
Safety and Efficacy of Cryoballoon Based Pulmonary Vein Isolation in Patients with Atrial Fibrillation and a History of Cancer

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Cryoballoon-Based Pulmonary Vein Isolation
2.3. Ablation Protocol
2.4. Postprocedural Care and Follow-Up
2.5. Definition of Complications and Cancer Activity
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Specific Disease Related Characteristics in Patients with a History of Cancer
3.3. Procedural Data
3.4. Periprocedural Complications
3.5. Arrhythmia Follow-Up and Repeat Ablation Procedures
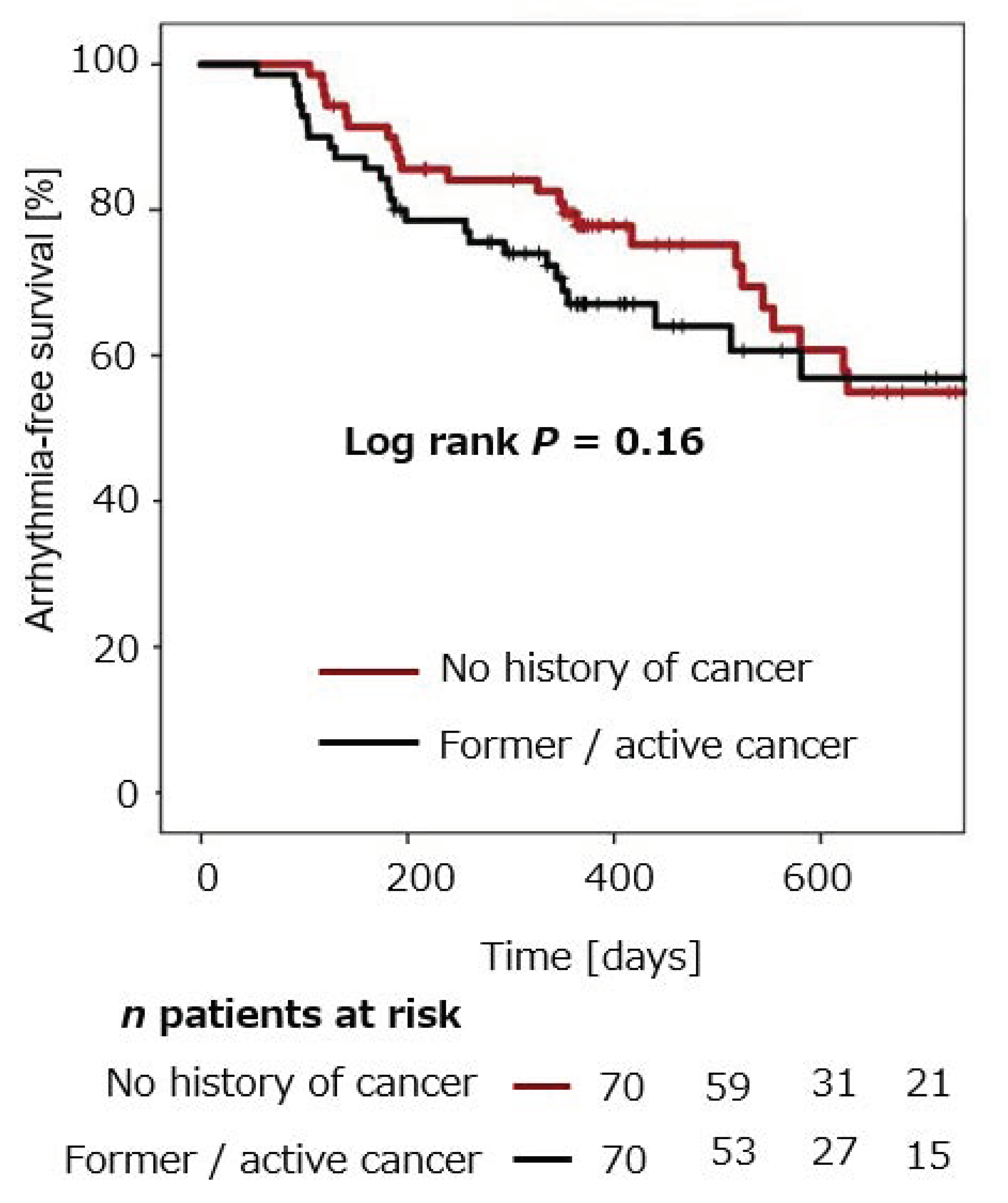
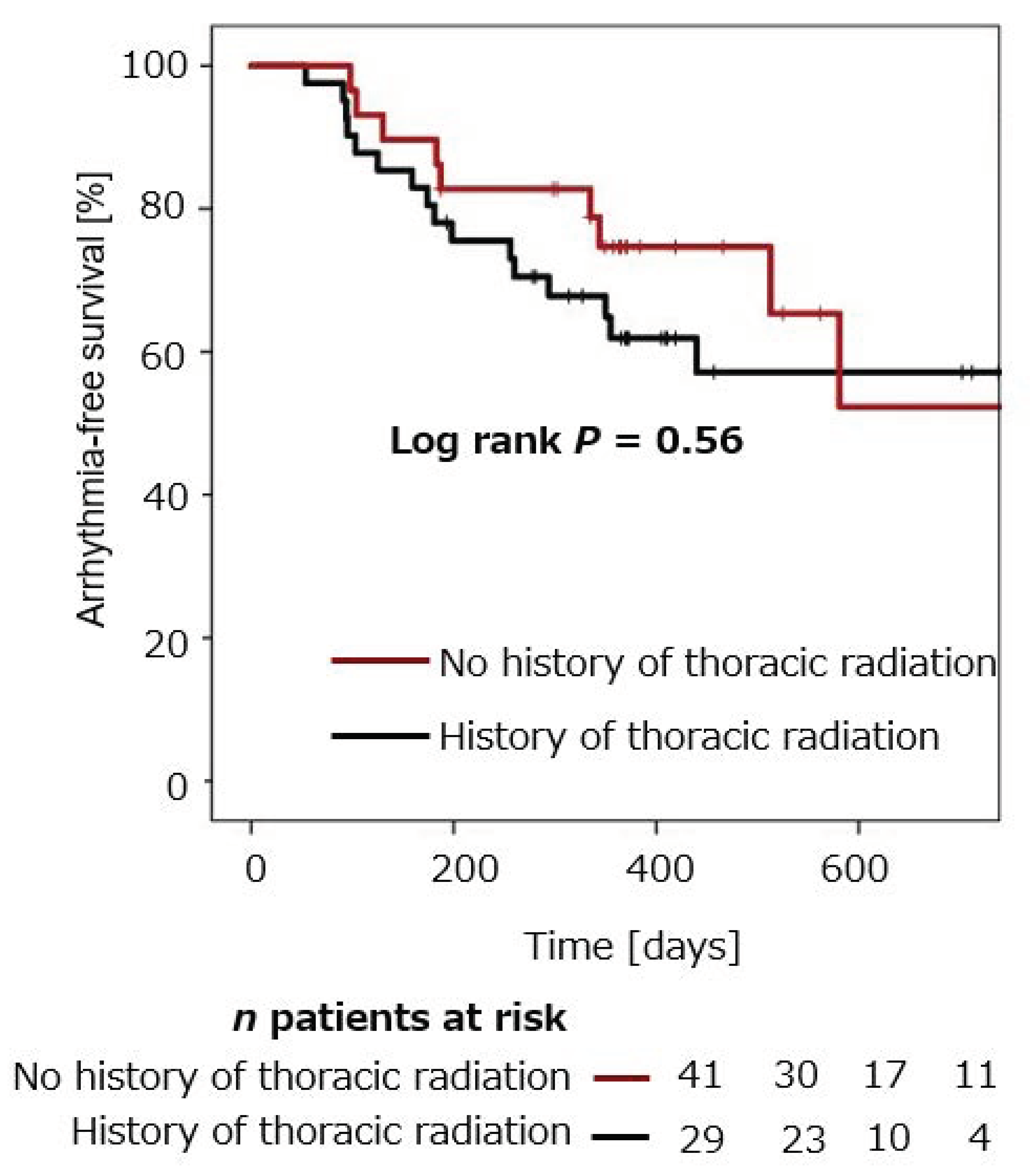
3.6. Estimation of Arrhythmia-Free Survival
4. Discussion
4.1. Atrial Fibrillation Ablation in Patients with Cancer Disease
4.2. Cryoballoon Ablation in Patients with Previous Thoracic Radiation
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AF | Atrial Fibrillation |
| AT | atrial tachycardia |
| BMI | body mass index |
| CB-PVI | cryoballoon-based pulmonary vein isolation |
| LSPV | left superior pulmonary vein |
| LIPV | left inferior pulmonary vein |
| PNP | phrenic nerve palsy |
| PVI | pulmonary vein isolation |
| RSPV | right superior pulmonary vein |
| RIPV | right inferior pulmonary vein |
References
- Chu, G.; Versteeg, H.H.; Verschoor, A.; Trines, S.; Hemels, M.E.; Ay, C.; Huisman, M.V.; Klok, E. Atrial fibrillation and cancer—An unexplored field in cardiovascular oncology. Blood Rev. 2019, 35, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Rahman, F.; Ko, D.; Benjamin, E.J. Association of Atrial Fibrillation and Cancer. JAMA Cardiol. 2016, 1, 384–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farmakis, D.; Parissis, J.; Filippatos, G. Insights into onco-cardiology: Atrial fibrillation in cancer. J. Am. Coll. Cardiol. 2014, 63, 945–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Neal, W.T.; Lakoski, S.G.; Qureshi, W.; Judd, S.E.; Howard, G.; Howard, V.J.; Cushman, M.; Soliman, E.Z. Relation between cancer and atrial fibrillation (from the REasons for Geographic And Racial Differences in Stroke Study). Am. J. Cardiol. 