
Ocular and Systemic Manifestations in Paediatric Multisystem Inflammatory Syndrome Associated with COVID-19


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Extraction of Variables
2.4. Statistical Analysis
3. Results
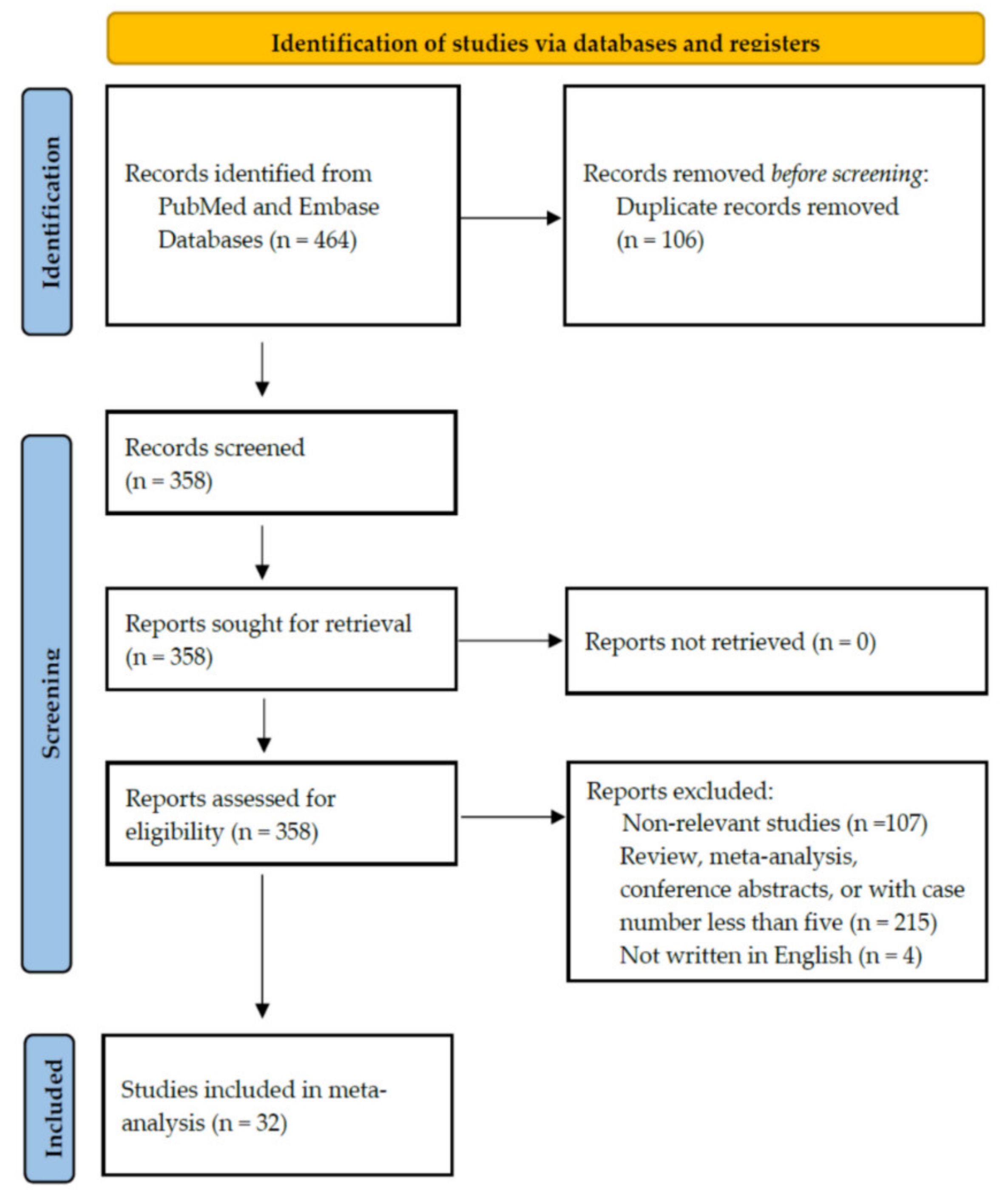
3.1. Search Results
3.2. Characteristics of Included Studies
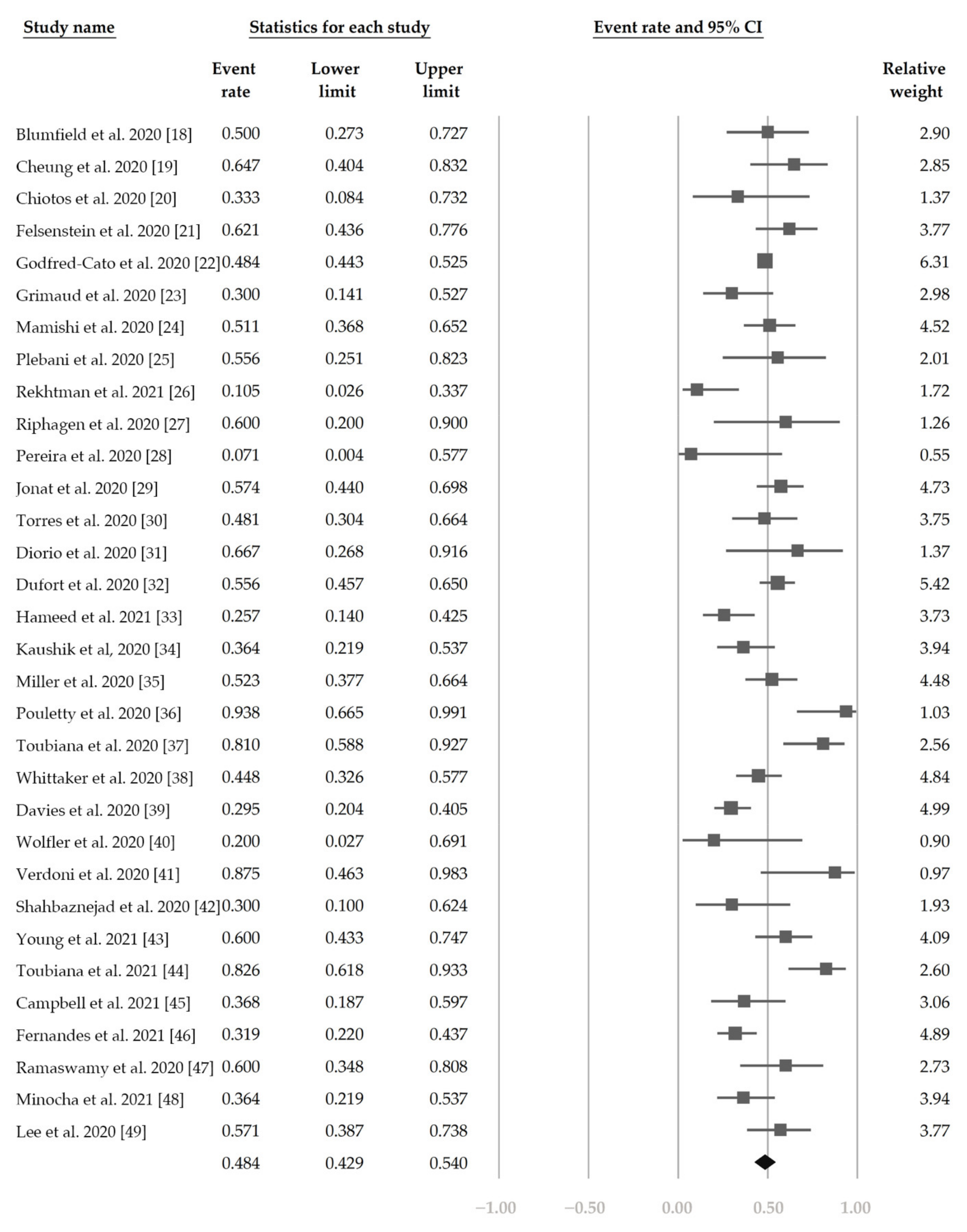
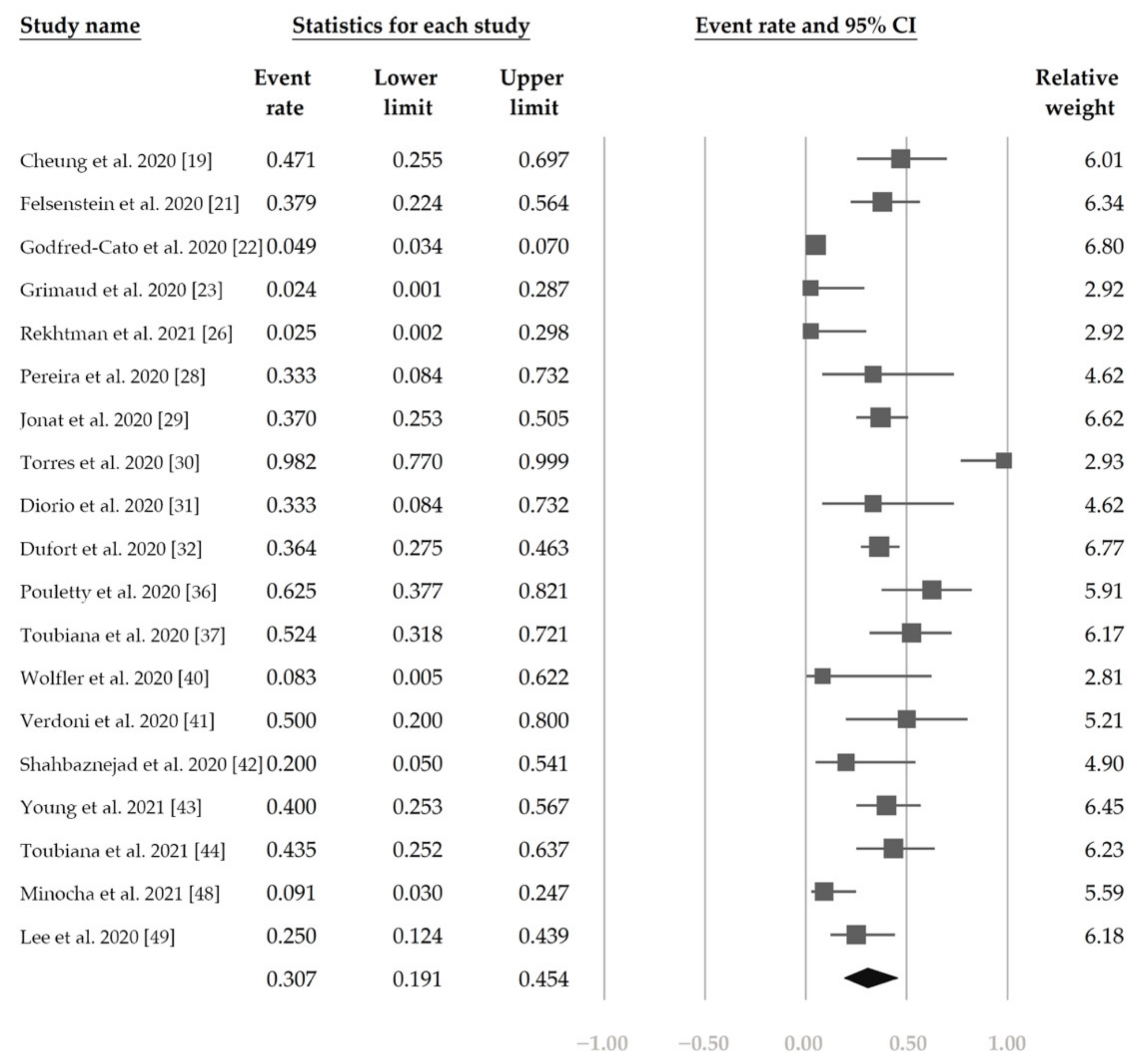
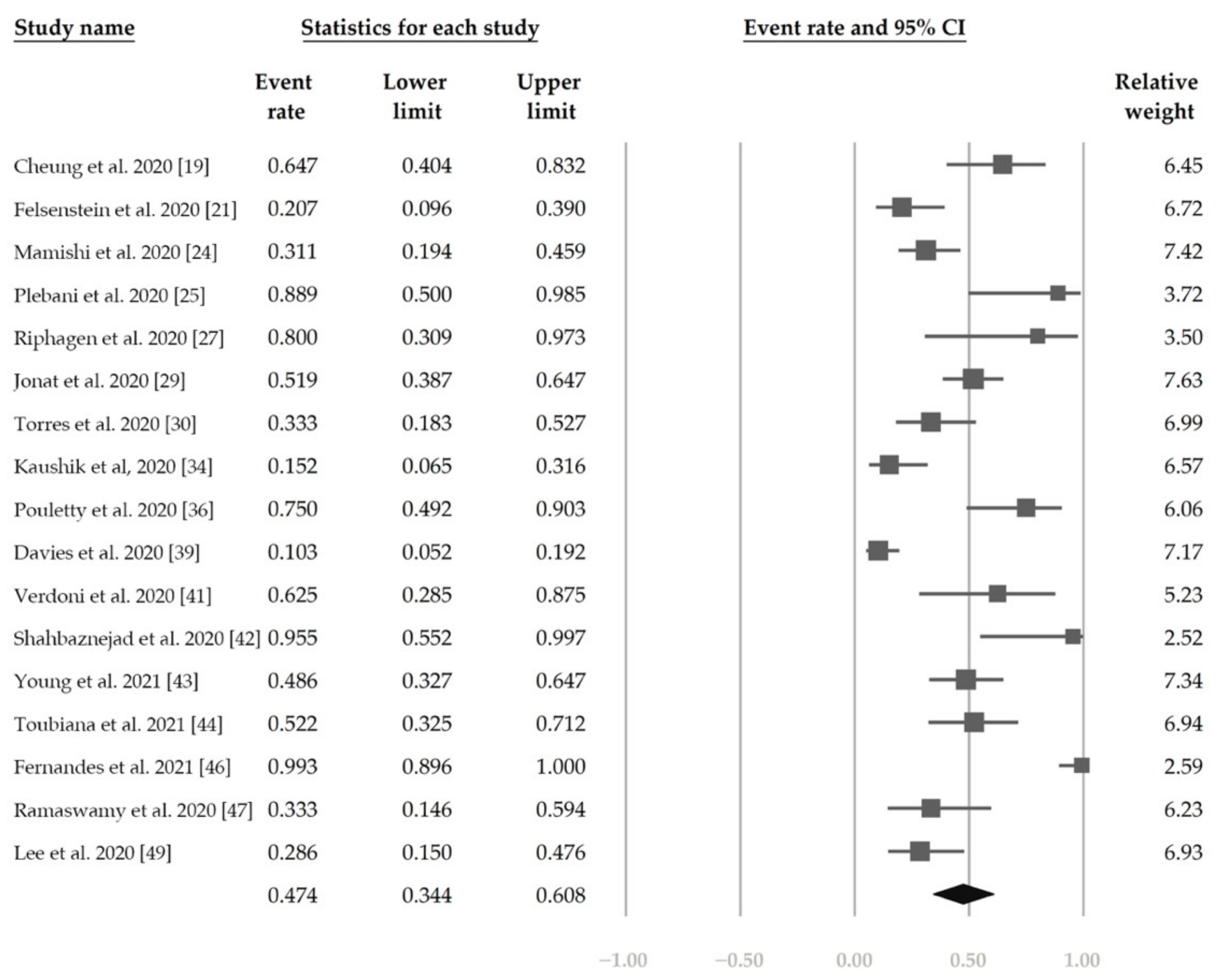
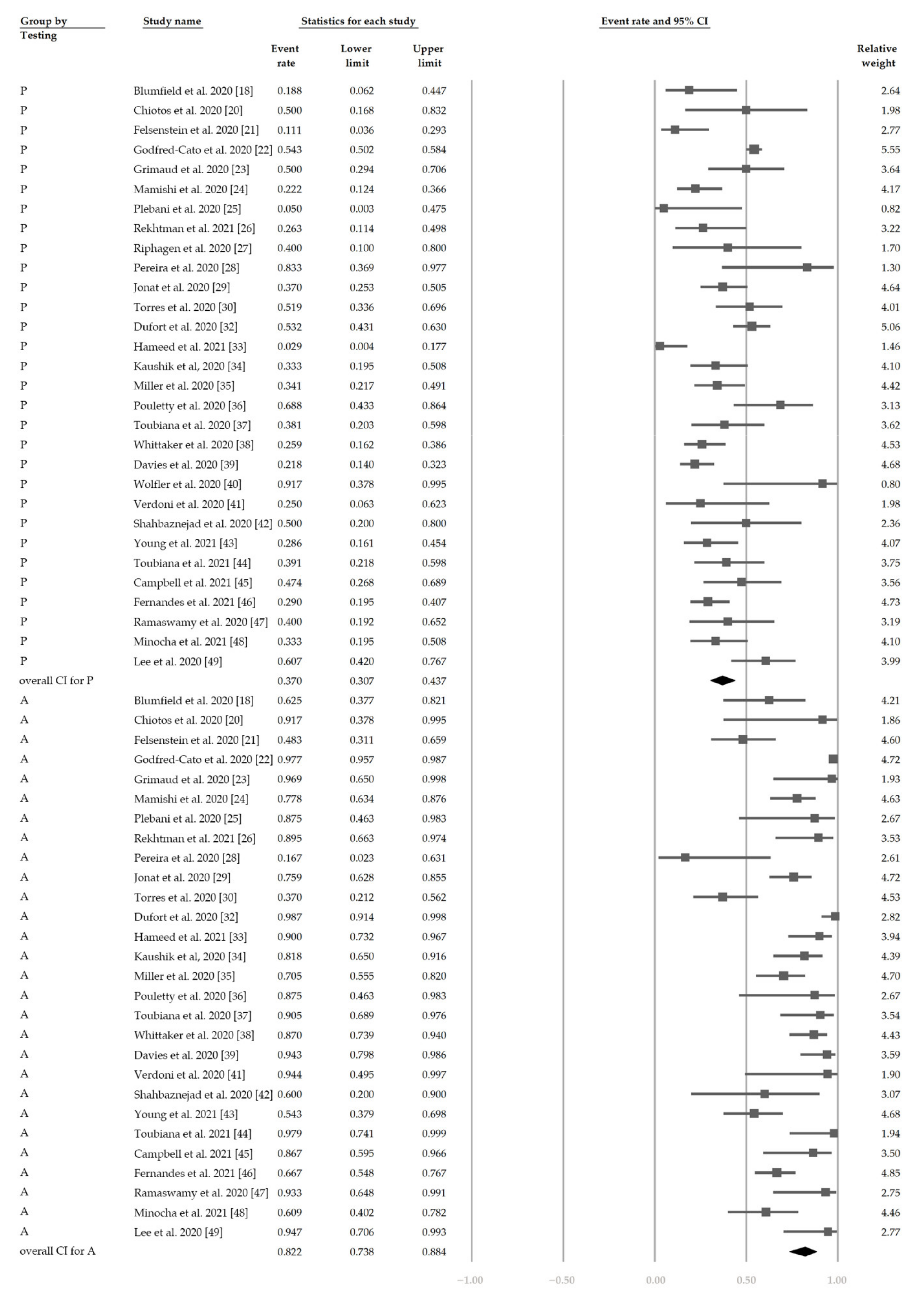
3.3. Primary Outcomes
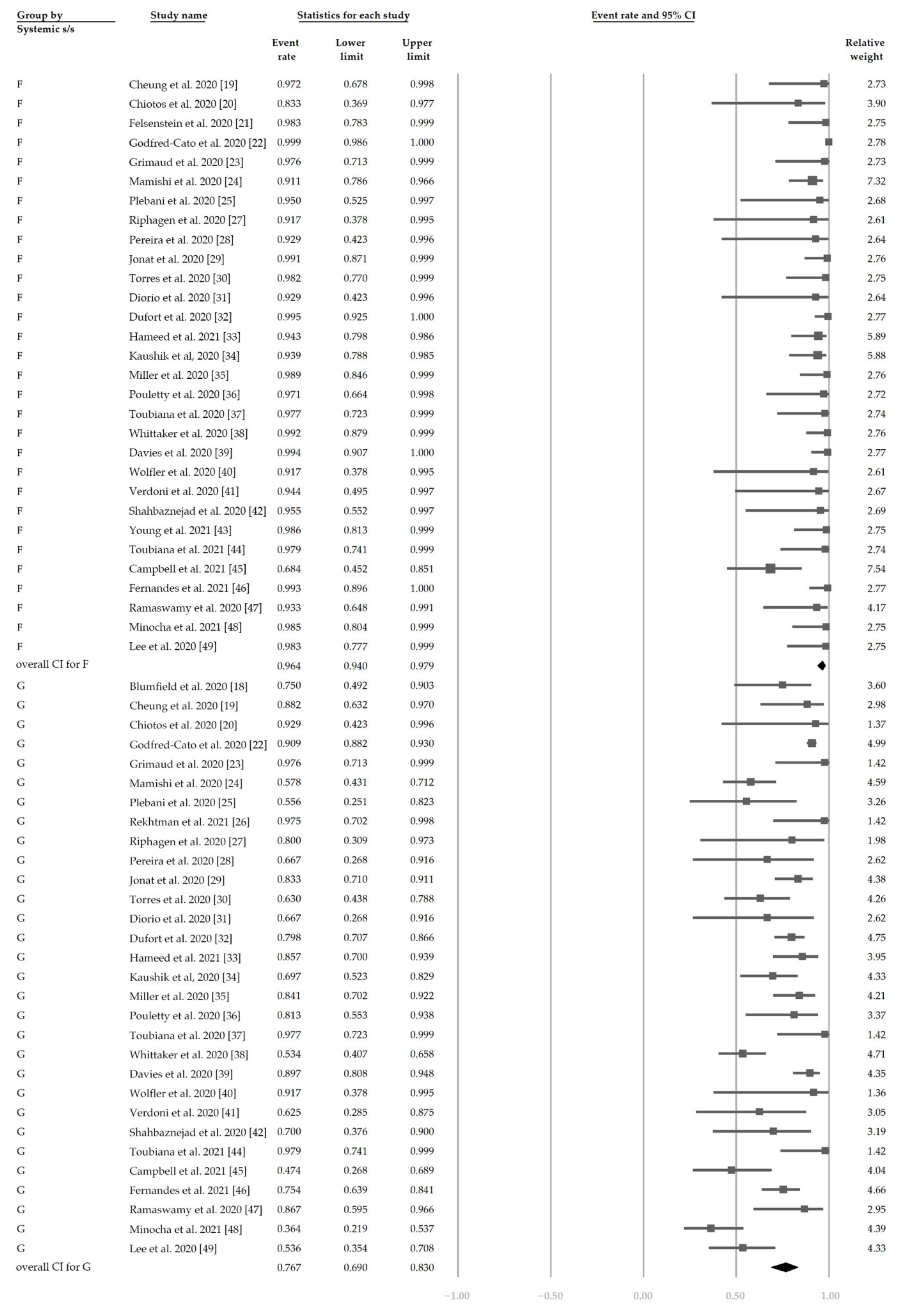
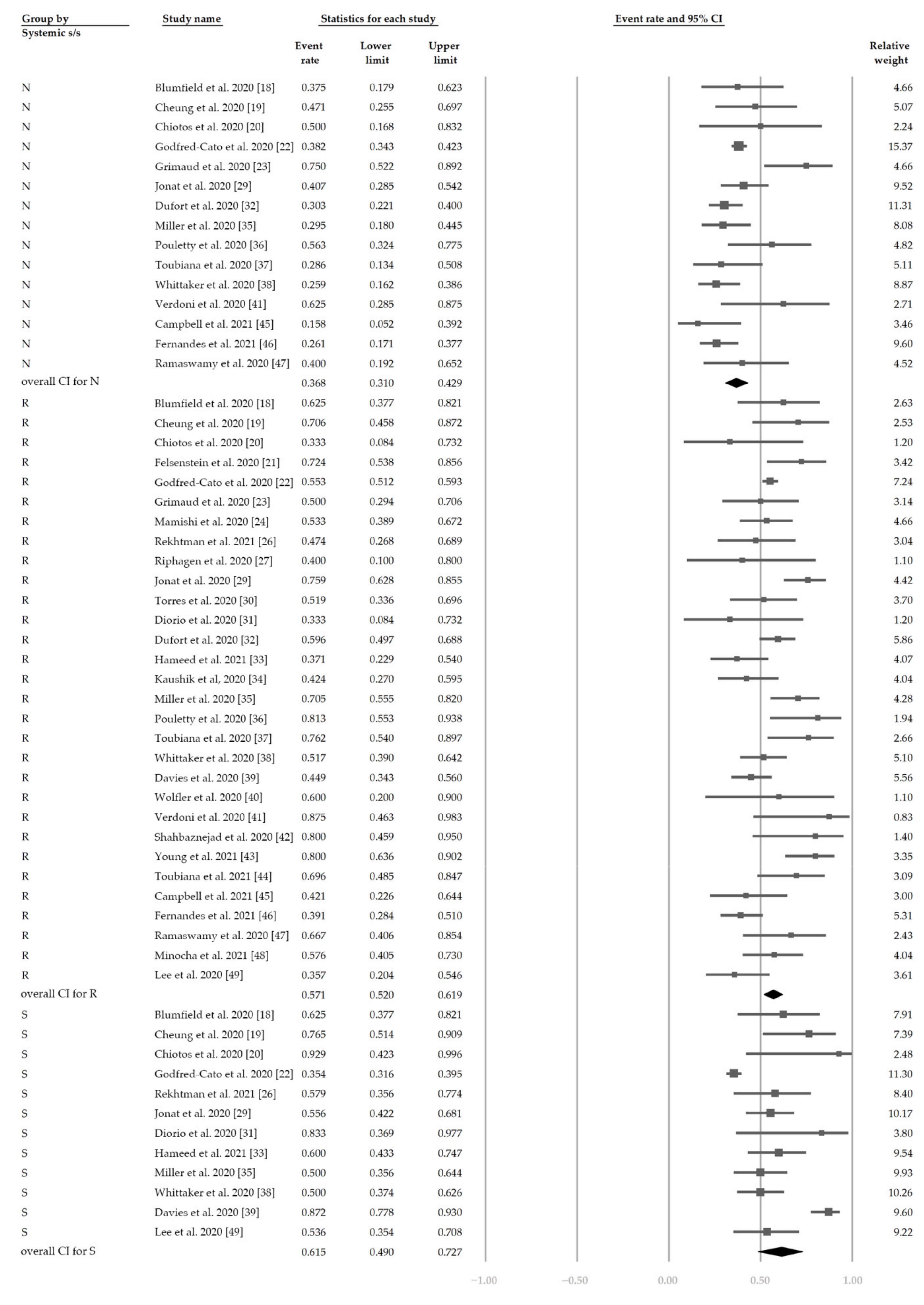
3.4. Secondary Outcomes
3.5. Heterogeneity and Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Danesh-Meyer, H.V.; McGhee, C.N.J. Implications of COVID-19 for ophthalmologists. Am. J. Ophthalmol. 2021, 223, 108–118. [Google Scholar] [CrossRef]
- Ludvigsson, J.F. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. 2020, 109, 1088–1095. [Google Scholar] [CrossRef]
- Zimmermann, P.; Curtis, N. Coronavirus infections in children including COVID-19: An overview of the epidemiology, clinical features, diagnosis, treatment and prevention options in children. Pediatric Infect. Dis. J. 2020, 39, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.I.; Hu, Y.L.; Chen, P.Y.; Huang, Y.C.; Hsueh, P.R. Are children less susceptible to COVID-19? J. Microbiol. Immunol. Infect. 2020, 53, 371–372. [Google Scholar] [CrossRef] [PubMed]
- PICS Statement: Increased Number of Reported Cases of Novel Presentation of Multisystem Inflammatory Disease, Paediatric Critical Care Society 2020. Available online: https://pccsociety.uk/news/pics-statement-regarding-novel-presentation-of-multi-system-inflammatory-disease/ (accessed on 23 March 2021).
- Baradaran, A.; Malek, A.; Moazzen, N.; Abbasi Shaye, Z. COVID-19 associated multisystem inflammatory syndrome: A systematic review and meta-analysis. Iran. J. Allergy Asthma Immunol. 2020, 19, 570–588. [Google Scholar]
- Hoste, L.; Van Paemel, R.; Haerynck, F. Multisystem inflammatory syndrome in children related to COVID-19: A systematic review. Eur. J. Pediatr. 2021, 180, 2019–2034. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Tang, K.; Levin, M.; Irfan, O.; Morris, S.K.; Wilson, K.; Klein, J.D.; Bhutta, Z.A. COVID-19 and multisystem inflammatory syndrome in children and adolescents. Lancet. Infect. Dis. 2020, 20, e276–e288. [Google Scholar] [CrossRef]
- Castagnoli, R.; Votto, M.; Licari, A.; Brambilla, I.; Bruno, R.; Perlini, S.; Rovida, F.; Baldanti, F.; Marseglia, G.L. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in children and adolescents: A systematic review. JAMA Pediatr. 2020, 174, 882–889. [Google Scholar] [CrossRef] [Green Version]
