
Telemedicine Strategy to Rescue CPAP Therapy in Sleep Apnea Patients with Low Treatment Adherence: A Pilot Study

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
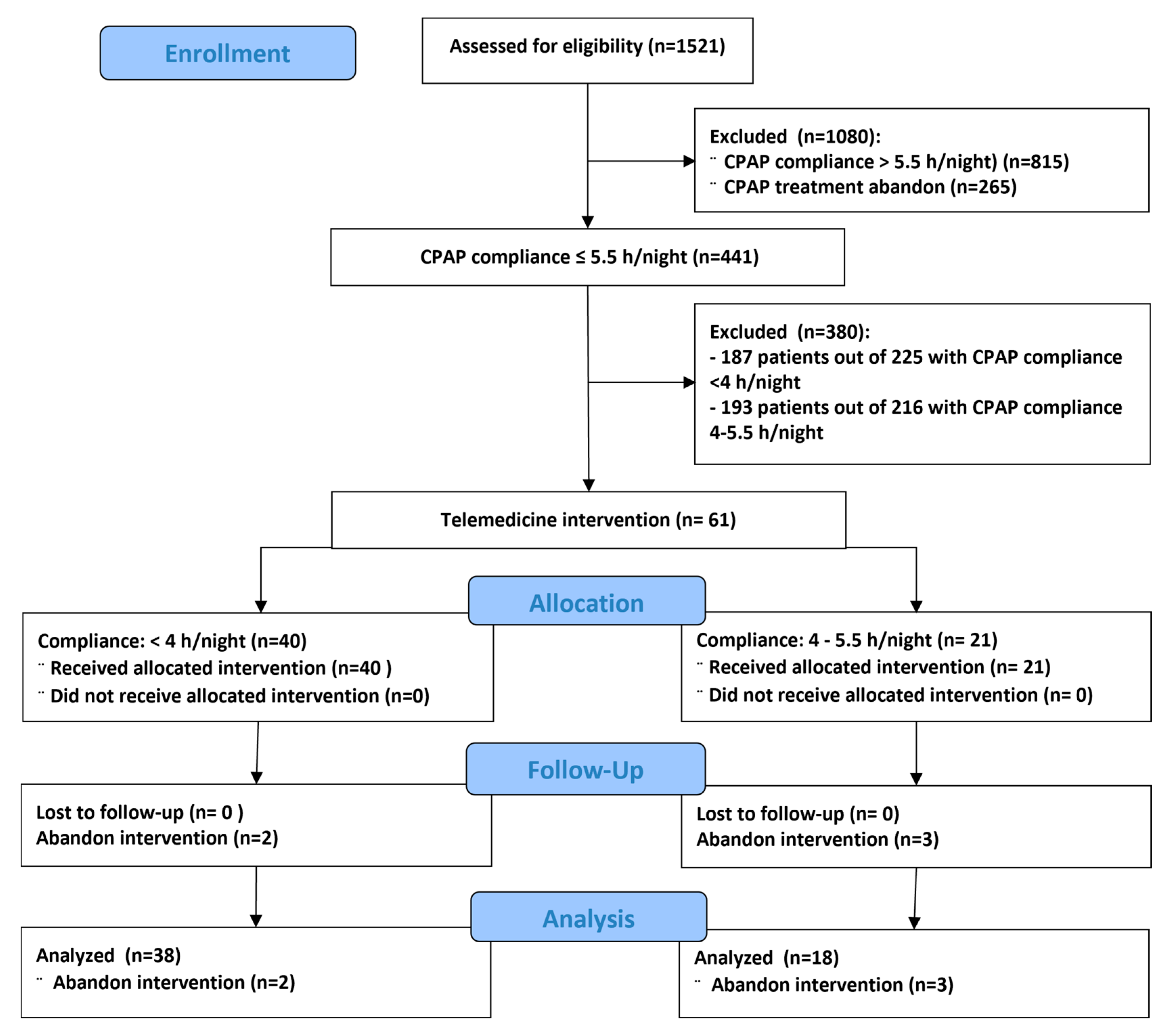
2.1. Patients
2.2. Intervention
2.3. Data Analysis
2.4. Cost Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bruyneel, M. Telemedicine in the diagnosis and treatment of sleep apnoea. Eur. Respir. Rev. 2019, 28, 180093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.L.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [Green Version]
- Jordan, A.S.; McSharry, D.G.; Malhotra, A. Adult obstructive sleep apnoea. Lancet 2014, 383, 736–747. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, C.E.; Issa, F.G.; Berthon-Jones, M.; Eves, L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet 1981, 1, 862–865. [Google Scholar] [CrossRef]
- Van Ryswyk, E.; Anderson, C.S.; Antic, N.A.; Barbe, F.; Bittencourt, L.; Freed, R.; Heeley, E.; Liu, Z.; Loffler, K.A.; Lorenzi-Filho, G.; et al. Predictors of long-term adherence to continuous positive airway pressure in patients with obstructive sleep apnea and cardiovascular disease. Sleep 2019, 42, zsz152. [Google Scholar] [CrossRef]
- McEvoy, R.D.; Antic, N.A.; Heeley, E.; Luo, Y.; Ou, Q.; Zhang, X.; Mediano, O.; Chen, R.; Drager, L.F.; Liu, Z.; et al. CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea. N. Engl. J. Med. 2016, 375, 919–931. [Google Scholar] [CrossRef]
- Askland, K.; Wright, L.; Wozniak, D.R.; Emmanuel, T.; Caston, J.; Smith, I. Educational, supportive and behavioural interventions to improve usage of continuous positive airway pressure machines in adults with obstructive sleep apnoea. Cochrane Database Syst. Rev. 2020, 4, CD007736. [Google Scholar] [CrossRef]
- Martínez-García, M.A.; Capote, F.; Campos-Rodríguez, F.; Lloberes, P.; Díaz de Atauri, M.J.; Somoza, M.; Masa, J.F.; González, M.; Sacristán, L.; Barbé, F.; et al. Effect of CPAP on blood pressure in patients with OSA and resistant hypertension: The HIPARCO trial. JAMA 2013, 310, 2407–2415. [Google Scholar] [CrossRef] [Green Version]
- Barbé, F.; Durán-Cantolla, J.; Capote, F.; de la Peña, M.; Chiner, E.; Masa, J.F.; Gonzalez, M.; Marín, J.M.; Garcia-Rio, F.; de Atauri, J.D.; et al. Long-term effect of continuous positive airway pressure in hypertensive patients with sleep apnea. Am. J. Respir. Crit. Care Med. 2010, 181, 718–726. [Google Scholar] [CrossRef] [Green Version]
