
Adiponectin Associates with Rheumatoid Arthritis Risk in Overweight and Obesity Independently of Other Adipokines

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
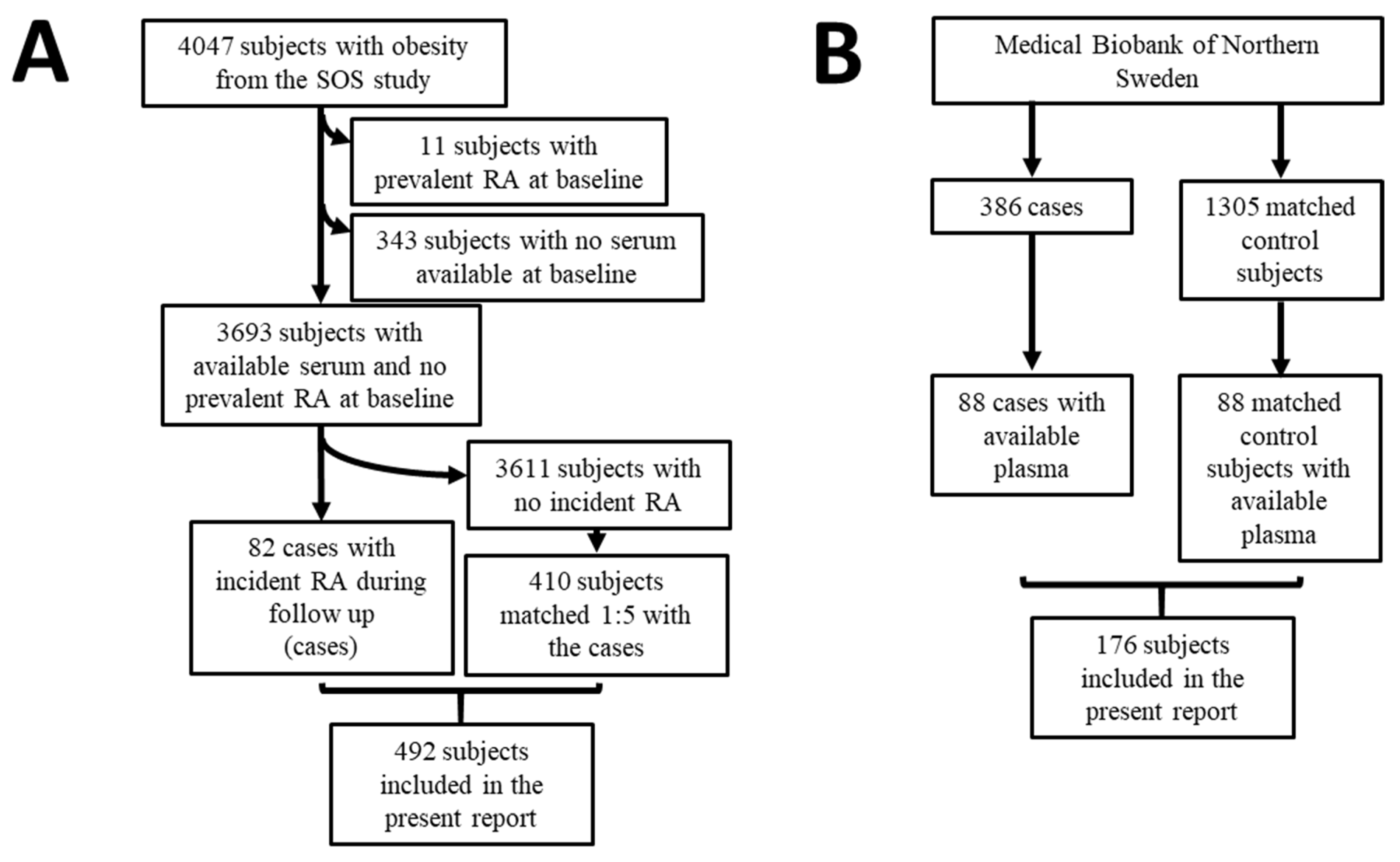
2.1. Baseline Characteristics of the Nested Case-Control Cohort from the SOS Study
2.2. Baseline Characteristics of the Nested Case-Control Cohort from the Medical Biobank of Northern Sweden
2.3. Multivariable Analyses for the Incidence of RA in the Nested Case-Control Cohort from the SOS Study
2.4. Multivariable Analysis for the Incidence of RA in the Nested Case-Control Cohort from the Medical Biobank of Northern Sweden
3. Discussion
4. Materials and Methods
4.1. SOS Study
4.2. The Cohort from the Medical Biobank of Northern Sweden
4.3. Biochemical Assessments
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kwon, H.; Pessin, J.E. Adipokines Mediate Inflammation and Insulin Resistance. Front. Endocrinol. 2013, 4, 71. [Google Scholar] [CrossRef] [Green Version]
- Mancuso, P. The role of adipokines in chronic inflammation. ImmunoTargets Ther. 2016, ume 5, 47–56. [Google Scholar] [CrossRef] [Green Version]
- Must, A.; Spadano, J.; Coakley, E.H.; Field, A.E.; Colditz, G.; Dietz, W.H. The Disease Burden Associated With Overweight and Obesity. JAMA 1999, 282, 1523–1529. [Google Scholar] [CrossRef]
- Choi, H.K.; Atkinson, K.; Karlson, E.W.; Curhan, G. Obesity, weight change, hypertension, diuretic use, and risk of gout in men: The health professionals follow-up study. Arch. Intern. Med. 2005, 165, 742–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- I Daïen, C.; Sellam, J. Obesity and inflammatory arthritis: Impact on occurrence, disease characteristics and therapeutic response. RMD Open 2015, 1, e000012. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Han, J.; Qureshi, A.A. Obesity and risk of incident psoriatic arthritis in US women. Ann. Rheum. Dis. 2012, 71, 1267–1272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, J.; Chen, Q.; Yu, F.; Wang, Z.; Chen, S.; Jin, Z.; Cai, Q.; Liu, Y.; He, J. Body Mass Index and Risk of Rheumatoid Arthritis: A Meta-Analysis of Observational Studies. Medicine 2016, 95, e2859. [Google Scholar] [CrossRef]
- Ouchi, N.; Parker, J.L.; Lugus, J.J.; Walsh, K. Adipokines in inflammation and metabolic disease. Nat. Rev. Immunol. 2011, 11, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Neumann, E.; Hasseli, R.; Ohl, S.; Lange, U.; Frommer, K.; Müller-Ladner, U. Adipokines and Autoimmunity in Inflammatory Arthritis. Cells 2021, 10, 216. [Google Scholar] [CrossRef] [PubMed]