- Paediatric Multisystem Inflammatory Syndrome Temporally Associated with COVID-19 (PIMS)—Guidance for Clinicians, Royal College of Paediatrics and Child Health. Available online: https://www.rcpch.ac.uk/resources/paediatric-multisystem-inflammatory-syndrome-temporally-associated-covid-19-pims-guidance (accessed on 12 March 2021).
- Multisystem Inflammatory Syndrome in Children and Adolescents Temporally Related to COVID-19, World Health Organization 2020. Available online: https://www.who.int/news-room/commentaries/detail/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19 (accessed on 12 March 2021).
- Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with Coronavirus Disease 2019 (COVID-19), Centers for Disease Control and Prevention. Available online: https://emergency.cdc.gov/han/2020/han00432.asp (accessed on 12 March 2021).
- Casagrande, M.; Fitzek, A.; Püschel, K.; Aleshcheva, G.; Schultheiss, H.P.; Berneking, L.; Spitzer, M.S.; Schultheiss, M. Detection of SARS-CoV-2 in human retinal biopsies of deceased COVID-19 patients. Ocul. Immunol. Inflamm. 2020, 28, 721–725. [Google Scholar] [CrossRef]
- Casagrande, M.; Fitzek, A.; Spitzer, M.; Püschel, K.; Glatzel, M.; Krasemann, S.; Aepfelbacher, M.; Nörz, D.; Lütgehetmann, M.; Pfefferle, S.; et al. Detection of SARS-CoV-2 genomic and subgenomic RNA in retina and optic nerve of patients with COVID-19. Br. J. Ophthalmol. 2021. [Google Scholar] [CrossRef]
- Guemes-Villahoz, N.; Burgos-Blasco, B.; Vidal-Villegas, B.; Donate-López, J.; de la Muela, M.H.; López-Guajardo, L.; Martín-Sánchez, F.J.; García-Feijoó, J. Reduced macular vessel density in COVID-19 patients with and without associated thrombotic events using optical coherence tomography angiography. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 1–7. [Google Scholar] [CrossRef]
- Wu, Q.; Xing, Y.; Shi, L.; Li, W.; Gao, Y.; Pan, S.; Wang, Y.; Wang, W.; Xing, Q. Coinfection and other clinical characteristics of COVID-19 in children. Pediatrics 2020, 146, e20200961. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The prisma statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumfield, E.; Levin, T.L.; Kurian, J.; Lee, E.Y.; Liszewski, M.C. Imaging findings in multisystem inflammatory syndrome in children (MIS-C) associated with COVID. Am. J. Roentgenol. 2020, 216, 507–517. [Google Scholar] [CrossRef]
- Cheung, E.W.; Zachariah, P.; Gorelik, M.; Boneparth, A.; Kernie, S.G.; Orange, J.S.; Milner, J.D. Multisystem inflammatory syndrome related to COVID-19 in previously healthy children and adolescents in New York City. JAMA 2020, 324, 294–296. [Google Scholar] [CrossRef]
- Chiotos, K.; Bassiri, H.; Behrens, E.M.; Blatz, A.M.; Chang, J.; Diorio, C.; Fitzgerald, J.C.; Topjian, A.; John, A.R.O. Multisystem inflammatory syndrome in children during the coronavirus 2019 pandemic: A case series. J. Pediatric Infect. Dis. Soc. 2020, 9, 393–398. [Google Scholar] [CrossRef]
