Do Women Have a Higher Mortality Risk Than Men following ICU Admission after Out-of-Hospital Cardiac Arrest? A Retrospective Cohort Analysis

 ,
,
Abstract
:1. Background
2. Material and Methods
2.1. Study Sample, Setting, and Design
2.2. Baseline Characteristics and Clinical Outcomes
2.3. Primary and Secondary Outcomes
2.4. Statistical Analysis
3. Results
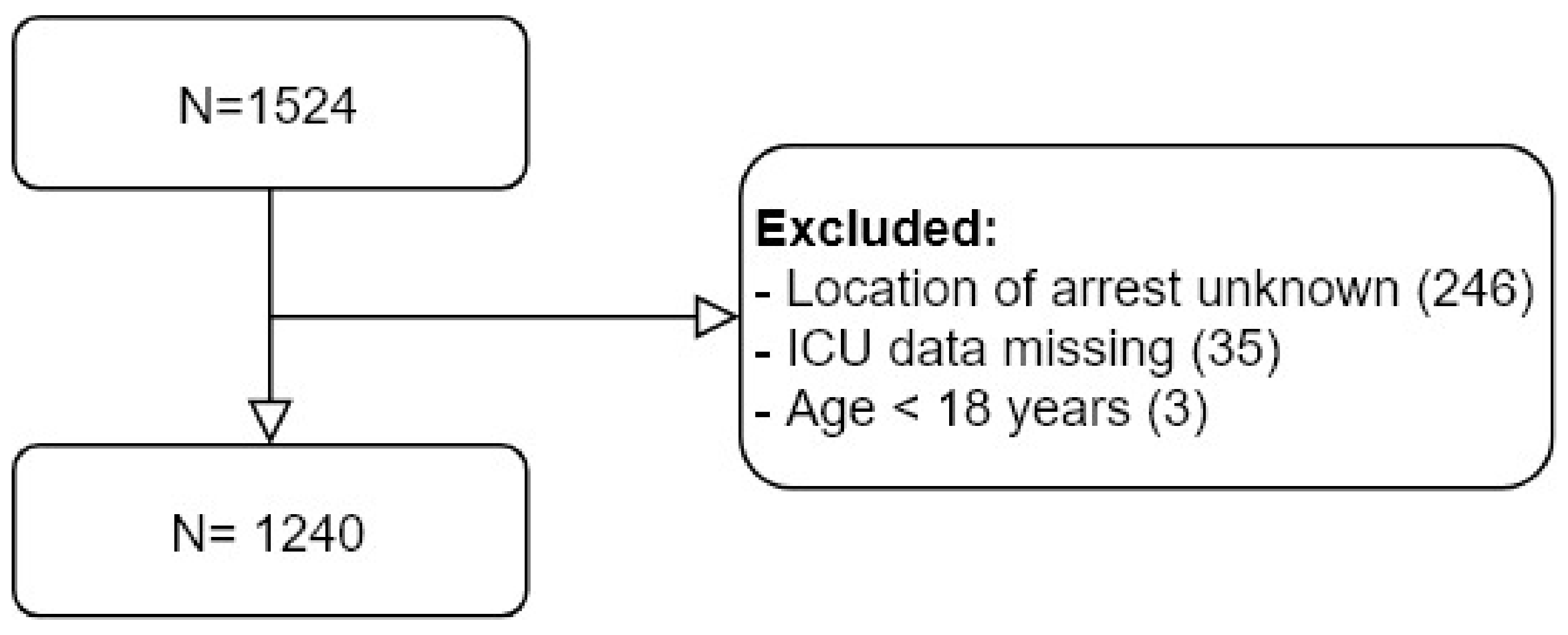
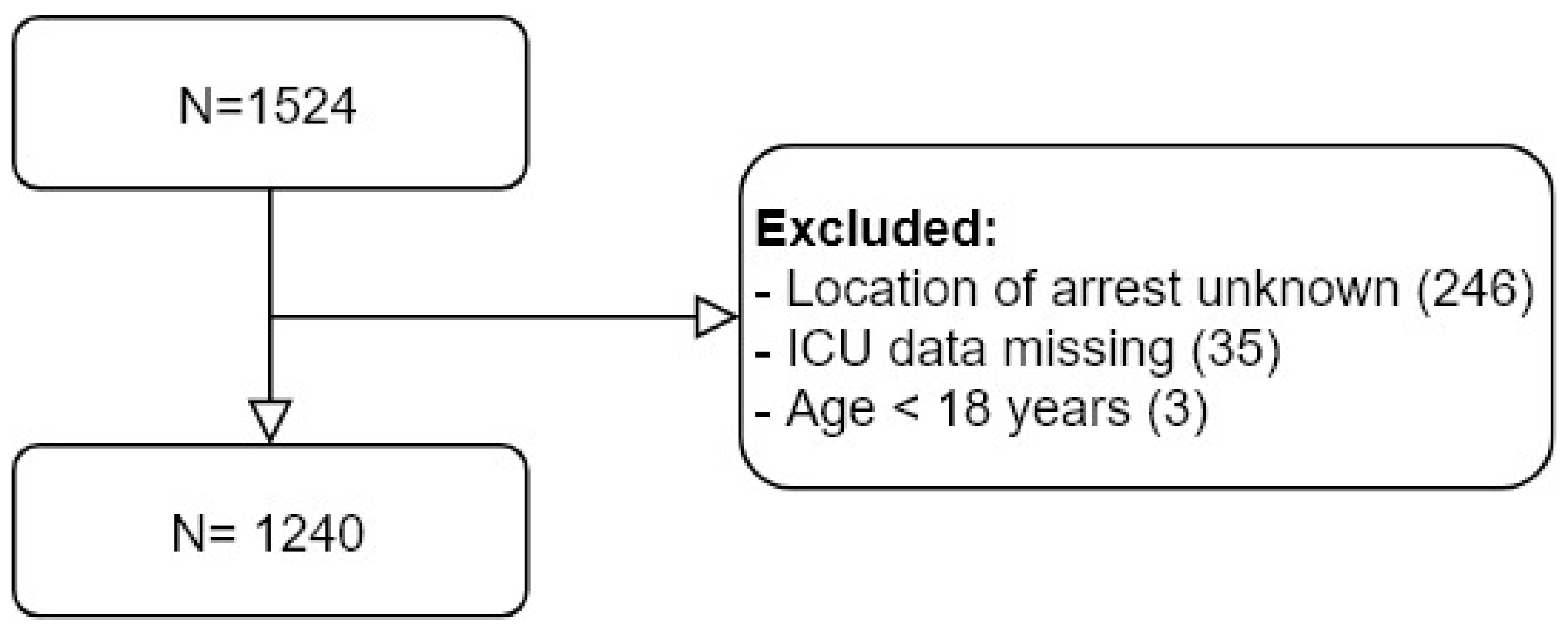
3.1. Study Sample
3.2. Descriptive Statistics: Baseline Characteristics
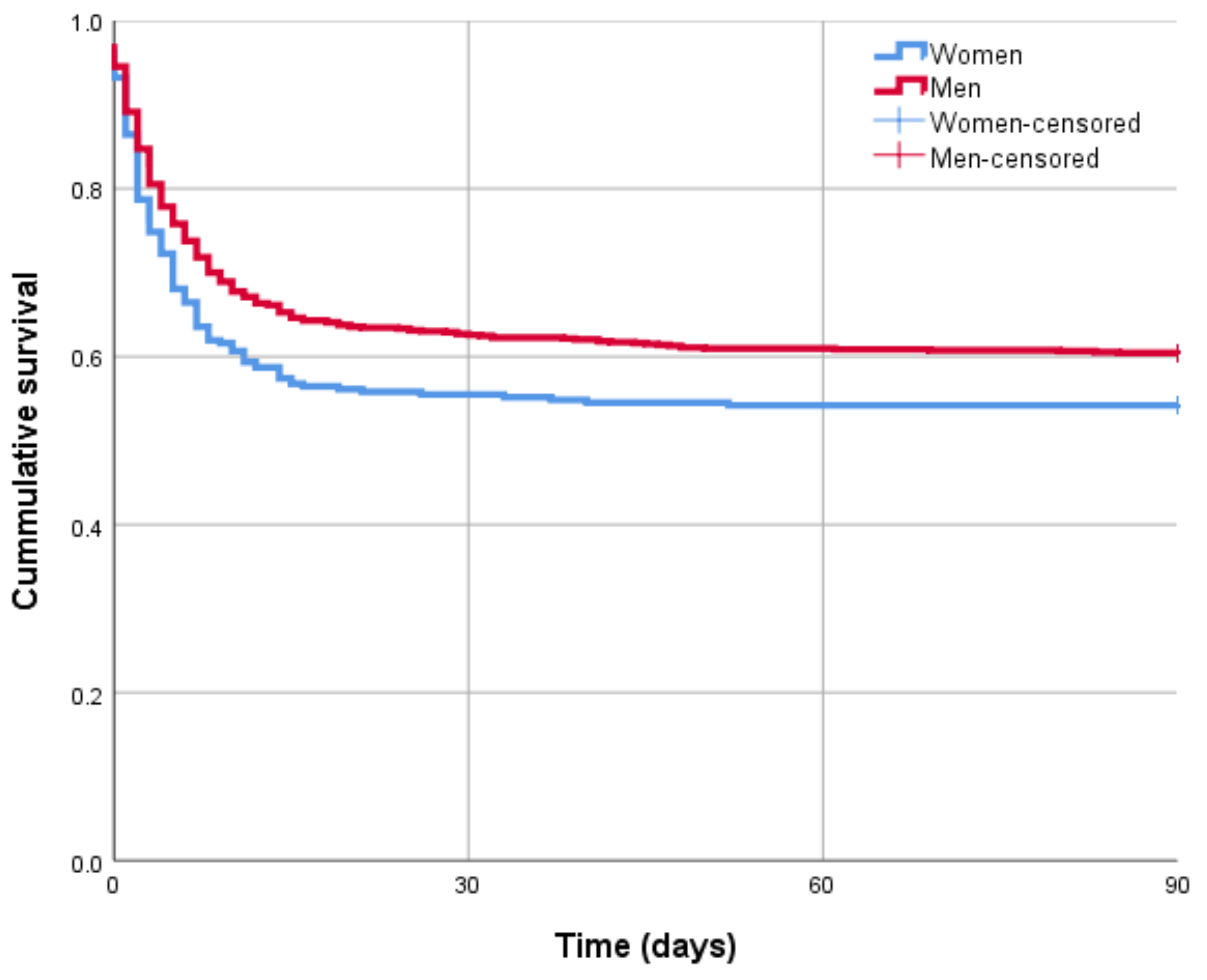
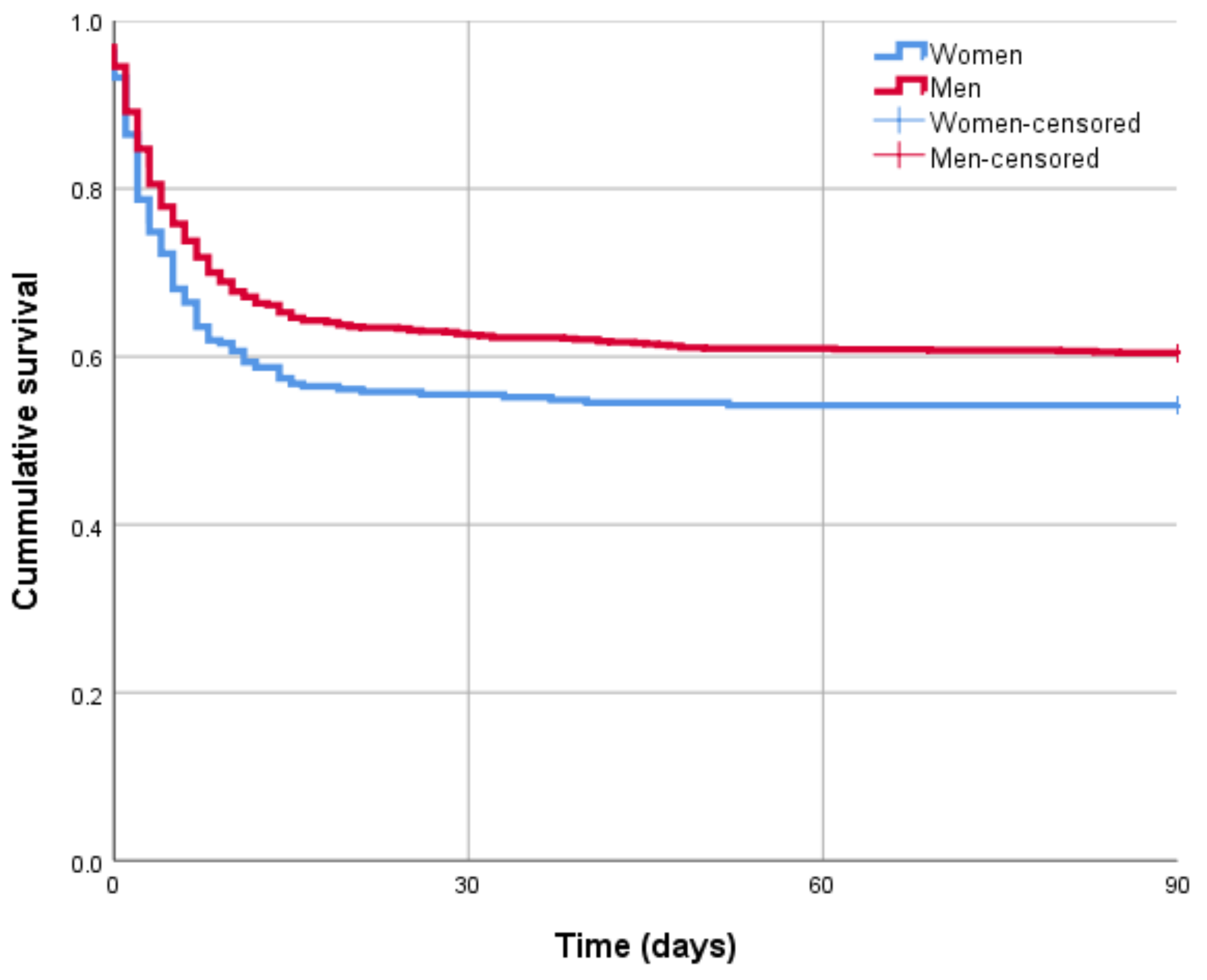
3.3. Primary Outcome: 90-Day Mortality
3.4. Secondary Outcome: CPC and ICU Length of Stay
3.5. Sensitivity Analysis
4. Discussion
4.1. Limitations
4.2. Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Atwood, C.; Eisenberg, M.S.; Herlitz, J.; Rea, T.D. Incidence of EMS-treated out-of-hospital cardiac arrest in Europe. Resuscitation 2005, 67, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Lei, H.; Hu, J.; Liu, L.; Xu, D. Sex differences in survival after out-of-hospital cardiac arrest: A meta-analysis. Crit. Care 2020, 24, 1–13. [Google Scholar] [CrossRef]
- Gräsner, J.T.; Lefering, R.; Koster, R.W.; Masterson, S.; Böttiger, B.W.; Herlitz, J.; Zeng, T. EuReCa ONE—27 Nations, ONE Europe, ONE Registry: A prospective one month analysis of out-of-hospital cardiac arrest outcomes in 27 countries in Europe. Resuscitation 2016, 105, 188–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berdowski, J.; Berg, R.A.; Tijssen, J.G.; Koster, R.W. Global incidences of out-of-hospital cardiac arrest and survival rates: Systematic review of 67 prospective studies. Resuscitation 2010, 81, 1479–1487. [Google Scholar] [CrossRef] [PubMed]
- Sasson, C.; Rogers, M.A.; Dahl, J.; Kellermann, A.L. Predictors of survival from out-of-hospital cardiac arrest: A systematic review and meta-analysis. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 63–81. [Google Scholar] [CrossRef] [Green Version]
- Pijls, R.W.; Nelemans, P.J.; Rahel, B.M.; Gorgels, A.P. A text message alert system for trained volunteers improves out-of-hospital cardiac arrest survival. Resuscitation 2016, 105, 182–187. [Google Scholar] [CrossRef] [Green Version]
- Regitz-Zagrosek, V.; Kararigas, G. Mechanistic pathways of sex differences in cardiovascular disease. Physiol. Rev. 2017, 97, 1–37. [Google Scholar] [CrossRef] [Green Version]
- Blom, M.T.; Oving, I.; Berdowski, J.; van Valkengoed, I.; Bardai, A.; Tan, H.L. Women have lower chances than men to be resuscitated and survive out-of-hospital cardiac arrest. Eur. Hear. J. 2019, 40, 3824–3834. [Google Scholar] [CrossRef]
- Pathak, L.A.; Shirodkar, S.; Ruparelia, R.; Rajebahadur, J. Coronary artery disease in women. Indian Heart J. 2017, 69, 532–538. [Google Scholar] [CrossRef]