- Weaver, T.E.; Maislin, G.; Dinges, D.F.; Bloxham, T.; George, C.F.; Greenberg, H.; Kader, G.; Mahowald, M.; Younger, J.; Pack, A.I. Relationship between hours of CPAP use and achieving normal levels of sleepiness and daily functioning. Sleep 2007, 30, 711–719. [Google Scholar] [CrossRef] [Green Version]
- Isetta, V.; Negrín, M.A.; Monasterio, C.; Masa, J.F.; Feu, N.; Álvarez, A.; Campos-Rodriguez, F.; Ruiz, C.; Abad, J.; Vazquez-Polo, F.J.; et al. A Bayesian cost-effectiveness analysis of a telemedicine-based strategy for the management of sleep apnoea: A multicentre randomised controlled trial. Thorax 2015, 70, 1054–1061. [Google Scholar] [CrossRef] [Green Version]
- Suarez-Giron, M.; Garmendia, O.; Lugo, V.; Ruiz, C.; Salord, N.; Alsina, X.; Farré, R.; Montserrat, J.M.; Torres, M. Mobile health application to support CPAP therapy in obstructive sleep apnoea: Design, feasibility and perspectives. ERJ Open Res. 2020, 6, 00220-2019. [Google Scholar] [CrossRef] [Green Version]
- Pépin, J.L.; Tamisier, R.; Hwang, D.; Mereddy, S.; Parthasarathy, S. Does remote monitoring change OSA management and CPAP adherence? Respirology 2017, 22, 1508–1517. [Google Scholar] [CrossRef]
- Shamim-Uzzaman, Q.A.; Bae, C.J.; Ehsan, Z.; Setty, A.R.; Devine, M.; Dhankikar, S.; Donskoy, I.; Fields, B.; Hearn, H.; Hwang, D.; et al. The use of telemedicine for the diagnosis and treatment of sleep disorders: An American Academy of Sleep Medicine update. J. Clin. Sleep Med. 2021, 17, 1103–1107. [Google Scholar] [CrossRef]
- Garmendia, O.; Monasterio, C.; Guzmán, J.; Saura, L.; Ruiz, C.; Salord, N.; Negrín, M.A.; Izquierdo Sanchez, C.; Suarez-Girón, M.; Montserrat, J.M.; et al. Telemedicine Strategy for CPAP Titration and Early Follow-up for Sleep Apnea During COVID-19 and Post-Pandemic Future. Arch. Bronconeumol. 2021, 57 (Suppl. 2), 56–58. [Google Scholar] [CrossRef]
- Kuna, S.T. Optimizing Chronic Management of Adults with Obstructive Sleep Apnea. Ann. Am. Thorac. Soc. 2020, 17, 280–281. [Google Scholar] [CrossRef]
- Lugo, V.; Villanueva, J.A.; Garmendia, O.; Montserrat, J.M. The role of telemedicine in obstructive sleep apnea management. Expert Rev. Respir. Med. 2017, 11, 699–709. [Google Scholar] [CrossRef]
- Hwang, D.; Chang, J.W.; Benjafield, A.V.; Crocker, M.E.; Kelly, C.; Becker, K.A.; Kim, J.B.; Woodrum, R.R.; Liang, J.; Derose, S.F. Effect of Telemedicine Education and Telemonitoring on Continuous Positive Airway Pressure Adherence. The Tele-OSA Randomized Trial. Am. J. Respir. Crit. Care Med. 2018, 197, 117–126. [Google Scholar] [CrossRef]