- Felsenstein, S.; Willis, E.; Lythgoe, H.; McCann, L.; Cleary, A.; Mahmood, K.; Porter, D.; Jones, J.; McDonagh, J.; Chieng, A.; et al. Presentation, treatment response and short-term outcomes in paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 (PIMS-TS). J. Clin. Med. 2020, 9, 3293. [Google Scholar] [CrossRef] [PubMed]
- Godfred-Cato, S.; Bryant, B.; Leung, J.; Oster, M.E.; Conklin, L.; Abrams, J.; Roguski, K.; Wallace, B.; Prezzato, E.; Koumans, E.H.; et al. COVID-19-associated multisystem inflammatory syndrome in children—United States, March–July 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1074–1080. [Google Scholar] [CrossRef] [PubMed]
- Grimaud, M.; Starck, J.; Levy, M.; Marais, C.; Chareyre, J.; Khraiche, D.; Leruez-Ville, M.; Quartier, P.; Léger, P.L.; Geslain, G.; et al. Acute myocarditis and multisystem inflammatory emerging disease following SARS-CoV-2 infection in critically ill children. Ann. Intensive Care 2020, 10, 69. [Google Scholar] [CrossRef]
- Mamishi, S.; Movahedi, Z.; Mohammadi, M.; Ziaee, V.; Khodabandeh, M.; Abdolsalehi, M.R.; Navaeian, A.; Heydari, H.; Mahmoudi, S.; Pourakbari, B. Multisystem inflammatory syndrome associated with SARS-CoV-2 infection in 45 children: A first report from Iran. Epidemiol. Infect. 2020, 148, e196. [Google Scholar] [CrossRef]
- Plebani, A.; Meini, A.; Cattalini, M.; Lougaris, V.; Bugatti, A.; Caccuri, F.; Caruso, A. Mycoplasma infection may complicate the clinical course of SARS-CoV-2 associated Kawasaki-like disease in children. Clin. Immunol. 2020, 221, 108613. [Google Scholar] [CrossRef]
- Rekhtman, S.; Tannenbaum, R.; Strunk, A.; Birabaharan, M.; Wright, S.; Garg, A. Mucocutaneous disease and related clinical characteristics in hospitalized children and adolescents with COVID-19 and multisystem inflammatory syndrome in children. J. Am. Acad. Dermatol. 2021, 84, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Riphagen, S.; Gomez, X.; Gonzalez-Martinez, C.; Wilkinson, N.; Theocharis, P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet 2020, 395, 1607–1608. [Google Scholar] [CrossRef]
- Pereira, M.F.B.; Litvinov, N.; Farhat, S.C.L.; Eisencraft, A.P.; Gibelli, M.; Carvalho, W.B.; Fernandes, V.R.; Fink, T.T.; Framil, J.V.S.; Galleti, K.V.; et al. Severe clinical spectrum with high mortality in pediatric patients with COVID-19 and multisystem inflammatory syndrome. Clinics 2020, 75, e2209. [Google Scholar] [CrossRef] [PubMed]
- Jonat, B.; Gorelik, M.; Boneparth, A.; Geneslaw, A.S.; Zachariah, P.; Shah, A.; Broglie, L.; Duran, J.; Morel, K.D.; Zorrilla, M.; et al. Multisystem inflammatory syndrome in children associated with coronavirus disease 2019 in a children’s hospital in New York City: Patient characteristics and an institutional protocol for evaluation, management, and follow-up. Pediatric Crit. Care Med. 2020, 22, e178. [Google Scholar] [CrossRef]
