
Chronic Critical Illness Elicits a Unique Circulating Leukocyte Transcriptome in Sepsis Survivors

 ,
, 
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
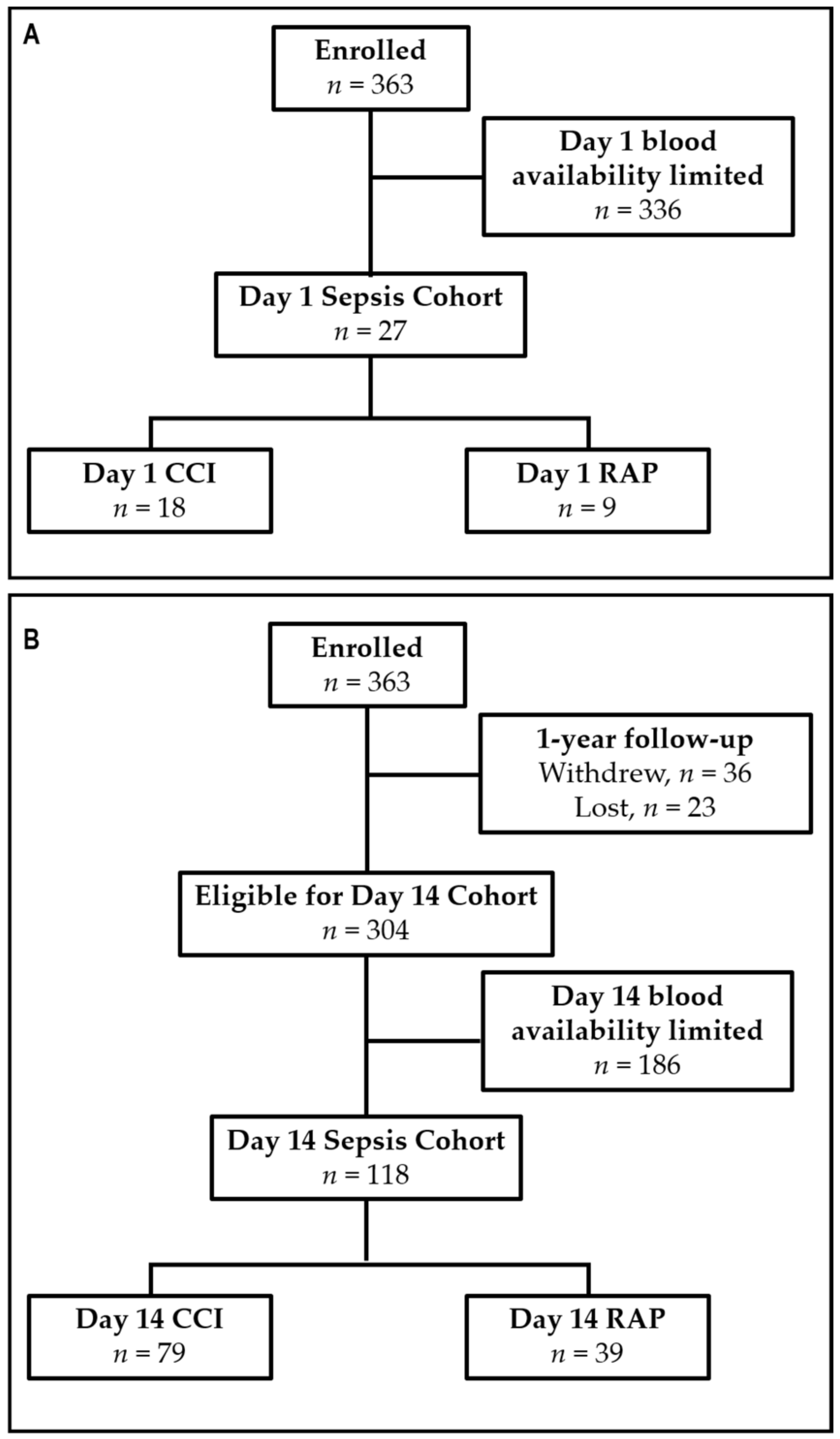
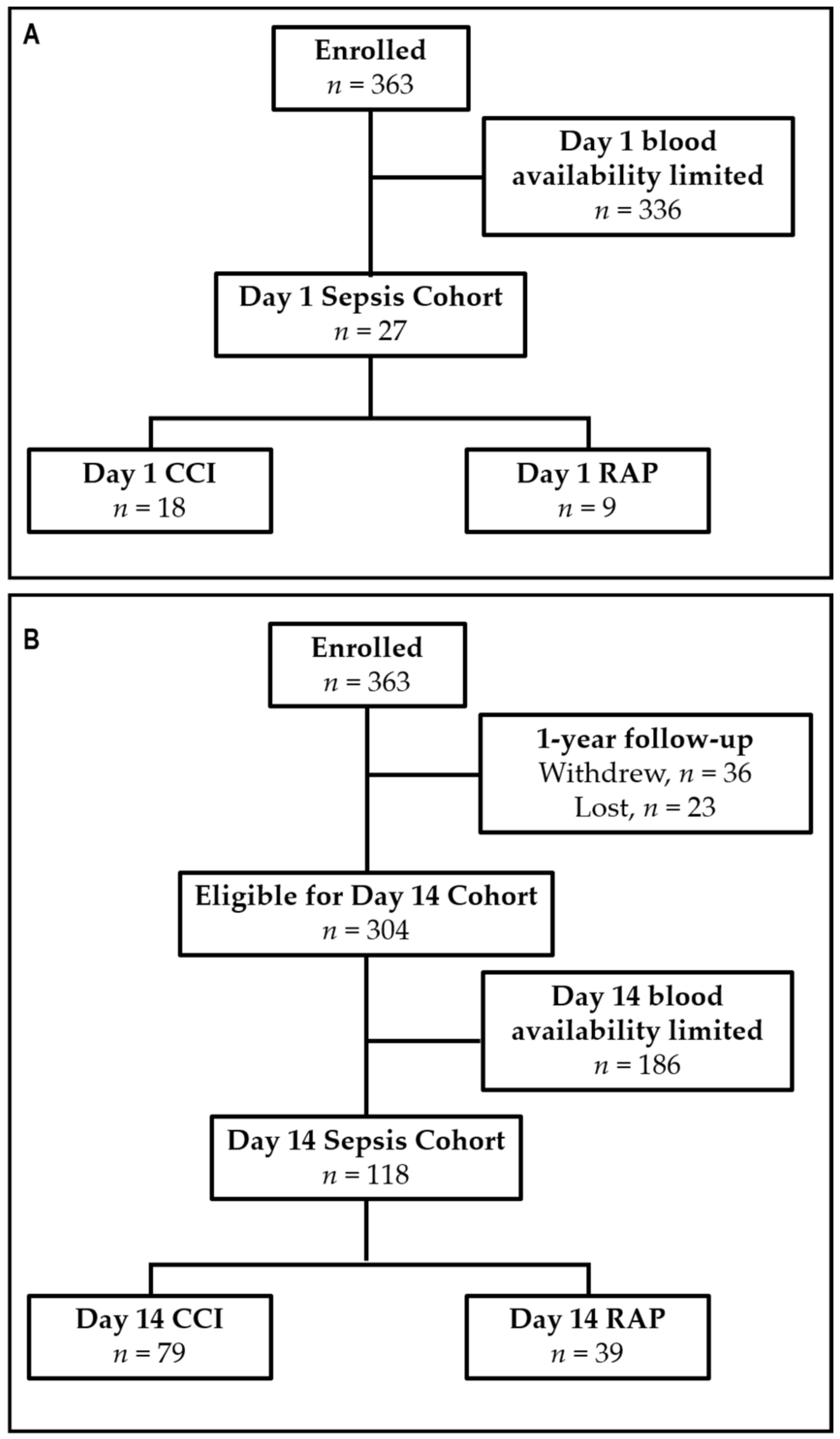
2.1. Study Design
2.2. Blood Collection
2.3. Gene Expression Profile and Statistical Analysis
3. Results
3.1. Patient Demographics
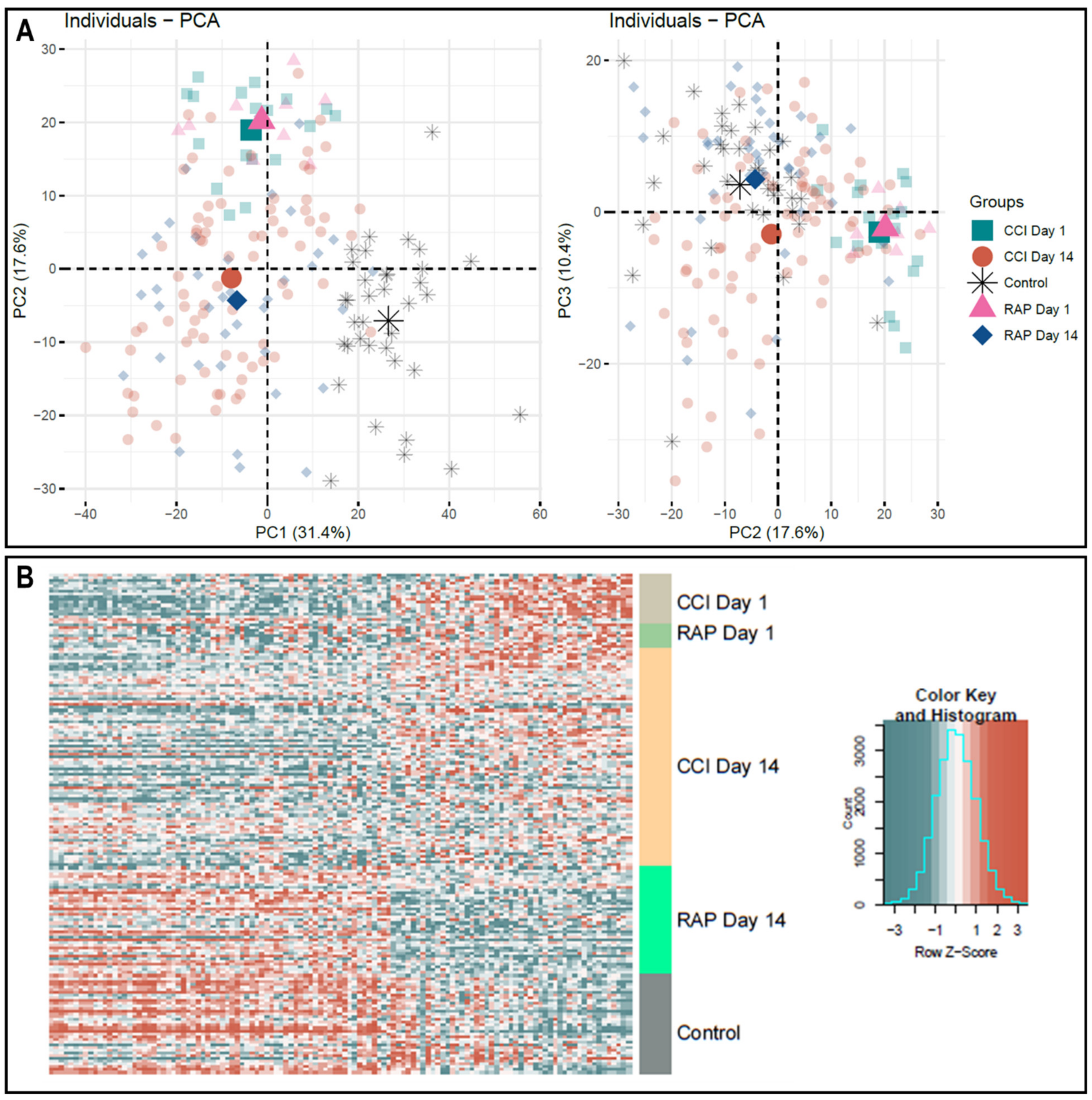
3.2. Time-Dependent Unique Leukocyte Transcriptome Pattern in CCI vs. Rapid Recovery
3.3. Unique Leukocyte Transcriptomic Pattern in Patients with Adverse Clinical Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stoller, J.; Halpin, L.; Weis, M.; Aplin, B.; Qu, W.; Georgescu, C.; Nazzal, M. Epidemiology of severe sepsis: 2008–2012. J. Crit. Care 2016, 31, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Brakenridge, S.C.; Efron, P.A.; Cox, M.C.; Stortz, J.A.; Hawkins, R.B.; Ghita, G.; Gardner, A.; Mohr, A.M.; Anton, S.D.; Moldawer, L.L.; et al. Current Epidemiology of Surgical Sepsis: Discordance Between Inpatient Mortality and 1-year Outcomes. Ann. Surg. 2019, 270, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.M.; Rhodes, A.; Phillips, G.S.; Townsend, S.R.; Schorr, C.A.; Beale, R.; Osborn, T.; Lemeshow, S.; Chiche, J.D.; Artigas, A.; et al. Surviving Sepsis Campaign: Association between performance metrics and outcomes in a 7.5-year study. Crit. Care Med. 2015, 43, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, E.K.; Rubenstein, A.R.; Radin, G.T.; Wiener, R.S.; Walkey, A.J. Two decades of mortality trends among patients with severe sepsis: A comparative meta-analysis. Crit. Care Med. 2014, 42, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Gardner, A.K.; Ghita, G.L.; Wang, Z.; Ozrazgat-Baslanti, T.; Raymond, S.L.; Mankowski, R.T.; Brumback, B.A.; Efron, P.A.; Bihorac, A.; Moore, F.A.; et al. The Development of Chronic Critical Illness Determines Physical Function, Quality of Life, and Long-Term Survival Among Early Survivors of Sepsis in Surgical ICUs. Crit. Care Med. 2019, 47, 566–573. [Google Scholar] [CrossRef]
- Stortz, J.A.; Murphy, T.J.; Raymond, S.L.; Mira, J.C.; Ungaro, R.; Dirain, M.L.; Nacionales, D.C.; Loftus, T.J.; Wang, Z.; Ozrazgat-Baslanti, T.; et al. Evidence for Persistent Immune Suppression in Patients Who Develop Chronic Critical Illness After Sepsis. Shock 2018, 49, 249–258. [Google Scholar] [CrossRef]
