
Risk Factors of Urothelial Cancer in Inflammatory Bowel Disease

 ,
, 
 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
- -
- all patients with a confirmed diagnosis of IBD according to the indications of the European Crohn’s and Colitis Organization (ECCO) [13];
- -
- minimum age of 16, with no upper age limits.
- -
- lack of data on the presence of tumor comorbidities.
- -
- categorical variables: sex, smoking habit, type of IBD, treatment with mesalazine, treatment with thiopurine, treatment with anti-tumor necrosis factor (TNF), treatment with anti-integrins, and surgical treatment for intestinal disease;
- -
- continuous variables: age at diagnosis of IBD, duration of treatment with mesalamine, duration of treatment with thiopurine, duration of treatment with anti-TNF, and duration of treatment with anti-integrins.
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Actis, G.C.; Pellicano, R.; Fagoonee, S.; Ribaldone, D.G. History of Inflammatory Bowel Diseases. J. Clin. Med. 2019, 8, 1970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkowitz, L.; Schultz, B.M.; Salazar, G.A.; Pardo-Roa, C.; Sebastián, V.P.; Álvarez-Lobos, M.M.; Bueno, S.M. Impact of cigarette smoking on the gastrointestinal tract inflammation: Opposing effects in Crohn’s disease and ulcerative colitis. Front. Immunol. 2018, 9, 74. [Google Scholar] [CrossRef] [Green Version]
- Karczewski, J.; Poniedziałek, B.; Rzymski, P.; Rychlewska-Hańczewska, A.; Adamski, Z.; Wiktorowicz, K. The effect of cigarette smoking on the clinical course of inflammatory bowel disease. Gastroenterol. Rev. 2014, 9, 153–159. [Google Scholar] [CrossRef]
- Pedersen, N.; Duricova, D.; Elkjaer, M.; Gamborg, M.; Munkholm, P.; Jess, T. Risk of Extra-Intestinal Cancer in Inflammatory Bowel Disease: Meta-Analysis of Population-Based Cohort Studies. Am. J. Gastroenterol. 2010, 105, 1480–1487. [Google Scholar] [CrossRef] [PubMed]
- Gakis, G. The role of inflammation in bladder cancer. Adv. Exp. Med. Biol. 2014, 816, 183–196. [Google Scholar]
- Bourrier, A.; Carrat, F.; Colombel, J.-F.; Bouvier, A.-M.; Abitbol, V.; Marteau, P.; Cosnes, J.; Simon, T.; Peyrin-Biroulet, L.; Beaugerie, L.; et al. Excess risk of urinary tract cancers in patients receiving thiopurines for inflammatory bowel disease: A prospective observational cohort study. Aliment. Pharmacol. Ther. 2016, 43, 252–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cumberbatch, M.G.K.; Jubber, I.; Black, P.C.; Esperto, F.; Figueroa, J.D.; Kamat, A.M.; Kiemeney, L.; Lotan, Y.; Pang, K.; Silverman, D.T.; et al. Epidemiology of Bladder Cancer: A Systematic Review and Contemporary Update of Risk Factors in 2018. Eur. Urol. 2018, 74, 784–795. [Google Scholar] [CrossRef] [Green Version]
- Boffetta, P. Tobacco smoking and risk of bladder cancer. Scand. J. Urol. Nephrol. 2008, 42, 45–54. [Google Scholar] [CrossRef]
- Persson, P.-G.; Karlén, P.; Bernell, O.; Leijonmarck, C.-E.; Broström, O.; Ahlbom, A.; Hellers, G. Crohn’s disease and cancer: A population-based cohort study. Gastroenterology 1994, 107, 1675–1679. [Google Scholar] [CrossRef]
- Jussila, A.; Virta, L.J.; Pukkala, E.; Färkkilä, M.A. Malignancies in patients with inflammatory bowel disease: A nationwide register study in Finland. Scand. J. Gastroenterol. 2013, 48, 1405–1413. [Google Scholar] [CrossRef]
- Beaugerie, L.; Itzkowitz, S.H. Cancers Complicating Inflammatory Bowel Disease. N. Engl. J. Med. 2015, 372, 1441–1452. [Google Scholar] [CrossRef]
- Biancone, L.; Armuzzi, A.; Scribano, M.L.; Castiglione, F.; D’Incà, R.; Orlando, A.; Papi, C.; Daperno, M.; Vecchi, M.; Riegler, G.; et al. Cancer Risk in Inflammatory Bowel Disease: A 6-Year Prospective Multicenter Nested Case-Control IG-IBD Study. Inflamm. Bowel Dis. 2020, 26, 450–459. [Google Scholar] [CrossRef]
- Maaser, C.; Sturm, A.; Vavricka, S.R.; Kucharzik, T.; Fiorino, G.; Annese, V.; Calabrese, E.; Baumgart, D.C.; Bettenworth, D.; Borralho Nunes, P.; et al. ECCO-ESGAR guideline for diagnostic assessment in IBD part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J. Crohn’s Colitis 2019, 13, 144–164. [Google Scholar] [CrossRef] [Green Version]
- Linee Guida Tumore Dell’urotelio. Available online: https://www.aiom.it/wp-content/uploads/2018/11/2018_LG_AIOM_Urotelio.pdf (accessed on 2 July 2021).
