
SARS-CoV-2 and Acute Cerebrovascular Events: An Overview

 ,
,  , ,
, ,
Abstract
:1. Introduction
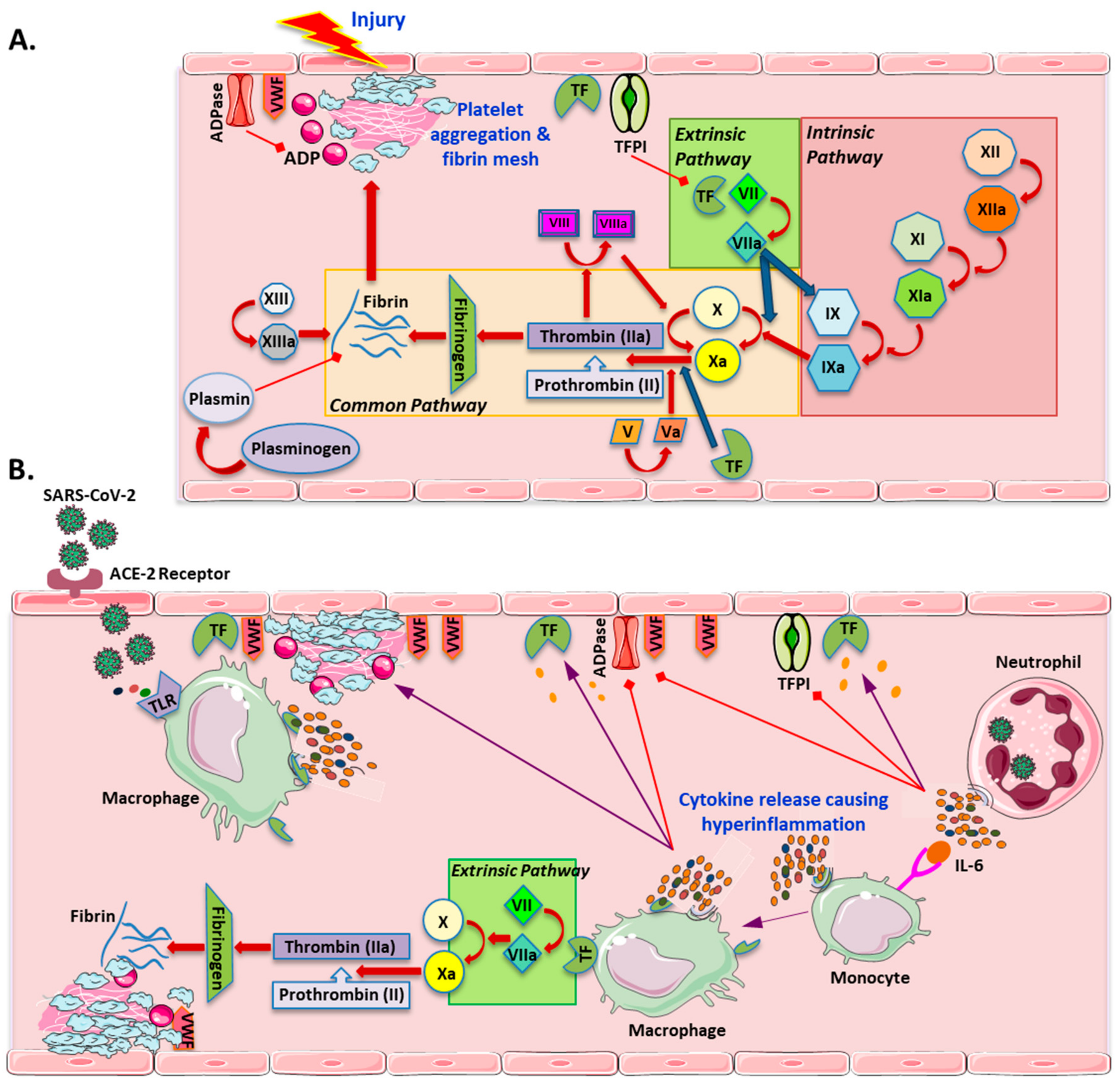
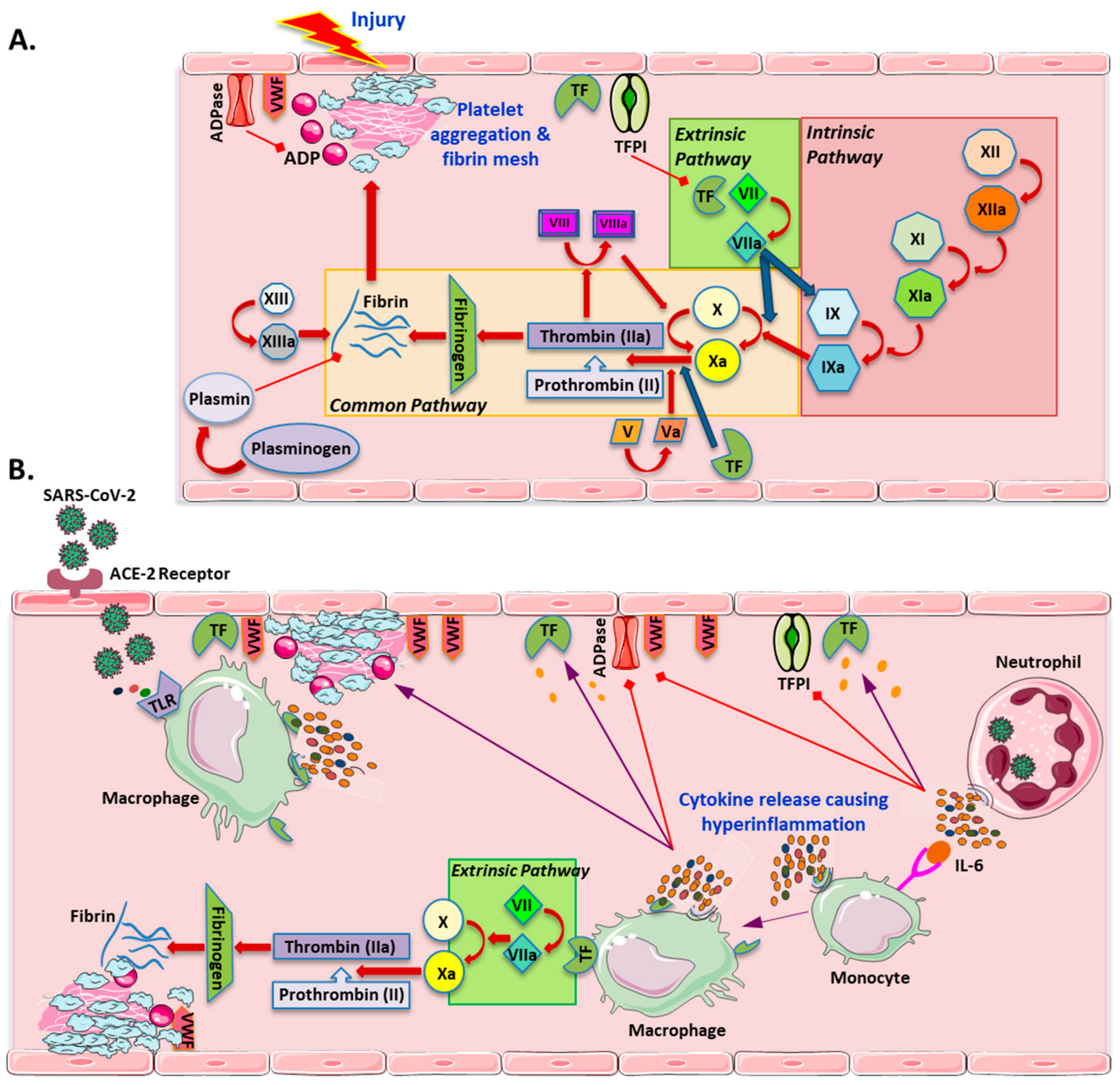
2. Hypercoagulability Related to SARS-CoV-2
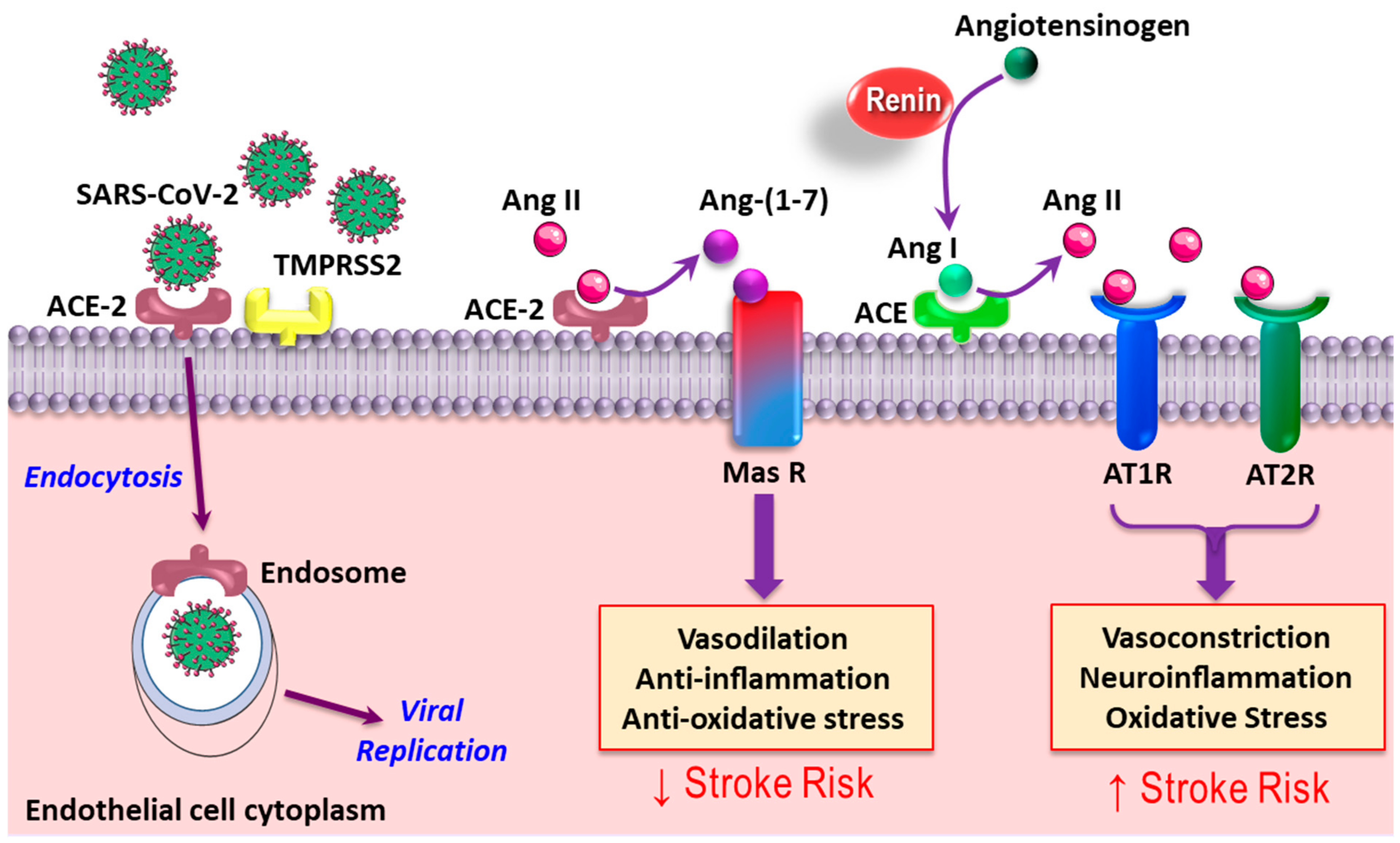
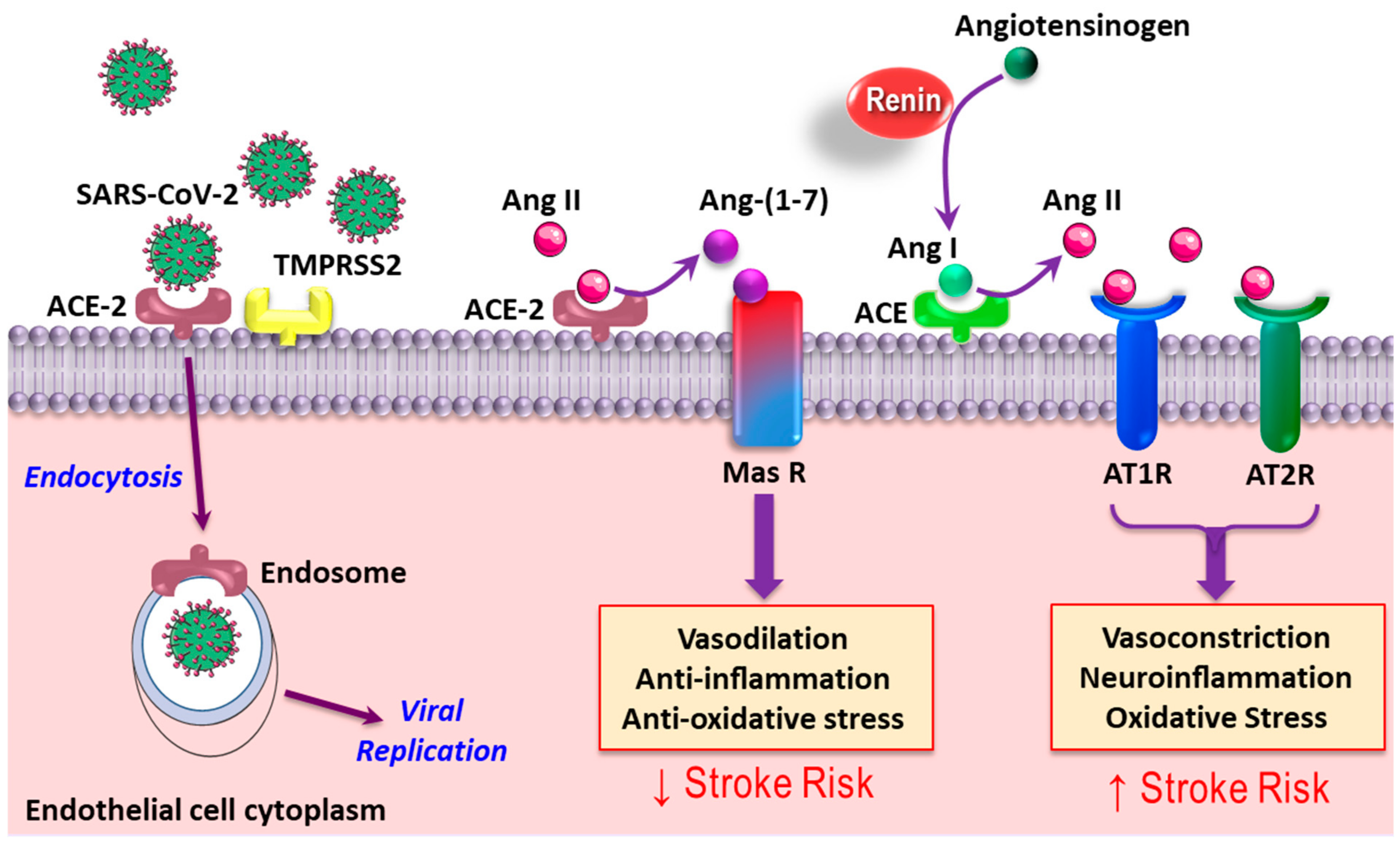
3. SARS-CoV-2 and Angiotensin-Converting Enzyme 2
4. Acute Cerebrovascular Events in COVID-19
4.1. Ischemic Stroke
4.2. Hemorrhagic Stroke
4.3. Cerebral Venous Thrombosis
5. Therapeutic Approaches
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 41, 145–151. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Li, Y.C.; Bai, W.Z.; Hashikawa, T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J. Med. Virol. 2020, 92, 552–555. [Google Scholar] [CrossRef]
- Nordvig, A.S.; Rimmer, K.T.; Willey, J.Z.; Thakur, K.T.; Boehme, A.K.; Vargas, W.S.; Smith, C.J.; Elkind, M.S.V. Potential Neurologic Manifestations of COVID-19. Neurol. Clin. Pract. 2020, 11, e135–e146. [Google Scholar] [CrossRef]
- Keyhanian, K.; Umeton, R.P.; Mohit, B.; Davoudi, V.; Hajighasemi, F.; Ghasemi, M. SARS-CoV-2 and nervous system: From pathogenesis to clinical manifestation. J. Neuroimmunol. 2021, 350, 577436. [Google Scholar] [CrossRef]
- Hartung, H.-P.; Aktas, O. COVID-19 and management of neuroimmunological disorders. Nat. Rev. Neurol. 2020, 16, 347–348. [Google Scholar] [CrossRef]
- Chen, J.; Vitetta, L. Gut-brain axis in the neurological comorbidity of COVID-19. Brain Commun. 2021, 3, fcab118. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Wu, Z.; Zhang, M.; Liu, S.; Zhou, L.; Yang, C.; Liu, C. The Role of the Gastrointestinal System in Neuroinvasion by SARS-CoV-2. Front. Neurosci. 2021, 15, 694446. [Google Scholar] [CrossRef]
- Deana, C.; Verriello, L.; Pauletto, G.; Corradi, F.; Forfori, F.; Cammarota, G.; Bignami, E.; Vetrugno, L.; Bove, T. Insights into neurological dysfunction of critically ill COVID-19 patients. Trends Anaesth. Crit. Care 2021, 36, 30–38. [Google Scholar] [CrossRef]
- Battaglini, D.; Brunetti, I.; Anania, P.; Fiaschi, P.; Zona, G.; Ball, L.; Giacobbe, D.R.; Vena, A.; Bassetti, M.; Patroniti, N.; et al. Neurological Manifestations of Severe SARS-CoV-2 Infection: Potential Mechanisms and Implications of Individualized Mechanical Ventilation Settings. Front. Neurol. 2020, 11, 845. [Google Scholar] [CrossRef] [PubMed]
- Oddo, M.; Nduom, E.; Frangos, S.; MacKenzie, L.; Chen, I.; Maloney-Wilensky, E.; Kofke, W.A.; Levine, J.M.; Leroux, P.D. Acute Lung Injury Is an Independent Risk Factor for Brain Hypoxia after Severe Traumatic Brain Injury. Neurosurgery 2010, 67, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Beyrouti, R.; Adams, M.E.; Benjamin, L.; Cohen, H.; Farmer, S.F.; Goh, Y.Y.; Humphries, F.; Jäger, H.R.; Losseff, N.A.; Perry, R.J.; et al. Characteristics of ischaemic stroke associated with COVID-19. J. Neurol. Neurosurg. Psychiatry 2020, 91, 889–891. [Google Scholar] [CrossRef] [PubMed]
- Al Saiegh, F.; Ghosh, R.; Leibold, A.; Avery, M.B.; Schmidt, R.F.; Theofanis, T.; Mouchtouris, N.; Philipp, L.; Peiper, S.C.; Wang, Z.-X.; et al. Status of SARS-CoV-2 in cerebrospinal fluid of patients with COVID-19 and stroke. J. Neurol. Neurosurg. Psychiatry 2020, 91, 846–848. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Poillon, G.; Obadia, M.; Perrin, M.; Savatovsky, J.; Lecler, A. Cerebral venous thrombosis associated with COVID-19 infection: Causality or coincidence? J. Neuroradiol. 2020. [Google Scholar] [CrossRef]
- Bielosludtseva, K.; Pertseva, T.; Kirieieva, T.; Krykhtina, M. Dynamic changes of markers of endothelial function, hemostasis, fibrinolysis and inflammation in hospitalized patients with community-acquired pneumonia. Eur. Resp. J. 2019, 54, PA5452. [Google Scholar] [CrossRef]
- Violi, F.; Oliva, A.; Cangemi, R.; Ceccarelli, G.; Pignatelli, P.; Carnevale, R.; Cammisotto, V.; Lichtner, M.; Alessandri, F.; De Angelis, M.; et al. Nox2 activation in COVID-19. Redox Biol. 2020, 36, 101655. [Google Scholar] [CrossRef]
- Zhang, C.; Wu, Z.; Li, J.-W.; Zhao, H.; Wang, G.-Q. The cytokine release syndrome (CRS) of severe COVID-19 and Interleukin-6 receptor (IL-6R) antagonist Tocilizumab may be the key to reduce the mortality. Int. J. Antimicrob. Agents 2020, 55, 105954. [Google Scholar] [CrossRef]
- Divani, A.A.; Andalib, S.; Di Napoli, M.; Lattanzi, S.; Hussain, M.S.; Biller, J.; McCullough, L.D.; Azarpazhooh, M.R.; Seletska, A.; Mayer, S.A.; et al. Coronavirus Disease 2019 and Stroke: Clinical Manifestations and Pathophysiological Insights. J. Stroke Cerebrovasc. Dis. 2020, 29, 104941. [Google Scholar] [CrossRef]
- Violi, F.; Pastori, D.; Cangemi, R.; Pignatelli, P.; Loffredo, L. Hypercoagulation and Antithrombotic Treatment in Coronavirus 2019: A New Challenge. Thromb. Haemost. 2020, 120, 949–956. [Google Scholar] [CrossRef] [PubMed]
- Palta, S.; Saroa, R.; Palta, A. Overview of the coagulation system. Indian J. Anaesth. 2014, 58, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Levy, J.H.; Raj, A.; Warkentin, T.E. Advance in the Management of Sepsis-Induced Coagulopathy and Disseminated Intravascular Coagulation. J. Clin. Med. 2019, 8, 728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Poll, T.; Van De Veerdonk, F.L.; Scicluna, B.; Netea, M.G. The immunopathology of sepsis and potential therapeutic targets. Nat. Rev. Immunol. 2017, 17, 407–420. [Google Scholar] [CrossRef]