- Mira, J.C.; Gentile, L.F.; Mathias, B.J.; Efron, P.A.; Brakenridge, S.C.; Mohr, A.M.; Moore, F.A.; Moldawer, L.L. Sepsis Pathophysiology, Chronic Critical Illness, and Persistent Inflammation-Immunosuppression and Catabolism Syndrome. Crit. Care Med. 2017, 4, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, R.B.; Raymond, S.L.; Stortz, J.A.; Horiguchi, H.; Brakenridge, S.C.; Gardner, A.; Efron, P.A.; Bihorac, A.; Segal, M.; Moore, F.A.; et al. Chronic Critical Illness and the Persistent Inflammation, Immunosuppression, and Catabolism Syndrome. Front. Immunol. 2018, 9, 1511. [Google Scholar] [CrossRef]
- Stortz, J.A.; Mira, J.C.; Raymond, S.L.; Loftus, T.J.; Ozrazgat-Baslanti, T.; Wang, Z.; Ghita, G.L.; Leeuwenburgh, C.; Segal, M.S.; Bihorac, A.; et al. Benchmarking clinical outcomes and the immunocatabolic phenotype of chronic critical illness after sepsis in surgical intensive care unit patients. J. Trauma Acute Care Surg. 2018, 84, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Yende, S.; Austin, S.; Rhodes, A.; Finfer, S.; Opal, S.; Thompson, T.; Bozza, F.A.; LaRosa, S.P.; Ranieri, V.M.; Angus, D.C. Long-Term Quality of Life Among Survivors of Severe Sepsis: Analyses of Two International Trials. Crit. Care Med. 2016, 44, 1461–1467. [Google Scholar] [CrossRef] [PubMed]
- Gentile, L.F.; Cuenca, A.G.; Efron, P.A.; Ang, D.; Bihorac, A.; McKinley, B.A.; Moldawer, L.L.; Moore, F.A. Persistent inflammation and immunosuppression: A common syndrome and new horizon for surgical intensive care. J. Trauma Acute Care Surg. 2012, 72, 1491–1501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coopersmith, C.M.; De Backer, D.; Deutschman, C.S.; Ferrer, R.; Lat, I.; Machado, F.R.; Martin, G.S.; Martin-Loeches, I.; Nunnally, M.E.; Antonelli, M.; et al. Surviving Sepsis Campaign: Research Priorities for Sepsis and Septic Shock. Crit. Care Med. 2018, 46, 1334–1356. [Google Scholar] [CrossRef] [PubMed]
- McHugh, L.; Seldon, T.A.; Brandon, R.A.; Kirk, J.T.; Rapisarda, A.; Sutherland, A.J.; Presneill, J.J.; Venter, D.J.; Lipman, J.; Thomas, M.R.; et al. A Molecular Host Response Assay to Discriminate Between Sepsis and Infection-Negative Systemic Inflammation in Critically Ill Patients: Discovery and Validation in Independent Cohorts. PLoS Med. 2015, 12, e1001916. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, T.E.; Khatri, P. Benchmarking Sepsis Gene Expression Diagnostics Using Public Data. Crit. Care Med. 2017, 45, R149. [Google Scholar] [CrossRef] [Green Version]