- Otero, M.; Lago, R.; Gomez, R.; Lago, F.; Dieguez, C.; Gomez-Reino, J.J.; Gualillo, O. Changes in plasma levels of fat-derived hormones adiponectin, leptin, resistin and visfatin in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2006, 65, 1198–1201. [Google Scholar] [CrossRef] [Green Version]
- Achari, A.E.; Jain, S.K. Adiponectin, a Therapeutic Target for Obesity, Diabetes, and Endothelial Dysfunction. Int. J. Mol. Sci. 2017, 18, 1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aritaa, Y.; Kiharaa, S.; Ouchia, N.; Takahashia, M.; Maedaa, K.; Ichiromiyagawaa, J.-; Hotta, K.; Shimomuraa, I.; Nakamuraa, T.; Miyaokaa, K.; et al. Paradoxical Decrease of an Adipose-Specific Protein, Adiponectin, in Obesity. Biochem. Biophys. Res. Commun. 1999, 257, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Kadowaki, T.; Yamauchi, T.; Kubota, N.; Hara, K.; Ueki, K.; Tobe, K. Adiponectin and adiponectin receptors in insulin resistance, diabetes, and the metabolic syndrome. J. Clin. Investig. 2006, 116, 1784–1792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.H.; Bae, S.-C. Circulating adiponectin and visfatin levels in rheumatoid arthritis and their correlation with disease activity: A meta-analysis. Int. J. Rheum. Dis. 2018, 21, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-W.; Park, M.-C.; Park, Y.-B.; Lee, S.-K. Measurement of the serum leptin level could assist disease activity monitoring in rheumatoid arthritis. Rheumatol. Int. 2007, 27, 537–540. [Google Scholar] [CrossRef]
- Van Laar, J.; O’Reilly, S.; Muraoka, S.; Kusunoki, N.; Takahashi, H.; Tsuchiya, K.; Kawai, S. Faculty of 1000 evaluation for Leptin stimulates interleukin-6 production via janus kinase 2/signal transducer and activator of transcription 3 in rheumatoid synovial fibroblasts. F1000 Post-Publ. Peer Rev. Biomed. Lit. 2013, 31, 589–595. [Google Scholar] [CrossRef]
- Senolt, L.; Housa, D.; Vernerova, Z.; Jirasek, T.; Svobodova, R.; Veigl, D.; Anderlova, K.; Muller-Ladner, U.; Pavelka, K.; Haluzik, M. Resistin in rheumatoid arthritis synovial tissue, synovial fluid and serum. Ann. Rheum. Dis. 2006, 66, 458–463. [Google Scholar] [CrossRef] [Green Version]
- Rho, Y.H.; Solus, J.; Sokka, T.; Oeser, A.; Chung, C.P.; Gebretsadik, T.; Shintani, A.; Pincus, T.; Stein, C.M. Adipocytokines are associated with radiographic joint damage in rheumatoid arthritis. Arthritis Rheum. 2009, 60, 1906–1914. [Google Scholar] [CrossRef] [Green Version]
- Sato, H.; Muraoka, S.; Kusunoki, N.; Masuoka, S.; Yamada, S.; Ogasawara, H.; Imai, T.; Akasaka, Y.; Tochigi, N.; Takahashi, H.; et al. Resistin upregulates chemokine production by fibroblast-like synoviocytes from patients with rheumatoid arthritis. Arthritis Res. 2017, 19, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Bokarewa, M.; Nagaev, I.; Dahlberg, L.; Smith, U.; Tarkowski, A. Resistin, an Adipokine with Potent Proinflammatory Properties. J. Immunol. 2005, 174, 5789–5795. [Google Scholar] [CrossRef]
