts in COVID-19 patients. Allergy 2020. [Google Scholar] [CrossRef] [PubMed]
- Frater, J.L.; Zini, G.; d’Onofrio, G.; Rogers, H.J. COVID-19 and the clinical hematology laboratory. Int. J. Lab. Hematol. 2020, 42, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Lindsley, A.W.; Schwartz, J.T.; Rothenberg, M.E. Eosinophil responses during COVID-19 infections and coronavirus vaccination. J. Allergy Clin. Immunol. 2020, 146, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Xu, A.; Zhang, Y.; Xuan, W.; Yan, T.; Pan, K.; Yu, W.; Zhang, J. Patients of COVID-19 may benefit from sustained lopinavir-combined regimen and the increase of eosinophil may predict the outcome of COVID-19 progression. Int. J. Infect. Dis. 2020, 95, 183–191. [Google Scholar] [CrossRef]
- Sun, S.; Cai, X.; Wang, H.; He, G.; Lin, Y.; Lu, B.; Chen, C.; Pan, Y.; Hu, X. Abnormalities of peripheral blood system in patients with COVID-19 in Wenzhou, China. Clin. Chim. Acta. 2020, 507, 174–180. [Google Scholar] [CrossRef]
- Lippi, G.; Henry, B.M. Eosinophil count in severe coronavirus disease 2019 (COVID-19). QJM 2020, 113, 511–512. Available online: https://academic.oup.com/qjmed/article-abstract/doi/10.1093/qjmed/hcaa137/5823309 (accessed on 9 December 2020). [CrossRef]
- Casas-Rojo, J.M.; Antón-Santos, J.M.; Millán-Núñez-Cortés, J.; Lumbreras-Bermejo, C.; Ramos-Rincón, J.M.; Roy-Vallejo, E.; Artero-Mora, A.; Arnalich-Fernández, F.; García-Bruñén, J.M.; Vargas-Núñez, J.A.; et al. Clinical characteristics of patients hospitalized with COVID-19 in Spain: Results from the SEMI-COVID-19 Registry. Rev. Clín. Esp. 2020, 220, 480–494. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Prev. Med. 2007, 45, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Echevarria, C.; Hartley, T.; Nagarajan, T.; Tedd, H.; Steer, J.; Gibson, G.J.; Bourke, S.C. 30 day mortality and eosinopenia in patients with pneumonia. Eur. Respir. J. 2014, 44 (Suppl. 58), P2550. [Google Scholar]
- Asosingh, K.; Aronica, M.A. Eosinophils: Ancient Cells with New Roles in Chronic Lung Inflammation. Am. J. Respir. Crit. Care Med. 2017, 195, 1281–1282. [Google Scholar] [CrossRef] [PubMed]
- Halpin, D.M.G.; Faner, R.; Sibila, O.; Badia, J.R.; Agusti, A. Do chronic respiratory diseases or their treatment affect the risk of SARS-CoV-2 infection? Lancet Respir. Med. 2020, 8, 436–438. [Google Scholar] [CrossRef]
- Ravin, K.A.; Loy, M. The eosinophil in infection. Clin. Rev. Allergy Immunol. 2015, 50, 214–227. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zhi, Y.; Ying, S. COVID-19 and Asthma: Reflection During the Pandemic. Clin. Rev. Allerg Immunol. 2020, 59, 78–88. [Google Scholar] [CrossRef]
- Chusid, M.J. Eosinophils: Friends or Foes? J. Allergy Clin. Immunol. Pract. 2018, 6, 1439–1444. [Google Scholar] [CrossRef]