- Torres, J.P.; Izquierdo, G.; Acuña, M.; Pavez, D.; Reyes, F.; Fritis, A.; González, R.; Rivacoba, C.; Contardo, V.; Tapia, L.I. Multisystem inflammatory syndrome in children (MIS-C): Report of the clinical and epidemiological characteristics of cases in Santiago de Chile during the SARS-CoV-2 pandemic. Int. J. Infect. Dis. 2020, 100, 75–81. [Google Scholar] [CrossRef]
- Diorio, C.; Henrickson, S.E.; Vella, L.A.; McNerney, K.O.; Chase, J.; Burudpakdee, C.; Lee, J.H.; Jasen, C.; Balamuth, F.; Barrett, D.M.; et al. Multisystem inflammatory syndrome in children and COVID-19 are distinct presentations of SARS-CoV-2. J. Clin. Investig. 2020, 130, 5967–5975. [Google Scholar] [CrossRef]
- Dufort, E.M.; Koumans, E.H.; Chow, E.J.; Rosenthal, E.M.; Muse, A.; Rowlands, J.; Barranco, M.A.; Maxted, A.M.; Rosenberg, E.S.; Easton, D.; et al. Multisystem inflammatory syndrome in children in New York state. N. Engl. J. Med. 2020, 383, 347–358. [Google Scholar] [CrossRef]
- Hameed, S.; Elbaaly, H.; Reid, C.E.L.; Santos, R.M.F.; Shivamurthy, V.; Wong, J.; Jogeesvaran, K.H. Spectrum of imaging findings at chest radiography, us, ct, and mri in multisystem inflammatory syndrome in children associated with COVID-19. Radiology 2021, 298, E1–E10. [Google Scholar] [CrossRef]
- Kaushik, S.; Aydin, S.I.; Derespina, K.R.; Bansal, P.B.; Kowalsky, S.; Trachtman, R.; Gillen, J.K.; Perez, M.M.; Soshnick, S.H.; Conway, E.E., Jr.; et al. Multisystem inflammatory syndrome in children associated with severe acute respiratory syndrome coronavirus 2 infection (MIS-C): A multi-institutional study from New York City. J. Pediatr. 2020, 224, 24–29. [Google Scholar] [CrossRef]
- Miller, J.; Cantor, A.; Zachariah, P.; Ahn, D.; Martinez, M.; Margolis, K.G. Gastrointestinal symptoms as a major presentation component of a novel multisystem inflammatory syndrome in children that is related to coronavirus disease 2019: A single center experience of 44 cases. Gastroenterology 2020, 159, 1571–1574. [Google Scholar] [CrossRef]
- Pouletty, M.; Borocco, C.; Ouldali, N.; Caseris, M.; Basmaci, R.; Lachaume, N.; Bensaid, P.; Pichard, S.; Kouider, H.; Morelle, G.; et al. Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 mimicking Kawasaki disease (Kawa-COVID-19): A multicentre cohort. Ann. Rheum. Dis. 2020, 79, 999–1006. [Google Scholar] [CrossRef]
- Toubiana, J.; Poirault, C.; Corsia, A.; Bajolle, F.; Fourgeaud, J.; Angoulvant, F.; Debray, A.; Basmaci, R.; Salvador, E.; Biscardi, S.; et al. Kawasaki-like multisystem inflammatory syndrome in children during the covid-19 pandemic in Paris, France: Prospective observational study. BMJ 2020, 369, m2094. [Google Scholar] [CrossRef]