- Coventry, L.L.; Finn, J.; Bremner, A. Sex differences in symptom presentation in acute myocardial infarction: A systematic review and meta-analysis. Hear. Lung 2011, 40, 477–491. [Google Scholar] [CrossRef]
- Kotini-Shah, P.; Del Rios, M.; Khosla, S.; Pugach, O.; Vellano, K.; McNally, B.; Hoek, T.V.; Chan, P.S. Sex differences in outcomes for out-of-hospital cardiac arrest in the United States. Resuscitation 2021, 163, 6–13. [Google Scholar] [CrossRef]
- Casey, S.D.; Mumma, B.E. Sex, race, and insurance status differences in hospital treatment and outcomes following out-of-hospital cardiac arrest. Resuscitation 2018, 126, 125–129. [Google Scholar] [CrossRef]
- Kim, C.; Fahrenbruch, C.E.; Cobb, L.A.; Eisenberg, M.S. Out-of-hospital cardiac arrest in men and women. Circulation 2001, 104, 2699–2703. [Google Scholar] [CrossRef] [Green Version]
- Mahapatra, S.; Bunch, T.J.; White, R.D.; Hodge, D.O.; Packer, D.L. Sex differences in outcome after ventricular fibrillation in out-of-hospital cardiac arrest. Resuscitation 2005, 65, 197–202. [Google Scholar] [CrossRef]
- Mandigers, L.; Termorshuizen, F.; de Keizer, N.F.; Rietdijk, W.; Gommers, D.; dos Reis Miranda, D.; Corstiaan, A. Higher 1-year mortality in women admitted to intensive care units after cardiac arrest: A nationwide overview from the Netherlands between 2010 and 2018. J. Crit. Care 2021, 64, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Mandigers, L.; Scholten, E.; Rietdijk, W.J.; Uil, C.A.D.; van Thiel, R.J.; Rigter, S.; Heijnen, B.G.; Gommers, D.; Miranda, D.D.R. Survival and neurological outcome with extracorporeal cardiopulmonary resuscitation for refractory cardiac arrest caused by massive pulmonary embolism: A two center observational study. Resuscitation 2019, 136, 8–13. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, T.J.; Jain, S.K.; Voigt, A.H.; Wang, N.C.; Saba, S. Comparison of long-term survival following sudden cardiac arrest in men versus women. Am. J. Cardiol. 2019, 124, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Wissenberg, M.; Hansen, C.M.; Folke, F.; Lippert, F.; Weeke, P.; Karlsson, L.; Rajan, S.; Søndergaard, K.B.; Kragholm, K.; Christensen, E.F.; et al. Survival after out-of-hospital cardiac arrest in relation to sex: A nationwide registry-based study. Resuscitation 2014, 85, 1212–1218. [Google Scholar] [CrossRef]
- Reinikainen, M.; Niskanen, M.; Uusaro, A.; Ruokonen, E. Impact of gender on treatment and outcome of ICU patients. Acta Anaesthesiol. Scand. 