- O’Sullivan, J.A.; Bochner, B.S. Eosinophils and eosinophil-associated diseases: An update. J. Allergy Clin. Immunol. 2018, 141, 505–517. [Google Scholar] [CrossRef]
- Esser, N.; Legrand-Poels, S.; Piette, J.; Scheen, A.J.; Paquot, N. Inflammation as a link between obesity, metabolic syndrome and type 2 diabetes. Diabetes Res. Clin. Pract. 2014, 105, 141–150. Available online: http://www.diabetesresearchclinicalpractice.com/article/S0168822714001879/fulltext (accessed on 9 December 2020). [CrossRef]
- De Ruiter, K.; Tahapary, D.L.; Sartono, E.; Soewondo, P.; Supali, T.; Smit, J.W.A.; Yazdanbakhsh, M. Helminths, hygiene hypothesis and type 2 diabetes. Parasite Immunol. 2017, 39, e12404. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, X.; Jia, X.; Li, J.; Hu, K.; Chen, G.; Wei, J.; Gong, Z.; Zhou, C.; Yu, H.; et al. Risk factors for disease severity, unimprovement, and mortality in COVID-19 patients in Wuhan, China. Clin. Microbiol. Infect. 2020, 26, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Bretscher, P. On Analyzing How the Th1/Th2 Phenotype of an Immune Response Is Determined: Classical Observations Must Not Be Ignored. Front. Immunol. 2019, 10, 1234. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Chong, M.M.; Littman, D.R. Plasticity of CD4+ T cell lineage differentiation. Immunity 2009, 30, 646–655. [Google Scholar] [CrossRef] [PubMed]
- Mosmann, T.R.; Coffman, R.L. TH1 and TH2 cells: Different patterns of lymphokine secretion lead to different functional properties. Annu. Rev. Immunol. 1989, 7, 145–173. [Google Scholar] [CrossRef]
- David, C.; Fajgenbaum, M.D.; Carl, H.; June, M.D. Cytokine Storm. December 3, 2020. N. Engl. J. Med. 2020, 383, 2255–2273. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of immune response in patients with COVID-19 in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Westreich, D.; Greenland, S. The Table 2 Fallacy: Presenting and Interpreting Confounder and Modifier Coefficients. Am. J. Epidemiol. 2013, 177, 292–298. [Google Scholar] [CrossRef]


{kind=link}
| KERRYPNX | Recoverers | Non-Recoverers | p |
|---|---|---|---|
| Demographics | |||
| Patients | 3335 (34.6) | 6309 (65.4) | |
| Age (years) (n = 9644) | 63.85 ± 15.57 | 67.52 ± 16.0 | <0.001 |
| Gender (male) (n = 5509) | 1904 (57.1) | 3605 (57.2) | 0.479 |
| Race/ethnicity (n = 9489) | <0.001 | ||
| Caucasian | 2797 (85.3) | 5603 (90.2) | |
| Latino/a | 406 (12.4) | 505 (8.1) | |
| African/Black | 15 (0.5) | 26 (0.4) | |
| Alcohol abuse (n = 9394) | 126 (3.9) | 298 (4.8) | 0.036 |
| Tobacco use (n = 9218) | |||
| Current smoker | 156 (4.9) | 332 (5.5) | |
| Former smoker | 741 (23.3) | 1562 (25.8) | 0.009 |
| Degree of dependency (n = 9527) | <0.001 | ||
| Independent or mild | 138 (4.2) | 439 (7.0) | |
| Moderate | 175 (5.3) | 587 (9.4) | |
| Severe | 2986 (90.5) | 5202 (83.5) | |
| Cardiovascular risk factors | |||
| Hypertension (n = 9628) | 1510 (45.3) | 3222 (51.2) | <0.001 |