- Sutherland, A.; Thomas, M.; Brandon, R.A.; Brandon, R.B.; Lipman, J.; Tang, B.; McLean, A.; Pascoe, R.; Price, G.; Nguyen, T.; et al. Development and validation of a novel molecular biomarker diagnostic test for the early detection of sepsis. Crit. Care 2011, 15, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Scicluna, B.P.; van Vught, L.A.; Zwinderman, A.H.; Wiewel, M.A.; Davenport, E.E.; Burnham, K.L.; Nurnberg, P.; Schultz, M.J.; Horn, J.; Cremer, O.L.; et al. Classification of patients with sepsis according to blood genomic endotype: A prospective cohort study. Lancet Respir. Med. 2017, 5, 816–826. [Google Scholar] [CrossRef]
- Brakenridge, S.C.; Efron, P.A.; Stortz, J.A.; Ozrazgat-Baslanti, T.; Ghita, G.; Wang, Z.; Bihorac, A.; Mohr, A.M.; Brumback, B.A.; Moldawer, L.L.; et al. The impact of age on the innate immune response and outcomes after severe sepsis/septic shock in trauma and surgical intensive care unit patients. J. Trauma Acute Care Surg. 2018, 85, 247–255. [Google Scholar] [CrossRef]
- Croft, C.A.; Moore, F.A.; Efron, P.A.; Marker, P.S.; Gabrielli, A.; Westhoff, L.S.; Lottenberg, L.; Jordan, J.; Klink, V.; Sailors, R.M.; et al. Computer versus paper system for recognition and management of sepsis in surgical intensive care. J. Trauma Acute Care Surg. 2014, 76, 318–319. [Google Scholar] [CrossRef]
- Loftus, T.J.; Mira, J.C.; Ozrazgat-Baslanti, T.; Ghita, G.L.; Wang, Z.; Stortz, J.A.; Brumback, B.A.; Bihorac, A.; Segal, M.S.; Anton, S.D.; et al. Sepsis and Critical Illness Research Center investigators: Protocols and standard operating procedures for a prospective cohort study of sepsis in critically ill surgical patients. BMJ Open 2017, 7, e015136. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Ferreira, F.L.; Bota, D.P.; Bross, A.; Melot, C.; Vincent, J.L. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA 2001, 286, 1754–1758. [Google Scholar] [CrossRef] [Green Version]
- Cuenca, A.G.; Gentile, L.F.; Lopez, M.C.; Ungaro, R.; Liu, H.; Xiao, W.; Seok, J.; Mindrinos, M.N.; Ang, D.; Baslanti, T.O.; et al. Development of a genomic metric that can be rapidly used to predict clinical outcome in severely injured trauma patients. Crit. Care Med. 2013, 41, 1175–1185. [Google Scholar] [CrossRef] [Green Version]
- Rosse, C.; Cole, S.B.; Appleton, C.; Press, O.W.; Clagett, J. The relative importance of the bone marrow and spleen in the production and dissemination of B lymphocytes. Cell Immunol. 1978, 37, 254–262. [Google Scholar] [CrossRef]