- Whittaker, E.; Bamford, A.; Kenny, J.; Kaforou, M.; Jones, C.E.; Shah, P.; Ramnarayan, P.; Fraisse, A.; Miller, O.; Davies, P.; et al. Clinical characteristics of 58 children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. Jama 2020, 324, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Davies, P.; Evans, C.; Kanthimathinathan, H.K.; Lillie, J.; Brierley, J.; Waters, G.; Johnson, M.; Griffiths, B.; du Pré, P.; Mohammad, Z.; et al. Intensive care admissions of children with paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) in the UK: A multicentre observational study. Lancet Child Adolesc. Health 2020, 4, 669–677. [Google Scholar] [CrossRef]
- Wolfler, A.; Mannarino, S.; Giacomet, V.; Camporesi, A.; Zuccotti, G. Acute myocardial injury: A novel clinical pattern in children with COVID-19. Lancet Child Adolesc. Health 2020, 4, e26–e27. [Google Scholar] [CrossRef]
- Verdoni, L.; Mazza, A.; Gervasoni, A.; Martelli, L.; Ruggeri, M.; Ciuffreda, M.; Bonanomi, E.; D’Antiga, L. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: An observational cohort study. Lancet 2020, 395, 1771–1778. [Google Scholar] [CrossRef]
- Shahbaznejad, L.; Navaeifar, M.R.; Abbaskhanian, A.; Hosseinzadeh, F.; Rahimzadeh, G.; Rezai, M.S. Clinical characteristics of 10 children with a pediatric inflammatory multisystem syndrome associated with COVID-19 in Iran. BMC Pediatr. 2020, 20, 513. [Google Scholar] [CrossRef]
- Young, T.K.; Shaw, K.S.; Shah, J.K.; Noor, A.; Alperin, R.A.; Ratner, A.J.; Orlow, S.J.; Betensky, R.A.; Shust, G.F.; Kahn, P.J.; et al. Mucocutaneous manifestations of multisystem inflammatory syndrome in children during the COVID-19 pandemic. JAMA Dermatol. 2021, 157, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Toubiana, J.; Cohen, J.F.; Brice, J.; Poirault, C.; Bajolle, F.; Curtis, W.; Moulin, F.; Matczak, S.; Leruez, M.; Casanova, J.L.; et al. Distinctive features of Kawasaki disease following SARS-CoV-2 infection: A controlled study in Paris, France. J. Clin. Immunol. 2021, 41, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.I.; Roberts, J.E.; Dubois, M.; Naureckas Li, C.; Sandora, T.J.; Lamb, G.S. Non-SARS-CoV-2 infections among patients evaluated for MIS-C associated with COVID-19. Pediatric Infect. Dis. J. 2021, 40, e90–e93. [Google Scholar] [CrossRef]
- Fernandes, D.M.; Oliveira, C.R.; Guerguis, S.; Eisenberg, R.; Choi, J.; Kim, M.; Abdelhemid, A.; Agha, R.; Agarwal, S.; Aschner, J.L.; et al. Severe acute respiratory syndrome coronavirus 2 clinical syndromes and predictors of disease severity in hospitalized children and youth. J. Pediatr. 2021, 230, 23–31. [Google Scholar] [CrossRef]
- Ramaswamy, A.; Brodsky, N.N.; Sumida, T.S.; Comi, M.; Asashima, H.; Hoehn, K.B.; Li, N.; Liu, Y.; Shah, A.; Ravindra, N.G.; et al. Post-infectious inflammatory disease in MIS-C features elevated cytotoxicity signatures and autoreactivity that correlates with severity. medRxiv. 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.12.01.20241364v1.full (accessed on 20 March 2021).