| Diabetes mellitus (n = 9612) | 558 (16.8) | 1259 (20.0) | <0.001 |
| Obesity (n = 8785) | 670 (22.0) | 1240 (21.6) | 0.346 |
| Respiratory diseases | |||
| COPD (n = 9619) | 159 (4.8) | 476 (7.6) | <0.001 |
| Asthma (n = 9617) | 245 (7.4) | 504 (8.0) | 0.263 |
| Chronic kidney failure (n = 9616) | 132 (4.0) | 410 (6.5) | <0.001 |
| Comorbidity (n = 9366) | <0.001 | ||
| No comorbidities | 373 (11.5) | 1158 (18.9) | |
| Mild | 329 (10.2) | 850 (13.9) | |
| Severe | 2538 (78.3) | 4118 (67.2) | |
| Previous chronic drug therapy | |||
| Chronic treatment with systemic corticoids (n = 9618) | 82 (2.5) | 313 (5.0) | <0.001 |
| Chronic treatment with inhaled corticoids (n = 9578) | 262 (7.9) | 657 (10.5) | <0.001 |
| Symptoms | |||
| Time from onset of symptoms (days) (n = 9644) | 7.4 (7.7) | 6.7 (4.8) | <0.001 |
| Cough (n = 9619) | 0.011 | ||
| No | 749 (22.5) | 1003 (25.2) | |
| Dry | 2044 (61.4) | 3703 (58.9) | |
| Productive | 534 (16.1) | 1586 (15.9) | |
| Dyspnoea (n = 9599) | 1850 (55.8) | 3683 (58.6) | 0.007 |
| Arthromyalgia (n = 9539) | 1172 (35.5) | 1910 (30.6) | <0.001 |
| Asthenia (n = 9513) | 1501 (45.6) | 2705 (43.5) | 0.048 |
| Anorexia (n = 9482) | 626 (19.1) | 1265 (20.4) | 0.123 |
| Fever at home (n = 9608) | 0.065 | ||
| <37 °C | 448 (13.5) | 915 (14.6) | |
| 37.0–37.9 °C | 651 (19.6) | 1307 (20.8) | |
| >38.0 °C | 2230 (67.0) | 4057 (64.6) | |
| Physical examination at admission | |||
| Confusion (n = 9530) | 223 (6.8) | 740 (11.9) | <0.001 |
| Tachypnoea (>20 brpm) (n = 9394) | 848 (26.0) | 2029 (33.1) | <0.001 |
| SBP (mmHg) (n = 9252) | 128.5 ± 20.28 | 128.8 ± 21.3 | 0.538 |
| Heart rate (bpm) (n = 9351) | 88.8 ± 16.90 | 88.6 ± 17.5 | 0.581 |
| Temperature (°C) (n = 9345) | 37.1 ± 0.98 | 37.1 ± 0.98 | 0.253 |
| Oxygen saturation (n = 9410) | 93.8 ± 4.45 | 92.9 ± 5.7 | <0.001 |
| Saturation <95% | 1550 (47.5) | 3197 (52) | <0.001 |
| Lung auscultation | |||
| Crackles (n = 9416) | 1726 (53.1) | 3290 (53.3) | 0.854 |
| Wheezing (n = 9414) | 143 (4.4) | 425 (6.9) | <0.001 |
| qSOFA score (n = 9644) | <0.001 | ||
| 0–1 | 3196 (95.8) | 5799 (91.9) | |
| 2–3 | 139 (4.2) | 510 (8.1) | |
| Additional tests | |||
| Radiological findings | |||
| Interstitial pulmonary infiltrates (n = 9600) | <0.001 | ||
| No pulmonary infiltrates | 348 (10.5) | 853 (13.6) | |
| Unilateral pulmonary infiltrates | 726 (21.9) | 1308 (20.8) | |
| Bilateral pulmonary infiltrates | 2247 (67.7) | 4118 (65.5) | |
| Laboratory findings upon admission | |||
| PO2/FiO2 ratio (mmHg) (n = 4859) | 303.3 ± 94.7 | 288.5 ± 98.6 | <0.001 |
| Leukocytes × 106/L (n = 9644) | 7262 ± 5002 | 7192 ± 5562 | 0.538 |
| Eosinophils × 106/L (n = 9644) | 18.25 ± 64.13 | 37.45 ± 107.64 | <0.001 |
| Eosinopenia <150 × 106/L | 3252 (97.5) | 5906 (93.6) | <0.001 |
| Lymphocytes × 106/L (n = 9644) | 1126 ± 1562 | 1098 ± 1805 | 0.443 |