- Kappelman, M.D.; Farkas, D.K.; Long, M.D.; Erichsen, R.; Sandler, R.S.; Sørensen, H.T.; Baron, J.A. Risk of Cancer in Patients With Inflammatory Bowel Diseases: A Nationwide Population-based Cohort Study With 30 Years of Follow-up Evaluation. Clin. Gastroenterol. Hepatol. 2014, 12, 265–273.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madanchi, M.; Zeitz, J.; Barthel, C.; Samaras, P.; Scharl, S.; Sulz, M.C.; Biedermann, L.; Frei, P.; Vavricka, S.R.; Rogler, G.; et al. Malignancies in Patients with Inflammatory Bowel Disease: A Single-Centre Experience. Digestion 2016, 94, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Heuvel, T.R.A.; Wintjens, D.S.J.; Jeuring, S.F.G.; Wassink, M.H.H.; Romberg-Camps, M.J.L.; Oostenbrug, L.E.; Sanduleanu, S.; Hameeteman, W.H.; Zeegers, M.P.; Masclee, A.A.; et al. Inflammatory bowel disease, cancer and medication: Cancer risk in the Dutch population-based IBDSL cohort. Int. J. Cancer 2016, 139, 1270–1280. [Google Scholar] [CrossRef] [PubMed]