- Minocha, P.K.; Phoon, C.K.L.; Verma, S.; Singh, R.K. Cardiac findings in pediatric patients with multisystem inflammatory syndrome in children associated with COVID-19. Clin. Pediatr. 2021, 60, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.Y.; Day-Lewis, M.; Henderson, L.A.; Friedman, K.G.; Lo, J.; Roberts, J.E.; Lo, M.S.; Platt, C.D.; Chou, J.; Hoyt, K.J.; et al. Distinct clinical and immunological features of SARS-CoV-2-induced multisystem inflammatory syndrome in children. J. Clin. Investig. 2020, 130, 5942–5950. [Google Scholar] [CrossRef] [PubMed]
- Abrams, J.Y.; Godfred-Cato, S.E.; Oster, M.E.; Chow, E.J.; Koumans, E.H.; Bryant, B.; Leung, J.W.; Belay, E.D. Multisystem inflammatory syndrome in children associated with severe acute respiratory syndrome coronavirus 2: A systematic review. J. Pediatr. 2020, 226, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Kiss, A.; Ryan, P.M.; Mondal, T. Management of COVID-19-associated multisystem inflammatory syndrome in children: A comprehensive literature review. Prog. Pediatric Cardiol. 2021, 101381. [Google Scholar] [CrossRef]
- Esposito, S.; Principi, N. Multisystem inflammatory syndrome in children related to SARS-CoV-2. Paediatric Drugs 2021, 23, 119–129. [Google Scholar]
- Kabeerdoss, J.; Pilania, R.K.; Karkhele, R.; Kumar, T.S.; Danda, D.; Singh, S. Severe COVID-19, multisystem inflammatory syndrome in children, and Kawasaki disease: Immunological mechanisms, clinical manifestations and management. Rheumatol. Int. 2021, 41, 19–32. [Google Scholar] [CrossRef]
- Belot, A.; Antona, D.; Renolleau, S.; Javouhey, E.; Hentgen, V.; Angoulvant, F.; Delacourt, C.; Iriart, X.; Ovaert, C.; Bader-Meunier, B.; et al. SARS-CoV-2-related paediatric inflammatory multisystem syndrome, an epidemiological study, France, 1 March to 17 May 2020. Eurosurveillance 2020, 25. [Google Scholar] [CrossRef]
- McCrindle, B.W.; Rowley, A.H.; Newburger, J.W.; Burns, J.C.; Bolger, A.F.; Gewitz, M.; Baker, A.L.; Jackson, M.A.; Takahashi, M.; Shah, P.B.; et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A scientific statement for health professionals from the American Heart Association. Circulation 2017, 135, e927–e999. [Google Scholar] [CrossRef]
- Rife, E.; Gedalia, A. Kawasaki disease: An update. Curr. Rheumatol. Rep. 2020, 22, 75. [Google Scholar] [CrossRef] [PubMed]
- Rowley, A.H.; Shulman, S.T. The epidemiology and pathogenesis of Kawasaki disease. Front. Pediatr. 2018, 6, 374. [Google Scholar] [CrossRef] [Green Version]
- Cohen, E.; Sundel, R. Kawasaki disease at 50 years. JAMA Pediatr. 2016, 170, 1093–1099. [Google Scholar] [CrossRef]
- Sood, M.; Sharma, S.; Sood, I.; Sharma, K.; Kaushik, A. Emerging evidence on multisystem inflammatory syndrome in children associated with SARS-CoV-2 infection: A systematic review with meta-analysis. SN Compr. Clin. Med. 2021, 1–10. [Google Scholar] [CrossRef]
- Aronoff, S.C.; Hall, A.; Del Vecchio, M.T. The natural history of severe acute respiratory syndrome coronavirus 2-related multisystem inflammatory syndrome in children: A systematic review. J. Pediatric Infect. Dis. Soc. 2020, 9, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Loffredo, L.; Pacella, F.; Pacella, E.; Tiscione, G.; Oliva, A.; Violi, F. Conjunctivitis and COVID-19: A meta-analysis. J. Med. Virol. 2020, 92, 1413–1414. [Google Scholar] [CrossRef]
- Tang, Y.; Li, W.; Baskota, M.; Zhou, Q.; Fu, Z.; Luo, Z.; Shi, Y.; Chen, Y.; Liu, E. Multisystem inflammatory syndrome in children during the coronavirus disease 2019 (COVID-19) pandemic: A systematic review of published case studies. Transl. Pediatr. 2021, 10, 121–135. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Hasani, H.; Mardi, S.; Shakerian, S.; Taherzadeh-Ghahfarokhi, N.; Mardi, P. The novel coronavirus disease (COVID-19): A PRISMA systematic review and meta-analysis of clinical and paraclinical characteristics. BioMed Res. Int. 2020, 2020, 3149020. [Google Scholar] [CrossRef] [PubMed]
- Panigrahy, N.; Policarpio, J.; Ramanathan, R. Multisystem inflammatory syndrome in children and SARS-CoV-2: A scoping review. J. Pediatric Rehabil. Med. 2020, 13, 301–316. [Google Scholar] [CrossRef]
- Makino, N.; Nakamura, Y.; Yashiro, M.; Kosami, K.; Matsubara, Y.; Ae, R.; Aoyama, Y.; Yanagawa, H. Nationwide epidemiologic survey of Kawasaki disease in Japan, 2015–2016. Pediatr. Int. 2019, 61, 397–403. [Google Scholar] [CrossRef]
- Holman, R.C.; Belay, E.D.; Christensen, K.Y.; Folkema, A.M.; Steiner, C.A.; Schonberger, L.B. Hospitalizations for Kawasaki syndrome among children in the United States, 1997–2007. Pediatric Infect. Dis. J. 2010, 29, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Nakra, N.A.; Blumberg, D.A.; Herrera-Guerra, A.; Lakshminrusimha, S. Multi-system inflammatory syndrome in children (MIS-C) following SARS-CoV-2 infection: Review of clinical presentation, hypothetical pathogenesis, and proposed management. Children 2020, 7, 69. [Google Scholar] [CrossRef] [PubMed]
- Henderson, L.A.; Canna, S.W.; Friedman, K.G.; Gorelik, M.; Lapidus, S.K.; Bassiri, H.; Behrens, E.M.; Ferris, A.; Kernan, K.F.; Schulert, G.S.; et al. American college of rheumatology clinical guidance for multisystem inflammatory syndrome in children associated with SARS-CoV-2 and hyperinflammation in pediatric COVID-19: Version 2. Arthritis Rheumatol. 2021, 73, e13–e29. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Type | Publication Date | Country | Pts, n | No. of Eyes | Median Age (IQR), Year | Range of Age, Year | Male, n (%) | Hospitalized Days † |