2015, 115, 1090–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, C.S.; Chang, C.H.; Lin, J.W.; Ho, Y.L.; Chen, M.F. The association between new onset atrial fibrillation and incident cancer-A nationwide cohort study. PLoS ONE 2018, 13, e0199901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostenfeld, E.B.; Erichsen, R.; Pedersen, L.; Farkas, D.K.; Weiss, N.S.; Sørensen, H.T. Atrial fibrillation as a marker of occult cancer. PLoS ONE 2014, 9, e102861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kattelus, H.; Kesäniemi, Y.A.; Huikuri, H.; Ukkola, O. Cancer increases the risk of atrial fibrillation during long-term follow-up (OPERA study). PLoS ONE 2018, 13, e0205454. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.; Delgado, J.M.; Moltò, J.M.; Vicent, J.M.; Manzanares, R.; Insa, R.; Matìas-Guiu, J. Cardiovascular reflexes in patients with malignant disease. Neurol. Sci. 1992, 13, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Guzzetti, S.; Costantino, G.; Fundarò, C. Systemic Inflammation, Atrial Fibrillation, and Cancer. Circulation 2002, 106, e40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuck, K.-H.; Brugada, J.; Fürnkranz, A.; Metzner, A.; Ouyang, F.; Chun, K.J.; Elvan, A.; Arentz, T.; Bestehorn, K.; Pocock, S.J.; et al. Cryoballoon or Radiofrequency Ablation for Paroxysmal Atrial Fibrillation. N. Engl. J. Med. 2016, 374, 2235–2245. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, J.; Sepahpour, A.; Chan, K.H.; Singarayar, S.; McGuire, M.A. Immediate balloon deflation for prevention of persistent phrenic nerve palsy during pulmonary vein isolation by balloon cryoablation. Heart Rhythm. 2013, 10, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Calkins, H.; Hindricks, G.; Cappato, R.; Kim, Y.; Saad, E.B.; Aguinaga, L.; Akar, J.G.; Badhwar, V.; Brugada, J.; Camm, J.; et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace 2018, 20, e1–e160. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ording, A.G.; Horváth-Puhó, E.; Adelborg, K.; Pedersen, L.; Prandoni, P.; Sørensen, H.T. Thromboembolic and bleeding complications during oral anticoagulation therapy in cancer patients with atrial fibrillation: A Danish nationwide population-based cohort study. Cancer Med. 2017, 6, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Sturgeon, K.M.; Deng, L.; Bluethmann, S.M.; Zhou, S.; Trifiletti, D.M.; Jiang, C.; Kelly, S.; Zaorsky, N.G. A population-based study of cardiovascular disease mortality risk in US cancer patients. Eur. Heart J. 2019, 40, 3889–3897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giustozzi, M.; Ali, H.; Reboldi, G.; Balla, C.; Foresti, S.; de Ambroggi, G.; Lupo, P.P.; Agnelli, G.; Cappato, R. Safety of catheter ablation of atrial fibrillation in cancer survivors. J. Interv. Card. Electrophysiol. 2021, 60, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Di Biase, L.; Burkhardt, J.D.; Santangeli, P.; Mohanty, P.; Sanchez, J.E.; Horton, R.; Gallinghouse, G.J.; Themistoclakis, S.; Rossillo, A.; Lakkireddy, D.; et al. Periprocedural stroke and bleeding complications in patients undergoing catheter ablation of atrial fibrillation with different anticoagulation management: Results from the Role of Coumadin in Preventing Thromboembolism in Atrial Fibrillation (AF) Patients Undergoing Catheter Ablation (COMPARE) randomized trial. Circulation 2014, 129, 2638–2644. [Google Scholar] [PubMed] [Green Version]
- Heeger, C.-H.; Subin, B.; Wissner, E.; Fink, T.; Mathew, S.; Maurer, T.; Lemes, C.; Rillig, A.; Wohlmuth, P.; Reissmann, B.; et al. Second-generation cryoballoon-based pulmonary vein isolation: Lessons from a five-year follow-up. Int. J. Cardiol. 2020, 312, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Mery, B.; Guichard, J.-B.; Guy, J.-B.; Vallard, A.; Barthelemy, J.-C.; Da Costa, A.; Magné, N.; Bertoletti, L. Atrial fibrillation in cancer patients: Hindsight, insight and foresight. Int. J. Cardiol. 2017, 240, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Hashiguchi, N.; Schenker, N.; Rottner, L.; Reißmann, B.; Rillig, A.; Maurer, T.; Lemes, C.; Kuck, K.-H.; Ouyang, F.; Mathew, S. Absence of detectable effect of radiotherapy and chemotherapy for breast cancer on the presence of low voltage areas in patients receiving left atrial catheter ablation. Acta Cardiol. 2020, 11, 1–8. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| No Cancer N = 70 | Cancer N = 70 | p-Value | |