- Del Prete, A.; Salvi, V.; Sozzani, S. Adipokines as Potential Biomarkers in Rheumatoid Arthritis. Mediat. Inflamm. 2014, 2014, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Meier, F.M.P.; Frommer, K.W.; Peters, M.A.; Brentano, F.; Lefèvre, S.; Schröder, D.; Kyburz, D.; Steinmeyer, J.; Rehart, S.; Gay, S.; et al. Visfatin/Pre-B-cell Colony-enhancing Factor (PBEF), a Proinflammatory and Cell Motility-changing Factor in Rheumatoid Arthritis. J. Biol. Chem. 2012, 287, 28378–28385. [Google Scholar] [CrossRef] [Green Version]
- Johansson, L.; Pratesi, F.; Brink, M.; Ärlestig, L.; D’Amato, C.; Bartaloni, D.; Migliorini, P.; Rantapää-Dahlqvist, S. Antibodies directed against endogenous and exogenous citrullinated antigens pre-date the onset of rheumatoid arthritis. Arthritis Res. 2016, 18, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Rantapää-Dahlqvist, S.; De Jong, B.A.W.; Berglin, E.; Hallmans, G.; Wadell, G.; Stenlund, H.; Sundin, U.; Van Venrooij, W.J. Antibodies against cyclic citrullinated peptide and IgA rheumatoid factor predict the development of rheumatoid arthritis. Arthritis Rheum. 2003, 48, 2741–2749. [Google Scholar] [CrossRef]
- Zhang, Y.; Peltonen, M.; Andersson-Assarsson, J.; Svensson, P.-A.; Herder, C.; Rudin, A.; Carlsson, L.; Maglio, C. Elevated adiponectin predicts the development of rheumatoid arthritis in subjects with obesity. Scand. J. Rheumatol. 2020, 49, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Maglio, C.; Zhang, Y.; Peltonen, M.; Andersson-Assarsson, J.; Svensson, P.-A.; Herder, C.; Rudin, A.; Carlsson, L. Bariatric surgery and the incidence of rheumatoid arthritis—A Swedish Obese Subjects study. Rheumatology 2020, 59, 303–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linauskas, A.; Overvad, K.; Symmons, D.; Johansen, M.B.; Stengaard-Pedersen, K.; de Thurah, A. Body Fat Percentage, Waist Circumference, and Obesity As Risk Factors for Rheumatoid Arthritis: A Danish Cohort Study. Arthritis Rheum. 2018, 71, 777–786. [Google Scholar] [CrossRef]
- Folco, E.J.; Rocha, V.Z.; López-Ilasaca, M.; Libby, P. Adiponectin Inhibits Pro-inflammatory Signaling in Human Macrophages Independent of Interleukin-10. J. Biol. Chem. 2009, 284, 25569–25575. [Google Scholar] [CrossRef] [Green Version]
- Senolt, L.; Pavelka, K.; Housa, D.; Haluzik, M. Increased adiponectin is negatively linked to the local inflammatory process in patients with rheumatoid arthritis. Cytokine 2006, 35, 247–252. [Google Scholar] [CrossRef]