2005, 49, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Angele, M.K.; Pratschke, S.; Hubbard, W.J.; Chaudry, I.H. Gender differences in sepsis: Cardiovascular and immunological aspects. Virulence 2014, 5, 12–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Offner, P.J.; Moore, E.E.; Biffl, W.L. Male gender is a risk factor for major infections after surgery. Arch. Surg. 1999, 134, 935–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsson, V.; Dankiewicz, J.; Nielsen, N.; Kern, K.B.; Mooney, M.R.; Riker, R.R.; Rubertsson, S.; Seder, D.B.; Stammet, P.; Sunde, K.; et al. Association of gender to outcome after out-of-hospital cardiac arrest—A report from the International Cardiac Arrest Registry. Crit. Care 2015, 19, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ko, S.Y.; Ahn, K.O.; Shin, S.D.; Park, J.H.; Lee, S.Y. Effects of telephone-assisted cardiopulmonary resuscitation on the sex disparity in provision of bystander cardiopulmonary resuscitation in public locations. Resuscitation 2021, 164, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Perman, S.M.; Shelton, S.K.; Knoepke, C.; Rappaport, K.; Matlock, D.D.; Adelgais, K.; Havranek, E.P.; Daugherty, S.L. Public perceptions on why women receive less bystander cardiopulmonary resuscitation than men in out-of-hospital cardiac arrest. Circulation 2019, 139, 1060–1068. [Google Scholar] [CrossRef]
- Kiyohara, K.; Katayama, Y.; Kitamura, T.; Kiguchi, T.; Matsuyama, T.; Ishida, K.; Sado, J.; Hirose, T.; Hayashida, S.; Nishiyama, C.; et al. Gender disparities in the application of public-access AED pads among OHCA patients in public locations. Resuscitation 2020, 150, 60–64. [Google Scholar] [CrossRef]
- Andersen, L.W.; Holmberg, M.J.; Granfeldt, A.; Løfgren, B.; Vellano, K.; McNally, B.F.; Siegerink, B.; Kurth, T.; Donnino, M.W. Neighborhood characteristics, bystander automated external defibrillator use, and patient outcomes in public out-of-hospital cardiac arrest. Resuscitation 2018, 126, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Kiyohara, K.; Nishiyama, C.; Kitamura, T.; Matsuyama, T.; Sado, J.; Shimamoto, T.; Kobayashi, D.; Kiguchi, T.; Okabayashi, S.; Kawamura, T.; et al. The association between public access defibrillation and outcome in witnessed out-of-hospital cardiac arrest with shockable rhythm. Resuscitation 2019, 140, 93–97. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Total (N = 1240) | 90-Day Mortality | p-Value | Missing Values (N) | ||
|---|---|---|---|---|---|
| Non-Survivors (N = 510) | Survivors (N = 730) | ||||
| Demographic characteristics | |||||
| Age (years) | 64.0 (53.8–73.0) | 68.5 (59.7–77.4) | 60.7 (50.5–69.3) | <0.001 | 0 |
| Gender | 0.053 | 0 | |||
| Men | 930 (75.0) | 368 (72.2) | 562 (77.0) | ||
| Women | 510 (25.0) | 142 (27.8) | 168 (23.0) | ||
| Medical history | |||||
| Hypertension | 435 (38.3) | 187 (41.5) | 248 (36.2) | 0,074 | 104 |
| Hypercholesterolemia | 283 (25.0) | 114 (25.5) | 169 (24.7) | 0.725 | 108 |
| Diabetes Mellitus | 229 (19.6) | 136 (29.1) | 93 (13.2) | <0.001 | 70 |
| Family history of cardiovascular disease | 199 (22.3) | 42 (13.5) | 157 (27.1) | <0.001 | 349 |
| Previous myocardial infarction | 279 (22.6) | 116 (22.9) | 163 (22.4) | 0.815 | 5 |
| Chronic heart failure | 151 (12.2) | 81 (16.1) | 70 (9.6) | 0.001 | 7 |