- Jess, T.; Horváth-Puhó, E.; Fallingborg, J.; Rasmussen, H.H.; Jacobsen, B.A. Cancer Risk in Inflammatory Bowel Disease According to Patient Phenotype and Treatment: A Danish Population-Based Cohort Study. Am. J. Gastroenterol. 2013, 108, 1869–1876. [Google Scholar] [CrossRef]
- Dulai, P.S.; Sandborn, W.J.; Gupta, S. Colorectal Cancer and Dysplasia in Inflammatory Bowel Disease: A Review of Disease Epidemiology, Pathophysiology, and Management. Cancer Prev. Res. 2016, 9, 887–894. [Google Scholar] [CrossRef] [Green Version]
- Carli, E.; Caviglia, G.; Pellicano, R.; Fagoonee, S.; Rizza, S.; Astegiano, M.; Saracco, G.; Ribaldone, D. Incidence of Prostate Cancer in Inflammatory Bowel Disease: A Meta-Analysis. Medicina 2020, 56, 285. [Google Scholar] [CrossRef] [PubMed]
- Algaba, A.; Guerra, I.; Castaño, Á.; de la Poza, G.; Castellano, V.M.; López, M.; Bermejo, F. Risk of cancer, with special reference to extra-intestinal malignancies, in patients with inflammatory bowel disease. World J. Gastroenterol. 2013, 19, 9359–9365. [Google Scholar] [CrossRef] [PubMed]
