
Optimal Upfront Treatment in Surgically Resectable Pancreatic Cancer Candidates: A High-Volume Center Retrospective Analysis

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Acquisition and Cohort Details
2.2. Statistical Analysis
2.3. Institutional Ethics
3. Results
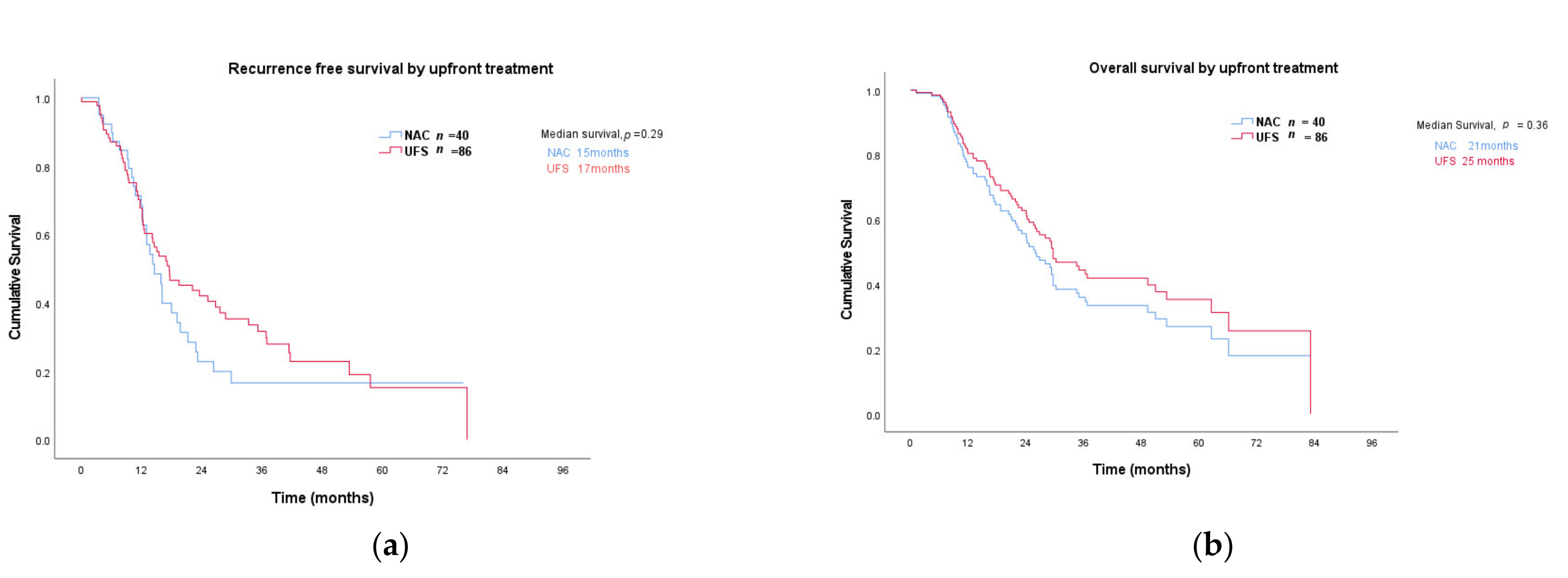
3.1. Survival
3.2. Upfront Radiological Stage and Location
3.3. Surgical Outcomes
3.4. Prognostic Factors
3.4.1. CA 19-9 and Imaging
3.4.2. Histopathological Markers
3.4.3. Chemotherapy Regimen
3.5. Predictive Markers of Chemotherapy Response in Patients Treated with NAC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Chemotherapy | Upfront Group: Neoadjuvant Chemotherapy | Upfront Group: Upfront Surgery |
|---|---|---|
| Neoadjuvant chemotherapy | ||
| Folfirinox | 12 | N/A |
| Gemcitabine + Nab-Paclitaxel | 25 | |
| Gemcitabine + capecitabine | 1 | |
| Gemcitabine alone | 2 | |
| Median duration weeks (range) | 8 (3–26) | N/A |
| Adjuvant chemotherapy | ||
| Folfirinox | 2 | |
| Gemcitabine + Nab-Paclitaxel | 1 | 4 |
| Gemcitabine + capecitabine | 4 | 24 |
| Gemcitabine alone | 11 | 36 |
| Capecitabine alone | 9 | 1 |
| S1 | 1 | |
| Unknown | 1 | |
| Median duration weeks (range) | 16 (3–24) | 24 (4–52) |
References
- Australian Institute of Health and Welfare. Cancer in Australia. Available online: https://www.aihw.gov.au/reports/cancer/cancer-in-australia-2019/contents/summary (accessed on 1 February 2020).
