
Obstructive Sleep Apnea, Hypercoagulability, and the Blood–Brain Barrier

 , ,
, ,  , , and
, , and
Abstract
1. Introduction
2. OSA: Definition, Clinical Consequences, and Treatments
3. OSA and the “Hypercoagulable State”
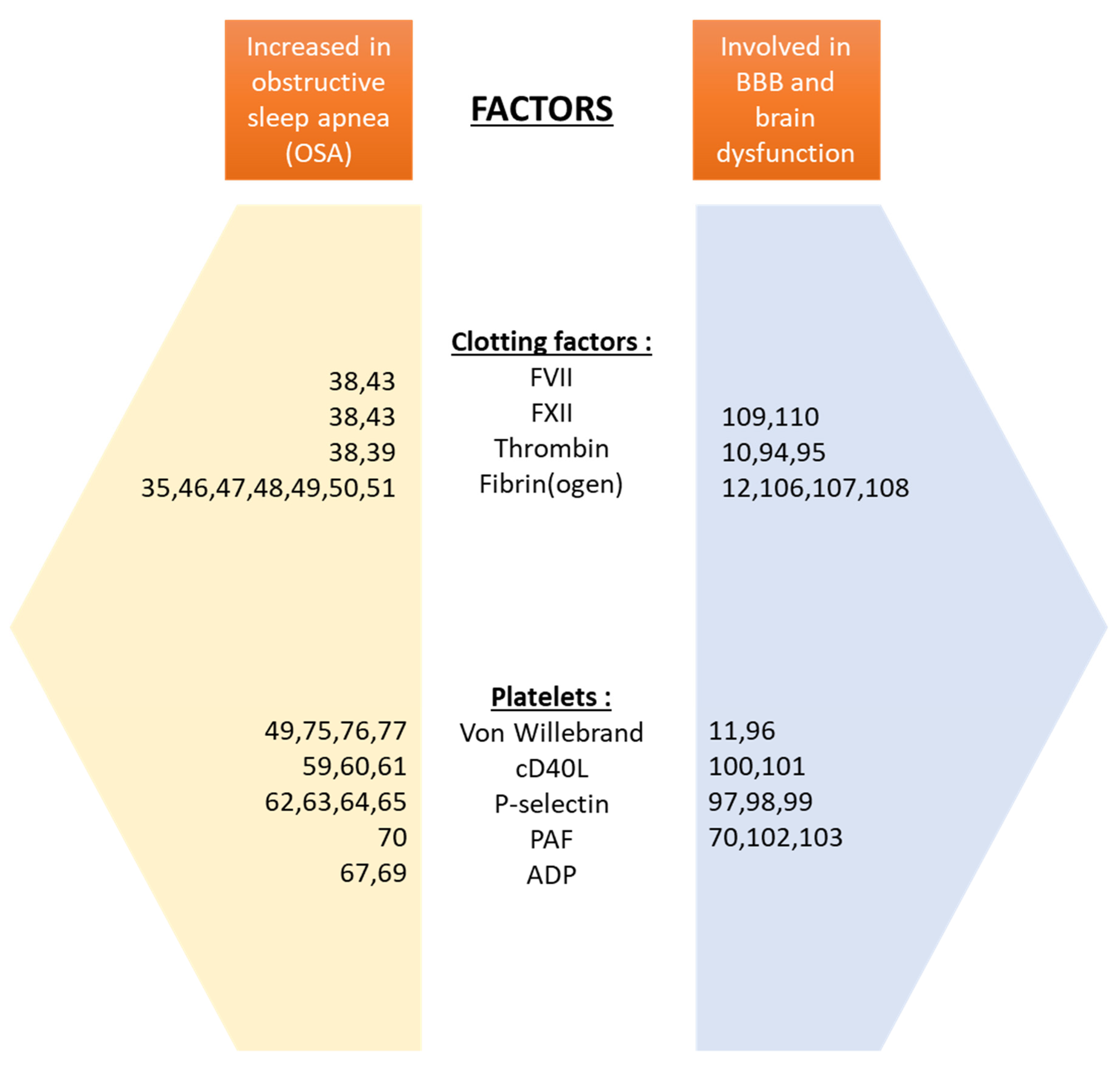
3.1. Factors Contributing to a Procoagulant State in OSA
3.1.1. Clotting Factors
3.1.2. Platelets
3.1.3. Von Willebrand Factor
3.2. Effects of CPAP on Coagulation Balance
4. Impact of OSA on BBB
4.1. Blood–Brain Barrier
4.2. OSA: Adverse Effects on BBB Function
4.3. Hypercoagulability and Possible Effects on BBB
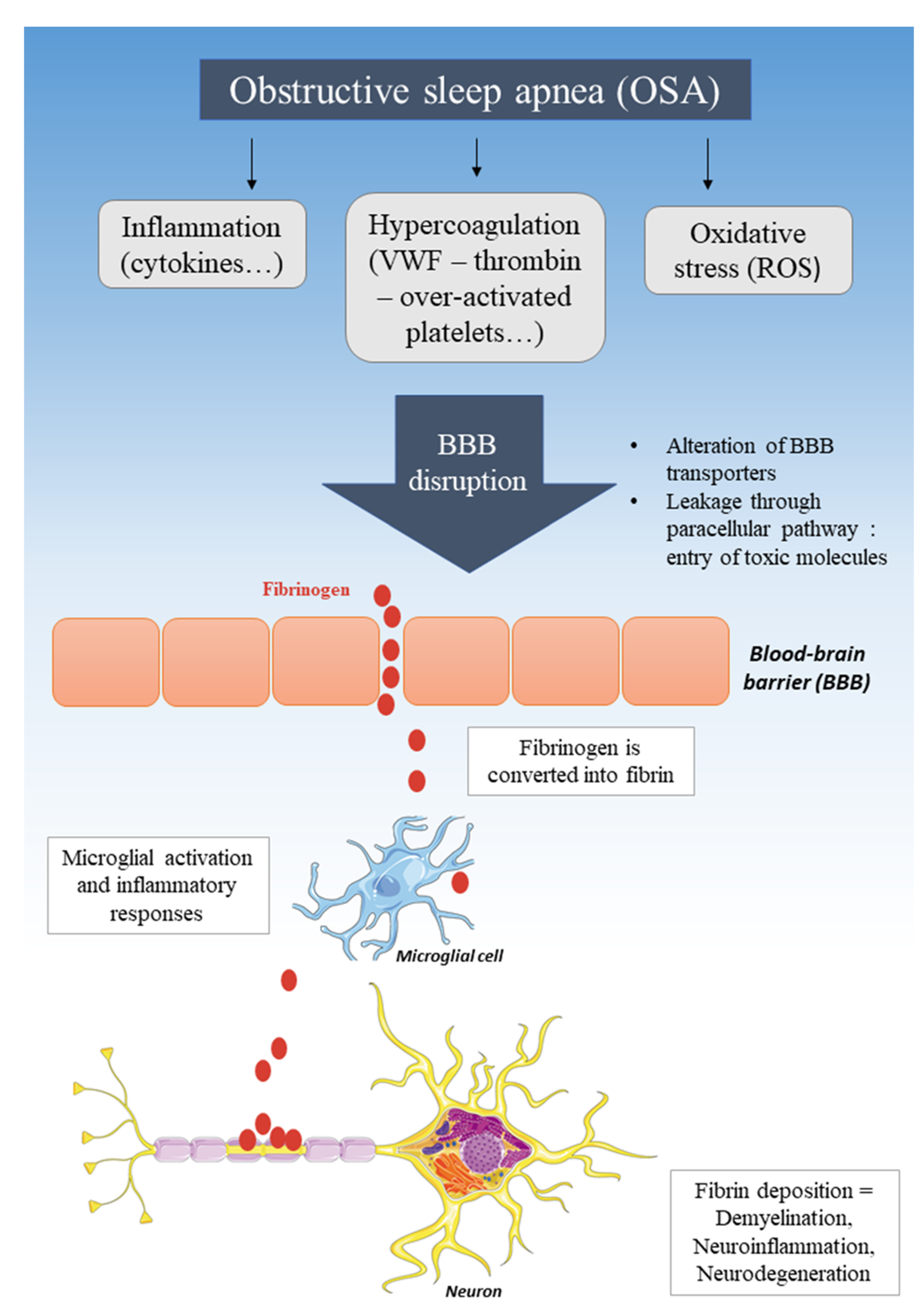
4.4. BBB Disruption, Entry of Fibrinogen, and Neurodegenerative Diseases
5. Potential Therapies
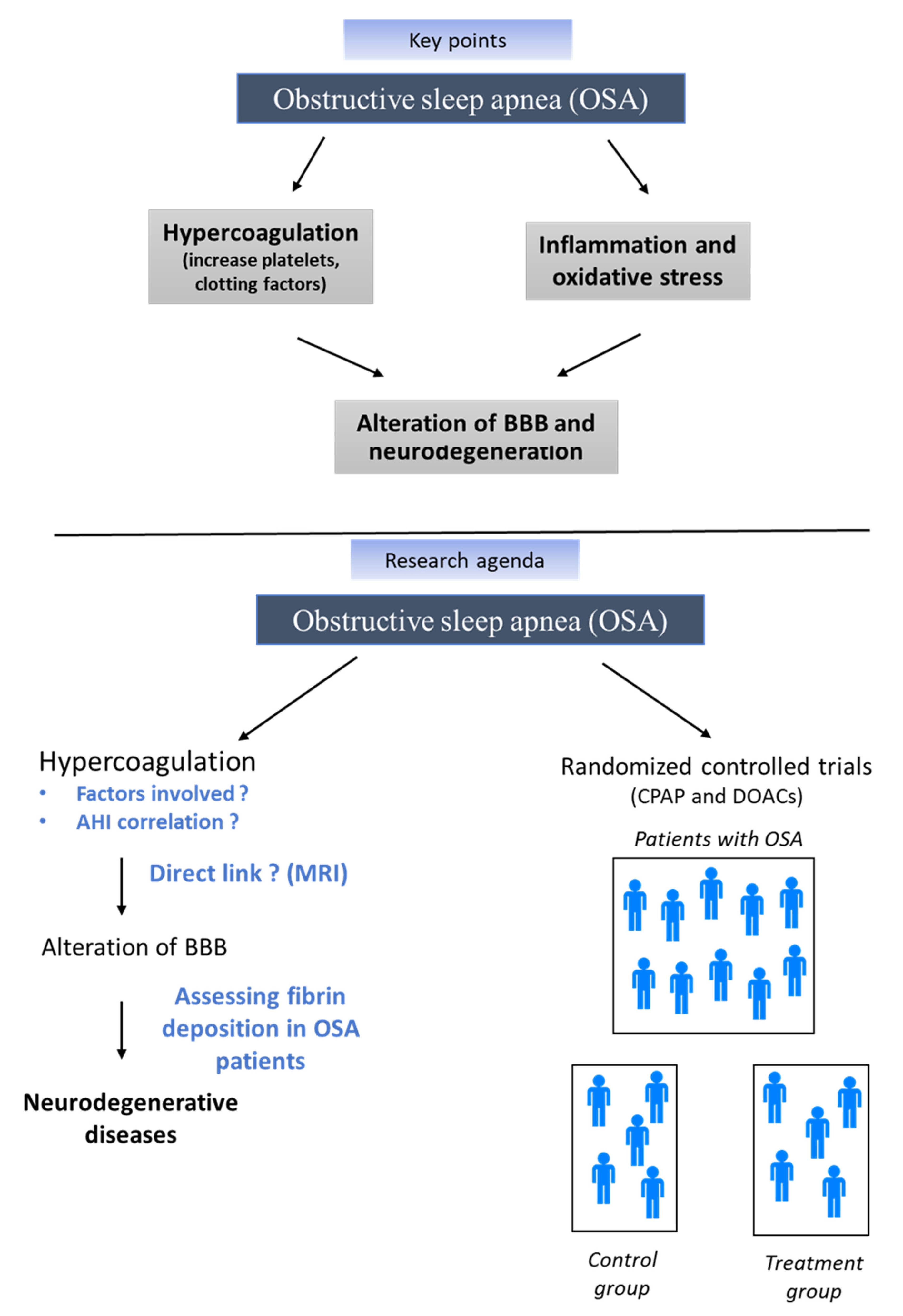
6. Conclusions
Funding
Conflicts of Interest
References
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of Obstructive Sleep Apnea in the General Population: A Systematic Review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef]
- Bonsignore, M.R.; Baiamonte, P.; Mazzuca, E.; Castrogiovanni, A.; Marrone, O. Obstructive Sleep Apnea and Comorbidities: A Dangerous Liaison. Multidiscip. Respir. Med. 2019, 14, 8. [Google Scholar] [CrossRef] [PubMed]
- Bahia, C.M.C.D.S.; Pereira, J.S. Obstructive Sleep Apnea and Neurodegenerative Diseases: A Bidirectional Relation. Dement. Neuropsychol. 2015, 9, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Lajoie, A.C.; Lafontaine, A.-L.; Kimoff, R.J.; Kaminska, M. Obstructive Sleep Apnea in Neurodegenerative Disorders: Current Evidence in Support of Benefit from Sleep Apnea Treatment. J. Clin. Med. 2020, 9, 297. [Google Scholar] [CrossRef] [PubMed]
- Cardiovascular Diseases. Available online: https://www.who.int/westernpacific/health-topics/cardiovascular-diseases (accessed on 26 April 2020).