- Von Brühl, M.-L.; Stark, K.; Steinhart, A.; Chandraratne, S.; Konrad, I.; Lorenz, M.; Khandoga, A.; Tirniceriu, A.; Coletti, R.; Köllnberger, M.; et al. Monocytes, neutrophils, and platelets cooperate to initiate and propagate venous thrombosis in mice in vivo. J. Exp. Med. 2012, 209, 819–835. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Tang, H. Aberrant coagulation causes a hyper-inflammatory response in severe influenza pneumonia. Cell. Mol. Immunol. 2016, 13, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Merad, M.; Martin, J.C. Pathological inflammation in patients with COVID-19: A key role for monocytes and macrophages. Nat. Rev. Immunol. 2020, 20, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Imai, Y.; Kuba, K.; Neely, G.; Yaghubian-Malhami, R.; Perkmann, T.; Van Loo, G.; Ermolaeva, M.; Veldhuizen, R.; Leung, Y.C.; Wang, H.; et al. Identification of Oxidative Stress and Toll-like Receptor 4 Signaling as a Key Pathway of Acute Lung Injury. Cell 2008, 133, 235–249. [Google Scholar] [CrossRef] [PubMed]
- Subramaniam, S.; Scharrer, I. Procoagulant activity during viral infections. Front. Biosci. (Landmark Ed.) 2018, 23, 1060–1081. [Google Scholar]
- Giannis, D.; Ziogas, I.A.; Gianni, P. Coagulation disorders in coronavirus infected patients: COVID-19, SARS-CoV-1, MERS-CoV and lessons from the past. J. Clin. Virol. 2020, 127, 104362. [Google Scholar] [CrossRef]
- Devreese, K.M.J.; Linskens, E.A.; Benoit, D.; Peperstraete, H. Antiphospholipid antibodies in patients with COVID-19: A relevant observation? J. Thromb. Haemost. 2020, 18, 2191–2201. [Google Scholar] [CrossRef]
- Hughes, C.; Nichols, T.; Pike, M.; Subbe, C.; Elghenzai, S. Cerebral Venous Sinus Thrombosis as a Presentation of COVID-19. Eur. J. Case Rep. Intern. Med. 2020, 7, 001691. [Google Scholar] [CrossRef]
- Klok, F.; Kruip, M.; van der Meer, N.; Arbous, M.; Gommers, D.; Kant, K.; Kaptein, F.; van Paassen, J.; Stals, M.; Huisman, M.; et al. Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-19: An updated analysis. Thromb. Res. 2020, 191, 148–150. [Google Scholar] [CrossRef]
- Ziegler, C.G.; Allon, S.J.; Nyquist, S.K.; Mbano, I.M.; Miao, V.N.; Tzouanas, C.N.; Cao, Y.; Yousif, A.; Bals, J.; Hauser, B.; et al. SARS-CoV-2 Receptor ACE2 Is an Interferon-Stimulated Gene in Human Airway Epithelial Cells and Is Detected in Specific Cell Subsets across Tissues. Cell 2020, 181, 1016–1035.e19. [Google Scholar] [CrossRef] [PubMed]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, T.; Navis, G.J.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Arroja, M.M.C.; Reid, E.; McCabe, C. Therapeutic potential of the renin angiotensin system in ischaemic stroke. Exp. Transl. Stroke Med. 2016, 8, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Penninger, J.M.; Li, Y.; Zhong, N.; Slutsky, A.S. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: Molecular mechanisms and potential therapeutic target. Intensive Care Med. 2020, 46, 586–590. [Google Scholar] [CrossRef] [Green Version]
- Kucharewicz, I.; Pawlak, R.; Matys, T.; Pawlak, D.; Buczko, W. Antithrombotic Effect of Captopril and Losartan Is Mediated by Angiotensin-(1-7). Hypertension 2002, 40, 774–779. [Google Scholar] [CrossRef] [Green Version]
- Fraga-Silva, R.A.; Sorg, B.S.; Wankhede, M.; DeDeugd, C.; Jun, J.Y.; Baker, M.B.; Li, Y.; Castellano, R.K.; Katovich, M.J.; Raizada, M.K.; et al. ACE2 Activation Promotes Antithrombotic Activity. Mol. Med. 2010, 16, 210–215. [Google Scholar] [CrossRef]
- Wu, Y.; Xu, X.; Chen, Z.; Duan, J.; Hashimoto, K.; Yang, L.; Liu, C.; Yang, C. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav. Immun. 2020, 87, 18–22. [Google Scholar] [CrossRef]
- Asadi-Pooya, A.A. Seizures associated with coronavirus infections. Seizure 2020, 79, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Benussi, A.; Pilotto, A.; Premi, E.; Libri, I.; Giunta, M.; Agosti, C.; Alberici, A.; Baldelli, E.; Benini, M.; Bonacina, S.; et al. Clinical characteristics and outcomes of inpatients with neurologic disease and COVID-19 in Brescia, Lombardy, Italy. Neurology 2020, 95, e910–e920. [Google Scholar] [CrossRef] [PubMed]
- Morassi, M.; Bagatto, D.; Cobelli, M.; D’Agostini, S.; Gigli, G.L.; Bnà, C.; Vogrig, A. Stroke in patients with SARS-CoV-2 infection: Case series. J. Neurol. 2020, 267, 2185–2192. [Google Scholar] [CrossRef] [PubMed]
- Vogrig, A.; Gigli, G.L.; Bnà, C.; Morassi, M. Stroke in patients with COVID-19: Clinical and neuroimaging characteristics. Neurosci. Lett. 2021, 743, 135564. [Google Scholar] [CrossRef] [PubMed]
- Morassi, M.; Bigni, B.; Cobelli, M.; Giudice, L.; Bnà, C.; Vogrig, A. Bilateral carotid artery dissection in a SARS-CoV-2 infected patient: Causality or coincidence? J. Neurol. 2020, 267, 2812–2814. [Google Scholar] [CrossRef]
- Anzalone, N.; Castellano, A.; Scotti, R.; Scandroglio, A.M.; Filippi, M.; Ciceri, F.; Tresoldi, M.; Falini, A. Multifocal laminar cortical brain lesions: A consistent MRI finding in neuro-COVID-19 patients. J. Neurol. 2020, 267, 2806–2809. [Google Scholar] [CrossRef] [PubMed]
- Gulko, E.; Overby, P.; Ali, S.; Mehta, H.; Al-Mufti, F.; Gomes, W. Vessel Wall Enhancement and Focal Cerebral Arteriopathy in a Pediatric Patient with Acute Infarct and COVID-19 Infection. Am. J. Neuroradiol. 2020, 41, 2348–2350. [Google Scholar] [CrossRef]
- Mirzaee, S.M.M.; Gonçalves, F.G.; Mohammadifard, M.; Tavakoli, S.M.; Vossough, A. Focal Cerebral Arteriopathy in a Pediatric Patient with COVID-19. Radiology 2020, 297, E274–E275. [Google Scholar] [CrossRef]