- DiGiandomenico, A.; Veach, R.A.; Zienkiewicz, J.; Moore, D.J.; Wylezinski, L.S.; Hutchens, M.A.; Hawiger, J. The “genomic storm” induced by bacterial endotoxin is calmed by a nuclear transport modifier that attenuates localized and systemic inflammation. PLoS ONE 2014, 9, e110183. [Google Scholar] [CrossRef] [Green Version]
- Xiao, W.; Mindrinos, M.N.; Seok, J.; Cuschieri, J.; Cuenca, A.G.; Gao, H.; Hayden, D.L.; Hennessy, L.; Moore, E.E.; Minei, J.P.; et al. A genomic storm in critically injured humans. J. Exp. Med. 2011, 208, 2581–2590. [Google Scholar] [CrossRef]
- Buttrick, T.S.; Wang, W.; Yung, C.; Trieu, K.G.; Patel, K.; Khoury, S.J.; Ai, X.; Elyaman, W. Foxo1 Promotes Th9 Cell Differentiation and Airway Allergy. Sci. Rep. 2018, 8, 818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, Y.; Zajac, A.J. IL-21 and T Cell Differentiation: Consider the Context. Trends. Immunol. 2016, 37, 557–568. [Google Scholar] [CrossRef] [Green Version]
- Shi, Y.; Liu, C.H.; Roberts, A.I.; Das, J.; Xu, G.; Ren, G.; Zhang, Y.; Zhang, L.; Yuan, Z.R.; Tan, H.S.; et al. Granulocyte-macrophage colony-stimulating factor (GM-CSF) and T-cell responses: What we do and don’t know. Cell Res. 2006, 16, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Horiguchi, H.; Loftus, T.J.; Hawkins, R.B.; Raymond, S.L.; Stortz, J.A.; Hollen, M.K.; Weiss, B.P.; Miller, E.S.; Bihorac, A.; Larson, S.D.; et al. Innate Immunity in the Persistent Inflammation, Immunosuppression, and Catabolism Syndrome and Its Implications for Therapy. Front. Immunol. 2018, 9, 595. [Google Scholar] [CrossRef] [PubMed]
- Drewry, A.M.; Samra, N.; Skrupky, L.P.; Fuller, B.M.; Compton, S.M.; Hotchkiss, R.S. Persistent lymphopenia after diagnosis of sepsis predicts mortality. Shock 2014, 42, 383–391. [Google Scholar] [CrossRef] [Green Version]
- Darden, D.B.; Kelly, L.S.; Fenner, B.P.; Moldawer, L.L.; Mohr, A.M.; Efron, P.A. Dysregulated Immunity and Immunotherapy after Sepsis. J. Clin. Med. 2021, 10, 1742. [Google Scholar] [CrossRef]
- Raymond, S.L.; Hawkins, R.B.; Murphy, T.J.; Rincon, J.C.; Stortz, J.A.; Lopez, M.C.; Ungaro, R.; Ellett, F.; Baker, H.V.; Wynn, J.L.; et al. Impact of toll-like receptor 4 stimulation on human neonatal neutrophil spontaneous migration, transcriptomics, and cytokine production. J. Mol. Med. 2018, 96, 673–684. [Google Scholar] [CrossRef]