- Lee, Y.-A.; Hahm, D.-H.; Kim, J.Y.; Sur, B.; Lee, H.M.; Ryu, C.J.; Yang, H.-I.; Kim, K.S. Potential therapeutic antibodies targeting specific adiponectin isoforms in rheumatoid arthritis. Arthritis Res. 2018, 20, 245. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Aldridge, J.; Vasileiadis, G.K.; Edebo, H.; Ekwall, A.-K.H.; Lundell, A.-C.; Rudin, A.; Maglio, C. Recombinant Adiponectin Induces the Production of Pro-Inflammatory Chemokines and Cytokines in Circulating Mononuclear Cells and Fibroblast-Like Synoviocytes From Non-Inflamed Subjects. Front. Immunol. 2021, 11, 569883. [Google Scholar] [CrossRef]
- Vasileiadis, G.; Lundell, A.-C.; Zhang, Y.; Andersson, K.; Gjertsson, I.; Rudin, A.; Maglio, C. Adipocytokines in Untreated Newly Diagnosed Rheumatoid Arthritis: Association with Circulating Chemokines and Markers of Inflammation. Biomolecules 2021, 11, 325. [Google Scholar] [CrossRef] [PubMed]
- Sjöström, L.; Narbro, K.; Sjöström, C.D.; Karason, K.; Larsson, B.; Wedel, H.; Lystig, T.; Sullivan, M.; Bouchard, C.; Carlsson, B.; et al. Effects of Bariatric Surgery on Mortality in Swedish Obese Subjects. N. Engl. J. Med. 2007, 357, 741–752. [Google Scholar] [CrossRef] [Green Version]
- Sjöström, L.; Larsson, B.; Backman, L.; Bengtsson, C.; Bouchard, C.; Dahlgren, S.; Hallgren, P.; Jonsson, E.; Karlsson, J.; Lapidus, L. Swedish obese subjects (SOS). Recruitment for an intervention study and a selected description of the obese state. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 1992, 16, 465–479. [Google Scholar]
- Zenténius, E.; Andersson-Assarsson, J.; Carlsson, L.M.; Svensson, P.-A.; Larsson, I. Self-Reported Weight-Loss Methods and Weight Change: Ten-Year Analysis in the Swedish Obese Subjects Study Control Group. Obesity 2018, 26, 1137–1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ludvigsson, J.F.; Almqvist, C.; Bonamy, A.-K.E.; Ljung, R.; Michaëlsson, K.; Neovius, M.; Stephansson, O.; Ye, W. Registers of the Swedish total population and their use in medical research. Eur. J. Epidemiol. 2016, 31, 125–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, C. Propensity Score Matching in Nonrandomized Studies: A Concept Simply Explained Using Antidepressant Treatment During Pregnancy as an Example. J. Clin. Psychiatry 2017, 78, e162–e165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnett, F.C.; Edworthy, S.M.; Bloch, D.A.; McShane, D.J.; Fries, J.F.; Cooper, N.S.; Healey, L.A.; Kaplan, S.R.; Liang, M.H.; Luthra, H.S.; et al. The american rheumatism association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988, 31, 315–324. [Google Scholar] [CrossRef]