- Baig, A.M. Neurological manifestations in COVID-19 caused by SARS-CoV-2. CNS Neurosci. Ther. 2020, 26, 499–501. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with COVID-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef] [PubMed]
- Lodigiani, C.; Iapichino, G.; Carenzo, L.; Cecconi, M.; Ferrazzi, P.; Sebastian, T.; Kucher, N.; Studt, J.-D.; Sacco, C.; Bertuzzi, A.; et al. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb. Res. 2020, 191, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantador, E.; Núñez, A.; Sobrino, P.; Espejo, V.; Fabia, L.; Vela, L.; De Benito, L.; Botas, J. Incidence and consequences of systemic arterial thrombotic events in COVID-19 patients. J. Thromb. Thrombolysis 2020, 50, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients with Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AHA/ASA Stroke Council Leadership. Temporary Emergency Guidance to US Stroke Centers during the Coronavirus Disease 2019 (COVID-19) Pandemic. Stroke 2020, 51, 1910–1912. [Google Scholar] [CrossRef] [Green Version]
- Dafer, R.M.; Osteraas, N.D.; Biller, J. Acute Stroke Care in the Coronavirus Disease 2019 Pandemic. J. Stroke Cerebrovasc. Dis. 2020, 29, 104881. [Google Scholar] [CrossRef] [PubMed]
- Baracchini, C.; Pieroni, A.; Viaro, F.; Cianci, V.; Cattelan, A.; Tiberio, I.; Munari, M.; Causin, F. Acute stroke management pathway during Coronavirus-19 pandemic. Neurol. Sci. 2020, 41, 1003–1005. [Google Scholar] [CrossRef] [Green Version]
- Aggour, M.; White, P.; Kulcsar, Z.; Fiehler, J.; Brouwer, P. European Society of Minimally Invasive Neurological Therapy (ESMINT) recommendations for optimal interventional neurovascular management in the COVID-19 era. J. NeuroInterv. Surg. 2020, 12, 542–544. [Google Scholar] [CrossRef]
- Fiorella, D.; Fargen, K.M.; Leslie-Mazwi, T.M.; Levitt, M.; Probst, S.; Bergese, S.; Hirsch, J.A.; Albuquerque, F.C. Neurointervention for emergent large vessel occlusion during the COVID-19 pandemic. J. NeuroInterv. Surg. 2020, 12, 537–539. [Google Scholar] [CrossRef] [Green Version]
- Yaghi, S.; Ishida, K.; Torres, J.; Mac Grory, B.; Raz, E.; Humbert, K.; Henninger, N.; Trivedi, T.; Lillemoe, K.; Alam, S.; et al. SARS-CoV-2 and Stroke in a New York Healthcare System. Stroke 2020, 51, 2002–2011. [Google Scholar] [CrossRef]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M.; et al. Neurologic Features in Severe SARS-CoV-2 Infection. N. Engl. J. Med. 2020, 382, 2268–2270. [Google Scholar] [CrossRef]
- Reddy, S.T.; Garg, T.; Shah, C.; Nascimento, F.A.; Imran, R.; Kan, P.; Bowry, R.; Gonzales, N.; Barreto, A.; Kumar, A.; et al. Cerebrovascular Disease in Patients with COVID-19: A Review of the Literature and Case Series. Case Rep. Neurol. 2020, 12, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Shahjouei, S.; Tsivgoulis, G.; Farahmand, G.; Koza, E.; Mowla, A.; Sadr, A.V.; Kia, A.; Far, A.V.; Mondello, S.; Cernigliaro, A.; et al. SARS-CoV-2 and Stroke Characteristics. Stroke 2021, 52, e117–e130. [Google Scholar] [CrossRef] [PubMed]
- Oxley, T.J.; Mocco, J.; Majidi, S.; Kellner, C.P.; Shoirah, H.; Singh, I.P.; De Leacy, R.A.; Shigematsu, T.; Ladner, T.R.; Yaeger, K.A.; et al. Large-Vessel Stroke as a Presenting Feature of COVID-19 in the Young. N. Engl. J. Med. 2020, 382, e60. [Google Scholar] [CrossRef] [PubMed]
- Zhai, P.; Ding, Y.; Li, Y. The impact of COVID-19 on ischemic stroke. Diagn. Pathol. 2020, 15, 1–5. [Google Scholar] [CrossRef]
- Avula, A.; Nalleballe, K.; Narula, N.; Sapozhnikov, S.; Dandu, V.; Toom, S.; Glaser, A.; Elsayegh, D. COVID-19 presenting as stroke. Brain Behav. Immun. 2020, 87, 115–119. [Google Scholar] [CrossRef]
- Valderrama, E.V.; Humbert, K.; Lord, A.; Frontera, J.; Yaghi, S. Severe Acute Respiratory Syndrome Coronavirus 2 Infection and Ischemic Stroke. Stroke 2020, 51, e124–e127. [Google Scholar] [CrossRef] [PubMed]
- Lushina, N.; Kuo, J.S.; Shaikh, H.A. Pulmonary, Cerebral, and Renal Thromboembolic Disease in a Patient with COVID-19. Radiology 2020, 296, E181–E183. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.L.; Khawaja, A.M.; Majjhoo, A.Q. Stroke as a delayed manifestation of multi-organ thromboembolic disease in COVID-19 infection. J. Neurol. Sci. 2020, 417, 117071. [Google Scholar] [CrossRef]
- Moshayedi, P.; Ryan, T.E.; Mejia, L.L.P.; Nour, M.; Liebeskind, D.S. Triage of Acute Ischemic Stroke in Confirmed COVID-19: Large Vessel Occlusion Associated with Coronavirus Infection. Front. Neurol. 2020, 11, 353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viguier, A.; Delamarre, L.; Duplantier, J.; Olivot, J.-M.; Bonneville, F. Acute ischemic stroke complicating common carotid artery thrombosis during a severe COVID-19 infection. J. Neuroradiol. 2020, 47, 393–394. [Google Scholar] [CrossRef]
- Duroi, I.; Van Durme, F.; Bruyns, T.; Louage, S.; Heyse, A. Fatal Ischaemic Stroke during COVID-19 and Acute Lung Injury. Eur. J. Case Rep. Intern. Med. 2020, 7, 001732. [Google Scholar] [CrossRef]
- González-Pinto, T.; Luna-Rodríguez, A.; Moreno-Estébanez, A.; Agirre-Beitia, G.; Rodríguez-Antigüedad, A.; Ruiz-Lopez, M. Emergency room neurology in times of COVID-19: Malignant ischaemic stroke and SARS-CoV-2 infection. Eur. J. Neurol. 2020, 27. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, S.; Petridis, A.; Cornelius, J.F.; Hänggi, D. Letter to editor: Severe brain haemorrhage and concomitant COVID-19 Infection: A neurovascular complication of COVID-19. Brain Behav. Immun. 2020, 87, 150–151. [Google Scholar] [CrossRef] [PubMed]