- Sweeney, T.E.; Azad, T.D.; Donato, M.; Haynes, W.A.; Perumal, T.M.; Henao, R.; Bermejo-Martin, J.F.; Almansa, R.; Tamayo, E.; Howrylak, J.A.; et al. Unsupervised Analysis of Transcriptomics in Bacterial Sepsis Across Multiple Datasets Reveals Three Robust Clusters. Crit. Care Med. 2018, 46, 915–925. [Google Scholar] [CrossRef]
- Sweeney, T.E.; Perumal, T.M.; Henao, R.; Nichols, M.; Howrylak, J.A.; Choi, A.M.; Bermejo-Martin, J.F.; Almansa, R.; Tamayo, E.; Davenport, E.E.; et al. A community approach to mortality prediction in sepsis via gene expression analysis. Nat. Commun. 2018, 9, 694. [Google Scholar] [CrossRef] [Green Version]
- Ulas, T.; Pirr, S.; Fehlhaber, B.; Bickes, M.S.; Loof, T.G.; Vogl, T.; Mellinger, L.; Heinemann, A.S.; Burgmann, J.; Schoning, J.; et al. S100-alarmin-induced innate immune programming protects newborn infants from sepsis. Nat. Immunol. 2017, 18, 622–632. [Google Scholar] [CrossRef] [PubMed]
- Davenport, E.E.; Burnham, K.L.; Radhakrishnan, J.; Humburg, P.; Hutton, P.; Mills, T.C.; Rautanen, A.; Gordon, A.C.; Garrard, C.; Hill, A.V.; et al. Genomic landscape of the individual host response and outcomes in sepsis: A prospective cohort study. Lancet Respir. Med. 2016, 4, 259–271. [Google Scholar] [CrossRef] [Green Version]
- Mira, J.C.; Szpila, B.E.; Nacionales, D.C.; Lopez, M.C.; Gentile, L.F.; Mathias, B.J.; Vanzant, E.L.; Ungaro, R.; Holden, D.; Rosenthal, M.D.; et al. Patterns of gene expression among murine models of hemorrhagic shock/trauma and sepsis. Physiol. Genom. 2016, 48, 135–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kangelaris, K.N.; Prakash, A.; Liu, K.D.; Aouizerat, B.; Woodruff, P.G.; Erle, D.J.; Rogers, A.; Seeley, E.J.; Chu, J.; Liu, T.; et al. Increased expression of neutrophil-related genes in patients with early sepsis-induced ARDS. Am. J. Physiol. Lung Cell. Mol. Physiol. 2015, 308, L1102–L1113. [Google Scholar] [CrossRef] [Green Version]
- Gentile, L.F.; Nacionales, D.C.; Lopez, M.C.; Vanzant, E.; Cuenca, A.; Cuenca, A.G.; Ungaro, R.; Szpila, B.E.; Larson, S.; Joseph, A.; et al. Protective immunity and defects in the neonatal and elderly immune response to sepsis. J. Immunol. 2014, 192, 3156–3165. [Google Scholar] [CrossRef] [Green Version]
- Desai, K.H.; Tan, C.S.; Leek, J.T.; Maier, R.V.; Tompkins, R.G.; Storey, J.D. Inflammation, the Host Response to Injury Large-Scale Collaborative Research P: Dissecting inflammatory complications in critically injured patients by within-patient gene expression changes: A longitudinal clinical genomics study. PLoS Med. 2011, 8, e1001093. [Google Scholar] [CrossRef] [Green Version]