- Lekka, K.; Tzitzi, E.; Giakoustidis, A.; Papadopoulos, V.; Giakoustidis, D. Contemporary management of borderline resectable pancreatic ductal adenocarcinoma. Ann. Hepatobiliary Pancreat. Surg. 2019, 23, 97–108. [Google Scholar] [CrossRef]
- Allen, P.J.; Kuk, D.; Castillo, C.F.; Basturk, O.; Wolfgang, C.L.; Cameron, J.L.; Lillemoe, K.D.; Ferrone, C.R.; Morales-Oyarvide, V.; He, J.; et al. Multi-institutional validation study of the American Joint Commission on Cancer (8th edition) changes for T and N staging in patients with pancreatic adenocarcinoma. Ann. Surg. 2017, 265, 185–191. [Google Scholar] [CrossRef]
- Bergenfeldt, M.; Albertsson, M. Current state of adjuvant therapy in resected pancreatic adenocarcinoma. Acta Oncol. 2006, 45, 124–135. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Pancreatic Adenocarcinoma. Available online: https://www.nccn.org/professionals/physician_gls/pdf/pancreatic_blocks.pdf (accessed on 20 February 2020).
- Janssen, Q.P.; Buettner, S.; Suker, M.; Beumer, B.R.; Addeo, P.; Bachellier, P.; Bahary, N.; Bekaii-Saab, T.; Bali, M.A.; Besselink, M.G.; et al. Neoadjuvant FOLFIRINOX in patients with borderline resectable pancreatic cancer: A systematic review and patient-level meta-analysis. J. Natl. Cancer Inst. 2019, 111, 782–794. [Google Scholar] [CrossRef]
- Scheufele, F.; Hartmann, D.; Friess, H. Treatment of pancreatic cancer-neoadjuvant treatment in borderline resectable/locally advanced pancreatic cancer. Transl. Gastroenterol. Hepatol. 2019, 4, 32. [Google Scholar] [CrossRef]
- Casadei, R.; Di Marco, M.; Ricci, C.; Santini, D.; Serra, C.; Calculli, L.; D’Ambra, M.; Guido, A.; Morselli-Labate, A.M.; Minni, F. Neoadjuvant chemoradiotherapy and surgery versus surgery alone in resectable pancreatic cancer: A single-center prospective, randomized, controlled trial which failed to achieve accrual targets. J. Gastrointest. Surg. 2015, 19, 1802–1812. [Google Scholar] [CrossRef]
- Golcher, H.; Brunner, T.B.; Witzigmann, H.; Marti, L.; Bechstein, W.O.; Bruns, C.; Jungnickel, H.; Schreiber, S.; Grabenbauer, G.G.; Meyer, T.; et al. Neoadjuvant chemoradiation therapy with gemcitabine/cisplatin and surgery versus im-mediate surgery in resectable pancreatic cancer: Results of the first prospective randomized phase II trial. Strahlenther. Onkol. 2015, 191, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Satoi, S.; Unno, M.; Motoi, F.; Matsuyama, Y.; Matsumoto, I.; Aosasa, S.; Shirakawa, H.; Wada, K.; Fujii, T.; Yoshitomi, H.; et al. The effect of neoadjuvant chemotherapy with gemcitabine and S-1 for resectable pancreatic cancer (randomized phase II/III trial; Prep-02/JSAP-05). J. Clin. Oncol. 2019, 37, 4126. [Google Scholar] [CrossRef]
- Petrelli, F.; Coinu, A.; Borgonovo, K.; Cabiddu, M.; Ghilardi, M.; Lonati, V.; Aitini, E.; Barni, S.; Gruppo Italiano per lo Studio dei Carcinomi dell’Aparato Digerente. FOLFIRINOX-based neoadjuvant therapy in borderline resectable or unresectable pancreatic cancer: A meta-analytical review of published studies. Pancreas 2015, 44, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Versteijne, E.; Suker, M.; Groothuis, K.; Akkermans-Vogelaar, J.M.; Besselink, M.G.; Bonsing, B.A.; Buijsen, J.; Busch, O.R.; Creemers, G.-J.M.; van Dam, R.M.; et al. Preoperative chemoradiotherapy versus immediate surgery for resectable and borderline resectable pancreatic cancer: Results of the Dutch randomized phase III PREOPANC Trial. J. Clin. Oncol. 2020, 38, 1763–1773. [Google Scholar] [CrossRef]