- Obermayer, G.; Afonyushkin, T.; Binder, C.J. Oxidized Low-Density Lipoprotein in Inflammation-Driven Thrombosis. J. Thromb. Haemost. 2018, 16, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Blokhin, I.O.; Lentz, S.R. Mechanisms of Thrombosis in Obesity. Curr. Opin. Hematol. 2013, 20, 437–444. [Google Scholar] [CrossRef]
- Punjabi, N.M.; Caffo, B.S.; Goodwin, J.L.; Gottlieb, D.J.; Newman, A.B.; O’Connor, G.T.; Rapoport, D.M.; Redline, S.; Resnick, H.E.; Robbins, J.A.; et al. Sleep-Disordered Breathing and Mortality: A Prospective Cohort Study. PLoS Med. 2009, 6, e1000132. [Google Scholar] [CrossRef] [PubMed]
- Toraldo, D.M.; Peverini, F.; De Benedetto, M.; De Nuccio, F. Obstructive Sleep Apnea Syndrome: Blood Viscosity, Blood Coagulation Abnormalities, and Early Atherosclerosis. Lung 2013, 191, 1–7. [Google Scholar] [CrossRef]
- Festoff, B.W.; Sajja, R.K.; van Dreden, P.; Cucullo, L. HMGB1 and Thrombin Mediate the Blood-Brain Barrier Dysfunction Acting as Biomarkers of Neuroinflammation and Progression to Neurodegeneration in Alzheimer’s Disease. J. Neuroinflamm. 2016, 13, 194. [Google Scholar] [CrossRef]
- Zhu, X.; Cao, Y.; Wei, L.; Cai, P.; Xu, H.; Luo, H.; Bai, X.; Lu, L.; Liu, J.-R.; Fan, W.; et al. Von Willebrand Factor Contributes to Poor Outcome in a Mouse Model of Intracerebral Haemorrhage. Sci. Rep. 2016, 6, 35901. [Google Scholar] [CrossRef]
- Petersen, M.A.; Ryu, J.K.; Akassoglou, K. Fibrinogen in Neurological Diseases: Mechanisms, Imaging and Therapeutics. Nat. Rev. Neurosci. 2018, 19, 283–301. [Google Scholar] [CrossRef]
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.-L.; et al. Estimation of the Global Prevalence and Burden of Obstructive Sleep Apnoea: A Literature-Based Analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef]
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G.; et al. Prevalence of Sleep-Disordered Breathing in the General Population: The HypnoLaus Study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef]
- Martin, M.S.; Sforza, E.; Roche, F.; Barthélémy, J.C.; Thomas-Anterion, C. PROOF study group Sleep Breathing Disorders and Cognitive Function in the Elderly: An 8-Year Follow-up Study. The Proof-Synapse Cohort. Sleep 2015, 38, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Sforza, E.; Saint Martin, M.; Barthélémy, J.C.; Roche, F. Mood Disorders in Healthy Elderly with Obstructive Sleep Apnea: A Gender Effect. Sleep Med. 2016, 19, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Gabryelska, A.; Łukasik, Z.M.; Makowska, J.S.; Białasiewicz, P. Obstructive Sleep Apnea: From Intermittent Hypoxia to Cardiovascular Complications via Blood Platelets. Front. Neurol. 2018, 9, 635. [Google Scholar] [CrossRef] [PubMed]
- Gabryelska, A.; Szmyd, B.; Panek, M.; Szemraj, J.; Kuna, P.; Białasiewicz, P. Serum Hypoxia-Inducible Factor-1α Protein Level as a Diagnostic Marker of Obstructive Sleep Apnea. Pol. Arch. Intern. Med. 2020, 130, 158–160. [Google Scholar] [CrossRef] [PubMed]
- Rius, J.; Guma, M.; Schachtrup, C.; Akassoglou, K.; Zinkernagel, A.S.; Nizet, V.; Johnson, R.S.; Haddad, G.G.; Karin, M. NF-KappaB Links Innate Immunity to the Hypoxic Response through Transcriptional Regulation of HIF-1alpha. Nature 2008, 453, 807–811. [Google Scholar] [CrossRef]
- Pratt-Ubunama, M.N.; Nishizaka, M.K.; Boedefeld, R.L.; Cofield, S.S.; Harding, S.M.; Calhoun, D.A. Plasma Aldosterone Is Related to Severity of Obstructive Sleep Apnea in Subjects with Resistant Hypertension. Chest 2007, 131, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Sforza, E.; Roche, F.; Chapelle, C.; Pichot, V. Internight Variability of Apnea-Hypopnea Index in Obstructive Sleep Apnea Using Ambulatory Polysomnography. Front. Physiol. 2019, 10, 849. [Google Scholar] [CrossRef]
- Yu, J.; Zhou, Z.; McEvoy, R.D.; Anderson, C.S.; Rodgers, A.; Perkovic, V.; Neal, B. Association of Positive Airway Pressure With Cardiovascular Events and Death in Adults With Sleep Apnea: A Systematic Review and Meta-Analysis. JAMA 2017, 318, 156–166. [Google Scholar] [CrossRef]
- Labarca, G.; Dreyse, J.; Drake, L.; Jorquera, J.; Barbe, F. Efficacy of Continuous Positive Airway Pressure (CPAP) in the Prevention of Cardiovascular Events in Patients with Obstructive Sleep Apnea: Systematic Review and Meta-Analysis. Sleep Med. Rev. 2020, 52, 101312. [Google Scholar] [CrossRef] [PubMed]
- Khot, S.P.; Davis, A.P.; Crane, D.A.; Tanzi, P.M.; Li Lue, D.; Claflin, E.S.; Becker, K.J.; Longstreth, W.T.; Watson, N.F.; Billings, M.E. Effect of Continuous Positive Airway Pressure on Stroke Rehabilitation: A Pilot Randomized Sham-Controlled Trial. J. Clin. Sleep Med. 2016, 12, 1019–1026. [Google Scholar] [CrossRef]
- Ramar, K.; Dort, L.C.; Katz, S.G.; Lettieri, C.J.; Harrod, C.G.; Thomas, S.M.; Chervin, R.D. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015. J. Clin. Sleep Med. 2015, 11, 773–827. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, B.; Hsia, J.; Capasso, R. Surgical Therapy of Obstructive Sleep Apnea: A Review. Neurotherapeutics 2012, 9, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Sedlák, V.; Kudela, O.; Kopecký, M.; Svarc, M.; Smolík, P.; Havel, V. Factors Influencing Efficacy of BiPAP Therapy in Severe Obstructive Sleep Apnea. Eur. Respir. J. 2013, 42, P4040. [Google Scholar]
- Kim, L.J.; Freire, C.; Fleury Curado, T.; Jun, J.C.; Polotsky, V.Y. The Role of Animal Models in Developing Pharmacotherapy for Obstructive Sleep Apnea. J. Clin. Med. 2019, 8, 49. [Google Scholar] [CrossRef]
- Paterson, G.G.; Young, J.M.; Willson, J.A.; Graham, C.J.; Dru, R.C.; Lee, E.W.; Torpey, G.S.; Walmsley, S.R.; Chan, M.V.; Warner, T.D.; et al. Hypoxia Modulates Platelet Purinergic Signalling Pathways. Thromb. Haemost. 2020, 120, 253–261. [Google Scholar] [CrossRef]