| Lymphopenia <800 × 106/L | 939 (28.2) | 2312 (36.6) | <0.001 |
| Lymphopenia <800 × 106/L | |||
| Lymphopenia <800 × 106/L | |||
| Neutrophils × 106/L (n = 9644) | 5230 ± 2927 | 5192 ± 3382 | 0.583 |
| CRP (mg/L) (n = 9285) | 82.2 ± 80 | 85.2 ± 86.3 | 0.097 |
| Glucose (mg/dL) (n = 9368) | 123.7 ± 52.9 | 127.3 ± 57.7 | 0.003 |
| Creatinine (mg/dL) (n = 9614) | 1.0 ± 0.69 | 1.11 ± 0.86 | <0.001 |
| Urea (mg/dL) (n = 7713) | 41.8 ± 31.5 | 48.3 ± 36.6 | <0.001 |
| LDH (U/L) (n = 8448) | 341.2 ± 155.1 | 355.7 ± 179.3 | <0.001 |
| AST (U/L) (n = 7616) | 47.4 ± 48.3 | 47.7 ± 59.1 | 0.847 |
| ALT (U/L) (n = 9120) | 42.2 ± 42.0 | 41.2 ± 52.4 | 0.373 |
| D-dimer (ng/mL) (n = 7567) | 1354.8 ± 5157 | 1619.7 ± 5548 | 0.043 |
| Recoverers | Non-Recoverers | p | |
|---|---|---|---|
| Treatment Received | |||
| LPV/r (n = 9606) | 2151 (64.6) | 4047 (64.5) | 0.868 |
| Hydroxychloroquine (n = 9617) | 3016 (90.5) | 5432 (86.4) | <0.001 |
| Systemic corticosteroids (n = 9644) | 458 (13.7) | 2003 (31.7) | <0.001 |
| Tocilizumab (n = 9578) | 274 (8.2) | 664 (10.6) | <0.001 |
| Azithromycin (n = 9592) | 2079 (62.6) | 3911 (62.4) | 0.501 |
| Inhaled corticosteroids (n = 9497) | 164 (5.0) | 400 (6.5) | 0.004 |
| LMWH (n = 9564) | 2804 (84.5) | 5256 (84.1) | 0.611 |
| Outcomes | |||
| Pneumonia (n = 9605) | 257 (7.7) | 791 (12.6) | <0.001 |
| ARDS (n = 9595) | <0.001 | ||
| No | 2605 (78.3) | 3933 (62.7) | |
| Mild | 299 (9.0) | 547 (8.7) | |
| Moderate | 156 (4.7) | 531 (8.5) | |
| Severe | 266 (8.0) | 1258 (20.1) | |
| Acute kidney failure (n = 9613) | 315 (9.5) | 985 (15.7) | <0.001 |
| Sepsis (n = 9604) | 102 (3.1) | 462 (7.4) | <0.001 |
| ICU admission (n = 9636) | 179 (5.4) | 678 (10.8) | <0.001 |
| Length of hospital stay (days) (n = 9644) | 11.0 ± 7.8 (*) | 11.5 ± 9.2 (*) | <0.001 |
| Death (in-hospital) (n = 9644) | 172 (5.2) | 1423 (22.6) | <0.001 |
| Composite endpoint (in-hospital death or ICU admission or ARDS) (n = 9612) | 472 (14.2) | 2170 (34.5) | <0.001 |
| Discharge | 3163 (94.8) | 4886 (77.4) | <0.001 |
| without ICU admission | 3040 (91.3) | 4484 (71.1) | |
| without ICU admission or ARDS | 2852 (85.8) | 4118 (65.5) | |
| Non-Survivors | Survivors | p | |
|---|---|---|---|
| Age (years) | 78.7 ± 10.5 | 63.8 ± 15.7 | <0.001 |
| Time from onset of symptoms at admission (days) | 5.7 ± 5.0 | 7.2 ± 6.1 | <0.001 |
| Length of hospital stay (days) | 10.5 ± 9.4 | 11.5 ± 8.6 | <0.001 |
| Factor | Mortality when present | Mortality when absent | |
| Demographics | |||
| Male gender | 1011 (18.4) | 581 (14.1) | <0.001 |
| Caucasian race/ethnicity | 1503 (17.9) | 72 (6.6) | <0.001 |
| Alcohol abuse | 86 (20.3) | 1468 (16.4) | 0.034 |
| Tobacco use | 585 (21.0) | 936 (14.6) | <0.001 |
| Moderate or severe dependency | 531 (39.7) | 1043 (12.7) | <0.001 |
| Hypertension | 1115 (13.6) | 477 (9.7) | <0.001 |
| Obesity | 359 (18.8) | 1067 (15.5) | 0.001 |