- Sharifi-Razavi, A.; Karimi, N.; Rouhani, N. COVID-19 and intracerebral haemorrhage: Causative or coincidental? New Microbes New Infect. 2020, 35, 100669. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, D.; Raz, E.; Shapiro, M.; Dehkharghani, S.; Yaghi, S.; Lillemoe, K.; Nossek, E.; Torres, J.; Jain, R.; Riina, H.; et al. Cerebral Venous Thrombosis Associated with COVID-19. Am. J. Neuroradiol. 2020, 41, 1370–1376. [Google Scholar] [CrossRef]
- Garaci, F.; Di Giuliano, F.; Picchi, E.; Da Ros, V.; Floris, R. Venous cerebral thrombosis in COVID-19 patient. J. Neurol. Sci. 2020, 414, 116871. [Google Scholar] [CrossRef]
- Bastidas, H.I.; Márquez-Pérez, T.; García-Salido, A.; Luglietto, D.; Moreno, R.G.; de Azagra-Garde, A.M.; Nieto-Moro, M.; Leoz-Gordillo, I.; Budke, M.; Rivero-Martín, B. Cerebral Venous Sinus Thrombosis in a Pediatric Patient With COVID-19. Neurol. Clin. Pract. 2020, 11, e208–e210. [Google Scholar] [CrossRef]
- Shahjouei, S.; Naderi, S.; Li, J.; Khan, A.; Chaudhary, D.; Farahmand, G.; Male, S.; Griessenauer, C.; Sabra, M.; Mondello, S.; et al. Risk of stroke in hospitalized SARS-CoV-2 infected patients: A multinational study. EBioMedicine 2020, 59, 102939. [Google Scholar] [CrossRef]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Fagot Gandet, F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Thachil, J.; Tang, N.; Gando, S.; Falanga, A.; Cattaneo, M.; Levi, M.; Clark, C.; Iba, T. ISTH interim guidance on recognition and management of coagulopathy in COVID-19. J. Thromb. Haemost. 2020, 18, 1023–1026. [Google Scholar] [CrossRef]
- Cuker, A.; Tseng, E.K.; Nieuwlaat, R.; Angchaisuksiri, P.; Blair, C.; Dane, K.; Davila, J.; DeSancho, M.T.; Diuguid, D.; Griffin, D.O.; et al. American Society of Hematology 2021 guidelines on the use of anticoagulation for thromboprophylaxis in patients with COVID-19. Blood Adv. 2021, 5, 872–888. [Google Scholar] [CrossRef]
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Li, D.; Sun, Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J. Thromb. Haemost. 2020, 18, 1094–1099. [Google Scholar] [CrossRef] [PubMed]
- Siniscalchi, A.; Gallelli, L. Could COVID-19 represent a negative prognostic factor in patients with stroke? Infect. Control Hosp. Epidemiol. 2020, 41, 1115–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.-Y.; Li, X.-L.; Yan, Z.-R.; Sun, X.-P.; Han, J.; Zhang, B.-W. Potential neurological symptoms of COVID-19. Ther. Adv. Neurol. Disord. 2020, 13, 1756286420917830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahiri, D.; Ardila, A. COVID-19 Pandemic: A Neurological Perspective. Cureus 2020, 12, e7889. [Google Scholar] [CrossRef]
- Mowla, A.; Shakibajahromi, B.; Shahjouei, S.; Borhani-Haghighi, A.; Rahimian, N.; Baharvahdat, H.; Naderi, S.; Khorvash, F.; Altafi, D.; Ebrahimzadeh, S.A.; et al. Cerebral venous sinus thrombosis associated with SARS-CoV-2; a multinational case series. J. Neurol. Sci. 2020, 419, 117183. [Google Scholar] [CrossRef] [PubMed]
- Al-Mufti, F.; Amuluru, K.; Sahni, R.; Bekelis, K.; Karimi, R.; Ogulnick, J.; Cooper, J.; Overby, P.; Nuoman, R.; Tiwari, A.; et al. Cerebral Venous Thrombosis in COVID-19: A New York Metropolitan Cohort Study. Am. J. Neuroradiol. 2021, 42, 1196–1200. [Google Scholar] [CrossRef]
- Siddiqui, F.M.; Dandapat, S.; Banerjee, C.; Zuurbier, S.M.; Johnson, M.; Stam, J.; Coutinho, J.M. Mechanical Thrombectomy in Cerebral Venous Thrombosis. Stroke 2015, 46, 1263–1268. [Google Scholar] [CrossRef]
- Léonard-Lorant, I.; Delabranche, X.; Séverac, F.; Helms, J.; Pauzet, C.; Collange, O.; Schneider, F.; Labani, A.; Bilbault, P.; Molière, S.; et al. Acute Pulmonary Embolism in Patients with COVID-19 at CT Angiography and Relationship to d-Dimer Levels. Radiology 2020, 296, E189–E191. [Google Scholar] [CrossRef] [Green Version]
- Mohamed-Hussein, A.A.; Aly, K.M.; Ibrahim, M.-E.A. Should aspirin be used for prophylaxis of COVID-19-induced coagulopathy? Med. Hypotheses 2020, 144, 109975. [Google Scholar] [CrossRef] [PubMed]
- Hess, D.C.; Eldahshan, W.; Rutkowski, E. COVID-19-Related Stroke. Transl. Stroke Res. 2020, 11, 322–325. [Google Scholar] [CrossRef]
- Escalard, S.; Maïer, B.; Redjem, H.; Delvoye, F.; Hébert, S.; Smajda, S.; Ciccio, G.; Desilles, J.-P.; Mazighi, M.; Blanc, R.; et al. Treatment of Acute Ischemic Stroke due to Large Vessel Occlusion with COVID-19. Stroke 2020, 51, 2540–2543. [Google Scholar] [CrossRef] [PubMed]
- Deana, C. The COVID-19 pandemic: Is our medicine still evidence-based? Ir. J. Med. Sci. 2020, 190, 11–12. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Region | Age, Gender | Neurological Symptoms on Admission (Day from Admission) | Other Symptoms (Onset Day Prior Neurologic Symptoms or after Admission) | Admission Serum Labs (or Day from Admission) | Imaging or EEG (Day from Admission) | Treatments Received | Outcome | Ref |
|---|---|---|---|---|---|---|---|---|
| Ischemic Stroke | ||||||||
| Wuhan, China | 79, M | One-day right limb weakness, mild expressive aphasia (on exam) | Cough (7 days prior) | Lymphocytopenia, ↑ CRP (36.1 mg/L), ESR (43 mm/h), & lipoprotein(a) (1276 mg/L); normal cardiac, renal, &coagulation functions | Head CT scan: lacunar cerebral infarction. 48-h Holter monitoring: paroxysmal AF. | Oseltamivir, ribavirin, moxifloxacin, dexamethasone, clopidogrel, atorvastatin | Favorable; recovery within 12 days | [65] |