- Maclay, J.D.; McAllister, D.A.; Johnston, S.; Raftis, J.; McGuinnes, C.; Deans, A.; Newby, D.E.; Mills, N.L.; MacNee, W. Increased Platelet Activation in Patients with Stable and Acute Exacerbation of COPD. Thorax 2011, 66, 769–774. [Google Scholar] [CrossRef]
- Sabit, R.; Thomas, P.; Shale, D.J.; Collins, P.; Linnane, S.J. The Effects of Hypoxia on Markers of Coagulation and Systemic Inflammation in Patients with COPD. Chest 2010, 138, 47–51. [Google Scholar] [CrossRef]
- Jankowski, M.; Undas, A.; Kaczmarek, P.; Butenas, S. Activated Factor XI and Tissue Factor in Chronic Obstructive Pulmonary Disease: Links with Inflammation and Thrombin Generation. Thromb. Res. 2011, 127, 242–246. [Google Scholar] [CrossRef]
- Popovic, B.; Zannad, F.; Louis, H.; Clerc-Urmès, I.; Lakomy, C.; Gibot, S.; Denis, C.V.; Lacolley, P.; Regnault, V. Endothelial-Driven Increase in Plasma Thrombin Generation Characterising a New Hypercoagulable Phenotype in Acute Heart Failure. Int. J. Cardiol. 2019, 274, 195–201. [Google Scholar] [CrossRef]
- Fan, Z.; Lu, X.; Long, H.; Li, T.; Zhang, Y. The Association of Hemocyte Profile and Obstructive Sleep Apnea. J. Clin. Lab. Anal. 2019, 33, e22680. [Google Scholar] [CrossRef]
- Reinhart, W.H.; Oswald, J.; Walter, R.; Kuhn, M. Blood Viscosity and Platelet Function in Patients with Obstructive Sleep Apnea Syndrome Treated with Nasal Continuous Positive Airway Pressure. Clin. Hemorheol. Microcirc. 2002, 27, 201–207. [Google Scholar]
- Dikmenoğlu, N.; Çiftçi, B.; İleri, E.; Güven, S.F.; Seringeç, N.; Aksoy, Y.; Ercil, D. Erythrocyte Deformability, Plasma Viscosity and Oxidative Status in Patients with Severe Obstructive Sleep Apnea Syndrome. Sleep Med. 2006, 7, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Tazbirek, M.; Slowinska, L.; Skoczynski, S.; Pierzchala, W. Short-Term Continuous Positive Airway Pressure Therapy Reverses the Pathological Influence of Obstructive Sleep Apnea on Blood Rheology Parameters. Clin. Hemorheol. Microcirc. 2009, 41, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Robinson, G.V.; Pepperell, J.C.T.; Segal, H.C.; Davies, R.J.O.; Stradling, J.R. Circulating Cardiovascular Risk Factors in Obstructive Sleep Apnoea: Data from Randomised Controlled Trials. Thorax 2004, 59, 777–782. [Google Scholar] [CrossRef] [PubMed]
- von Känel, R.; Loredo, J.S.; Powell, F.L.; Adler, K.A.; Dimsdale, J.E. Short-Term Isocapnic Hypoxia and Coagulation Activation in Patients with Sleep Apnea. Clin. Hemorheol. Microcirc. 2005, 33, 369–377. [Google Scholar]
- Olson, N.C.; Raffield, L.M.; Lange, L.A.; Lange, E.M.; Longstreth, W.T.; Chauhan, G.; Debette, S.; Seshadri, S.; Reiner, A.P.; Tracy, R.P. Associations of Activated Coagulation Factor VII and Factor VIIa-Antithrombin Levels with Genome-Wide Polymorphisms and Cardiovascular Disease Risk. J. Thromb. Haemost. 2018, 16, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Nickel Katrin, F.; Long Andy, T.; Fuchs Tobias, A.; Butler Lynn, M. Renné Thomas Factor XII as a Therapeutic Target in Thromboembolic and Inflammatory Diseases. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 13–20. [Google Scholar] [CrossRef]
- Johansson, K.; Jansson, J.-H.; Johansson, L.; Bylesjö, I.; Nilsson, T.K.; Eliasson, M.; Söderberg, S.; Lind, M. Factor XII as a Risk Marker for Hemorrhagic Stroke: A Prospective Cohort Study. Cerebrovasc. Dis. Extra 2017, 7, 84–94. [Google Scholar] [CrossRef]
- Chin, K.; Kita, H.; Noguchi, T.; Otsuka, N.; Tsuboi, T.; Nakamura, T.; Shimizu, K.; Mishima, M.; Ohi, M. Improvement of Factor VII Clotting Activity Following Long-Term NCPAP Treatment in Obstructive Sleep Apnoea Syndrome. QJM 1998, 91, 627–633. [Google Scholar] [CrossRef][Green Version]
- Folsom, A.R.; Lutsey, P.L.; Astor, B.C.; Cushman, M. C-Reactive Protein and Venous Thromboembolism. A Prospective Investigation in the ARIC Cohort. Thromb. Haemost. 2009, 102, 615–619. [Google Scholar] [CrossRef]
- Stec James, J.; Silbershatz, H.; Tofler Geoffrey, H.; Matheney Travis, H.; Sutherland, P.; Lipinska, I.; Massaro Joseph, M.; Wilson Peter, F.W.; Muller James, E.; D’Agostino Ralph, B. Association of Fibrinogen With Cardiovascular Risk Factors and Cardiovascular Disease in the Framingham Offspring Population. Circulation 2000, 102, 1634–1638. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Yin, K.; Wang, H.; Su, M.; Yang, Y. Effect of Continuous Positive Airway Pressure Treatment on Elderly Chinese Patients with Obstructive Sleep Apnea in the Prethrombotic State. Chin. Med. J. 2003, 116, 1426–1428. [Google Scholar] [PubMed]
- Nobili, L.; Schiavi, G.; Bozano, E.; De Carli, F.; Ferrillo, F.; Nobili, F. Morning Increase of Whole Blood Viscosity in Obstructive Sleep Apnea Syndrome. Clin. Hemorheol. Microcirc. 2000, 22, 21–27. [Google Scholar] [PubMed]
- Comondore, V.R.; Cheema, R.; Fox, J.; Butt, A.; John Mancini, G.B.; Fleetham, J.A.; Ryan, C.F.; Chan, S.; Ayas, N.T. The Impact of CPAP on Cardiovascular Biomarkers in Minimally Symptomatic Patients with Obstructive Sleep Apnea: A Pilot Feasibility Randomized Crossover Trial. Lung 2009, 187, 17–22. [Google Scholar] [CrossRef]
- von Känel, R.; Malan, N.T.; Hamer, M.; Lambert, G.W.; Schlaich, M.; Reimann, M.; Malan, L. Three-Year Changes of Prothrombotic Factors in a Cohort of South Africans with a High Clinical Suspicion of Obstructive Sleep Apnea. Thromb. Haemost. 2016, 115, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Hizli, O.; Cayir, S.; Coluk, Y.; Kayabasi, S.; Yildirim, G. The Novel Indicators of Moderate to Severe Sleep Apnea: Fibrinogen to Albumin Ratio vs. CRP to Albumin Ratio. Eur. Arch. Otorhinolaryngol. 2020. [Google Scholar] [CrossRef]
- Mehra, R.; Xu, F.; Babineau, D.C.; Tracy, R.P.; Jenny, N.S.; Patel, S.R.; Redline, S. Sleep-Disordered Breathing and Prothrombotic Biomarkers. Am. J. Respir. Crit. Care Med. 2010, 182, 826–833. [Google Scholar] [CrossRef]