|---|---|---|---|---|---|---|---|---|---|
| Blumfield et al. 2020 [18] | R | Aug, 2020 | USA | 16 | 32 | 9.2 ± 4.9 * | 1.7–20 | 10 (63) | NR |
| Cheung et al. 2020 [19] | P | Jun, 2020 | USA | 17 | 34 | 8(4.9–12) | 1.8–16 | 8 (47) | 13–18 |
| Chiotos et al. 2020 [20] | CS | May, 2020 | USA | 6 | 12 | 7.5 (5–12) | 5–14 | 1 (17) | 8–17 |
| Felsenstein et al. 2020 [21] | R | Oct, 2020 | UK | 29 | 58 | 6 (3.8–9.9) | NR | 20 (69) | 14 |
| Godfred-Cato et al. 2020 [22] | C | Aug, 2020 | USA | 570 | 1140 | 8 (4–12) | NR | 316 (55) | 6 |
| Grimaud et al. 2020 [23] | R | Jun, 2020 | France | 20 | 40 | 8.6 (7–11.6) | 2.9–15 | 10 (50) | 1–10 |
| Mamishi et al. 2020 [24] | R | Aug, 2020 | Iran | 45 | 90 | 7 (4–9.9) | 0.8–17 | 24 (53) | 8 (6–11) |
| Plebani et al. 2020 [25] | CS | Oct, 2020 | Italy | 9 | 18 | 10 (3–11) | 1.1–14 | 6 (67) | 3–15 |
| Rekhtman et al. 2021 [26] | P | Dec, 2020 | USA | 19 | 38 | 9 (8.5–11.5) | NR | 13 (68) | 7 (5–10) |
| Riphagen et al. 2020 [27] | CS | May, 2020 | UK | 5 | 10 | 8 (6–11) | 6–14 | 3 (60) | 3–7 |
| Pereira et al. 2020 [28] | CS | Aug, 2020 | Brazil | 6 | 12 | 7.8 (3.9–12.7) | 0.01–17.6 | 5 (83) | NR |
| Jonat et al. 2020 [29] | P | Oct, 2020 | USA | 54 | 108 | 7 (3.9–13.5) | 0.8–20 | 25 (46) | 1–19 |
| Torres et al. 2020 [30] | CS | Aug, 2020 | Chile | 27 | 54 | 6 (3–10) | 0–14 | 14 (52) | 9 (6–13) |
| Diorio et al. 2020 [31] | P | Jul, 2020 | USA | 6 | 12 | 6 (5–7) | 5–13 | 2 (33) | NR |
| Dufort et al. 2020 [32] | R | Jul, 2020 | USA | 99 | 198 | 9 (4.0–13.3) | NR | 53 (54) | 6 (4–9) |
| Hameed et al. 2021 [33] | R | Jun, 2020 | UK | 35 | 70 | 11 (6–14) | NR | 27 (77) | 25 |
| Kaushik et al, 2020 [34] | R | Jun, 2020 | USA | 33 | 66 | 10 (6–13) | 0.2–20 | 20 (61) | 7.8 (6.0–10.1) |
| Miller et al. 2020 [35] | R | Jun, 2020 | USA | 44 | 88 | 7.3 (4.0–13.7) | 0.6–20 | 20 (45) | 26 |
| Pouletty et al. 2020 [36] | R | Jun, 2020 | France | 16 | 32 | 10 (4.7–12.5) | NR | 8 (50) | 21 (21–24) |
| Toubiana et al. 2020 [37] | R | Jun, 2020 | France | 21 | 42 | 7.9 (5.8–12.3) | 3.7–16.6 | 9 (43) | 5–17 |
| Whittaker et al. 2020 [38] | P | Jun, 2020 | England | 58 | 116 | 9 (5.7–14) | NR | 38 (66) | NR |
| Davies et al. 2020 [39] | R | Jul, 2020 | England | 78 | 156 | 11 (8–14) | NR | 52 (67) | 5.0 (3.0–6.5) |
| Wolfler et al. 2020 [40] | R | Jun, 2020 | Italy | 5 | 10 | NR | 0.1–14 | NR | 5–10 |
| Verdoni et al. 2020 [41] | P | May, 2020 | Italy | 8 | 16 | 6.3 (5.3–7.6) | 2.9–9.2 | 5 (63) | NR |
| Shahbaznejad et al. 2020 [42] | P | Nov, 2020 | Iran | 10 | 20 | 5.4 ± 3.9 * | 1.1–12 | 6 (60) | NR |
| Young et al. 2021 [43] | R | Dec, 2020 | USA | 35 | 70 | 2 (1.1–9.5) | 0.2–17 | 19 (54) | 2–55 |
| Toubiana et al. 2021 [44] | R | Jan, 2021 | France | 23 | 46 | 8.2 (7.4–10) | NR | 12 (52) | NR |
| Campbell et al. 2021 [45] | R | Nov, 2020 | USA | 19 | 38 | NR | NR | 9 (47) | 5–57 |
| Fernandes et al. 2021 [46] | R | Nov, 2020 | USA | 69 | 138 | 7 (3–11) | NR | 42 (60) | 6 (3–8) |
| Ramaswamy et al. 2020 [47] | P | Dec, 2020 | USA | 15 | 30 | 10.4 (2.6–18) | NR | 8 (53) | NR |
| Minocha et al. 2021 [48] | R | Sep, 2020 | USA | 33 | 66 | 2.8 (1.4–9) | NR | 19 (58) | 120 |
| Lee et al. 2020 [49] | R | Jul, 2020 | USA | 28 | 56 | 9 (4.5–13) | 0.1–17 | 16 (57) | 1–10 |
| Pts, n | Conjunctivitis, n (%) | Fever, n (%) | GI s/s, n (%) | Rash, n (%) | Shock, n (%) | Neurological s/s, n (%) | Respiratory s/s, n (%) | Lips and Oral Changes, n (%) | Cervical Lymphadenopathy, n (%) | Cardiovascular, n (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Blumfield et al. 2020 [18] | 16 | 8 (50.0) | NR | 12 (75) | 10 (63) | 10 (63) | 6 (38) | NR | 5 (31) | NR | NR |
| Cheung et al. 2020 [19] | 17 | 11 (64.7) | 17 (100) | 15 (88) | 12 (70) | 13 (76) | 8 (47) | 7 (41) | 9 (53) | 6 (35) | NR |
| Chiotos et al. 2020 [20] | 6 | 2 (33.3) | 5 (83) | 6 (100) | 2 (33) | 6 (100) | 3 (50) | 4 (67) | NR | NR | NR |
| Felsenstein et al. 2020 [21] | 29 | 18 (62.1) | 29 (100) | NR | 21 (72) | NR | NR | 6 (21) | NR | NR | 25 (86) |
| Godfred-Cato et al. 2020 [22] | 570 | 276 (48.4) | 570 (100) | 518 (90) | 315 (55) | 202 (36) | 218 (38) | 359 (63) | NR | NR | 493 (86) |
| Grimaud et al. 2020 [23] | 20 | 6 (30.0) | 20 (100) | 20 (100) | 10 (50) | NR | 15 (75) | NR | NR | NR | NR |
| Mamishi et al. 2020 [24] | 45 | 23 (51.1) | 41 (91) | 26 (58) | 24 (53) | NR | NR | NR | NR | 9 (20) | NR |
| Plebani et al. 2020 [25] | 9 | 5 (55.6) | 9 (100) | 5 (56) | NR | NR | NR | 3 (33) | NR | NR | NR |
| Rekhtman et al. 2021 [26] | 19 | 2 (10.5) | NR | 19 (100) | 9 (47) | 11 (58) | NR | 11 (58) | NR | NR | NR |
| Riphagen et al. 2020 [27] | 5 | 3 (60.0) | 5 (100) | 4 (80) | 2 (40) | NR | NR | NR | NR | NR | NR |
| Pereira et al. 2020 [28] | 6 | 0 (0) | 6 (100) | 4 (67) | NR | NR | NR | 5 (83) | NR | NR | NR |
| Jonat et al. 2020 [29] | 54 | 31 (57.4) | 54 (100) | 45 (83) | 41 (76) | 30 (56) | 22 (41) | 12 (22) | 20 (37) | 16 (30) | NR |
| Torres et al. 2020 [30] | 27 | 13 (48.1) | 27 (100) | 17 (63) | 14 (52) | NR | NR | 7 (26) | 11 (41) | NR | NR |
| Diorio et al. 2020 [31] | 6 | 4 (66.7) | 6 (100) | 4 (67) | 2 (33) | 5 (83) | NR | 4 (67) | NR | NR | NR |