| Diabetes mellitus | 480 (26.4) | 1111 (14.3) | <0.001 |
| COPD | 200 (31.5) | 1390 (15.5) | <0.001 |
| Asthma | 89 (11.9) | 1500 (16.9) | <0.001 |
| Chronic kidney disease | 200 (36.9) | 1389 (15.3) | <0.001 |
| Moderate or severe comorbidity | 523 (34.2) | 1023 (13.1) | <0.001 |
| Chronic treatment with systemic corticosteroids | 113 (28.6) | 1476 (16.0) | <0.001 |
| Chronic treatment with inhaled corticosteroids | 208 (22.6) | 1372 (15.8) | <0.001 |
| Symptoms | |||
| Cough | 1093 (15.0) | 494 (21.2) | <0.001 |
| Dyspnoea | 1100 (19.9) | 485 (11.9) | <0.001 |
| Arthromyalgia | 309 (10.0) | 1261 (19.5) | <0.001 |
| Asthenia | 640 (15.2) | 924 (17.4) | 0.004 |
| Anorexia | 373 (19.7) | 1182 (15.6) | <0.001 |
| Fever at home | 1266 (15.4) | 315 (23.1) | <0.001 |
| Physical examination | |||
| Confusion | 439 (45.6) | 1135 (13.2) | <0.001 |
| Tachypnoea >20 brpm | 848 (29.5) | 699 (10.7) | <0.001 |
| Hypotension (<90 mmHg) | 56 (36.4) | 1492 (16.4) | <0.001 |
| Tachycardia >100 bpm | 335 (16.0) | 1215 (16.8) | 0.383 |
| Temperature >37.7 °C | 431 (17.5) | 1106 (16.1) | 0.115 |
| Oxygen saturation via pulse oximetry (%) | <0.001 | ||
| Normal (>94%) | 375 (8.0) | ||
| Hypoxemia (90–94%) | 551 (16.9) | ||
| Desaturation (<90%) | 628 (42.2) | ||
| Crackles | 943 (18.8) | 603 (13.7) | <0.001 |
| Wheezing | 152 (26.8) | 1392 (15.7) | <0.001 |
| qSOFA score ≥2 | 333 (51.3) | 1262 (14.0) | <0.001 |
| Findings upon admission | |||
| Pulmonary infiltrates on radiological tests | 1417 (16.9) | 173 (14.4) | 0.320 |
| Eosinophils (×106/L) | 0.084 | ||
| >300 | 26 (15.1) | ||
| 150–299 | 38 (12.1) | ||
| <150 | 1531 (16.7) | ||
| Eosinopenia <150 × 106/L | 1531 (16.7) | 64 (13.2) | 0.040 |
| Lymphocytes (×106/L) | <0.001 | ||
| >1200 | 337 (10.9) | ||
| 1000–1199 | 184 (12.1) | ||
| 800–999 | 269 (15.0) | ||
| <800 | 805 (24.8) | ||
| Lymphopenia <800 × 106/L | 805 (24.8) | 790 (12.4) | <0.001 |
| Basal glucose >125 mg/dL | 792 (27.4) | 761 (11.8) | <0.001 |
| High creatinine (>1.4 mg/dL) | 568 (42.2) | 1025 (12.4) | <0.001 |
| LDH >360 U/L | 702 (23.1) | 585 (10.8) | <0.001 |
| AST >60 U/L | 322 (21.4) | 893 (14.6) | <0.001 |
| ALT >60 U/L | 193 (13.0) | 1246 (16.3) | 0.001 |
| D-dimer (ng/mL) | <0.001 | ||
| <500 | 269 (8.9) | ||
| 500–999 | 289 (12.4) | ||
| >1000 | 535 (24.1) | ||
| D-dimer >1000 ng/mL | 535 (24.1) | 558 (10.4) | <0.001 |
| Treatment | |||
| Lopinavir/ritonavir | 929 (15.0) | 656 (19.2) | <0.001 |
| Hydroxychloroquine | 1246 (14.7) | 341 (29.2) | <0.001 |
| Systemic corticosteroids | 532 (21.6) | 1063 (14.8) | <0.001 |
| Tocilizumab | 214 (22.8) | 1372 (15.9) | <0.001 |
| Azithromycin | 914 (15.3) | 664 (18.4) | <0.001 |
| Inhaled corticosteroids | 117 (20.7) | 1446 (16.2) | 0.005 |
| Low-molecular-weight heparin | 1324 (16.4) | 252 (16.8) | 0.753 |
| Findings during progress | |||