- Hemminki, K.; Li, X.; Sundquist, J.; Sundquist, K. Cancer risks in ulcerative colitis patients. Int. J. Cancer 2008, 123, 1417–1421. [Google Scholar] [CrossRef]
- Hemminki, K.; Li, X.; Sundquist, J.; Sundquist, K. Cancer risks in Crohn disease patients. Ann. Oncol. 2009, 20, 574–580. [Google Scholar] [CrossRef]
- Jung, Y.S.; Han, M.; Park, S.; Kim, W.H.; Cheon, J.H. Cancer Risk in the Early Stages of Inflammatory Bowel Disease in Korean Patients: A Nationwide Population-based Study. J. Crohn’s Coliti 2017, 11, 954–962. [Google Scholar] [CrossRef]
- Ekbom, A.; Helmick, C.; Zack, M.; Adami, H.-O. Extracolonic malignancies in inflammatory bowel disease. Cancer 1991, 67, 2015–2020. [Google Scholar] [CrossRef]
- Mosher, C.A.; Brown, G.R.; Weideman, R.A.; Crook, T.W.; Cipher, D.J.; Spechler, S.J.; Feagins, L.A. Incidence of Colorectal Cancer and Extracolonic Cancers in Veteran Patients With Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2018, 24, 617–623. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Blanchard, J.F.; Kliewer, E.; Wajda, A. Cancer risk in patients with inflammatory bowel disease: A population-based study. Cancer 2001, 91, 854–862. [Google Scholar] [CrossRef]
- Reulen, R.C.; Kellen, E.; Buntinx, F.; Brinkman, M.; Zeegers, M. A meta-analysis on the association between bladder cancer and occupation. Scand. J. Urol. Nephrol. 2008, 42, 64–78. [Google Scholar] [CrossRef]
- Zhang, C.; Liu, S.; Peng, L.; Wu, J.; Zeng, X.; Lu, Y.; Shen, H.; Luo, D. Does inflammatory bowel disease increase the risk of lower urinary tract tumors: A meta-analysis. Transl. Androl. Urol. 2021, 10, 164–173. [Google Scholar] [CrossRef]
- Long, M.D.; Herfarth, H.H.; Pipkin, C.A.; Porter, C.Q.; Sandler, R.S.; Kappelman, M.D. Increased Risk for Non-Melanoma Skin Cancer in Patients With Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2010, 8, 268–274. [Google Scholar] [CrossRef] [Green Version]