|---|---|---|---|
| Age (years); mean ± SD | 69.7 ± 8.7 | 71.3 ± 8.3 | 0.27 |
| Sex, male; n (%) | 39 (55.7) | 39 (55.7) | 1.00 |
| BMI, kg/m2; mean ± SD | 28.0 ± 6.5 | 27.6 ± 5.9 | 0.70 |
| Paroxysmal AF, n (%) | 23 (32.9) | 22 (31.4) | 0.86 |
| Persistent AF, n (%) | 47 (67.1) | 48 (68.6) | 0.86 |
| CHA2DS2-VASC score; median (IQR) | 3 (2;4) | 3 (2;4) | 0.15 |
| Oral anticoagulation with DOAC, n (%) | 55 (78.6) | 56 (80) | 1.0 |
| Oral anticoagulation with vitamin K antagonist, n (%) | 15 (21.4%) | 14 (20) | 1.0 |
| Medical History | |||
| Arterial Hypertension; n (%) | 55 (78.6) | 49 (70) | 0.33 |
| Coronary Artery Disease; n (%) | 10 (14.3) | 12 (17.1) | 0.81 |
| Chronic Renal Insufficiency; n (%) | 17 (24.3) | 22 (31.4) | 0.45 |
| Diabetes mellitus | 7 (10) | 6 (8.6) | 1.00 |
| Implanted cardiac device (%) | 11 (15.7) | 12 (17.1) | 1.00 |
| LVEF (%); mean ± SD | 52.2 ± 8.7 | 50.4 ± 11.6 | 0.30 |
| No Cancer N = 70 | Cancer N = 70 | p-Value | |
|---|---|---|---|
| Procedure duration (min); mean ± SD | 137.9 ± 27.3 | 116.4 ± 42.4 | <0.001 |
| Fluoroscopy time (min); mean ± SD | 24.8 ± 8.5 | 18.2 ± 9.8 | <0.001 |
| Number of freezes RSPV; mean ± SD | 1.3 ± 0.6 | 1.4 ± 0.8 | 0.40 |
| Number of freezes RIPV; mean ± SD | 1.4 ± 0.6 | 1.4 ± 0.6 | 1.00 |
| Number of freezes LSPV; mean ± SD | 1.5 ± 0.7 | 1.4 ± 0.5 | 0.33 |
| Number of freezes LIPV; mean ± SD | 1.3 ± 0.5 | 1.4 ± 0.7 | 0.33 |
| Common left ostium; n (%) | 11 (15.7) | 4 (5.7) | 0.10 |
| Real time isolation RSPV; n (%) | 49 (70) | 29 (41.4) | 0.001 |
| Real time isolation RIPV; n (%) | 45 (64.3) | 15 (21.4) | <0.001 |
| Real time isolation LSPV; n (%) | 31 (44.3) | 29 (41.4) | 0.86 |
| Real time isolation LIPV; n (%) | 43 (61.4) | 25 (35.7) | 0.004 |
| Freezing time RSPV (s); mean ± SD | 249.9 ± 136.8 | 223.1 ± 94.5 | 0.18 |
| Freezing time RIPV (s); mean ± SD | 291.1 ± 151.9 | 278.9 ± 136.3 | 0.62 |
| Freezing time LSPV (s); mean ± SD | 304.1 ± 153.5 | 250.9 ± 104.6 | 0.02 |