- Steiner, S.; Jax, T.; Evers, S.; Hennersdorf, M.; Schwalen, A.; Strauer, B.E. Altered Blood Rheology in Obstructive Sleep Apnea as a Mediator of Cardiovascular Risk. Cardiology 2005, 104, 92–96. [Google Scholar] [CrossRef]
- Wessendorf, T.E.; Thilmann, A.F.; Wang, Y.M.; Schreiber, A.; Konietzko, N.; Teschler, H. Fibrinogen Levels and Obstructive Sleep Apnea in Ischemic Stroke. Am. J. Respir. Crit. Care Med. 2000, 162, 2039–2042. [Google Scholar] [CrossRef]
- Shamsuzzaman, A.; Amin, R.S.; Calvin, A.D.; Davison, D.; Somers, V.K. Severity of Obstructive Sleep Apnea Is Associated with Elevated Plasma Fibrinogen in Otherwise Healthy Patients. Sleep Breath. 2014, 18, 761–766. [Google Scholar] [CrossRef]
- Bouloukaki, I.; Mermigkis, C.; Tzanakis, N.; Kallergis, E.; Moniaki, V.; Mauroudi, E.; Schiza, S.E. Evaluation of Inflammatory Markers in a Large Sample of Obstructive Sleep Apnea Patients without Comorbidities. Mediat. Inflamm. 2017, 2017, 4573756. [Google Scholar] [CrossRef]
- Geiser, T.; Buck, F.; Meyer, B.J.; Bassetti, C.; Haeberli, A.; Gugger, M. In Vivo Platelet Activation Is Increased during Sleep in Patients with Obstructive Sleep Apnea Syndrome. Respiration 2002, 69, 229–234. [Google Scholar] [CrossRef]
- Bokinsky, G.; Miller, M.; Ault, K.; Husband, P.; Mitchell, J. Spontaneous Platelet Activation and Aggregation during Obstructive Sleep Apnea and Its Response to Therapy with Nasal Continuous Positive Airway Pressure. A Preliminary Investigation. Chest 1995, 108, 625–630. [Google Scholar] [CrossRef]
- von Känel, R.; Dimsdale, J.E. Hemostatic Alterations in Patients with Obstructive Sleep Apnea and the Implications for Cardiovascular Disease. Chest 2003, 124, 1956–1967. [Google Scholar] [CrossRef]
- Akinnusi, M.E.; Paasch, L.L.; Szarpa, K.R.; Wallace, P.K.; El Solh, A.A. Impact of Nasal Continuous Positive Airway Pressure Therapy on Markers of Platelet Activation in Patients with Obstructive Sleep Apnea. Respiration 2009, 77, 25–31. [Google Scholar] [CrossRef]
- Kosacka, M.; Brzecka, A.; Piesiak, P.; Korzeniewska, A.; Jankowska, R. Soluble Ligand CD40 and Uric Acid as Markers of Atheromatosis in Patients with Obstructive Sleep Apnea. Adv. Exp. Med. Biol. 2015, 839, 55–60. [Google Scholar] [CrossRef]
- Kobayashi, K.; Nishimura, Y.; Shimada, T.; Yoshimura, S.; Funada, Y.; Satouchi, M.; Yokoyama, M. Effect of Continuous Positive Airway Pressure on Soluble CD40 Ligand in Patients with Obstructive Sleep Apnea Syndrome. Chest 2006, 129, 632–637. [Google Scholar] [CrossRef]
- Cofta, S.; Wysocka, E.; Dziegielewska-Gesiak, S.; Michalak, S.; Piorunek, T.; Batura-Gabryel, H.; Torlinski, L. Plasma Selectins in Patients with Obstructive Sleep Apnea. Adv. Exp. Med. Biol. 2013, 756, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, M.; Kamio, K.; Haida, M.; Ono, Y.; Miyachi, H.; Yamamoto, M.; Shinohara, Y.; Ando, Y. Platelet Activation in Patients with Obstructive Sleep Apnea Syndrome and Effects of Nasal-Continuous Positive Airway Pressure. Tokai. J. Exp. Clin. Med. 2002, 27, 107–112. [Google Scholar] [PubMed]
- Horváth, P.; Lázár, Z.; Gálffy, G.; Puskás, R.; Kunos, L.; Losonczy, G.; Mészáros, M.; Tárnoki, Á.D.; Tárnoki, D.L.; Bikov, A. Circulating P-Selectin Glycoprotein Ligand 1 and P-Selectin Levels in Obstructive Sleep Apnea Patients. Lung 2020, 198, 173–179. [Google Scholar] [CrossRef]
- Winiarska, H.M.; Cofta, S.; Bielawska, L.; Płóciniczak, A.; Piorunek, T.; Wysocka, E. Circulating P-Selectin and Its Glycoprotein Ligand in Nondiabetic Obstructive Sleep Apnea Patients. Adv. Exp. Med. Biol. 2020. [Google Scholar] [CrossRef]
- Sanner, B.M.; Konermann, M.; Tepel, M.; Groetz, J.; Mummenhoff, C.; Zidek, W. Platelet Function in Patients with Obstructive Sleep Apnoea Syndrome. Eur. Respir. J. 2000, 16, 648–652. [Google Scholar] [CrossRef]
- Oga, T.; Chin, K.; Tabuchi, A.; Kawato, M.; Morimoto, T.; Takahashi, K.; Handa, T.; Takahashi, K.; Taniguchi, R.; Kondo, H.; et al. Effects of Obstructive Sleep Apnea with Intermittent Hypoxia on Platelet Aggregability. J. Atheroscler. Thromb. 2009, 16, 862–869. [Google Scholar] [CrossRef]
- Kontos, A.; Willoughby, S.; Lushington, K.; Martin, J.; Wabnitz, D.; Dorrian, J.; Kennedy, D. Increased Platelet Aggregation in Children and Adolescents with Sleep-Disordered Breathing. Am. J. Respir. Crit. Care Med. 2020, 202, 1560–1566. [Google Scholar] [CrossRef]
- Alkhiary, W.; Morsy, N.E.; Yousef, A.M.; El-Saddik, A.M.; Arram, E.O. Adenosine Diphosphate-Induced Platelets Aggregability in Polysomnographically Verified Obstructive Sleep Apnea. Clin. Appl. Thromb. Hemost. 2017, 23, 360–366. [Google Scholar] [CrossRef]
- Deng, Y.; Fang, W.; Li, Y.; Cen, J.; Fang, F.; Lv, P.; Gong, S.; Mao, L. Blood-Brain Barrier Breakdown by PAF and Protection by XQ-1H Due to Antagonism of PAF Effects. Eur. J. Pharmacol. 2009, 616, 43–47. [Google Scholar] [CrossRef]
- Row, B.W.; Kheirandish, L.; Li, R.C.; Guo, S.Z.; Brittian, K.R.; Hardy, M.; Bazan, N.G.; Gozal, D. Platelet-Activating Factor Receptor-Deficient Mice Are Protected from Experimental Sleep Apnea-Induced Learning Deficits. J. Neurochem. 2004, 89, 189–196. [Google Scholar] [CrossRef]
- Liak, C.; Fitzpatrick, M. Coagulability in Obstructive Sleep Apnea. Can. Respir. J. 2011, 18, 338–348. [Google Scholar] [CrossRef]
- Reininger, A.J. Function of von Willebrand Factor in Haemostasis and Thrombosis. Haemophilia 2008, 14, 11–26. [Google Scholar] [CrossRef]
- von Känel, R.; Loredo, J.S.; Ancoli-Israel, S.; Dimsdale, J.E. Association between Sleep Apnea Severity and Blood Coagulability: Treatment Effects of Nasal Continuous Positive Airway Pressure. Sleep Breath. 2006, 10, 139–146. [Google Scholar] [CrossRef] [PubMed]