- Herder, C.; Peltonen, M.; Svensson, P.-A.; Carstensen, M.; Jacobson, P.; Roden, M.; Sjöström, L.; Carlsson, L. Adiponectin and Bariatric Surgery: Associations With Diabetes and Cardiovascular Disease in the Swedish Obese Subjects Study. Diabetes Care 2014, 37, 1401–1409. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristic | Cases (n = 82) | Matched Controls (n = 410) | p-Value |
|---|---|---|---|
| Age, years * | 48 ± 6 | 48 ± 6 | 0.91 |
| Men, No (%) * | 17 (21) | 85 (21) | 0.99 |
| BMI, kg/m2 * | 42 ± 5 | 41 ± 4 | 0.60 |
| Surgery group, No (%) * | 43 (52) | 218 (53) | 0.90 |
| Current or previous smoking, No (%) * | 18 (22) | 85 (21) | 0.80 |
| Diabetes, No (%) | 7 (9) | 45 (11) | 0.50 |
| CRP, mg/L | 10 ± 12 | 7 ± 7 | 0.001 |
| ESR, mm/h | 18 ± 11 | 15 ± 10 | 0.048 |
| Adiponectin, ng/mL | 9041 ± 4766 | 8068 ± 4622 | 0.08 |
| Leptin, ng/mL | 45 ± 32 | 49 ± 29 | 0.26 |
| Resistin, ng/mL | 12 ± 6 | 12 ± 6 | 0.84 |
| Visfatin, ng/mL | 2.8 ± 2.3 | 2.6 ± 1.9 | 0.35 |
| Characteristic | Cases (n = 88) | Matched Controls (n = 88) | p-Value |
|---|---|---|---|
| Age, years * | 56 ± 10 | 55 ± 10 | 0.54 |
| Men, No (%) * | 20 (23) | 20 (23) | 1.00 |
| BMI, kg/m2 | 26 ± 4 | 26 ± 3 | 0.56 |
| Current or previous smoking, No (%) | 43 (49) | 28 (32) ** | 0.03 |
| Adiponectin, ng/mL | 7482 ± 4936 | 6628 ± 4654 | 0.18 |
| Leptin, ng/mL | 21 ± 17 | 20 ± 19 | 0.44 |
| Resistin, ng/mL | 6.7 ± 3.5 | 6.9 ± 2.8 | 0.42 |
| A. Model 1 | OR | 95% CI | p-Value |
| Adiponectin, per 1000 ng/mL | 1.05 | 1.00–1.10 | 0.05 |
| Leptin, per 10 ng/mL | 0.93 | 0.84–1.03 | 0.16 |
| Resistin, per 10 ng/mL | 0.93 | 0.59–1.47 | 0.75 |
| Visfatin, per 1 ng/mL | 1.07 | 0.95–1.21 | 0.29 |
| B. Model 2 | OR | 95% CI | p-Value |
| Adiponectin, per 1000 ng/mL | 1.06 | 1.01–1.12 | 0.02 |
| Leptin, per 10 ng/mL | 0.92 | 0.83–1.02 | 0.13 |
| Resistin, per 10 ng/mL | 0.67 | 0.40–1.15 | 0.15 |
| Visfatin, per 1 ng/mL | 1.04 | 0.91–1.19 | 0.57 |
| CRP, per 10 mg/L | 1.67 | 1.17–2.42 | 0.01 |
| ESR, per 10 mm/h | 1.14 | 0.88–1.48 | 0.32 |
| Characteristic | OR | 95% CI | p-Value |
|---|---|---|---|
| A. | |||
| Adiponectin, per 1000 ng/mL | 1.05 | 0.98–1.13 | 0.19 |
| Leptin, per 10 ng/mL | 1.01 | 0.99–1.03 | 0.56 |
| Resistin, per 10 ng/mL | 0.75 | 0.85–1.12 | 0.75 |
| Smoking, yes/no | 2.27 | 1.12–4.62 | 0.02 |
| B. BMI ≤ 25 kg/m2 | |||
| Adiponectin, per 1000 ng/mL | 1.02 | 0.94–1.11 | 0.64 |
| Leptin, per 10 ng/mL | 1.00 | 0.93–1.07 | 0.92 |
| Resistin, per 10 ng/mL | 1.05 | 0.85–1.29 | 0.68 |
| Women, yes/no | 1.42 | 0.25–8.03 | 0.69 |
| Age, per 1 year | 0.99 | 0.94–1.05 | 0.79 |
| Smoking, yes/no | 2.04 | 0.72–5.81 | 0.18 |
| C. BMI > 25 kg/m2 | |||