| Dufort et al. 2020 [32] | 99 | 55 (55.6) | 99 (100) | 79 (80) | 59 (60) | NR | 30 (30) | 40 (40) | 27 (27) | 6 (6) | NR |
| Hameed et al. 2021 [33] | 35 | 9 (25.7) | 33 (94) | 30 (86) | 13 (37) | 21 (60) | NR | NR | NR | NR | NR |
| Kaushik et al, 2020 [34] | 33 | 12 (36.4) | 31 (94) | 23 (67) | 14 (42) | NR | NR | 11 (33) | NR | NR | NR |
| Miller et al. 2020 [35] | 44 | 23 (52.3) | 44 (100) | 37 (84) | 31 (70) | 22 (50) | 13 (30) | 11 (25) | 23 (52) | NR | 22 (67) |
| Pouletty et al. 2020 [36] | 16 | 15 (93.7) | 16 (100) | 13 (81) | 13 (81) | NR | 9 (56) | 2 (13) | 14 (88) | 6 (38) | NR |
| Toubiana et al. 2020 [37] | 21 | 17 (81.0) | 21 (100) | 21 (100) | 16 (76) | NR | 6 (29) | NR | 16 (76) | 12 (57) | NR |
| Whittaker et al. 2020 [38] | 58 | 26 (44.8) | 58 (100) | 31 (53) | 30 (52) | 29 (50) | 15 (26) | 12 (21) | 17 (29) | 9 (24) | NR |
| Davies et al. 2020 [39] | 78 | 23 (29.5) | 78 (100) | 70 (90) | 35 (45) | 68 (87) | NR | NR | NR | NR | NR |
| Wolfler et al. 2020 [40] | 5 | 1 (20.0) | 5 (100) | 5 (100) | 3 (60) | NR | NR | 3 (60) | NR | NR | NR |
| Verdoni et al. 2020 [41] | 8 | 7 (87.5) | 8 (100) | 5 (63) | 7 (88) | NR | 5 (63) | NR | NR | NR | NR |
| Shahbaznejad et al. 2020 [42] | 10 | 3 (30.0) | 10 (100) | 7 (70) | 8 (80) | NR | NR | 8 (80) | 4 (40) | NR | NR |
| Young et al. 2021 [43] | 35 | 21 (60.0) | 35 (100) | NR | 28 (80) | NR | NR | NR | 17 (49) | NR | NR |
| Toubiana et al. 2021 [44] | 23 | 19 (82.6) | 23 (100) | 23 (100) | 16 (70) | NR | NR | NR | 17 (74) | 14 (61) | NR |
| Campbell et al. 2021 [45] | 19 | 7 (36.8) | 13 (68) | 9 (20) | 8 (42) | NR | 3 (16) | 14 (74) | NR | NR | 18 (95) |
| Fernandes et al. 2021 [46] | 69 | 22 (31.9) | 69 (100) | 52 (75) | 27 (39) | NR | 18 (26) | 24 (35) | NR | NR | NR |
| Ramaswamy et al. 2020 [47] | 15 | 9 (60.0) | 14 (93) | 13 (87) | 10 (67) | NR | 6 (40) | NR | NR | NR | NR |
| Minocha et al. 2021 [48] | 33 | 12 (36.4) | 33 (100) | 12 (36) | 19 (58) | NR | NR | NR | NR | 8 (24) | NR |
| Lee et al. 2020 [49] | 28 | 16 (57.1) | 28 (100) | 15 (54) | 10 (36) | 15 (54) | NR | NR | 7 (25) | NR | NR |
| First Author | Number of Patients | With Complete Kawasaki Disease | Exposure History, * n (%) | Nasopharyngeal RT-PCR (+) | Serum Antibody (+) |
|---|---|---|---|---|---|
| Blumfield et al. 2020 [18] | 16 | NR | NR | 3/16 | 10/16 |
| Cheung et al. 2020 [19] | 17 | 8 (47.1%) | 11 (64.7%) | 8/unknown | 9/unknown |
| Chiotos et al. 2020 [20] | 6 | NR | NR | 3/6 | 5/5 |
| Felsenstein et al. 2020 [21] | 29 | 11 (37.9%) | 6 (20.7%) | 3/27 | 14/29 |
| Godfred-Cato et al. 2020 [22] | 570 | 28 (4.9%) | NR | 302/556 | 418/428 |
| Grimaud et al. 2020 [23] | 20 | 0 | NR | 10/20 | 15/15 |
| Mamishi et al. 2020 [24] | 45 | NR | 14 (31.1%) | 10/45 | 35/45 |
| Plebani et al. 2020 [25] | 9 | NR | 8 (88.9%) | 0 (0%) | 7/8 |
| Rekhtman et al. 2021 [26] | 19 | 0 (0%) | NR | 5/19 | 17/19 |
| Riphagen et al. 2020 [27] | 5 | NR | 4 (80.0%) | 2/5 | NR |
| Pereira et al. 2020 [28] | 6 | 2 (33.3%) | NR | 5/6 | 1/6 |
| Jonat et al. 2020 [29] | 54 | 20 (37.0%) | 28 (51.9%) | 20/54 | 41/54 |
| Torres et al. 2020 [30] | 27 | 27 (100%) | 9 (33.3%) | 14/27 | 10/27 |
| Diorio et al. 2020 [31] | 6 | 2 (33.3%) | NR | 5/unknown | 1/unknown |
| Dufort et al. 2020 [32] | 99 | 36 (36.4%) | NR | 50/94 | 76/77 |
| Hameed et al. 2021 [33] | 35 | NR | NR | 1/35 | 27/30 |
| Kaushik et al. 2020 [34] | 33 | NR | 5 (15.2%) | 11/33 | 27/33 |
| Miller et al. 2020 [35] | 44 | NR | NR | 15/44 | 31/44 |
| Pouletty et al. 2020 [36] | 16 | 10 (62.5%) | 12 (75.0%) | 11/16 | 7/8 |
| Toubiana et al. 2020 [37] | 21 | 11 (52.4%) | NR | 8/21 | 19/21 |
| Whittaker et al. 2020 [38] | 58 | NR | NR | 15/58 | 40/46 |
| Davies et al. 2020 [39] | 78 | NR | 8 (10.3%) | 17/78 | 33/35 |
| Wolfler et al. 2020 [40] | 5 | 0 (0%) | NR | 5/5 | NR |
| Verdoni et al. 2020 [41] | 8 | 4 (50.0%) | 5 (62.5%) | 2/8 | 8/8 |
| Shahbaznejad et al. 2020 [42] | 10 | 2 (20.0%) | 10 (100%) | 4/8 | 3/5 |
| Young et al. 2021 [43] | 35 | 14 (40.0%) | 17 (48.6%) | 10/35 | 19/35 |
| Toubiana et al. 2021 [44] | 23 | 10 (43.5%) | 12 (52.2%) | 9/23 | 23/23 |
| Campbell et al. 2021 [45] | 19 | NR | NR | 9/19 | 13/15 |
| Fernandes et al. 2021 [46] | 69 | NR | 69 (100%) | 20/69 | 46/69 |
| Ramaswamy et al. 2020 [47] | 15 | NR | 5 (33.3%) | 6/15 | 14/15 |
| Minocha et al. 2021 [48] | 33 | 3 (9.1%) | NR | 11/33 | 14/23 |
| Lee et al. 2020 [49] | 28 | 7 (25.0%) | 8 (28.6%) | 17/28 | 18/19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo, T.-C.; Chen, Y.-Y. Ocular and Systemic Manifestations in Paediatric Multisystem Inflammatory Syndrome Associated with COVID-19. J. Clin. Med. 2021, 10, 2953. https://doi.org/10.3390/jcm10132953
Lo T-C, Chen Y-Y. Ocular and Systemic Manifestations in Paediatric Multisystem Inflammatory Syndrome Associated with COVID-19. Journal of Clinical Medicine. 2021; 10(13):2953. https://doi.org/10.3390/jcm10132953
Chicago/Turabian StyleLo, Tzu-Chen, and Yu-Yen Chen. 2021. "Ocular and Systemic Manifestations in Paediatric Multisystem Inflammatory Syndrome Associated with COVID-19" Journal of Clinical Medicine 10, no. 13: 2953. https://doi.org/10.3390/jcm10132953
APA StyleLo, T.-C., & Chen, Y.-Y. (2021). Ocular and Systemic Manifestations in Paediatric Multisystem Inflammatory Syndrome Associated with COVID-19. Journal of Clinical Medicine, 10(13), 2953. https://doi.org/10.3390/jcm10132953