- Shridhar, R.; Takahashi, C.; Huston, J.; Meredith, K.L. Neoadjuvant therapy and pancreatic cancer: A national cancer database analysis. J. Gastrointest. Oncol. 2019, 10, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Waddell, N.; Pajic, M.; Patch, A.-M.; Chang, D.K.; Kassahn, K.S.; Bailey, P.; Johns, A.L.; Miller, D.; Nones, K.; Quek, K.; et al. Whole genomes redefine the mutational landscape of pancreatic cancer. Nature 2015, 518, 495–501. [Google Scholar] [CrossRef]
- Barreto, S.G.; Shukla, P.J.; Shrikhande, S.V. Tumors of the pancreatic body and tail. World J. Oncol. 2010, 1, 52–65. [Google Scholar] [CrossRef] [PubMed]
- Artinyan, A.; Soriano, P.A.; Prendergast, C.; Low, T.; Ellenhorn, J.D.I.; Kim, J. The anatomic location of pancreatic cancer is a prognostic factor for survival. HPB 2008, 10, 371–376. [Google Scholar] [CrossRef]
- Itchins, M.; Arena, J.; Nahm, C.B.; Rabindran, J.; Kim, S.; Gibbs, E.; Bergamin, S.; Chua, T.C.; Gill, A.J.; Maher, R.; et al. Retrospective cohort analysis of neo-adjuvant treatment and survival in resectable and borderline resectable pancreatic ductal adenocarcinoma in a high volume referral centre. Eur. J. Surg. Oncol. 2017, 43, 1711–1717. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, L.H.; Litière, S.; de Vries, E.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. RECIST 1.1—Update and clarification: From the RECIST committee. Eur. J. Cancer 2016, 62, 132–137. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Strobel, O.; Hank, T.; Hinz, U.; Bergmann, F.; Schneider, L.; Springfeld, C.; Jäger, D.; Schirmacher, P.; Hackert, T.; Büchler, M.W. Pancreatic cancer surgery: The new R-status counts. Ann. Surg. 2017, 265, 565–573. [Google Scholar] [CrossRef]
- Cong, L.; Liu, Q.; Zhang, R.; Cui, M.; Zhang, X.; Gao, X.; Guo, J.; Dai, M.; Zhang, T.; Liao, Q.; et al. Tumor size classification of the 8th edition of TNM staging system is superior to that of the 7th edition in predicting the survival outcome of pancreatic cancer patients after radical resection and adjuvant chemotherapy. Sci. Rep. 2018, 8, 10383. [Google Scholar] [CrossRef]
- Townend, P.; de Reuver, P.R.; Chua, T.C.; Mittal, A.; Clark, S.J.; Pavlakis, N.; Gill, A.J.; Samra, J.S. Histopathological tumour viability after neoadjuvant chemotherapy influences survival in resected pancreatic cancer: Analysis of early out-come data. ANZ J. Surg. 2018, 88, E167–E172. [Google Scholar] [CrossRef]
- Schellenberg, D.; Quon, A.; Minn, A.Y.; Graves, E.E.; Kunz, P.; Ford, J.M.; Fisher, G.A.; Goodman, K.A.; Koong, A.C.; Chang, D.T. 18Fluorodeoxyglucose PET is prognostic of progression-free and overall survival in locally advanced pancreas cancer treated with stereotactic radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 1420–1425. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council; Australian Research Council; Universities Australia. National Statement on Ethical Conduct in Human Research; Commonwealth of Australia: Canberra, ACT, Australia, 2007.