| London, UK | 64, M | Mild left arm weakness, word-finding difficulty & incoordination (day 5); evolving to bilateral incoordination & right homonymous hemianopia (day 12) | Cough, dyspnea, fever, myalgia & poor appetite (10 days prior); evolving to respiratory failure (admission day) & PE (day 9) | ↓ Hgb (119 g/L); ↑ LDH (654 U/L), ALT (137 U/L), PT (12.5 s), fibrinogen (950 mg/dL), D-dimer (>80,000 µg/L), ferritin (4927 µg/L) & CRP (305.4 mg/L); lupus anticoagulant (+); normal CBCdiff, aPTT & INR. | Brain MRI (day 5): acute left vertebral artery thrombus and acute left PICA territory infarction with petechial hemorrhagic transformation. DWI MRI (day 12): bilateral acute PCA territory infarcts despite therapeutic anticoagulation. Lower limb Doppler ultrasound: occlusive DVT in left posterior tibial & peroneal veins. CT pulmonary angiogram (day 9): bilateral PE. | Initially aspirin & clopidogrel; then high-intensity LMWH anticoagulation (for PE) | Poor; ICU admission | [13] |
| London, UK | 53, F | Acute confusion, incoordination, impaired consciousness (GCS 13/15) | Malaise, cough, fever & dyspnea (24 days prior) | ↓ Hgb (94 g/L); leukocytosis (WBC 23K), ↑ LDH (664 U/L), PT (34.4 s), INR (3.6), aPTT (41 s), D-dimer (7750 µg/L), ferritin (1853 µg/L) & CRP (150.1 mg/L); lupus anticoagulant (+); Normal fibrinogen & LFT. | Head CT Scan: acute right parietal cortical & left cerebellar infarct with mass effect & hydrocephalus, despite therapeutic anticoagulation. | EVD for hydrocephalus & therapeutic LMWH anticoagulation | Death due to COVID-19 related cardiorespiratory failure | [13] |
| London, UK | 85, M | Dysarthria, right facial droop, right-sided hemiparesis | Cough (10 days prior) | ↓ Hgb (128 g/L); ↑ LDH (461 U/L), D-dimer (16,100 µg/L), fibrinogen (530 mg/dL), ferritin (1027 µg/L) & CRP (161.2 mg/L); lupus anticoagulant (−); normal CBCdiff, PT, aPTT, INR & LFT. | Head CT Scan: hyperdensity consistent with thrombus in the left PCA & acute infarction in left temporal stem and cerebral peduncle. | Apixaban for AF | NR | [13] |
| London, UK | 61, M | Acute dysarthria & left facial droop & hemiparesis (2 days prior COVID-19 symptoms started) | Fever, cough, dyspnea & tachypnea (2 days after admission) | ↓ Hgb (126 g/L) & aPTT (24 s); thrombocytosis (408 K), ↑ LDH (444 U/L), fibrinogen (463 mg/dL), D-dimer (27,190 µg/L) & ferritin (1167 µg/L); lupus anticoagulant (+); normal CRP, PT, INR & LFT. | DWI brain MRI: acute infarction in the right corpus striatum suggesting transient occlusion of the M1 segment of the right MCA; FLAIR MRI: an established infarct in the same region with moderate background cerebral small vessel disease. CT pulmonary angiogram: pulmonary embolus in the left upper lobe segmental artery. | Therapeutic LMWH anticoagulation | NR | [13] |
| London, UK | 83, M | Acute dysarthria, left facial droop & hemiparesis, & left-sided sensory inattention | Fever, cough, dyspnea & fatigue (15 days prior) | ↓ Hgb (121 g/L); leukocytosis (WBC 11K), ↑ LDH (353 U/L), fibrinogen (496 mg/dL), D-dimer (19,450 µg/L) & CRP (27.7 mg/L); lupus anticoagulant (+); normal PT, aPTT, INR & LFT. | Head CT/CT angiogram: thrombotic occlusion of a proximal M2 branch of the right MCA; Repeat CT (24 h): a focus of parenchymal low density involving the right insular cortex in keeping with an evolving right MCA territory infarct | Intravenous thrombolysis | NR | [13] |
| London, UK | 73, M | Acute aphasia & right facial droop & hemiparesis | Dyspnea & tachypnea (8 days prior) | Thrombocytosis (403 K), ↑ LDH (439 U/L), PT (12.3 s), D-dimer (1080 µg/L), ferritin (655 µg/L) & CRP (179.9 mg/L); lupus anticoagulant (+); normal PT, aPTT, INR & LFT. | DWI brain MRI: acute infarction in the right thalamus, left pons, right occipital lobe and right cerebellar hemisphere. Time-of-flight images: thrombotic material in the basilar artery and bilateral mild-to-moderate P2 segment stenosis. | Intravenous thrombolysis, decreasing D-dimer (1080 μg/L). | NR | [13] |
| New York, USA | 33, F | 28-h left hemiplegia, facial droop, gaze preference, homonymous hemianopia, dysarthria, sensory deficit, admission NIHSS 19 | Cough, headache & chills (7 days prior) | ↑ fibrinogen (501 mg/dL); normal WBC, platelets, PT, aPTT, D-dimer & ferritin. | Head CT/CT angiogram/MRI: partial infarction of the right MCA with a partially occlusive thrombus in the right carotid artery at the cervical bifurcation. | Apixaban (5 mg twice daily) | Favorable; complete resolution of thrombus in repeat CT angiogram (day 10), follow up NIHSS 13 (day 14) | [64] |
| New York, USA | 37, M | 16-h impaired consciousness, dysphasia, right hemiplegia, dysarthria, sensory deficit, admission NIHSS 13 | No symptoms; exposed to family member with PCR-positive COVID-19 | ⭡ aPTT (42.7 s); normal WBC, platelets, PT, INR, fibrinogen, D-dimer & ferritin. | Head CT/CT angiogram/MRI: left MCA territory ischemic infarction | Clot retrieval, apixaban (5 mg twice daily) | Favorable; follow up NIHSS 5 (day 10) | [64] |
| New York, USA | 39, M | 8-h impaired consciousness, gaze preference to the right, left homonymous hemianopia, left hemiplegia, ataxia, admission NIHSS 16 | No symptoms | ↑ fibrinogen (739 mg/dL), D-dimer (2230 µg/L) & ferritin (1564 µg/L); normal CBCdiff, PT & aPTT. | Head CT/CT angiogram/MRI: right PCA territory ischemic infarction | Clot retrieval, aspirin (81 mg/day) | Poor; multiple organ failure & intubated/sedated in ICU | [64] |