- Fietze, I.; Herberger, S.; Wewer, G.; Woehrle, H.; Lederer, K.; Lips, A.; Willes, L.; Penzel, T. Initiation of therapy for obstructive sleep apnea syndrome: A randomized comparison of outcomes of telemetry-supported home-based vs. sleep lab-based therapy initiation. Sleep Breath. 2021, in press. [Google Scholar] [CrossRef]
- Frasnelli, M.; Baty, F.; Niedermann, J.; Brutsche, M.H.; Schoch, O.D. Effect of telemetric monitoring in the first 30 days of continuous positive airway pressure adaptation for obstructive sleep apnoea syndrome—A controlled pilot study. J. Telemed. Telecare 2016, 22, 209–214. [Google Scholar] [CrossRef]
- Aardoom, J.J.; Loheide-Niesmann, L.; Ossebaard, H.C.; Riper, H. Effectiveness of eHealth Interventions in Improving Treatment Adherence for Adults With Obstructive Sleep Apnea: Meta-Analytic Review. J. Med. Internet Res. 2020, 22, e16972. [Google Scholar] [CrossRef] [PubMed]
- Pépin, J.L.; Bailly, S.; Rinder, P.; Adler, D.; Szeftel, D.; Malhotra, A.; Cistulli, P.A.; Benjafield, A.; Lavergne, F.; Josseran, A.; et al. CPAP Therapy Termination Rates by OSA Phenotype: A French Nationwide Database Analysis. J. Clin. Med. 2021, 10, 936. [Google Scholar] [CrossRef] [PubMed]
- Peker, Y.; Glantz, H.; Eulenburg, C.; Wegscheider, K.; Herlitz, J.; Thunström, E. Effect of Positive Airway Pressure on Cardiovascular Outcomes in Coronary Artery Disease Patients with Nonsleepy Obstructive Sleep Apnea. The RICCADSA Randomized Controlled Trial. Am. J. Respir. Crit. Care Med. 2016, 194, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Bakker, J.P.; Weaver, T.E.; Parthasarathy, S.; Aloia, M.S. Adherence to CPAP: What Should We Be Aiming For, and How Can We Get There? Chest 2019, 155, 1272–1287. [Google Scholar] [CrossRef] [PubMed]
- Murase, K.; Tanizawa, K.; Minami, T.; Matsumoto, T.; Tachikawa, R.; Takahashi, N.; Tsuda, T.; Toyama, Y.; Ohi, M.; Akahoshi, T.; et al. A Randomized Controlled Trial of Telemedicine for Long-Term Sleep Apnea Continuous Positive Airway Pressure Management. Ann. Am. Thorac. Soc. 2020, 17, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Rossi, V.A.; Stoewhas, A.C.; Camen, G.; Steffel, J.; Bloch, K.E.; Stradling, J.R.; Kohler, M. The effects of continuous positive airway pressure therapy withdrawal on cardiac repolarization: Data from a randomized controlled trial. Eur. Heart J. 2012, 33, 2206–2212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guest, J.F.; Helter, M.T.; Morga, A.; Stradling, J.R. Cost effectiveness of using continuous positive airway pressure in the treatment of severe obstructive sleep apnoea/hypopnoea syndrome in the UK. Thorax 2008, 63, 860–865. [Google Scholar] [CrossRef] [Green Version]