| Previous cardiac arrhythmia | 199 (17.0) | 89 (19.2) | 110 (15.5) | 0.101 | 69 |
| Previous TIA or stroke | 105 (8.5) | 60 (11.8) | 45 (6.2) | <0.001 | 6 |
| Peripheral vascular disease | 111 (9.5) | 64 (13.7) | 47 (6.7) | <0.001 | 72 |
| Smoking | 345 (34.7) | 134 (34.7) | 211 (34.3) | 0.736 | 246 |
| Chronic lung disease | 146 (11.8) | 75 (14.8) | 71 (9.8) | 0.007 | 7 |
| Pulmonary embolism | 17 (1.4) | 9 (1.8) | 8 (1.1) | 0.317 | 6 |
| Previous percutaneous coronary intervention | 166 (13.5) | 64 (12.6) | 102 (14.0) | 0.479 | 8 |
| Previous coronary artery bypass grafting | 81 (6.6) | 35 (6.9) | 46 (6.3) | 0.681 | 7 |
| Previous ICD implantation | 28 (2.3) | 12 (2.4) | 16 (2.2) | 0.85 | 7 |
| Previous pacemaker implantation | 35 (2.8) | 19 (3.7) | 16 (2.2) | 0.108 | 7 |
| Medication use history | |||||
| Aspirin | 233 (19.0) | 104 (20.6) | 129 (17.8) | 0.222 | 11 |
| Antiplatelet therapy | 81 (6.6) | 40 (7.9) | 41 (5.7) | 0.115 | 10 |
| Oral anticoagulants | 175 (14.2) | 81 (16.0) | 94 (13.0) | 0.129 | 10 |
| ACE inhibitors | 221 (18.0) | 90 (17.8) | 131 (18.1) | 0.912 | 10 |
| Aldosterone antagonists | 1 (0.1) | 1 (0.1) | 0 (0.0) | 0.231 | 11 |
| Angiotensin-II blocker | 108 (8.8) | 52 (10.3) | 56 (7.7) | 0.117 | 10 |
| Beta blocker | 303 (24.7) | 127 (25.2) | 176 (24.3) | 0.712 | 11 |
| Calcium channel blocker | 98 (8.0) | 50 (9.9) | 48 (6.6) | 0.037 | 10 |
| Nitrates | 85 (6.9) | 37 (7.3) | 48 (6.6) | 0.631 | 10 |
| Diuretics | 235 (19.1) | 114 (22.6) | 121 (16.7) | 0.01 | 10 |
| Statins | 302 (24.6) | 133 (26.3) | 169 (23.3) | 0.225 | 10 |
| Non-statin lipid lowering agents | 19 (1.5) | 7 (1.4) | 12 (1.7) | 0.707 | 10 |
| Anti-arrhythmic | 57 (4.6) | 26 (5.1) | 31 (4.3) | 0.471 | 9 |
| Cardiac arrest characteristics | |||||
| Location of arrest | <0.001 | 0 | |||
| Home | 654 (52.7) | 317 (62.2) | 337 (46.2) | ||
| Public | 586 (47.3) | 193 (37.8) | 393 (53.8) | ||
| Witnessed arrest | 908 (76.4) | 340 (70.2) | 566 (80.6) | <0.001 | 54 |
| Bystander CPR | 768 (64.9) | 266 (55.1) | 502 (71.7) | <0.001 | 57 |
| Estimated time patient found until CPR | <0.001 | 234 | |||
| 0–5 min | 777 (77,2) | 263 (67.4) | 514 (83.4) | ||
| 6–10 min | 180 (17.9) | 96 (24.6) | 84 (13.6) | ||
| 11–20 min | 41 (4.1) | 26 (6.7) | 15 (2.4) | ||
| > 20 min | 8 (0.8) | 5 (1.3) | 3 (0.5) | ||
| Defibrillation by AED | 442 (36.0) | 110 (21.8) | 332 (46.0) | <0.001 | 13 |
| Initial rhythm | <0.001 | 65 | |||
| Shock | 924 (78.6) | 298 (60.7) | 626 (91.5) | ||
| Non-shock | 251 (21.4) | 193 (39.3) | 58 (8.5) | ||
| Defibrillation by EMS | 792 (64.1) | 300 (59.2) | 492 (67.6) | 0.002 | 5 |
| Time interval arrest to ROSC | <0.001 | 271 | |||
| 0–5 min | 78 (8.0) | 16 (4.0) | 62 (10.9) | ||
| 6–10 min | 191 (19.7) | 48 (12.0) | 143 (25.1) | ||
| 11–20 min | 392 (40.5) | 139 (34.8) | 253 (44.5) | ||