| Eosinophils increased >80 × 106/L | 172 (5.2) | 1423 (22.6) | <0.001 |
| Lymphocyte increased >200 × 106/L | 288 (6.2) | 1307 (26.1) | <0.001 |
| LDH increased >50% | 349 (48.9) | 760 (11.0) | <0.001 |
| Creatinine increased >50% | 224 (62.0) | 1350 (14.7) | <0.001 |
| D-dimer increased >500 ng/mL | 339 (26.8) | 491 (9.8) | <0.001 |
| Glycaemia increased >100 mg/dL | 136 (42.6) | 1353 (15.6) | <0.001 |
| AST increased 3× | 72 (24.4) | 1045 (15.5) | <0.001 |
| ALT increased 3× | 125 (13.4) | 1228 (15.9) | 0.040 |
| Adjusted OR | p | |
|---|---|---|
| Demographics | ||
| Age (years) | 1.050 (1.036 to 1.065) | 0.000 |
| Gender (female) | 0.644 (0.471 to 0.881) | 0.006 |
| Hypertension | 1.320 (0.996 to 1.816) | 0.087 |
| Moderate-to-severe dependency | 2.250 (1.515 to 3.342) | 0.000 |
| Clinical manifestations at admission | ||
| Cough | 0.670 (0.483 to 0.929) | 0.016 |
| Confusion | 1.718 (1.149 to 2.569) | 0.008 |
| Tachypnoea | 1.894 (1.397 to 2.566) | 0.000 |
| Wheezing | 1.597 (0.966 to 2.639) | 0.068 |
| Desaturation | ||
| Saturation 90–94% | 1.701 (1.196 to 2.420) | 0.003 |
| Saturation <90% | 4.594 (3.084 to 6.843) | 0.000 |
| Treatment during hospitalisation | ||
| Hydroxychloroquine | 0.662 (0.432 to 1.013) | 0.057 |
| Azithromycin | 0.647 (0.475 to 0.881) | 0.006 |
| Laboratory findings at admission | ||
| Creatinine >1.4 at admission | 1.564 (1.103 to 2.219) | 0.012 |
| LDH >360 at admission | 2.450 (1.757 to 3.416) | 0.000 |
| AST >60 at admission | 2.462 (1.637 to 3.704) | 0.000 |
| ALT >60 at admission | 0.444 (0.274 to 0.720) | 0.001 |
| Glycaemia >125 at admission | 1.405 (1.045 to 1.889) | 0.024 |
| Lymphopenia <800 × 106/L at admission | 1.452 (1.086 to 1.942) | 0.012 |
| Laboratory findings on the seventh day of hospitalisation | ||
| Eosinophil counts increased >80 × 106/L | 0.234 (0.154 to 0.354) | 0.000 |
| LDH increased >1.5× | 10.614 (7.101 to 15.867) | 0.000 |
| Creatinine increased >1.5× | 6.032 (3.528 to 10.315) | 0.000 |
| D-dimer increased >500 | 2.341 (1.718 to 3.189) | 0.000 |
| ALT increased >3× | 0.536 (0.321 to 0.894) | 0.017 |
| Adjusted OR | p | |
|---|---|---|
| Demographics | ||
| Race (Caucasian) | 0.715 (0.528 to 0.969) | 0.030 |
| Clinical manifestations at admission | ||
| Duration of symptoms at admission (days) | 0.962 (0.942 to 0.983) | 0.000 |
| Cough | 1.070 (0.856 to 1.337) | 0.055 |
| Confusion | 1.783 (1.320 to 2.409) | 0.000 |
| Tachypnoea >20 brpm | 2.057 (1.697 to 2.495) | 0.000 |
| Wheezing | 1.402 (0.987 to 1.991) | 0.059 |
| Fever | 1.375 (1.125 to 1.681) | 0.002 |
| Desaturation | ||
| Saturation 90–94% | 1.694 (1.377 to 2.084) | 0.000 |
| Saturation <90% | 4.856 (3.730 to 6.322) | 0.000 |
| Treatment during hospitalization | ||
| Hydroxychloroquine | 0.684 (0.504 to 0.928) | 0.015 |
| Corticosteroids | 1.634 (1.348 to 1.979) | 0.000 |
| Laboratory findings at admission | ||