- Lopez, A.; Mounier, M.; Bouvier, A.M.; Carrat, F.; Maynadié, M.; Beaugerie, L.; Peyrin-Biroulet, L. Increased risk of acute myeloid leukemias and myelodysplastic syndromes in patients who received thiopurine treatment for inflammatory bowel disease. Clin. Gastroenterol. Hepatol. 2014, 12, 1324–1329. [Google Scholar] [CrossRef]
- Sands, B.E.; Grabert, S. Epidemiology of inflammatory bowel disease and overview of pathogenesis. Med. Health R. I. 2009, 92, 73–77. [Google Scholar]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Risk Factors | Cases (n = 23) | Controls (n = 250) | p Value |
|---|---|---|---|
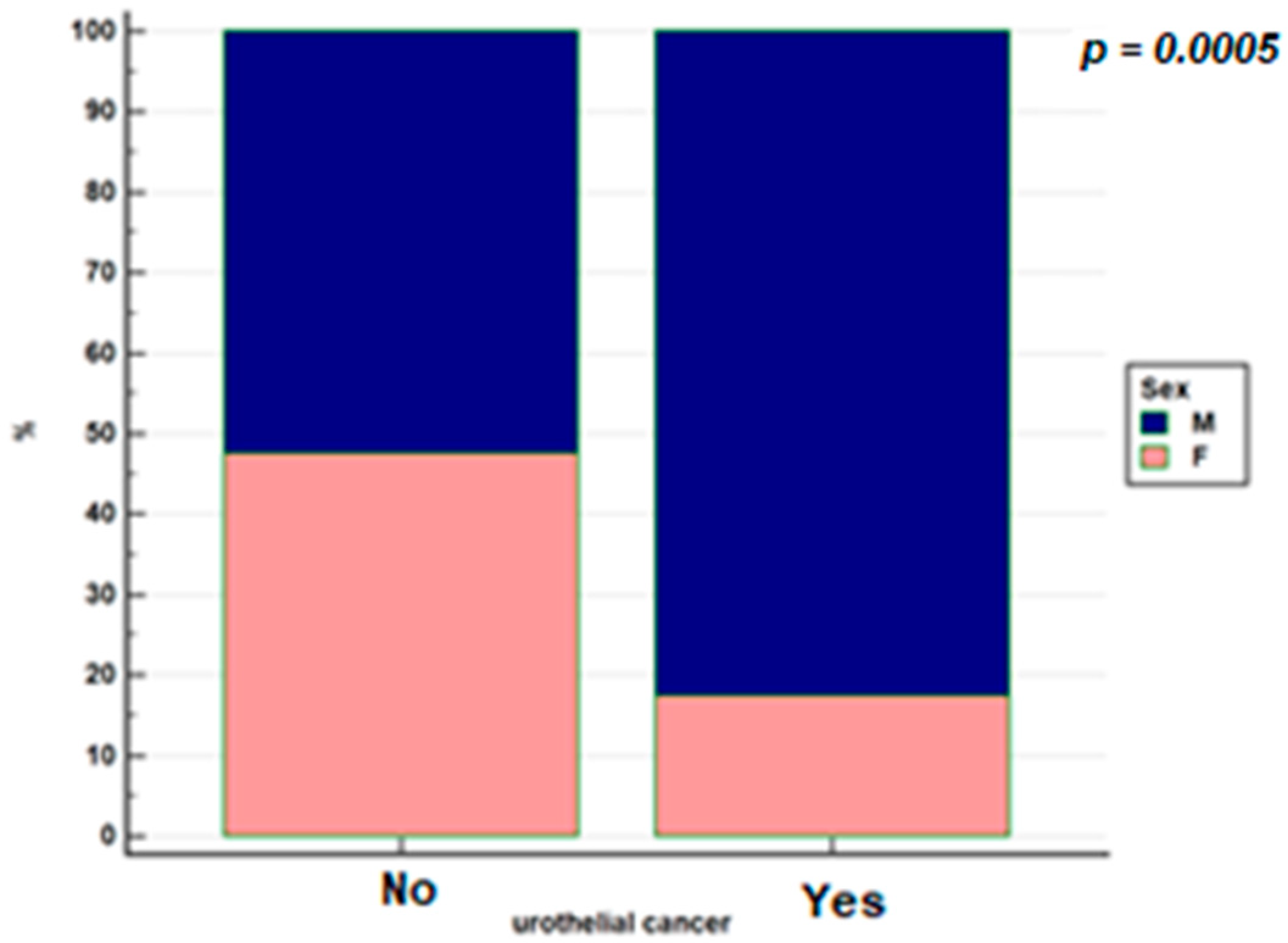
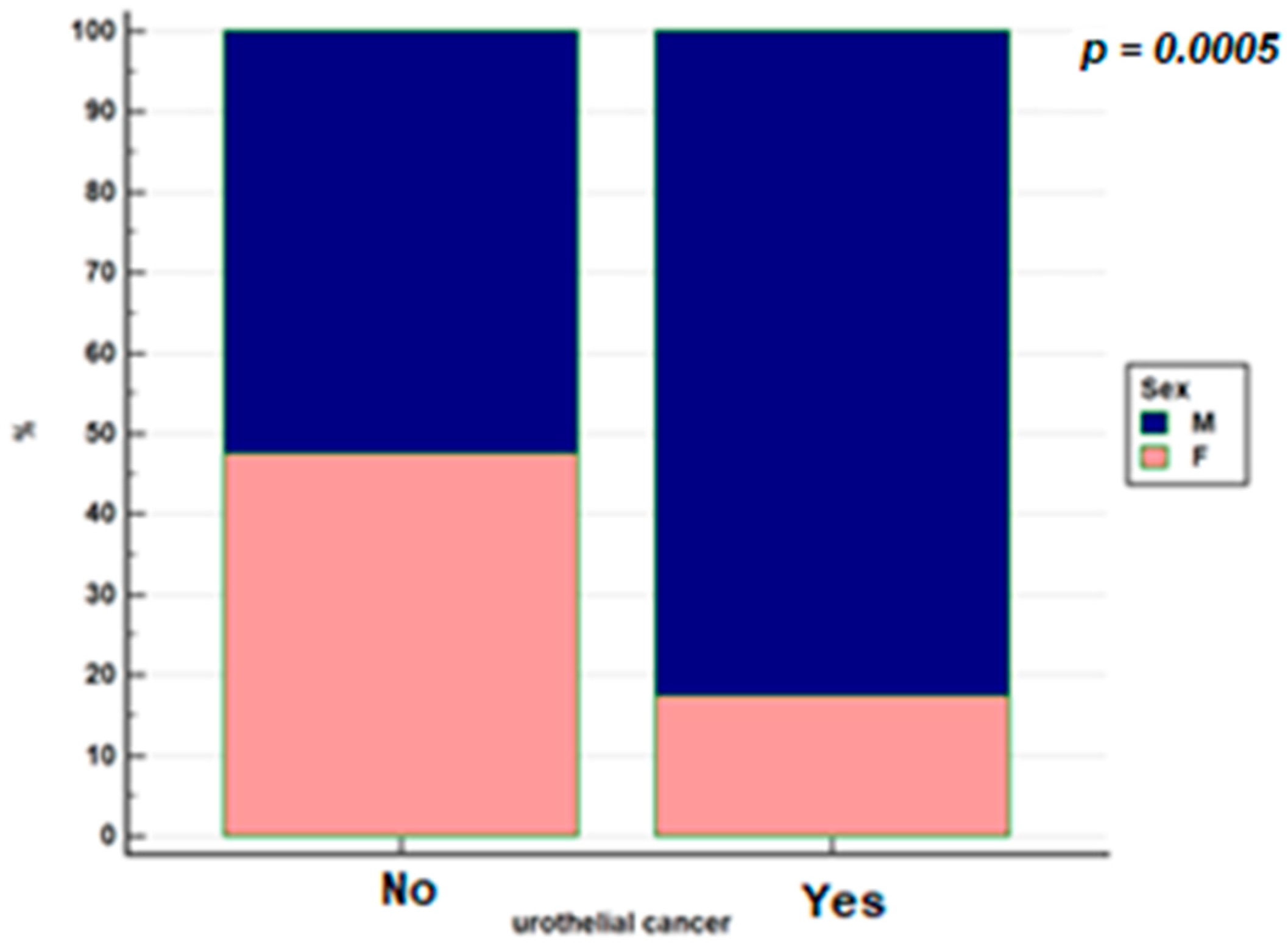
| Sex | p = 0.005 | ||
| Males | 19 (82.6%) | 131 (52.4%) | |
| Females | 4 (17.4%) | 119 (47.6%) | |
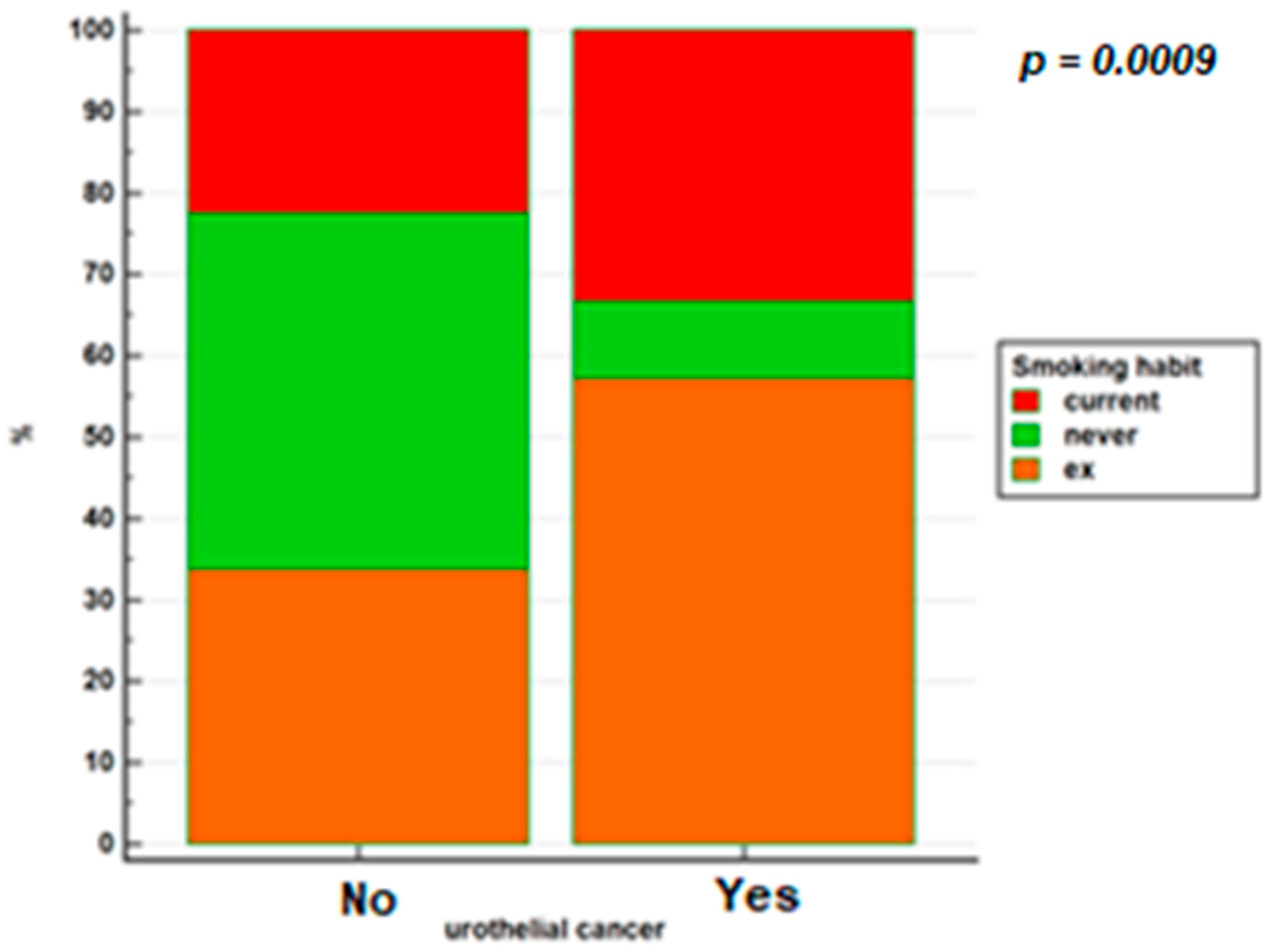
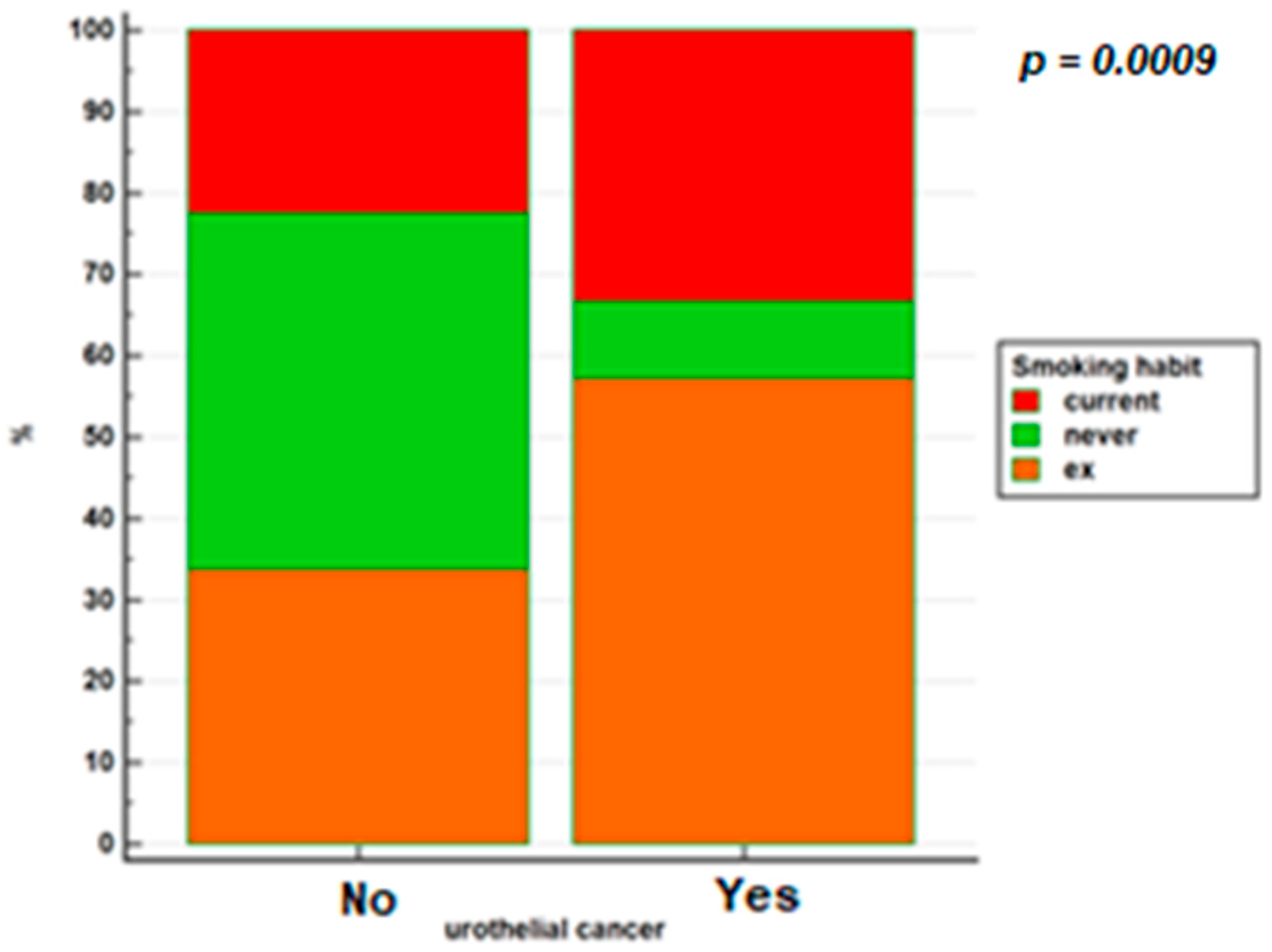
| Smoking habit | p = 0.009 | ||
| Active smokers | 7 (33%) | 56 (22.5%) | |
| Former smokers | 12 (57%) | 84 (33.7%) | |
| Never smokers | 2 (9.5%) | 109 (43.8%) | |
| IBD type | p = 0.19 | ||
| Crohn’s disease | 17 (73.9%) | 154 (61.1%) | |