- von Känel, R.; Loredo, J.S.; Ancoli-Israel, S.; Mills, P.J.; Natarajan, L.; Dimsdale, J.E. Association between Polysomnographic Measures of Disrupted Sleep and Prothrombotic Factors. Chest 2007, 131, 733–739. [Google Scholar] [CrossRef] [PubMed]
- El Solh, A.A.; Akinnusi, M.E.; Berim, I.G.; Peter, A.M.; Paasch, L.L.; Szarpa, K.R. Hemostatic Implications of Endothelial Cell Apoptosis in Obstructive Sleep Apnea. Sleep Breath. 2008, 12, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Phillips, C.L.; McEwen, B.J.; Morel-Kopp, M.-C.; Yee, B.J.; Sullivan, D.R.; Ward, C.M.; Tofler, G.H.; Grunstein, R.R. Effects of Continuous Positive Airway Pressure on Coagulability in Obstructive Sleep Apnoea: A Randomised, Placebo-Controlled Crossover Study. Thorax 2012, 67, 639–644. [Google Scholar] [CrossRef]
- Lim, D.C.; Pack, A.I. Obstructive Sleep Apnea and Cognitive Impairment: Addressing the Blood–Brain Barrier. Sleep Med. Rev. 2014, 18, 35–48. [Google Scholar] [CrossRef]
- Khalyfa, A.; Gozal, D.; Kheirandish-Gozal, L. Plasma Exosomes Disrupt the Blood–Brain Barrier in Children with Obstructive Sleep Apnea and Neurocognitive Deficits. Am. J. Respir. Crit. Care Med. 2018, 197, 1073–1076. [Google Scholar] [CrossRef]
- Voirin, A.-C.; Celle, S.; Perek, N.; Roche, F. Sera of Elderly Obstructive Sleep Apnea Patients Alter Blood–Brain Barrier Integrity in Vitro: A Pilot Study. Sci. Rep. 2020, 10, 11309. [Google Scholar] [CrossRef]
- Daneman, R.; Prat, A. The Blood–Brain Barrier. Cold Spring Harb. Perspect. Biol. 2015, 7. [Google Scholar] [CrossRef]
- Mahringer, A.; Fricker, G. ABC Transporters at the Blood–Brain Barrier. Expert Opin. Drug Metab. Toxicol. 2016, 12, 499–508. [Google Scholar] [CrossRef]
- Daneman, R. The Blood-Brain Barrier in Health and Disease. Ann. Neurol. 2012, 72, 648–672. [Google Scholar] [CrossRef]
- Zhou, L.; Chen, P.; Peng, Y.; Ouyang, R. Role of Oxidative Stress in the Neurocognitive Dysfunction of Obstructive Sleep Apnea Syndrome. Oxid. Med. Cell. Longev. 2016, 2016, 9626831. [Google Scholar] [CrossRef] [PubMed]
- Gozal, D.; Gileles-Hillel, A.; Cortese, R.; Li, Y.; Almendros, I.; Qiao, Z.; Khalyfa, A.A.; Andrade, J.; Khalyfa, A. Visceral White Adipose Tissue after Chronic Intermittent and Sustained Hypoxia in Mice. Am. J. Respir. Cell Mol. Biol. 2017, 56, 477–487. [Google Scholar] [CrossRef]
- Israel, L.P.; Benharoch, D.; Gopas, J.; Goldbart, A.D. A Pro-Inflammatory Role for Nuclear Factor Kappa B in Childhood Obstructive Sleep Apnea Syndrome. Sleep 2013, 36, 1947–1955. [Google Scholar] [CrossRef]
- Nadeem, R.; Molnar, J.; Madbouly, E.M.; Nida, M.; Aggarwal, S.; Sajid, H.; Naseem, J.; Loomba, R. Serum Inflammatory Markers in Obstructive Sleep Apnea: A Meta-Analysis. J. Clin. Sleep Med. 2013, 9, 1003–1012. [Google Scholar] [CrossRef]
- Kheirandish-Gozal, L.; Gozal, D. Obstructive Sleep Apnea and Inflammation: Proof of Concept Based on Two Illustrative Cytokines. Int. J. Mol. Sci. 2019, 20, 459. [Google Scholar] [CrossRef]
- Kim, L.J.; Martinez, D.; Fiori, C.Z.; Baronio, D.; Kretzmann, N.A.; Barros, H.M.T. Hypomyelination, Memory Impairment, and Blood-Brain Barrier Permeability in a Model of Sleep Apnea. Brain Res. 2015, 1597, 28–36. [Google Scholar] [CrossRef]
- Kilicarslan, R.; Alkan, A.; Sharifov, R.; Akkoyunlu, M.E.; Aralasmak, A.; Kocer, A.; Kart, L. The Effect of Obesity on Brain Diffusion Alteration in Patients with Obstructive Sleep Apnea. Sci. World J. 2014, 2014, 768415. [Google Scholar] [CrossRef]
- György, B.; Szabó, T.G.; Pásztói, M.; Pál, Z.; Misják, P.; Aradi, B.; László, V.; Pállinger, É.; Pap, E.; Kittel, Á.; et al. Membrane Vesicles, Current State-of-the-Art: Emerging Role of Extracellular Vesicles. Cell Mol. Life Sci. 2011, 68, 2667–2688. [Google Scholar] [CrossRef]
- Wood, M.J.A.; O’Loughlin, A.J.; Samira, L. Exosomes and the Blood-Brain Barrier: Implications for Neurological Diseases. Ther. Deliv. 2011, 2, 1095–1099. [Google Scholar] [CrossRef]
- Khalyfa, A.; Gozal, D.; Kheirandish-Gozal, L. Plasma Extracellular Vesicles in Children with OSA Disrupt Blood-Brain Barrier Integrity and Endothelial Cell Wound Healing in Vitro. Int. J. Mol. Sci. 2019, 20, 6233. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.-Z.; Ander, B.P.; Xu, H.; Shen, Y.; Kaur, P.; Deng, W.; Sharp, F.R. Blood-Brain Barrier Breakdown and Repair by Src after Thrombin-Induced Injury. Ann. Neurol. 2010, 67, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Kawakita, K.; Kawai, N.; Kuroda, Y.; Yasashita, S.; Nagao, S. Expression of Matrix Metalloproteinse-9 in Thrombin-Induced Brain Edema Formation in Rats. J. Stroke Cerebrovasc. Dis. 2006, 15, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Suidan, G.L.; Brill, A.; De Meyer, S.F.; Voorhees, J.R.; Cifuni, S.M.; Cabral, J.E.; Wagner, D.D. Endothelial Von Willebrand Factor Promotes Blood-Brain Barrier Flexibility and Provides Protection from Hypoxia and Seizures in Mice. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 2112–2120. [Google Scholar] [CrossRef] [PubMed]
- Kisucka, J.; Chauhan, A.K.; Zhao, B.-Q.; Patten, I.S.; Yesilaltay, A.; Krieger, M.; Wagner, D.D. Elevated Levels of Soluble P-Selectin in Mice Alter Blood-Brain Barrier Function, Exacerbate Stroke, and Promote Atherosclerosis. Blood 2009, 113, 6015–6022. [Google Scholar] [CrossRef]
- Paul, J.; Strickland, S.; Melchor, J.P. Fibrin Deposition Accelerates Neurovascular Damage and Neuroinflammation in Mouse Models of Alzheimer’s Disease. J. Exp. Med. 2007, 204, 1999–2008. [Google Scholar] [CrossRef] [PubMed]
- Jin, A.Y.; Tuor, U.I.; Rushforth, D.; Kaur, J.; Muller, R.N.; Petterson, J.L.; Boutry, S.; Barber, P.A. Reduced Blood Brain Barrier Breakdown in P-Selectin Deficient Mice Following Transient Ischemic Stroke: A Future Therapeutic Target for Treatment of Stroke. BMC Neurosci. 2010, 11, 12. [Google Scholar] [CrossRef]