- Kapur, V.; Blough, D.K.; Sandblom, R.E.; Hert, R.; de Maine, J.B.; Sullivan, S.D.; Psaty, B.M. The medical cost of undiagnosed sleep apnoea. Sleep 1999, 22, 749–755. [Google Scholar] [CrossRef] [Green Version]
- Knauert, M.; Naik, S.; Gillespie, M.B.; Kryer, M. Clinical consequences and economic costs of untreated obstructive sleep apnea syndrome. World J. Otorhinolaryngol. Head Neck Surg. 2015, 1, 17–27. [Google Scholar] [CrossRef] [Green Version]
- Farré, R.; Navajas, D.; Montserrat, J.M. Is Telemedicine a Key Tool for Improving Continuous Positive Airway Pressure Adherence in Patients with Sleep Apnea? Am. J. Respir. Crit. Care Med. 2018, 197, 12–14. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | 56 |
| Gender (male; %) | 78.6 |
| Age (yr; m ± SD) | 57.9 ± 8.9 |
| Apnea-hypopnea index (events/h; m ± SD) | 45.8 ± 20.1 |
| Time on CPAP therapy (yr; m ± SD) | 2.46 ± 0.90 |
| Main Comorbidity: | |
| Cardiovascular (%) | 41.1 |
| Metabolic (%) | 39.3 |
| Neurological (%) | 1.8 |
| Respiratory (%) | 19.6 |
| Depression (%) | 12.5 |
| Neurological (%) | 1.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garmendia, O.; Farré, R.; Ruiz, C.; Suarez-Girón, M.; Torres, M.; Cebrian, R.; Saura, L.; Monasterio, C.; Negrín, M.A.; Montserrat, J.M. Telemedicine Strategy to Rescue CPAP Therapy in Sleep Apnea Patients with Low Treatment Adherence: A Pilot Study. J. Clin. Med. 2021, 10, 4123. https://doi.org/10.3390/jcm10184123
Garmendia O, Farré R, Ruiz C, Suarez-Girón M, Torres M, Cebrian R, Saura L, Monasterio C, Negrín MA, Montserrat JM. Telemedicine Strategy to Rescue CPAP Therapy in Sleep Apnea Patients with Low Treatment Adherence: A Pilot Study. Journal of Clinical Medicine. 2021; 10(18):4123. https://doi.org/10.3390/jcm10184123
Chicago/Turabian StyleGarmendia, Onintza, Ramon Farré, Concepción Ruiz, Monique Suarez-Girón, Marta Torres, Raisa Cebrian, Laura Saura, Carmen Monasterio, Miguel A. Negrín, and Josep M. Montserrat. 2021. "Telemedicine Strategy to Rescue CPAP Therapy in Sleep Apnea Patients with Low Treatment Adherence: A Pilot Study" Journal of Clinical Medicine 10, no. 18: 4123. https://doi.org/10.3390/jcm10184123
APA StyleGarmendia, O., Farré, R., Ruiz, C., Suarez-Girón, M., Torres, M., Cebrian, R., Saura, L., Monasterio, C., Negrín, M. A., & Montserrat, J. M. (2021). Telemedicine Strategy to Rescue CPAP Therapy in Sleep Apnea Patients with Low Treatment Adherence: A Pilot Study. Journal of Clinical Medicine, 10(18), 4123. https://doi.org/10.3390/jcm10184123