| > 20 min | 308 (31.8) | 197 (49.3) | 111 (19.5) | ||
| Intubation out of hospital | 713 (57.9) | 339 (67.4) | 164 (32.6) | <0.001 | 8 |
| Cause of arrest—no (%) | <0.001 | 74 | |||
| Cardiac cause | 1064 (91.3) | 402 (85.2) | 662 (95.4) | ||
| Non-cardiac cause | 102 (8.7) | 70 (14.8) | 32 (4.6) | ||
| GCS at ED | <0.001 | 303 | |||
| 3 to 6 | 596 (63.6) | 309 (88.8) | 287 (48.7) | ||
| 7 to 11 | 145 (15.5) | 25 (7.2) | 120 (20.4) | ||
| 11 to 15 | 196 (20.9) | 14 (4.0) | 182 (30.9) | ||
| Cardiac cause—no (%) | 0.842 | 0 | |||
| Acute myocardial infarction | 681 (64.4) | 258 (64.7) | 423 (64.2) | ||
| Old myocardial infarction/scar | 121 (11.4) | 47 (11.8) | 74 (11.2) | ||
| Non-ischemic cardiomyopathy | 97 (9.2) | 32 (8.0) | 65 (9.9) | ||
| Primary rhythm or conduction disturbance | 108 (10.2) | 40 (10.0) | 68 (10.3) | ||
| Intoxication (heart medication) | 4 (0.4) | 1 (0.3) | 3 (0.5) | ||
| Cardiac tamponade | 1 (0.1) | 0 (0.0) | 1 (0.2) | ||
| Other | 15 (1.4) | 6 (1.5) | 9 (1.4) | ||
| Unknown cardiac cause | 31 (2.9) | 15 (3.8) | 16 (2.4) | ||
| Non-cardiac causes—no (%) | 0.023 | 0 | |||
| Epilepsy | 5 (5.0) | 4 (5.8) | 1 (3.1) | ||
| Trauma | 2 (2.0) | 1 (1.4) | 1 (3.1) | ||
| Intoxication | 10 (9.9) | 6 (8.7) | 4 (12.5) | ||
| Submersion | 6 (5.9) | 5 (7.2) | 1 (3.1) | ||
| Intracranial bleeding | 6 (5.9) | 6 (8.7) | 0 (0.0) | ||
| Pulmonary embolism | 18 (17.8) | 11 (15.9) | 7 (21.9) | ||
| Septic shock | 7 (6.9) | 7 (10.1) | 0 (0.0) | ||
| Asphyxia | 14 (13.9) | 10 (14.5) | 4 (12.5) | ||
| Hypoxia | 23 (22.8) | 17 (24.6) | 6 (18.8) | ||
| Other | 10 (9.9) | 2 (2.9) | 8 (25.0) | ||
| Total (N = 1240) | Women (N = 310) | Men (N = 930) | p-value | Missing Values (N) | |
|---|---|---|---|---|---|
| Demographic characteristics | |||||
| Age (years) | 64.0 (53.8–73.0) | 61.8 (49.6–72.1) | 64.4 (55.0–73.2) | 0.014 | 0 |
| Medical history | |||||
| Hypertension | 435 (38.3) | 117 (39.9) | 318 (37.7) | 0.503 | 104 |
| Hypercholesterolemia | 283 (25.0) | 48 (16.7) | 235 (27.8) | <0.001 | 108 |
| Diabetes Mellitus | 229 (19.6) | 60 (20.2) | 169 (19.4) | 0.752 | 70 |
| Family history of cardiovascular disease | 199 (22.3) | 46 (20.6) | 153 (22.9) | 0.48 | 349 |
| Previous myocardial infarction | 279 (22.6) | 37 (12.0) | 242 (26.1) | <0.001 | 5 |
| Chronic heart failure | 151 (12.2) | 36 (11.7) | 115 (12.4) | 0.712 | 7 |
| Previous cardiac arrhythmia | 199 (17.0) | 51 (17.3) | 148 (16.9) | 0.852 | 69 |
| Previous TIA or stroke | 105 (8.5) | 22 (7.1) | 83 (9.0) | 0.312 | 6 |
| Peripheral vascular disease | 111 (9.5) | 27 (9.3) | 84 (9.6) | 0.897 | 72 |
| Smoking | 345 (34.7) | 73 (28.0) | 272 (37.1) | 0.008 | 246 |
| Chronic lung disease | 146 (11.8) | 61 (19.7) | 85 (9.2) | <0.001 | 7 |
| Pulmonary embolism | 17 (1.4) | 9 (2.9) | 8 (0.9) | 0.008 | 6 |
| Previous percutaneous coronary intervention | 166 (13.5) | 25 (8.1) | 141 (15.3) | 0.001 | 8 |