- Masuda, H.; Mori, M.; Umehara, K.; Furihata, T.; Uchida, T.; Uzawa, A.; Kuwabara, S. Soluble CD40 Ligand Disrupts the Blood–Brain Barrier and Exacerbates Inflammation in Experimental Autoimmune Encephalomyelitis. J. Neuroimmunol. 2018, 316, 117–120. [Google Scholar] [CrossRef]
- Davidson, D.C.; Hirschman, M.P.; Sun, A.; Singh, M.V.; Kasischke, K.; Maggirwar, S.B. Excess Soluble CD40L Contributes to Blood Brain Barrier Permeability in Vivo: Implications for HIV-Associated Neurocognitive Disorders. PLoS ONE 2012, 7, e51793. [Google Scholar] [CrossRef]
- Brailoiu, E.; Barlow, C.L.; Ramirez, S.H.; Abood, M.E.; Brailoiu, G.C. Effects of Platelet-Activating Factor on Brain Microvascular Endothelial Cells. Neuroscience 2018, 377, 105–113. [Google Scholar] [CrossRef]
- Fang, W.; Zhang, R.; Sha, L.; Lv, P.; Shang, E.; Han, D.; Wei, J.; Geng, X.; Yang, Q.; Li, Y. Platelet Activating Factor Induces Transient Blood-Brain Barrier Opening to Facilitate Edaravone Penetration into the Brain. J. Neurochem. 2014, 128, 662–671. [Google Scholar] [CrossRef]
- Abdel Salam, O.A.; Ghonimi, N.A.M.; Ismail, M.H. Risk of Obstructive Sleep Apnea in Multiple Sclerosis: Frequency, Clinical and Radiological Correlates. Mult. Scler. Relat. Disord. 2019, 28, 184–188. [Google Scholar] [CrossRef]
- Andrade, A.; Bubu, O.M.; Varga, A.W.; Osorio, R.S. The Relationship between Obstructive Sleep Apnea and Alzheimer’s Disease. J. Alzheimers Dis. 2018, 64, S255–S270. [Google Scholar] [CrossRef]
- Ryu, J.K.; McLarnon, J.G. A Leaky Blood–Brain Barrier, Fibrinogen Infiltration and Microglial Reactivity in Inflamed Alzheimer’s Disease Brain. J. Cell. Mol. Med. 2009, 13, 2911–2925. [Google Scholar] [CrossRef]
- Ryu, J.K.; Petersen, M.A.; Murray, S.G.; Baeten, K.M.; Meyer-Franke, A.; Chan, J.P.; Vagena, E.; Bedard, C.; Machado, M.R.; Rios Coronado, P.E.; et al. Blood Coagulation Protein Fibrinogen Promotes Autoimmunity and Demyelination via Chemokine Release and Antigen Presentation. Nat. Commun. 2015, 6, 8164. [Google Scholar] [CrossRef] [PubMed]
- Ziliotto, N.; Bernardi, F.; Jakimovski, D.; Zivadinov, R. Coagulation Pathways in Neurological Diseases: Multiple Sclerosis. Front. Neurol. 2019, 10, 409. [Google Scholar] [CrossRef]
- Merlini, M.; Akassoglou, K. Alzheimer Disease Makes New Blood Contacts. Blood 2017, 129, 2462–2463. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.-L.; Revenko, A.S.; Singh, P.; MacLeod, A.R.; Norris, E.H.; Strickland, S. Depletion of Coagulation Factor XII Ameliorates Brain Pathology and Cognitive Impairment in Alzheimer Disease Mice. Blood 2017, 129, 2547–2556. [Google Scholar] [CrossRef] [PubMed]
- Gong, W.; Wang, X.; Fan, J.; Nie, S.; Wei, Y. Impact of Obstructive Sleep Apnea on Platelet Function Profiles in Patients With Acute Coronary Syndrome Taking Dual Antiplatelet Therapy. J. Am. Heart Assoc. 2018, 7, e008808. [Google Scholar] [CrossRef]
- Latina, J.M.; Estes, N.A.M.; Garlitski, A.C. The Relationship between Obstructive Sleep Apnea and Atrial Fibrillation: A Complex Interplay. Pulm. Med. 2013, 2013, 621736. [Google Scholar] [CrossRef] [PubMed]
- Marti-Almor, J.; Marques, P.; Jesel, L.; Garcia, R.; Girolamo, E.D.; Locati, F.; Defaye, P.; Venables, P.; Dompnier, A.; Barcelo, A.; et al. Incidence of Sleep Apnea and Association with Atrial Fibrillation in an Unselected Pacemaker Population: Results of the Observational RESPIRE Study. Heart Rhythm. 2020, 17, 195–202. [Google Scholar] [CrossRef]
- Jehan, S.; Farag, M.; Zizi, F.; Pandi-Perumal, S.R.; Chung, A.; Truong, A.; Jean-Louis, G.; Tello, D.; McFarlane, S.I. Obstructive Sleep Apnea and Stroke. Sleep Med. Disord. 2018, 2, 120–125. [Google Scholar] [PubMed]
- García-Ortega, A.; Mañas, E.; López-Reyes, R.; Selma, M.J.; García-Sánchez, A.; Oscullo, G.; Jiménez, D.; Martínez-García, M.Á. Obstructive Sleep Apnoea and Venous Thromboembolism: Pathophysiological Links and Clinical Implications. Eur. Respir. J. 2019, 53, 1800893. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Fernández, A.; Suquia, A.G.; Peña, M.D.L.; Casitas, R.; Pierola, J.; Barceló, A.; Soriano, J.B.; Fernández-Capitán, C.; Martinez-Ceron, E.; Carrera, M.; et al. OSA is a Risk Factor for Recurrent VTE. Chest 2016, 150, 1291–1301. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.-M.; Qian, X.-S.; Gao, X.-F.; Ge, Z.; Tian, N.-L.; Kan, J.; Zhang, J.-J. Obstructive Sleep Apnea Affecting Platelet Reactivity in Patients Undergoing Percutaneous Coronary Intervention. Chin. Med. J. Engl. 2018, 131, 1023–1029. [Google Scholar] [CrossRef]
- Xie, J.; Wei, Y.-X.; Liu, S.; Zhang, W.; Zhang, X.-F.; Li, J. Obstructive Sleep Apnea Hypopnea Syndrome as a Reason for Active Management of Pulmonary Embolism. Chin. Med. J. Engl. 2015, 128, 2147–2153. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, B.T.; Gu, Y.-H.; Izawa, Y.; del Zoppo, G.J. Dabigatran Abrogates Brain Endothelial Cell Permeability in Response to Thrombin. J. Cereb. Blood Flow Metab. 2015, 35, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Ploen, R.; Sun, L.; Zhou, W.; Heitmeier, S.; Zorn, M.; Jenetzky, E.; Veltkamp, R. Rivaroxaban Does Not Increase Hemorrhage after Thrombolysis in Experimental Ischemic Stroke. J. Cereb. Blood Flow Metab. 2014, 34, 495–501. [Google Scholar] [CrossRef]
- Sun, L.; Zhou, W.; Ploen, R.; Zorn, M.; Veltkamp, R. Anticoagulation with Dabigatran Does Not Increase Secondary Intracerebral Haemorrhage after Thrombolysis in Experimental Cerebral Ischaemia. Thromb. Haemost. 2013, 110, 153–161. [Google Scholar] [CrossRef]
- Pétrault, M.; Ouk, T.; Pétrault, O.; Bastide, M.; Bordet, R.; Bérézowski, V. Safety of Oral Anticoagulants on Experimental Brain Microbleeding and Cognition. Neuropharmacology 2019, 155, 162–172. [Google Scholar] [CrossRef]