| New York, USA | 44, M | 2-h impaired consciousness, global dysphasia, right hemiplegia, gaze preference, admission NIHSS 23 | Lethargy | ↑ D-dimer (13,800 µg/L) & ferritin (987 µg/L); normal CBCdiff, LFT, RFT, PT, aPTT & fibrinogen. | Head CT/CT angiogram/MRI: left MCA territory ischemic infarction | IV t-PA, clot retrieval, hemicraniectomy, & aspirin (81 mg/day) | NR; stay in stroke unit, follow up NIHSS 19 (day 12) | [64] |
| New York, USA | 49, M | 8-h impaired consciousness, left hemiplegia, dysarthria, facial weakness, admission NIHSS 13 | Fever, cough & lethargy | ↑ PT (15.2 s), aPTT (37 s), fibrinogen (531 mg/dL), D-dimer (1750 µg/L) & ferritin (596 µg/L); normal CBCdiff, LFT & RFT. | Head CT/CT angiogram/MRI: right MCA territory ischemic infarction | Clot retrieval & stent, aspirin (325 mg/day), & clopidogrel (75 mg/day) | Favorable; follow up NIHSS 7 (day 4) | [64] |
| New York, USA | 73, M | Acute altered mental status with hypoxemic respiratory failure (intubation) | Fever & dyspepsia (admission); nausea, vomiting & poor appetite (2 days prior) | ⭡ CRP (26 mg/dL), prolonged PT (13.5 s), normal aPTT, LFT, & RFT; D-dimer, CRP & ferritin not checked. | Head CT scan: loss of gray-white differentiation at the left occipital & parietal lobes, consistent with acute infarction. Repeat CT head: progression toward a large acute infarct of the left MCA territory with hyperdense appearance of left MCA vessels - consistent with an acute thrombus. | Aspirin & supportive care | Poor; comfort measures only & terminally extubation | [66] |
| New York, USA | 83, F | Admission: acute left facial droop, slurred speech, admission NIHSS 2. Day 3: left hemineglect, worsening left facial droop, & left hemiparesis, NIHSS 16 | Fever & poor oral intake (admission) | Leukopenia & lymphocytopenia; D-dimer not checked. | Head CT/ CT angiogram (admission): No acute change, focal moderate stenosis of right MCA. Head CT (day 3): new moderate hypodensity in the right frontal lobe representing acute infarction. | Integrellin not started due to respiratory failure | Poor; respiratory failure & withdrawal of care | [66] |
| New York, USA | 80, F | Acute altered mental status, aphasia & left side weakness, admission NIHSS 36 | No symptoms; frequent falls (for 7 days) | Leukocytosis, lymphocytopenia, ⭡ D-dimer (13,966 µg/L), LDH (712 U/L) & CRP (16.24 mg/dL); prolonged PT (15.2 s); normal procalcitonin, aPTT, LFT & RFT. | Head CT scan: an acute right MCA stroke. Head/neck CTA: occlusion of the right internal carotid artery at origin. CT perfusion: a 305-cc core infarct in the right MCA distribution and a surrounding 109 cc ischemic penumbra. | Supportive care | Poor, comfort measures only and terminally extubation | [66] |
| New York, USA | 88, F | Transient 15-min right arm weakness & numbness, & word-finding difficulty | Mild dyspnea & cough (admission) | ⭡ D-dimer (3442 µg/L), CRP (12.7 mg/L) & IL-6 (8.5 pg/mL); prolonged PT (13.5 s); normal ferritin, procalcitonin, aPTT, Hgb, CBCdiff, LDH, LFT & RFT. | Head CT scan: normal. Brain MRI: acute infarct in the left medial temporal lobe. Head/neck MR angiogram: mild stenosis of the right M1 segment | Aspirin & statins | Favorable | [66] |
| New York, USA | 52, M | Acute global aphasia, right hemiparesis & left gaze preference, admission NIHSS 20 | Fever, cough & dyspnea (7 days prior) | ⭡ D-dimer (>10,000 µg/L), fibrinogen (235 mg/dL), ferritin (588 µg/L), CRP (11 mg/L) & ESR (37 mm/h). | Head CT scan: hyperdensity of the M1 segment of the left MCA. Head/neck CT angiogram: a left intracranial internal carotid artery occlusion. Repeat CT head: early infarct signs of in the left basal ganglia, internal capsule, caudate head, insular ribbon, operculum, & right posterior frontal lobe. CT perfusion: a favorable mismatch ratio of 4.1 | IV alteplase, clot retrieval, aspirin, statin, & hydroxychloroquine | Partial recovery upon discharge | [67] |
| New Jersey, USA | 84, M | Respiratory distress & unequal pupils | Fever, dyspnea, cough, & abdominal pain (14 days prior) | Lymphocytopenia, ↑ D-dimer (21,600 µg/L) & procalcitonin (0.25 ng/mL). | Head/neck CT/CTA: distal basilar artery occlusion extending into the proximal PCA, small aortic arch thrombus. Chest CT: bilateral lobar pulmonary emboli | LMWH (for PE); Clot retrieval | Death (Day 1) | [68] |
| Detroit, USA | 72, F | Impaired consciousness, GCS 3 (day 10) | Progressive cough, myalgia, & dyspnea (21 days prior) | Admission: leukocytosis, acute kidney injury, transaminitis, & rhabdomyolysis; ↑ CRP & ferritin. Day 7: ↑ aPTT (28.5 s), PT (13.5 s), INR (1.32), mild thrombocytopenia (146K), | Head CT scan (day 10): bilateral cerebral infarcts in multiple vascular territories including cortical & subcortical regions. | Palliative care | Death | [69] |
| Philadelphia, USA | 62, F | First admission: acute aphasia & right hemiparesis.2nd admission (10 days after): altered mental status | No symptoms | Negative COVID-19 rRT-PCR in CSF (two times in 2nd admission). | Head CT angiogram (first admission): left MCA occlusion. Head CT scan (2nd admission): hemorrhagic conversion with midline shift & obstructive hydrocephalus | Clot retrieval (first admission), decompressive hemicraniectomy & EVD (2nd admission) | Poor; stay in ICU | [14] |