| Previous coronary artery bypass grafting | 81 (6.6) | 9 (2.9) | 72 (7.8) | 0.003 | 7 |
| Previous ICD implantation | 28 (2.3) | 8 (2.6) | 20 (2.2) | 0.657 | 7 |
| Previous pacemaker implantation | 35 (2.8) | 12 (3.9) | 23 (2.5) | 0.201 | 7 |
| Medication use history | |||||
| Aspirin | 233 (19.0) | 44 (14.3) | 189 (20.5) | 0.016 | 11 |
| Antiplatelet therapy | 81 (6.6) | 13 (4.2) | 68 (7.4) | 0.053 | 10 |
| Oral anticoagulants | 175 (14.2) | 52 (16.8) | 123 (13.4) | 0.13 | 10 |
| ACE inhibitors | 221 (18.0) | 45 (14.6) | 176 (19.1) | 0.076 | 10 |
| Aldosterone antagonists | 1 (0.1) | 0 (0.0) | 1 (0.1) | 0.563 | 11 |
| Angiotensin-II blocker | 108 (8.8) | 29 (9.4) | 79 (8.6) | 0.649 | 10 |
| Beta blocker | 303 (24.7) | 73 (23.8) | 230 (24.9) | 0.681 | 11 |
| Calcium channel blocker | 98 (8.0) | 33 (10.7) | 65 (7.0) | 0.04 | 10 |
| Nitrates | 85 (6.9) | 19 (6.2) | 66 (7.2) | 0.553 | 10 |
| Diuretics | 235 (19.1) | 68 (22.1) | 167 (18.1) | 0.125 | 10 |
| Statins | 302 (24.6) | 55 (17.9) | 247 (26.8) | 0.002 | 10 |
| Non-statin lipids lowering agents | 19 (1.5) | 3 (1.0) | 16 (1.7) | 0.348 | 10 |
| Anti-arrhythmic | 57 (4.6) | 14 (4.5) | 43 (4.7) | 0.935 | 9 |
| Cardiac arrest characteristics | |||||
| Location of arrest | <0.001 | 0 | |||
| Home | 654 (52.7) | 211 (68.1) | 443 (47.6) | ||
| Public | 586 (47.3) | 99 (31.9) | 487 (52.4) | ||
| Witnessed arrest | 908 (76.4) | 215 (74.4) | 691 (77.0) | 0.358 | 54 |
| Bystander CPR | 768 (64.9) | 188 (64.8) | 580 (64.9) | 0.97 | 57 |
| Estimated time patient found until CPR | 0.535 | 234 | |||
| 0–5 min | 777 (77.2) | 185 (75.2) | 592 (77.9) | ||
| 6–10 min | 180 (17.9) | 51 (20.7) | 129 (17.0) | ||
| 11–20 min | 41 (4.1) | 8 (3.3) | 33 (4.3) | ||
| > 20 min | 8 (0.8) | 2 (0.8) | 6 (0.8) | ||
| Defibrillation by AED | 442 (36.0) | 90 (29.5) | 352 (38.2) | 0.006 | 13 |
| Initial rhythm | <0.001 | 65 | |||
| Shock | 924 (78.6) | 199 (67.2) | 725 (82.5) | ||
| Non-shock | 251 (21.4) | 97 (32.8) | 154 (17.5) | ||
| Defibrillation by EMS | 792 (64.1) | 175 (57.0) | 617 (66.5) | 0.003 | 5 |
| Time interval arrest to ROSC | 0.803 | 271 | |||
| 0–5 min | 78 (8.0) | 16 (6.6) | 62 (8.5) | ||
| 6–10 min | 191 (19.7) | 47 (19.4) | 144 (19.8) | ||
| 11–20 min | 392 (40.5) | 101 (41.7) | 291 (40.0) | ||
| > 20 min | 308 (31.8) | 78 (32.2) | 230 (31.6) | ||
| Intubation out of hospital | 713 (57.9) | 180 (58.8) | 533 (57.6) | 0.698 | 8 |
| Cause of arrest—no (%) | <0.001 | 74 | |||
| Cardiac cause | 1064 (91.3) | 234 (82.4) | 830 (94.1) | ||
| Non-cardiac cause | 102 (8.7) | 50 (17.6) | 52 (5.9) | ||
| GCS at ED | 0.945 | 303 | |||
| 3 to 6 | 596 (63.6) | 145 (62.8) | 451 (63.9) | ||
| 7 to 11 | 145 (15.5) | 36 (15.6) | 109 (15.4) | ||
| 11 to 15 | 196 (20.9) | 50 (21.6) | 146 (20.7) | ||
| Cardiac cause—no (%) | <0.001 | 0 | |||
| Acute myocardial infarction | 681 (64.4) | 131 (56.2) | 550 (66.7) | ||