- Puech, C.; Delavenne, X.; He, Z.; Forest, V.; Mismetti, P.; Perek, N. Direct Oral Anticoagulants are Associated with Limited Damage of Endothelial Cells of the Blood-Brain Barrier Mediated by the Thrombin/PAR-1 Pathway. Brain Res. 2019, 1719, 57–63. [Google Scholar] [CrossRef]
- Sweeney, M.D.; Sagare, A.P.; Zlokovic, B.V. Blood-Brain Barrier Breakdown in Alzheimer Disease and Other Neurodegenerative Disorders. Nat. Rev. Neurol. 2018, 14, 133–150. [Google Scholar] [CrossRef] [PubMed]
- Cortes-Canteli, M.; Kruyer, A.; Fernandez-Nueda, I.; Marcos-Diaz, A.; Ceron, C.; Richards, A.T.; Jno-Charles, O.C.; Rodriguez, I.; Callejas, S.; Norris, E.H.; et al. Long-Term Dabigatran Treatment Delays Alzheimer’s Disease Pathogenesis in the TgCRND8 Mouse Model. J. Am. Coll. Cardiol. 2019, 74, 1910–1923. [Google Scholar] [CrossRef]
- Mukherjee, S.; Saxena, R.; Palmer, L.J. The Genetics of Obstructive Sleep Apnoea. Respirology 2018, 23, 18–27. [Google Scholar] [CrossRef]
- Roche, F.; Mouhli, L.; Pichot, V.; Celle, S. OSAHS Phenotypes after Night Sleep Recordings: How to Get to Precision Medicine in 2021. Sleep 2021, zsab154. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Increased Factors in Osa | Authors | Type of Study—Subjects | CPAP Used? (>4 hours/night) Effects |
|---|---|---|---|
| FVII and FXII | Chin, 1998 [43] | Nonrandomized, controlled trial—15 males with OSA | Yes, decreased FVII levels after six months of CPAP |
| Robinson, 2004 [38] | Randomized controlled trial—220 patients with OSA | Yes, no effects on FVII or FVIIa levels after one month CPAP | |
| Thrombin | Robinson, 2004 [38] | Randomized controlled trial—220 patients with OSA | Yes, no effects on thrombin levels after one month |
| Von Kanel, 2005 [39] | Uncontrolled intervention study—32 patients with OSA | No | |
| Fibrinogen | Bouloukaki, 2017 [55] | Cross-sectional study—858 patients with OSA | No |
| Chin, 1998 [43] | Uncontrolled intervention study—11 patients with OSA | Yes, decreased in fibrinogen levels after one night | |
| Comondore, 2009 [48] | Randomized crossover trial—13 patients with OSA | Yes, no effects in fibrinogen after 4 weeks CPAP | |
| Hizli, 2020 [50] | Randomized crossover trial—126 patients with OSA | No | |
| Mehra, 2010 [51] | Cross-sectional study—537 patients with OSA | No | |
| Nobili, 2000 [47] | Case-control study—12 patients with OSA | No | |
| Reinhart, 2002 [35] | Case-control study—13 patients with OSA | Yes, no effects in fibrinogen level after one night | |
| Shamsuzzaman, 2014 [54] | Case-control study—36 men with OSA | No | |
| Steiner, 2005 [52] | Case-control study—63 patients with OSA | No | |
| Von Kanel, 2016 [49] | Longitudinal study—329 patients with OSA | No | |
| Wessendorf, 2000 [53] | Case-control study—69 patients with OSA | No | |
| Zhang, 2003 [46] | Nonrandomized—41 patients with OSA | Yes, decreased in fibrinogen levels, after 30 days CPAP | |
| Platelet activation | Bokinsky, 1995 [57] | Non-randomized study—6 patients with OSA | Yes, no effects |
| Geiser, 2002 [56] | Case-control study—12 patients with OSA | No | |
| sCD40L | Akinnusi, 2009 [59] | Non-randomized study—12 patients with OSA | Yes, decreased in sCD40L after 8 weeks |
| Kobayashi, 2006 [61] | Case-control study—35 patients with OSA | Yes, decreased in sCD40L after 1 night | |
| Kosacka, 2015 [60] | Case-control study—79 OSA patients | No | |
| P-selectin | Cofta, 2013 [62] | Group comparaison study—80 patients with OSA | No |
| Horváth, 2020 [64] | Case-control study—51 patients with OSA | No | |
| Shimizu, 2002 [63] | Non-randomized study—94 patients with OSA | Yes, decreased in P-selectin after 1 month | |
| Winiarska, 2020 [65] | Group comparaison study—48 patients with OSA | No | |
| Platelet aggregation | Bokinsky, 1995 [57] | Non-randomized study—6 patients with OSA | Yes, no effects |
| Sanner, 2000 [66] | Non-randomized study—17 patients with OSA | Yes, decreased after 6 months | |
| Zhang, 2003 [46] | Non-randomized study—41 patients with OSA | Yes, decreased after 30 days | |
| Kontos, 2020 [68] | Non-randomized study—30 children with SDB | No | |
| ADP | Alkhiary, 2017 [69] | Case-control study—64 patients with OSA | No |
| Oga, 2009 [67] | Non-randomized study—58 patients with OSA | Yes, decreased in platelet aggregation | |
| VWF | El Solh, 2008 [76] | Non-randomized study—35 patients with OSA | No |
| Phillips, 2012 [77] | Randomized, placebo-controlled crossover study—28 patients | Yes, decreased in VWF level after 2 months | |
| Von Kanel, 2007 [75] | Cross-sectional study—135 patients | No | |
| Von Kanel, 2016 [49] | Longitudinal study—329 patients with OSA | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zolotoff, C.; Bertoletti, L.; Gozal, D.; Mismetti, V.; Flandrin, P.; Roche, F.; Perek, N. Obstructive Sleep Apnea, Hypercoagulability, and the Blood–Brain Barrier. J. Clin. Med. 2021, 10, 3099. https://doi.org/10.3390/jcm10143099
Zolotoff C, Bertoletti L, Gozal D, Mismetti V, Flandrin P, Roche F, Perek N. Obstructive Sleep Apnea, Hypercoagulability, and the Blood–Brain Barrier. Journal of Clinical Medicine. 2021; 10(14):3099. https://doi.org/10.3390/jcm10143099
Chicago/Turabian StyleZolotoff, Cindy, Laurent Bertoletti, David Gozal, Valentine Mismetti, Pascale Flandrin, Frédéric Roche, and Nathalie Perek. 2021. "Obstructive Sleep Apnea, Hypercoagulability, and the Blood–Brain Barrier" Journal of Clinical Medicine 10, no. 14: 3099. https://doi.org/10.3390/jcm10143099
APA StyleZolotoff, C., Bertoletti, L., Gozal, D., Mismetti, V., Flandrin, P., Roche, F., & Perek, N. (2021). Obstructive Sleep Apnea, Hypercoagulability, and the Blood–Brain Barrier. Journal of Clinical Medicine, 10(14), 3099. https://doi.org/10.3390/jcm10143099