| Freezing time LIPV (s); mean ± SD | 266.8 ± 122.1 | 260.9 ± 136.8 | 0.79 |
| Complications | |||
| Phrenic nerve palsy, n (%) | 1 (1.4) | 4 (5.7) | 0.36 |
| Pseudoaneurysm, n (%) | 1 (1.4) | 2 (2.8) | 1.0 |
| No Cancer N = 70 | Cancer N = 70 | p-Value | |
|---|---|---|---|
| Arrhythmia recurrence, n (%) | 26 (37.1) | 32 (45.7) | 0.23 |
| Mode of arrhythmia recurrence | |||
| AF, n (%) | 21 (80.8) | 27 (84.4) | 0.92 |
| AT, n (%) | 4 (15.4) | 5 (15.6) | 0.92 |
| Repeat ablation, n (%) | 16 (22.9) | 8 (11.4) | 0.11 |
| AF at repeat procedure, n (%) | 9 (56.3) | 2 (25) | 0.23 |
| AT at repeat procedure, n (%) | 7 (43.8) | 6 (75) | 0.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eitel, C.; Sciacca, V.; Bartels, N.; Saraei, R.; Fink, T.; Keelani, A.; Gaßmann, A.; Kuck, K.-H.; Vogler, J.; Heeger, C.-H.; et al. Safety and Efficacy of Cryoballoon Based Pulmonary Vein Isolation in Patients with Atrial Fibrillation and a History of Cancer. J. Clin. Med. 2021, 10, 3669. https://doi.org/10.3390/jcm10163669
Eitel C, Sciacca V, Bartels N, Saraei R, Fink T, Keelani A, Gaßmann A, Kuck K-H, Vogler J, Heeger C-H, et al. Safety and Efficacy of Cryoballoon Based Pulmonary Vein Isolation in Patients with Atrial Fibrillation and a History of Cancer. Journal of Clinical Medicine. 2021; 10(16):3669. https://doi.org/10.3390/jcm10163669
Chicago/Turabian StyleEitel, Charlotte, Vanessa Sciacca, Nina Bartels, Roza Saraei, Thomas Fink, Ahmad Keelani, André Gaßmann, Karl-Heinz Kuck, Julia Vogler, Christian-Hendrik Heeger, and et al. 2021. "Safety and Efficacy of Cryoballoon Based Pulmonary Vein Isolation in Patients with Atrial Fibrillation and a History of Cancer" Journal of Clinical Medicine 10, no. 16: 3669. https://doi.org/10.3390/jcm10163669
APA StyleEitel, C., Sciacca, V., Bartels, N., Saraei, R., Fink, T., Keelani, A., Gaßmann, A., Kuck, K.-H., Vogler, J., Heeger, C.-H., & Tilz, R. R. (2021). Safety and Efficacy of Cryoballoon Based Pulmonary Vein Isolation in Patients with Atrial Fibrillation and a History of Cancer. Journal of Clinical Medicine, 10(16), 3669. https://doi.org/10.3390/jcm10163669