| Old myocardial infarction | 121 (11.4) | 19 (8.2) | 102 (12.4) | ||
| Cardiomyopathy | 97 (9.2) | 24 (10.3) | 73 (8.8) | ||
| Primary rhythm or conduction disturbance | 108 (10.2) | 41 (17.6) | 67 (8.1) | ||
| Intoxication (heart medication) | 4 (0.4) | 1 (0.4) | 3 (0.4) | ||
| Cardiac tamponade | 1 (0.1) | 1 (0.4) | 0 (0.0) | ||
| Other | 15 (1.4) | 4 (1.7) | 11 (1.3) | ||
| Unknown cardiac cause | 31 (2.9) | 12 (5.2) | 19 (2.3) | ||
| Non-cardiac causes—no (%) | 0.451 | 0 | |||
| Epilepsy | 5 (5.0) | 1 (2.0) | 4 (7.8) | ||
| Trauma | 2 (2.0) | 1 (2.0) | 1 (2.0) | ||
| Intoxication | 10 (9.9) | 5 (10.0) | 5 (9.8) | ||
| Submersion | 6 (5.9) | 3 (6.0) | 3 (5.9) | ||
| Intracranial bleeding | 6 (5.9) | 3 (6.0) | 3 (5.9) | ||
| Pulmonary embolism | 18 (17.8) | 13 (26.0) | 5 (9.8) | ||
| Septic shock | 7 (6.9) | 3 (6.0) | 4 (7.8) | ||
| Asphyxia | 14 (13.9) | 4 (8.0) | 10 (19.6) | ||
| Hypoxia | 23 (22.8) | 13 (26.0) | 10 (19.6) | ||
| Other | 10 (9.9) | 4 (8.0) | 6 (11.8) |
| Total (N = 1240) | Women (N = 310) | Men (N = 930) | Missing Values (N) | p-Value | |
|---|---|---|---|---|---|
| 90-day mortality | 510 (41.1) | 142 (45.8) | 368 (40.0) | 0 | 0.053 |
| ICU length of stay (days) | 4.0 (2.0–7.0) | 4.0 (2.0–7.0) | 4.0 (3.0–7.0) | 36 | 0.084 |
| Favorable neurologic outcome, CPC 1–2 | 686 (55.3) | 155 (50.0) | 531 (57.0) | 44 | 0.038 |
| Poor neurologic outcome, CPC 3–5 | 510 (41.1) | 142 (45.8) | 368 (39.6) |
| Cox Regression Analysis for the Time to 90-Day Mortality after ICU Admission | ||
|---|---|---|
| Men | 1.150 (0.898–1.473) | |
| Age | 1.034 (1.025–1.042) | |
| Medical history | Hypercholesterolemia | 0.912 (0.710–1.170) |
| Former myocardial infarction | 1.064 (0.789–1.434) | |
| Chronic lung disease | 0.905 (0.672–1.218) | |
| Pulmonary embolism | 1.109 (0.564–2.180) | |
| Former PCI | 0.782 (0.547–1.119) | |
| Former CABG | 0.737 (0.480–1.132) | |
| Medication use history | Aspirin | 1.023 (0.775–1.350) |
| Calcium channel blocker | 0.896 (0.642–1.250) | |
| Statins | 0.933 (0.706–1.233) | |
| Cardiac arrest characteristics | Location of arrest | |
| Home | 1.606 (1.293–1.996) | |
| Public | Reference | |
| Defibrillation by AED | 0.540 (0.414–0.705) | |
| Initial rhythm | ||
| Shock | 0.380 (0.287–0.505) | |
| Non-shock | Reference | |
| Defibrillation by EMS | 1.106 (0.828–1.477) | |
| Cause of arrest | ||
| Cardiac | 0.623 (0.439–0.884) | |
| Non-cardiac | Reference | |
| N | 992 | |
| −2 LogLikelihood | 5,003,168 | |
| Chi-square (df, p-value) | 252.51 (16, <0.001) |
| Favorable CPC Score | ICU Length of Stay | ||
|---|---|---|---|
| (model 1) | (model 2) | ||
| Men | 1.123 (0.780–1.617) | 0.428 (−0.442 to 1.298) | |
| Age | 0.957 (0.946–0.969) | −0.024 (−0.051 to 0.003) | |
| Medical history | Hypercholesterolemia | 0.876 (0.599–1.281) | 0.017 (−0.893 to 0.927) |