- Warren, H.S.; Elson, C.M.; Hayden, D.L.; Schoenfeld, D.A.; Cobb, J.P.; Maier, R.V.; Moldawer, L.L.; Moore, E.E.; Harbrecht, B.G.; Pelak, K.; et al. A genomic score prognostic of outcome in trauma patients. Mol. Med. 2009, 15, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Borozan, I.; Feld, J.; Sun, J.; Tannis, L.L.; Coltescu, C.; Heathcote, J.; Edwards, A.M.; McGilvray, I.D. Hepatic gene expression discriminates responders and nonresponders in treatment of chronic hepatitis C viral infection. Gastroenterology 2005, 128, 1437–1444. [Google Scholar] [CrossRef] [PubMed]
- Raymond, S.L.; Hawkins, R.B.; Wang, Z.; Mira, J.C.; Stortz, J.A.; Han, F.; Lanz, J.D.; Hennessy, L.V.; Brumback, B.A.; Baker, H.V.; et al. Prospective Validation of a Transcriptomic Metric in Severe Trauma. Ann. Surg. 2020, 271, 802–810. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, T.E.; Shidham, A.; Wong, H.R.; Khatri, P. A comprehensive time-course-based multicohort analysis of sepsis and sterile inflammation reveals a robust diagnostic gene set. Sci. Transl. Med. 2015, 7, 287ra71. [Google Scholar] [CrossRef] [Green Version]
- Stortz, J.A.; Cox, M.C.; Hawkins, R.B.; Ghita, G.L.; Brumback, B.A.; Mohr, A.M.; Moldawer, L.L.; Efron, P.A.; Brakenridge, S.C.; Moore, F.A. Phenotypic heterogeneity by site of infection in surgical sepsis: A prospective longitudinal study. Crit. Care 2020, 24, 203. [Google Scholar] [CrossRef]
- Mankowski, R.T.; Anton, S.D.; Ghita, G.L.; Brumback, B.; Darden, D.B.; Bihorac, A.; Moldawer, L.L.; Efron, P.A.; Brakenridge, S.C.; Moore, F.A. Older adults demonstrate biomarker evidence of the persistent inflammation, immunosuppression and catabolism syndrome (PICS) after sepsis. J. Gerontol. Biol. Sci. Med. Sci. 2021. [Google Scholar] [CrossRef]
- Darden, D.B.; Brakenridge, S.C.; Efron, P.A.; Ghita, G.L.; Fenner, B.P.; Kelly, L.S.; Brumback, B.A.; Mohr, A.M.; Moldawer, L.L.; Moore, F.A. Biomarker Evidence of the Persistent Inflammation, Immunosuppression and Catabolism Syndrome (PICS) in Chronic Critical Illness (CCI) after Surgical Sepsis. Ann. Surg. 2021, in press. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Overall (n = 118) | CCI (n = 79) | RAP (n = 39) | p-Value | |
|---|---|---|---|---|
| Demographics | ||||
| Male, n (%) | 67 (56.8) | 48 (60.8) | 19 (48.7) | 0.2401 |