- Isaji, S.; Mizuno, S.; Windsor, J.A.; Bassi, C.; Fernández-Del Castillo, C.; Hackert, T.; Hayasaki, A.; Katz, M.H.G.; Kim, S.-W.; Kishiwada, M.; et al. International consensus on definition and criteria of borderline resectable pancreatic ductal adenocarcinoma 2017. Pancreatology 2018, 18, 2–11. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Palmer, D.H.; Ghaneh, P.; Psarelli, E.E.; Valle, J.W.; Halloran, C.M.; Faluyi, O.; O’Reilly, D.A.; Cunningham, D.; Wadsley, J.; et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine mono-therapy in patients with resected pancreatic cancer (ESPAC-4): A multicentre, open-label, randomised, phase 3 trial. Lancet 2017, 389, 1011–1024. [Google Scholar] [CrossRef]
- Valle, J.W.; Palmer, D.; Jackson, R.; Cox, T.; Neoptolemos, J.P.; Ghaneh, P.; Rawcliffe, C.L.; Bassi, C.; Stocken, D.D.; Cunningham, D.; et al. Optimal duration and timing of adjuvant chemotherapy after definitive surgery for ductal adenocarcinoma of the pancreas: Ongoing lessons from the ESPAC-3 study. J. Clin. Oncol. 2014, 32, 504–512. [Google Scholar] [CrossRef]
- Versteijne, E.; Vogel, J.A.; Besselink, M.G.; Busch, O.R.C.; Wilmink, J.W.; Daams, J.G.; van Eijck, C.H.J.; Koerkamp, B.G.; Rasch, C.R.N.; van Tienhoven, G. Meta-analysis comparing upfront surgery with neoadjuvant treatment in patients with resectable or borderline resectable pancreatic cancer. Br. J. Surg. 2018, 105, 946–958. [Google Scholar] [CrossRef] [PubMed]
- Uhl, W.; Ettrich, T.J.; Reinacher-Schick, A.C.; Algül, H.; Friess, H.; Kornmann, M.; Koenig, A.; Ghadimi, M.; Wittel, U.A.; Gallmeier, E.; et al. NEONAX trial: Neoadjuvant plus adjuvant or only adjuvant nab-paclitaxel plus gemcitabine for resectable pancreatic cancer, a phase II study of the AIO pancreatic cancer group (AIO-PAK-0313)—Safety interim analysis. J. Clin. Oncol. 2019, 37, 4128. [Google Scholar] [CrossRef]
- Dreyer, S.B.; Pinese, M.; Jamieson, N.B.; Scarlett, C.J.; Colvin, E.K.; Pajic, M.; Johns, A.L.; Humphris, J.L.; Wu, J.; Cowley, M.J.; et al. Precision oncology in surgery: Patient selection for operable pancreatic cancer. Ann. Surg. 2020, 272, 366–376. [Google Scholar] [CrossRef]
- Nahm, C.; Turchini, J.; Chou, A.; Colvin, E.; Howell, V.; Samra, J.; Gill, A.; Mittal, A. Matching treatment strategies to clinical phenotype: Biomarker-driven selection for neoadjuvant therapy in pancreatic cancer. HPB 2019, 21, S200. [Google Scholar] [CrossRef][Green Version]
- Nahm, C.B.; Turchini, J.; Jamieson, N.; Moon, E.; Sioson, L.; Itchins, M.; Arena, J.; Colvin, E.; Howell, V.M.; Pavlakis, N.; et al. Biomarker panel predicts survival after resection in pancreatic ductal adenocarcinoma: A multi-institutional cohort study. Eur. J. Surg. Oncol. 2019, 45, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Sahni, S.; Nahm, C.; Krisp, C.; Molloy, M.P.; Mehta, S.; Maloney, S.; Itchins, M.; Pavlakis, N.; Clarke, S.; Chan, D.; et al. Identification of novel biomarkers in pancreatic tumor tissue to predict response to neoadjuvant chemotherapy. Front. Oncol. 2020, 10, 237. [Google Scholar] [CrossRef]



| Neoadjuvant Chemotherapy | Upfront Surgery | |
|---|---|---|
| Median age (years, range) | 71 (42–85) | 69 (41–90) |
| Sex | ||
| F | 20 | 53 |
| M | 20 | 33 |
| Upfront radiological stage a | ||
| 1a | 12 | 32 |
| 1b | 26 | 41 |
| 2a | 2 | 5 |
| 2b | 8 | |
| Total | 40 | 86 |
| Tumor location | ||
| Head | 38 | 63 |
| Body/tail | 2 | 23 |
| RFS | Univariate | Multivariate | OS | Univariate | Multivariate | |||
|---|---|---|---|---|---|---|---|---|