| Former myocardial infarction | 1.065 (0.686–1.654) | 0.659 (−0.430 to 1.749) | |
| Chronic lung disease | 1.061 (0.650–1.733) | 0.063 (−1.090 to 1.216) | |
| Pulmonary embolism | 0.630 (0.196–2.031) | −0.537 (−3.398 to 2.325) | |
| Former PCI | 1.520 (0.901–2.563) | −0.319 (−1.570 to 0.932) | |
| Former CABG | 2.234 (1.167–4.280) | 0.069 (−1.490 to 1.627) | |
| Medication use history | Aspirin | 0.898 (0.568–1.419) | −0.659 (−1.744 to 0.426) |
| Calcium channel blocker | 0.973 (0.568–1.419) | 0.855 (−0.451 to 2.161) | |
| Statins | 1.105 (0.715–1.708) | −0.227 (−1.268 to 0.814) | |
| Cardiac arrest characteristics | Location of arrest | ||
| Home | 0.456 (0.336–0.619) | Reference | |
| Public | Reference | 0.056 (−0.675 to 0.787) | |
| Defibrillation by AED | 2.071 (1.457–2.945) | 0.259 (−0.585 to 1.104) | |
| Initial rhythm | |||
| Shock | Reference | 0.030 (−1.126 to 1.185) | |
| Non-shock | 0.194 (0.118–0.317) | Reference | |
| Defibrillation by EMS | 0.747 (0.488–1.145) | 0.648 (−0.309 to 1.606) | |
| Cause of arrest | |||
| Cardiac | 2.742 (1.376–5.465) | Reference | |
| Non-cardiac | Reference | −0.570 (−2.130 to 0.991) | |
| N | 960 | 969 | |
| F-test (df; p-value) | 0.882 (16,952; 0.590) | ||
| −2 LogLikelihood | 1051.10 | ||
| Likelihood ratio test p-value | <0.001 | ||
| (Nagelkerke) R-square | 0.303 | 0.015 | |
| AIC |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Wees, C.; Rietdijk, W.; Mandigers, L.; van der Graaf, M.; Scholte, N.T.B.; Adriaansens, K.O.; van den Berg, R.C.M.; den Uil, C.A. Do Women Have a Higher Mortality Risk Than Men following ICU Admission after Out-of-Hospital Cardiac Arrest? A Retrospective Cohort Analysis. J. Clin. Med. 2021, 10, 4286. https://doi.org/10.3390/jcm10184286
van Wees C, Rietdijk W, Mandigers L, van der Graaf M, Scholte NTB, Adriaansens KO, van den Berg RCM, den Uil CA. Do Women Have a Higher Mortality Risk Than Men following ICU Admission after Out-of-Hospital Cardiac Arrest? A Retrospective Cohort Analysis. Journal of Clinical Medicine. 2021; 10(18):4286. https://doi.org/10.3390/jcm10184286
Chicago/Turabian Stylevan Wees, Christiaan, Wim Rietdijk, Loes Mandigers, Marisa van der Graaf, Niels T. B. Scholte, Karst O. Adriaansens, Remco C. M. van den Berg, and Corstiaan A. den Uil. 2021. "Do Women Have a Higher Mortality Risk Than Men following ICU Admission after Out-of-Hospital Cardiac Arrest? A Retrospective Cohort Analysis" Journal of Clinical Medicine 10, no. 18: 4286. https://doi.org/10.3390/jcm10184286
APA Stylevan Wees, C., Rietdijk, W., Mandigers, L., van der Graaf, M., Scholte, N. T. B., Adriaansens, K. O., van den Berg, R. C. M., & den Uil, C. A. (2021). Do Women Have a Higher Mortality Risk Than Men following ICU Admission after Out-of-Hospital Cardiac Arrest? A Retrospective Cohort Analysis. Journal of Clinical Medicine, 10(18), 4286. https://doi.org/10.3390/jcm10184286