| Age in years, mean (SD) | 60.3 (15) | 62.1 (13.4) | 56.5 (17.3) | 0.101 |
| Age ≥ 65, n (%) | 49 (41.5) | 34 (43) | 15 (38.5) | 0.6941 |
| Race, n (%) | 0.3041 | |||
| Caucasian | 104 (88.1) | 71 (89.9) | 33 (84.6) | |
| African American | 11 (9.3) | 7 (8.9) | 4 (10.3) | |
| Asian | 1 (0.8) | 0 (0) | 1 (2.6) | |
| Other | 2 (1.6) | 1 (1.3) | 1 (2.6) | |
| BMI, median (25th, 75th) | 29.5 (24.4, 38) | 29.5 (24.7, 39.2) | 28.7 (24.1, 37.3) | 0.6288 |
| Charlson comorbidity index, median (25th, 75th) | 3 (2, 5) | 3 (2, 5) | 3 (0, 4) | 0.0834 |
| APACHE II, median (25th, 75th) | 20 (14, 25) | 22 (16, 26) | 16 (11, 22) | 0.0029 |
| Inter-facility hospital transfer, n (%) | 55 (46.6) | 41 (51.9) | 14 (35.9) | 0.119 |
| Sepsis severity by Sepsis 3 criteria, n (%) | 0.1401 | |||
| Sepsis | 83 (70.3) | 52 (65.8) | 31 (79.5) | |
| Septic shock | 35 (29.7) | 27 (34.2) | 8 (20.5) | |
| Primary Sepsis Diagnosis, n (%) | 0.36 | |||
| CLABSI/Bacteremia | 2 (1.7) | 1 (1.3) | 1 (2.6) | |
| De Novo Intra-Abdominal Infection | 27 (22.9) | 20 (25.3) | 7 (17.9) | |
| Necrotizing Soft Tissue Infection | 15 (12.7) | 6 (7.6) | 9 (23.1) | |
| Pneumonia | 26 (22) | 19 (24.1) | 7 (17.9) | |
| Surgical Site Infection | 34 (28.8) | 23 (29.1) | 11 (28.2) | |
| Urosepsis | 6 (5.1) | 4 (5.1) | 2 (5.1) | |
| Other | 8 (6.8) | 6 (7.6) | 2 (5.1) | |
| Creatinine at sepsis onset, median (25th, 75th) | 1.1 (0.7, 1.7) | 1.1 (0.8, 2) | 1.1 (0.6, 1.2) | 0.1773 |
| ALC at sepsis onset, median (25th, 75th) | 0.3 (0, 0.6) | 0.3 (0, 0.6) | 0.2 (0, 0.6) | 0.6492 |
| Lactate at sepsis onset, median (25th, 75th) | 1.7 (1.1, 2.7) | 1.8 (1.2, 2.8) | 1.5 (1.1, 2.7) | 0.6106 |
| Inpatient outcomes | ||||
| In-hospital mortality, n (%) | 6 (5.1) | 6 (7.6) | 0 (0) | 0.1761 |
| ICU Length of Stay (LOS), median (25th, 75th) | 19 (11, 28) | 24 (18, 39) | 9 (5, 12) | <0.0001 |
| Hospital LOS, median (25th, 75th) | 28 (21, 38) | 32 (24, 48) | 21 (17, 30) | <0.0001 |
| Max SOFA score 24 h, median (25th, 75th) | 9 (7, 12) | 10 (9, 13) | 7 (5, 9) | <0.0001 |
| Multiple Organ Failure incidence, n (%) | 74 (62.7) | 60 (75.9) | 14 (35.9) | <0.0001 |
| Discharge disposition, n (%) | ||||
| “Good” disposition | 44 (37.3) | 18 (22.8) | 26 (66.7) | <0.0001 |
| Home | 7 (5.9) | 1 (1.3) | 6 (15.4) | |
| Home healthcare services | 26 (22) | 9 (11.4) | 17 (43.6) | |
| Rehab | 11 (9.3) | 8 (10.1) | 3 (7.7) | |
| “Poor” disposition | 74 (62.7) | 61 (77.2) | 13 (33.3) | <0.0001 |