| Los Angeles, USA | 70s, | Acute aphasia, right hemiparesis & facial droop (day 5) | acute chest pain, diaphoresis, & hypotension with ST-elevation myocardial infarction (admission) | ↑ aPTT (>85.5) while on heparin, renal failure, normal platelet count | Brain MRI: 60-cc acute infarct in the left insular, temporal, parietal, and frontal lobes, as well as smaller acute infarcts in the right caudate & left cerebellar hemisphere. MR angiogram: left MCA proximal M1 segment occlusion. | Palliative care | Poor | [70] |
| Toulouse, France | 73, M | 9-h acute aphasia & right hemiparesis, admission NIHSS 10 | Fever & cough (7 days prior) | Lymphocytopenia, ⭡ CRP (219 mg/L), ferritin (109.6 µ/dL), fibrinogen (820 mg/dL) & D-dimer (2220 µg/L); normal platelets; negative antiphospholipid antibodies. | Head CT/CT angiogram/perfusion/MRI: subtle cortical left frontal hypoattenuation with more extended surrounding hypoperfusion & distal occlusion of left MCA branch; a large intraluminal floating thrombus appended to a hypoattenuated non-stenosing plaque of the left common carotid artery wall. | LMWH anticoagulation (enoxaparin) | Favorable; resolution of thrombus on carotid ultrasound (15 days after onset); follow up NIHSS 3 (day 10, discharge day) | [71] |
| Ronse, Belgium | 74, F | Continued unconsciousness after extubation on day 16 & a mild endorotation of the arms | Fever, dyspnea & cough (7 days prior); evolving to hypoxic respiratory failure & intubation (admission day 3) | Slight lymphocytopenia, ⭡ CRP (18.79 mg/L), procalcitonin (1.93 ng/mL), ferritin (846.1 μg/L) & mild ⭡ creatinine (1.02 mg/dL); Day 2: ⭡ D-dimer (2504 µg/L). Day 16: ⭡ D-dimer (3941 µg/L) & fibrinogen (606 mg/dL); normal PT & platelets. | Head CT scan: large left MCA ischemic infarction with additional edema and midline shift; hyperdense artery sign was seen due to a thrombotic occlusion at the transition of the left internal carotid artery to the origin of the MCA. | Palliative care | Death (day 16) | [72] |
| Bilbao, Spain | 36, F | 48-h aphasia & acute right hemiplegia, admission NIHSS 21 | No symptoms | Leukocytosis (23.6K), ⭡ CK (8669 U/L) & D-dimer (7540 µg/L) & CRP (15.6 mg/L). | Head CT scan: established infarct in the left MCA territory with a mild deviation of the midline. Head/neck CT angiogram: occlusion of the left internal carotid artery, MCA & ACA with a free-floating thrombus in the ascending aorta with no signs of aortic atheromatosis. CT pulmonary angiogram: bilateral PE. | Palliative care | Death within 72 h | [73] |
| Intracranial hemorrhage | ||||||||
| Philadelphia, USA | 31, M | Acute headache & loss of consciousness | Malaise, fever, cough & arthralgia (7 days prior) | Negative COVID-19 rRT-PCR in CSF. | Head CT scan: SAH centered in the posterior fossa, including the 4th ventricle with hydrocephalus. Head CT angiogram: right-sided ruptured dissecting PICA aneurysm. | EVD for hydrocephalus & flow-diverting stent for aneurysm | Favorable; gradual improvement in mental status | [14] |
| Düsseldorf, Germany | 60, F | Loss of consciousness | Concurrent respiratory insufficiency requiring intubation | Leukocytosis (14.2K), ⭡ troponin (45 ng/mL), CK (4920 U/L), CRP (11 mg/L), LDH (360 U/L) & GGT (103 U/L); normal CSF study. | Head CT/CT angiogram: left frontal haemorrhage with ventricle bleeding from a ruptured pericallosal artery aneurysm (~5 mm). CT perfusion (day 3, 6, 9 & 12): no cerebral vasospasm. | Aneurysm clipping & pneumonia treatment | Favorable | [74] |
| Brescia, Italy | 57, M | Bilaterally fixed & dilated pupils, GCS 3 (day 11) | Fever & cough (7 days prior), worsening dyspnea (3 days prior) | Day 4: ↑ CRP, LDH, AST, & GGT.Day 11: prolonged aPTT (53.1 s), ↑ D-dimer (2866 µg/L). | Head CT scan (day 11): bilateral cerebellar hemispheric hemorrhage with 4th ventricle & brainstem compression and supratentorial hydrocephalus & diffuse obliteration of sulci. CT angiogram: Normal. | NR | Death (1 h after CT) | [43] |
| Brescia, Italy | 57, M | bilaterally fixed and dilated pupils, GCS 3 (day 12) | Fever & cough (10 days prior), dyspnea (3 days prior) | Admission: ↑ CRP (21 mg/L), LDH (771 U/L), AST (100 U/L), GGT (152 U/L). | Head CT scan: diffuse cerebral edema with a large right frontal hemorrhage extending to ventricles. | LMWH (for PE) prior neurological deterioration | Death (shortly after CT) | [43] |
| Sari, Iran | 79, M | Acute loss of consciousness | Fever & cough (3 days prior) | Lymphocytopenia, thrombocytosis (210 K); prolonged PT (12 s), INR (1), & aPTT (64 s); ↑ ESR (85 mm/h), CRP (10 mg/L), & creatinine (1.4 mg/dL); normal LFT | Head CT scan: massive right-hemispheric hemorrhage extending to ventricles & SAH | NR | NR | [75] |
| Cerebral venous thrombosis | ||||||||
| Wales, UK | 59, M | First admission: 4-day progressive headache Second admission (4 days later): acute right sided weakness & numbness, slurred speech, expressive aphasia, admission NIHSS 10 | First admission: fever & hypertension. | Prolonged aPTT (22.3 s), ⭡ CRP (15 mg/L) & creatinine (57 mg/dL); normal CBCdiff, PT & fibrinogen. | Head CT scan (1st admission): hyperdensity within the superior sagittal sinus, right transverse sinus, sigmoid sinus & upper right internal jugular vein suggestive of venous thrombosis. Head CT venogram (1st admission): normal; however, it was re-reviewed 4 days later (2nd admission): filling defect in the right sigmoid & transverse sinus involving the torcula. | LMWH | Favorable; NIHSS 4 within 24 h | [32] |