| Adiponectin, per 1000 ng/mL | 1.17 | 1.01–1.36 | 0.03 |
| Leptin, per 10 ng/mL | 1.00 | 0.98–1.03 | 0.94 |
| Resistin, per 10 ng/mL | 0.98 | 0.87–1.09 | 0.69 |
| Women, yes/no | 0.84 | 0.25–2.78 | 0.77 |
| Age, per 1 year | 1.00 | 0.97–1.05 | 0.70 |
| Smoking, yes/no | 1.63 | 0.71–3.72 | 0.25 |
| Characteristic | Cases | Matched Controls | p-Value |
|---|---|---|---|
| BMI ≤ 25 | n = 30 | n = 37 | |
| Age, years | 53 ± 11 | 54 ± 9 | 0.67 |
| Women, No (%) | 26 (87) | 32 (87) | 0.64 |
| BMI, Kg/m2 | 22 ± 2 | 23 ± 1 | 0.13 |
| Current or previous smoking, No (%) | 15 (50) | 12 (32) | 0.15 |
| Adiponectin, ng/mL | 9233 ± 6575 | 8708 ± 5921 | 0.73 |
| Leptin, ng/mL | 13 ± 8 | 12 ± 9 | 0.79 |
| Resistin, ng/mL | 6.9 ± 2.5 | 6.8 ± 2.5 | 0.99 |
| BMI > 25 | n = 58 | n = 51 | |
| Age, years | 57 ± 9 | 57 ± 10 | 0.63 |
| Women, No (%) | 42 (72) | 36 (71) | 0.83 |
| BMI, Kg/m2 | 28 ± 3 | 28 ± 3 | 0.76 |
| Current or previous smoking, No (%) | 28 (48) | 16 (31) * | 0.09 |
| Adiponectin, ng/mL | 6575 ± 3570 | 5118 ± 2630 | 0.02 |
| Leptin, ng/mL | 25 ± 18 | 26 ± 22 | 0.80 |
| Resistin, ng/mL | 6.7 ± 3.9 | 6.9 ± 2.5 | 0.74 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Johansson, L.; Andersson-Assarsson, J.; Taube, M.; Peltonen, M.; Svensson, P.-A.; Herder, C.; Rudin, A.; Carlsson, L.; Rantapää-Dahlqvist, S.; et al. Adiponectin Associates with Rheumatoid Arthritis Risk in Overweight and Obesity Independently of Other Adipokines. J. Clin. Med. 2021, 10, 2791. https://doi.org/10.3390/jcm10132791
Zhang Y, Johansson L, Andersson-Assarsson J, Taube M, Peltonen M, Svensson P-A, Herder C, Rudin A, Carlsson L, Rantapää-Dahlqvist S, et al. Adiponectin Associates with Rheumatoid Arthritis Risk in Overweight and Obesity Independently of Other Adipokines. Journal of Clinical Medicine. 2021; 10(13):2791. https://doi.org/10.3390/jcm10132791
Chicago/Turabian StyleZhang, Yuan, Linda Johansson, Johanna Andersson-Assarsson, Magdalena Taube, Markku Peltonen, Per-Arne Svensson, Christian Herder, Anna Rudin, Lena Carlsson, Solbritt Rantapää-Dahlqvist, and et al. 2021. "Adiponectin Associates with Rheumatoid Arthritis Risk in Overweight and Obesity Independently of Other Adipokines" Journal of Clinical Medicine 10, no. 13: 2791. https://doi.org/10.3390/jcm10132791
APA StyleZhang, Y., Johansson, L., Andersson-Assarsson, J., Taube, M., Peltonen, M., Svensson, P.-A., Herder, C., Rudin, A., Carlsson, L., Rantapää-Dahlqvist, S., & Maglio, C. (2021). Adiponectin Associates with Rheumatoid Arthritis Risk in Overweight and Obesity Independently of Other Adipokines. Journal of Clinical Medicine, 10(13), 2791. https://doi.org/10.3390/jcm10132791