| Ulcerative colitis | 5 (21.7%) | 93 (37.2%) | |
| IBD-U | 1 (4.4%) | 3 (1.2%) | |
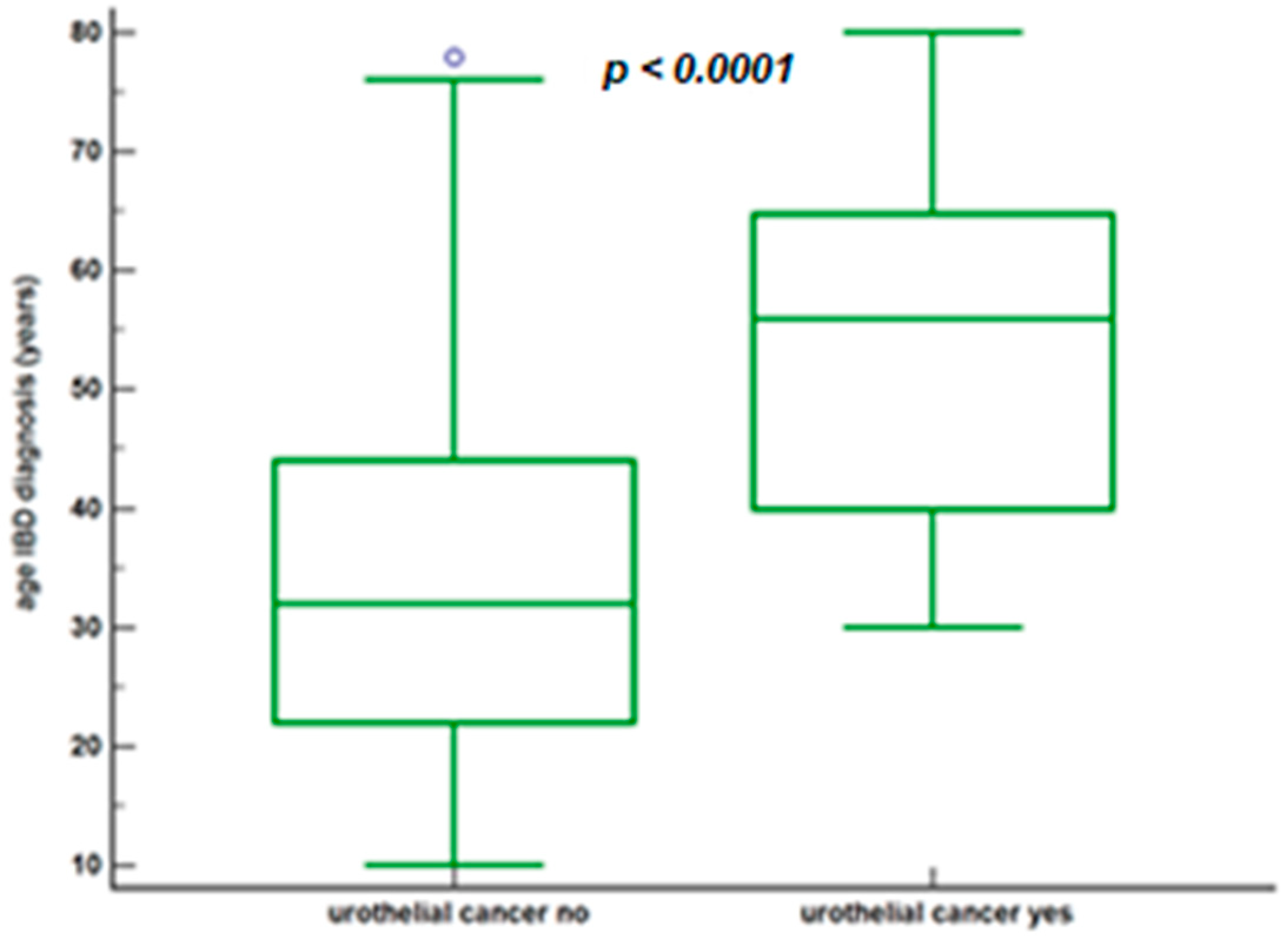
| Age at diagnosis of IBD | p < 0.0001 | ||
| Year (median, IQR) | 56.0, 40.0–64.8 | 32.0, 22.0–44.0 | |
| Mesalazine | p = 0.02 | ||
| Yes | 19 (82.6%) | 237 (94.8%) | |
| No | 4 (17.4%) | 13 (5.2%) | |
| Duration mesalazine | p = 0.053 | ||
| Months (median, IQR) | 48.0, 8.25–188.25 | 88.5, 48.00–179.00 | |
| Thiopurine | p = 0.38 | ||
| Yes | 5 (21.7%) | 76 (30.4%) | |
| No | 18 (78.3%) | 174 (69.9%) | |
| Duration thiopurine | p = 0.79 | ||
| Months (median, IQR) | 40.00, 18.25–60.00 | 31, 6.00–82.00 | |
| Anti-TNF | p = 0.012 | ||
| Yes | 1 (4.3%) | 71 (28.4%) | |
| No | 22 (95.7%) | 179 (71.6%) | |
| Surgical resection | p = 0.69 | ||
| Yes | 8 (34.8%) | 77 (30.8%) | |
| No | 15 (65.2%) | 173 (69.2%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caviglia, G.P.; Martini, G.; Armandi, A.; Rosso, C.; Vernero, M.; Bugianesi, E.; Astegiano, M.; Saracco, G.M.; Ribaldone, D.G. Risk Factors of Urothelial Cancer in Inflammatory Bowel Disease. J. Clin. Med. 2021, 10, 3257. https://doi.org/10.3390/jcm10153257
Caviglia GP, Martini G, Armandi A, Rosso C, Vernero M, Bugianesi E, Astegiano M, Saracco GM, Ribaldone DG. Risk Factors of Urothelial Cancer in Inflammatory Bowel Disease. Journal of Clinical Medicine. 2021; 10(15):3257. https://doi.org/10.3390/jcm10153257
Chicago/Turabian StyleCaviglia, Gian Paolo, Giorgio Martini, Angelo Armandi, Chiara Rosso, Marta Vernero, Elisabetta Bugianesi, Marco Astegiano, Giorgio Maria Saracco, and Davide Giuseppe Ribaldone. 2021. "Risk Factors of Urothelial Cancer in Inflammatory Bowel Disease" Journal of Clinical Medicine 10, no. 15: 3257. https://doi.org/10.3390/jcm10153257
APA StyleCaviglia, G. P., Martini, G., Armandi, A., Rosso, C., Vernero, M., Bugianesi, E., Astegiano, M., Saracco, G. M., & Ribaldone, D. G. (2021). Risk Factors of Urothelial Cancer in Inflammatory Bowel Disease. Journal of Clinical Medicine, 10(15), 3257. https://doi.org/10.3390/jcm10153257