| Creatinine >1.4 at admission | 1.497 (1.162 to 1.928) | 0.002 |
| D-dimer >1000 at admission | 1.226 (1.006 to 1.495) | 0.044 |
| LDH >360 at admission | 2.306 (1.907 to 2.790) | 0.000 |
| Glycaemia >125 at admission | 1.386 (1.143 to 1.681) | 0.001 |
| Lymphopenia <800 × 106/L at admission | 1.541 (1.222 to 1.944) | 0.000 |
| Any pulmonary infiltrates | 2.306 (1.601 to 3.321) | 0.000 |
| Laboratory findings on the seventh day of hospitalisation | ||
| Eosinophil counts increased >80 × 106/L | 0.474 (0.383 to 0.586) | 0.000 |
| LDH increased >1.5× | 6.437 (4.779 to 8.669) | 0.000 |
| Creatinine increased >1.5× | 3.485 (2.160 to 5.620) | 0.000 |
| D-dimer increased >500 | 2.643 (2.155 to 3.241) | 0.000 |
| Glycaemia increased >100 mg/dL | 1.661 (1.083 to 2.548) | 0.020 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mateos González, M.; Sierra Gonzalo, E.; Casado Lopez, I.; Arnalich Fernández, F.; Beato Pérez, J.L.; Monge Monge, D.; Vargas Núñez, J.A.; García Fenoll, R.; Suárez Fernández, C.; Freire Castro, S.J.; et al. The Prognostic Value of Eosinophil Recovery in COVID-19: A Multicentre, Retrospective Cohort Study on Patients Hospitalised in Spanish Hospitals. J. Clin. Med. 2021, 10, 305. https://doi.org/10.3390/jcm10020305
Mateos González M, Sierra Gonzalo E, Casado Lopez I, Arnalich Fernández F, Beato Pérez JL, Monge Monge D, Vargas Núñez JA, García Fenoll R, Suárez Fernández C, Freire Castro SJ, et al. The Prognostic Value of Eosinophil Recovery in COVID-19: A Multicentre, Retrospective Cohort Study on Patients Hospitalised in Spanish Hospitals. Journal of Clinical Medicine. 2021; 10(2):305. https://doi.org/10.3390/jcm10020305
Chicago/Turabian StyleMateos González, María, Elena Sierra Gonzalo, Irene Casado Lopez, Francisco Arnalich Fernández, José Luis Beato Pérez, Daniel Monge Monge, Juan Antonio Vargas Núñez, Rosa García Fenoll, Carmen Suárez Fernández, Santiago Jesús Freire Castro, and et al. 2021. "The Prognostic Value of Eosinophil Recovery in COVID-19: A Multicentre, Retrospective Cohort Study on Patients Hospitalised in Spanish Hospitals" Journal of Clinical Medicine 10, no. 2: 305. https://doi.org/10.3390/jcm10020305
APA StyleMateos González, M., Sierra Gonzalo, E., Casado Lopez, I., Arnalich Fernández, F., Beato Pérez, J. L., Monge Monge, D., Vargas Núñez, J. A., García Fenoll, R., Suárez Fernández, C., Freire Castro, S. J., Mendez Bailon, M., Perales Fraile, I., Madrazo, M., Pesqueira Fontan, P. M., Magallanes Gamboa, J. O., González García, A., Crestelo Vieitez, A., Fonseca Aizpuru, E. M., Aranguren Arostegui, A., ... for the SEMI-COVID-19 Network. (2021). The Prognostic Value of Eosinophil Recovery in COVID-19: A Multicentre, Retrospective Cohort Study on Patients Hospitalised in Spanish Hospitals. Journal of Clinical Medicine, 10(2), 305. https://doi.org/10.3390/jcm10020305