| p-Value | Hazard Ratio (HR) (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | |
| Initial CA19-9 ≥ 500 kU/L | 0.33 | 1.3 (0.77–2.19) | 0.95 | 5.51 (0–5.621) | 0.06 | 1.7 (0.99–2.92) | 0.63 | 3.66 (0–3.2833) |
| Radiological stage | 0.11 | 0.78 (0.58–1.06 | 0.95 | 0.18 (1.7820) | 0.36 | 0.87 (0.64–1.2) | 0.44 | 2.995 (0–3.1619) |
| Viability (%) | * 0.04 | 1.02 (1–1.03) | 0.79 | 0.99 (0.9–1.08) | * 0.004 | 1.03 (1.01–1.047) | 0.92 | 1.07 (0.27–4.239) |
| Grade | * 0.005 | 1.8 (1.2–2.72) | 0.58 | 1.79 (2.741) | * 0.017 | 1.7 (1.10–2.73) | 0.29 | 5.8612 (0–2.5736) |
| Baseline FDG PET ≥ 5 | * 0.02 | 2.4 (1.12–4.49) | 0.88 | 0 (0–3.077) | * 0.007 | 3.4 (1.40–8.33) | 0.73 | 694 (0–1.7819) |
| Surgical stage T a | 0.12 | 1.3 (0.94–1.78) | 0.81 | 0 (0–4.527) | * 0.02 | 1.6 (1.08–2.48) | 0.88 | 65.6 (0–7.4224) |
| Surgical stage N a | * 0.01 | 1.4 (1.09–1.99) | 0.86 | 9.6 (0–3.611) | 0.05 | 1.4 (1.00–1.95) | 0.57 | 0.1 (0–9.244) |
| Perineural invasion | 0.18 | 1.4 (0.86–2.36) | 0.79 | 1.84 (0–8.835) | 0.51 | 1.2 (0.7–2.04) | 0.38 | 1.1916 (0–2.0452) |
| Small/large vessel invasion | 0.14 | 1.4 (0.89–2.16) | 0.67 | 1.39 (0–2.951) | * 0.001 | 2.4 (1.4–4.08) | 0.26 | 1.515 (0–6.2241) |
| R1 | * 0.049 | 1.5 (1.002–2.40) | 0.73 | 75 (0–4.312) | 0.21 | 1.4 (0.84–2.1) | 0.39 | 1.366 (0–9.8419) |
| NAC GEM/ABR | 0.28 | 0.65 (0.30–1.42) | 0.88 | 2.6 (0–5.65) | 0.25 | 0.59 (0.24–1.45) | 0.62 | 44.17 (0–1.58) |
| NAC ≥ 12 weeks | 0.29 | 0.95 (0.87–1.04) | 0.98 | 0.20 (0–6.351) | 0.26 | 0.60 (0.25–1.46) | 0.66 | 0 (0–1.7918) |
| AC GEM/CAPE | 0.06 | 0.76 (0.58–1.01) | 0.97 | 10.9 (0–1.448) | * 0.01 | 0.60 (0.41–0.88) | 0.74 | 2.63 (0–4.4823) |
| AC ≥ 24 weeks | * 0.007 | 0.50 (0.30–0.82) | 0.93 | 0.43 (0–1.1630) | * 0.0002 | 0.33 (0.19–0.59) | 0.96 | 0.38 (0–6.610) |
| p-Value | Correlation Coefficient (Spearmans) | |
|---|---|---|
| CT response-RECIST a | 0.72 | 0.317 |
| Baseline CA 19-9 ≥ 500 | 0.28 | −0.18 |
| Pre-operative CA 19-9 ≥ 500 | 0.32 | −0.17 |
| Initial SUVmax: ≥5 | * 0.023 | 0.369 |
| Pre-operative SUVmax: ≥5 | 0.45 | 0.175 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maloney, S.; Itchins, M.; Arena, J.; Sahni, S.; Howell, V.M.; Hayes, S.A.; Gill, A.J.; Clarke, S.J.; Samra, J.; Mittal, A.; et al. Optimal Upfront Treatment in Surgically Resectable Pancreatic Cancer Candidates: A High-Volume Center Retrospective Analysis. J. Clin. Med. 2021, 10, 2700. https://doi.org/10.3390/jcm10122700
Maloney S, Itchins M, Arena J, Sahni S, Howell VM, Hayes SA, Gill AJ, Clarke SJ, Samra J, Mittal A, et al. Optimal Upfront Treatment in Surgically Resectable Pancreatic Cancer Candidates: A High-Volume Center Retrospective Analysis. Journal of Clinical Medicine. 2021; 10(12):2700. https://doi.org/10.3390/jcm10122700
Chicago/Turabian StyleMaloney, Sarah, Malinda Itchins, Jennifer Arena, Sumit Sahni, Viive M. Howell, Sarah A. Hayes, Anthony J. Gill, Stephen J. Clarke, Jaswinder Samra, Anubhav Mittal, and et al. 2021. "Optimal Upfront Treatment in Surgically Resectable Pancreatic Cancer Candidates: A High-Volume Center Retrospective Analysis" Journal of Clinical Medicine 10, no. 12: 2700. https://doi.org/10.3390/jcm10122700
APA StyleMaloney, S., Itchins, M., Arena, J., Sahni, S., Howell, V. M., Hayes, S. A., Gill, A. J., Clarke, S. J., Samra, J., Mittal, A., & Pavlakis, N. (2021). Optimal Upfront Treatment in Surgically Resectable Pancreatic Cancer Candidates: A High-Volume Center Retrospective Analysis. Journal of Clinical Medicine, 10(12), 2700. https://doi.org/10.3390/jcm10122700