| New York, USA | 38, M | Seven-day headache & 2-day impaired consciousness; evolving to extensor posturing of the arms & clonus with NIHSS 14 | Persistent diarrhea & vomiting (10 days prior) | NR | Head CT scan: Hyperdensity in the straight sinus, distal superior sagittal sinus, torcular & right transverse sinus, & in several cortical veins adjacent to the superior sagittal sinus, suggestive of cerebral venous thrombosis.Head CT venogram: near-occlusive thrombus in the right internal cerebral vein. | Enoxaparin (70 mg subcutaneously twice a day) & clot retrieval, lopinavir, ritonavir | Death within 32 h | [76] |
| New York, USA | 41, F | Acute confusion, global aphasia & left gaze preference, admission NIHSS 16; rapidly worsening mental status & extensor posturing to noxious stimulation requiring intubation | Prior admission for COVID-19 | ⭡ D-dimer (2032 µg/L). CSF: ⭡ protein (616 mg/dL) & 41 WBC (PMN 84%), normal glucose. | Head CT/CT angiogram (admission): normal. Repeat CT head: a venous infarction in the left basal ganglia, thalamus, & mesial temporal lobe with hemorrhagic transformation, intraventricular hemorrhage, & obstructive hydrocephalus. Head CT venogram: occlusion of the internal cerebral veins. | EVD & heparin infusion | Death within 4 days | [76] |
| New York, USA | 32, M | One-week headache & impaired consciousness | Concurrent 7-day fever & dry cough | ↑ Glucose (1384 mg/dL), D-dimer (>11000 µg/L) & ferritin (18,431 µg/L) | Head CT scan: patchy areas of low density in the bilateral cerebral hemispheres with foci of subcortical hemorrhage in the left parieto-occipital region. Head CT angiogram: normal. Brain MRI: confluent, nonenhancing regions of pathologically reduced diffusion throughout the subcortical & deep hemispheric white matter bilaterally, left greater than right. Punctate foci of susceptibility artifacts consistent with petechial hemorrhage on gradient recalled-echo images, suspecting diabetic ketoacidosis related venous thrombosis. | Azithromycin, hydroxychloroquine | Death within few days | [76] |
| Rome, Italy | 44, F | Ingravescent dyspnea, headache, impaired consciousness, aphasia & right hemiparesis | Fever, cough & dyspnea (14 days prior) | Neutrophilic leukocytosis, lymphocytopenia, thrombocytopenia (42 K); ↑ D-dimer (5975 µg/L), CK-MB (6.9 µg/L),; Negative anti-cardiolipin, -β2-glycoprotein & -dsDNA antibodies | Head CT angiogram: Dural sinus thrombosis with poor representation of left internal cerebral vein. Pulmonary CT angiogram: Filling defect within the inferior trunk of the right pulmonary artery and along the superior vena cava by thrombi. | NR | NR | [77] |
| Paris, France | 62, F | Headache & altered vision, evolving to sudden right hemicorporeal deficit & impaired consciousness | Fever, cough &dyspnea (15 days prior) | Leukocytosis (20 K); ↑ AST (54 U/L), ALT (68 U/L), GGT (87 U/L), & D-dimer (14,200 µg/L) | Head CT scan & brain MRI: large confluent intraparenchymal hemorrhage in the left fronto-temporal lobes. CT venogram: cerebral venous thrombosis of the left transverse sinus, straight vein, vein of Galen and internal cerebral veins. | NR | NR | [16] |
| Paris, France | 54, F | Severe headache | Fever & asthenia (14 days prior) | Leukocytosis (18K), ↑ CRP (170.8 mg/L) & D-dimer (2360 µg/L) | Head CT scan & brain MRI: large hemorrhagic infarction in the left temporal lobe. CT venogram and MR angiography: cerebral venous thrombosis of the left transverse sinus | NR | NR | [16] |
| Madrid, Spain | 13, F | Impaired consciousness & intense headache | Fever, cough, & odynophagia (7 days prior) followed by frontal headache & vomiting | Leukocytosis (14.4 K), lymphocytopenia, thrombocytopenia; ↑ D-dimer (33,960 µg/L), CRP (12.55 mg/dL), LDH (322 U/L), & ferritin (240 ng/mL); fibrinogen (0 mg/dL). | Head CT scan: right occipital intracerebral hemorrhage. MR angiogram: bilateral transverse sinus thrombosis extending to right sigmoid sinus & internal jugular vein.Body angio-CT scan (day 3): thrombosis progression towards the posterior half of superior sagittal sinus, bilateral PE & bilateral deep femoral and iliac veins thrombosis reaching infrarenal cava. | IV fluid, empiric antibiotics, hypertonic saline, Fibrinogen, platelet & plasma transfusion; later lopinavir, ritonavir, hydroxychloroquine, & azithromycin; LMWH | Favorable; recovery within 24 days | [78] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghasemi, M.; Umeton, R.P.; Keyhanian, K.; Mohit, B.; Rahimian, N.; Eshaghhosseiny, N.; Davoudi, V. SARS-CoV-2 and Acute Cerebrovascular Events: An Overview. J. Clin. Med. 2021, 10, 3349. https://doi.org/10.3390/jcm10153349
Ghasemi M, Umeton RP, Keyhanian K, Mohit B, Rahimian N, Eshaghhosseiny N, Davoudi V. SARS-CoV-2 and Acute Cerebrovascular Events: An Overview. Journal of Clinical Medicine. 2021; 10(15):3349. https://doi.org/10.3390/jcm10153349
Chicago/Turabian StyleGhasemi, Mehdi, Raffaella Pizzolato Umeton, Kiandokht Keyhanian, Babak Mohit, Nasrin Rahimian, Niloofarsadaat Eshaghhosseiny, and Vahid Davoudi. 2021. "SARS-CoV-2 and Acute Cerebrovascular Events: An Overview" Journal of Clinical Medicine 10, no. 15: 3349. https://doi.org/10.3390/jcm10153349
APA StyleGhasemi, M., Umeton, R. P., Keyhanian, K., Mohit, B., Rahimian, N., Eshaghhosseiny, N., & Davoudi, V. (2021). SARS-CoV-2 and Acute Cerebrovascular Events: An Overview. Journal of Clinical Medicine, 10(15), 3349. https://doi.org/10.3390/jcm10153349