| Long Term Acute Care facility | 34 (28.8) | 34 (43) | 0 (0) | |
| Skilled Nursing facility | 20 (16.9) | 8 (10.1) | 12 (30.8) | |
| Another Hospital | 9 (7.6) | 8 (10.1) | 1 (2.6) | |
| Hospice | 5 (4.2) | 5 (6.3) | 0 (0) | |
| Death | 6 (5.1) | 6 (7.6) | 0 (0) | |
| 30-day mortality, n (%) | 8 (6.8) | 7 (8.9) | 1 (2.6) | 0.2679 |
| 12-month mortality, n (%) | 35 (29.7) | 33 (41.8) | 2 (5.1) | <0.0001 |
| Zubrod at 12 months, median (25th, 75th) | 3 (1, 5) | 4 (2, 5) | 1 (1, 3) | <0.0001 |
| Genes | Function |
|---|---|
| ATG12 | Promotes autophagy |
| BAG6 | Antigen degradation and immune cell function and response |
| BLK | B-cell development and signaling |
| EHD1 | IL-2 secretion and T-cell proliferation |
| ERF | Hematopoietic stem cell differentiation |
| FOXO4 | Quiescence and maintenance of hematopoietic stem cells |
| NACC1 | Stem cell self-renewal and maintenance |
| SLC7A5 | T-cell differentiation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Darden, D.B.; Ghita, G.L.; Wang, Z.; Stortz, J.A.; Lopez, M.-C.; Cox, M.C.; Hawkins, R.B.; Rincon, J.C.; Kelly, L.S.; Fenner, B.P.; et al. Chronic Critical Illness Elicits a Unique Circulating Leukocyte Transcriptome in Sepsis Survivors. J. Clin. Med. 2021, 10, 3211. https://doi.org/10.3390/jcm10153211
Darden DB, Ghita GL, Wang Z, Stortz JA, Lopez M-C, Cox MC, Hawkins RB, Rincon JC, Kelly LS, Fenner BP, et al. Chronic Critical Illness Elicits a Unique Circulating Leukocyte Transcriptome in Sepsis Survivors. Journal of Clinical Medicine. 2021; 10(15):3211. https://doi.org/10.3390/jcm10153211
Chicago/Turabian StyleDarden, Dijoia B., Gabriela L. Ghita, Zhongkai Wang, Julie A. Stortz, Maria-Cecilia Lopez, Michael C. Cox, Russell B. Hawkins, Jaimar C. Rincon, Lauren S. Kelly, Brittany P. Fenner, and et al. 2021. "Chronic Critical Illness Elicits a Unique Circulating Leukocyte Transcriptome in Sepsis Survivors" Journal of Clinical Medicine 10, no. 15: 3211. https://doi.org/10.3390/jcm10153211
APA StyleDarden, D. B., Ghita, G. L., Wang, Z., Stortz, J. A., Lopez, M.-C., Cox, M. C., Hawkins, R. B., Rincon, J. C., Kelly, L. S., Fenner, B. P., Ozrazgat-Baslanti, T., Leeuwenburgh, C., Bihorac, A., Loftus, T. J., Moore, F. A., Brakenridge, S. C., Baker, H. V., Bacher, R., Mohr, A. M., ... Efron, P. A. (2021). Chronic Critical Illness Elicits a Unique Circulating Leukocyte Transcriptome in Sepsis Survivors. Journal of Clinical Medicine, 10(15), 3211. https://doi.org/10.3390/jcm10153211