The Efficacy of Injections for Partial Rotator Cuff Tears: A Systematic Review



Abstract
1. Introduction
2. Experimental Section
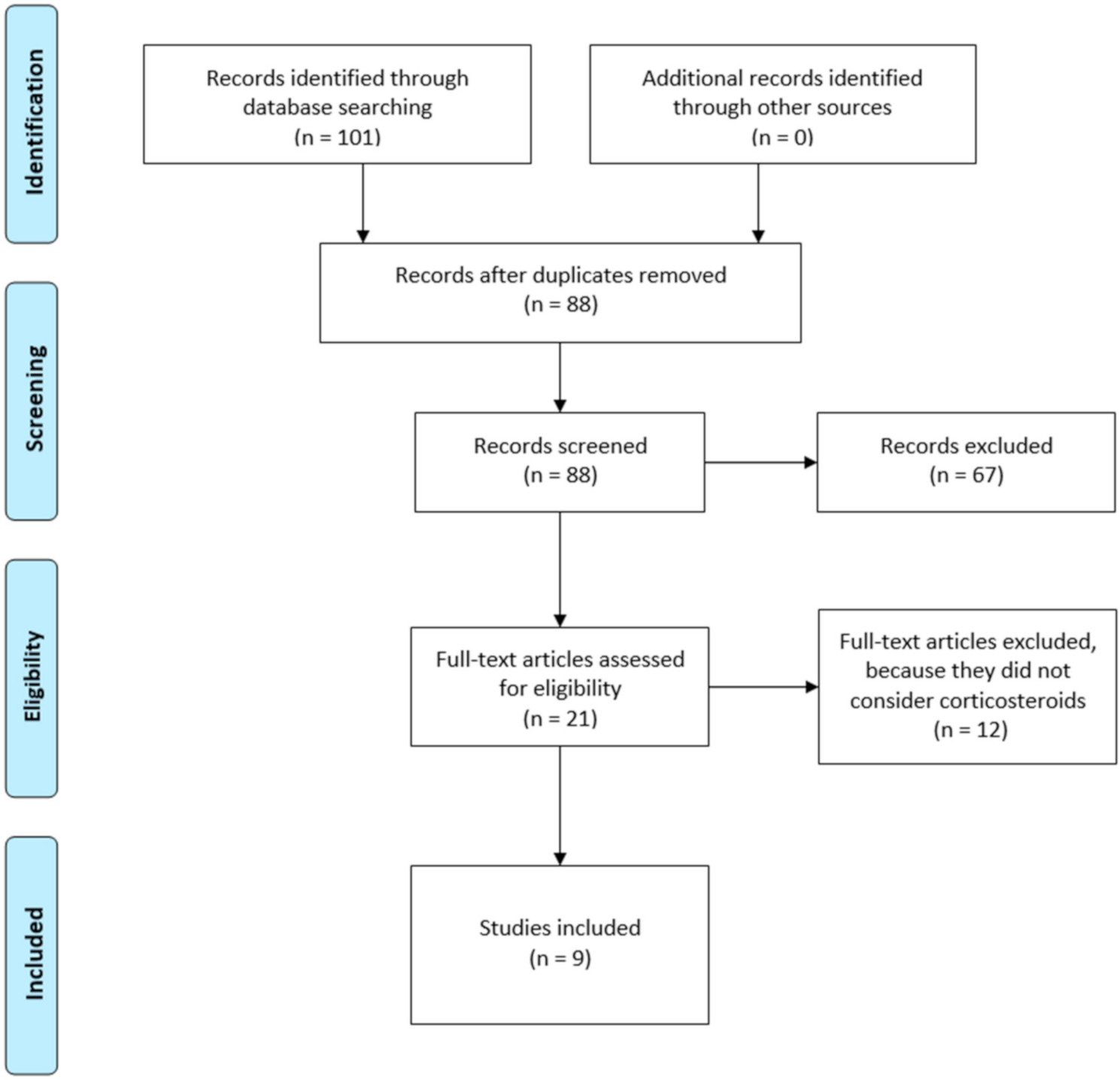
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Data Extraction
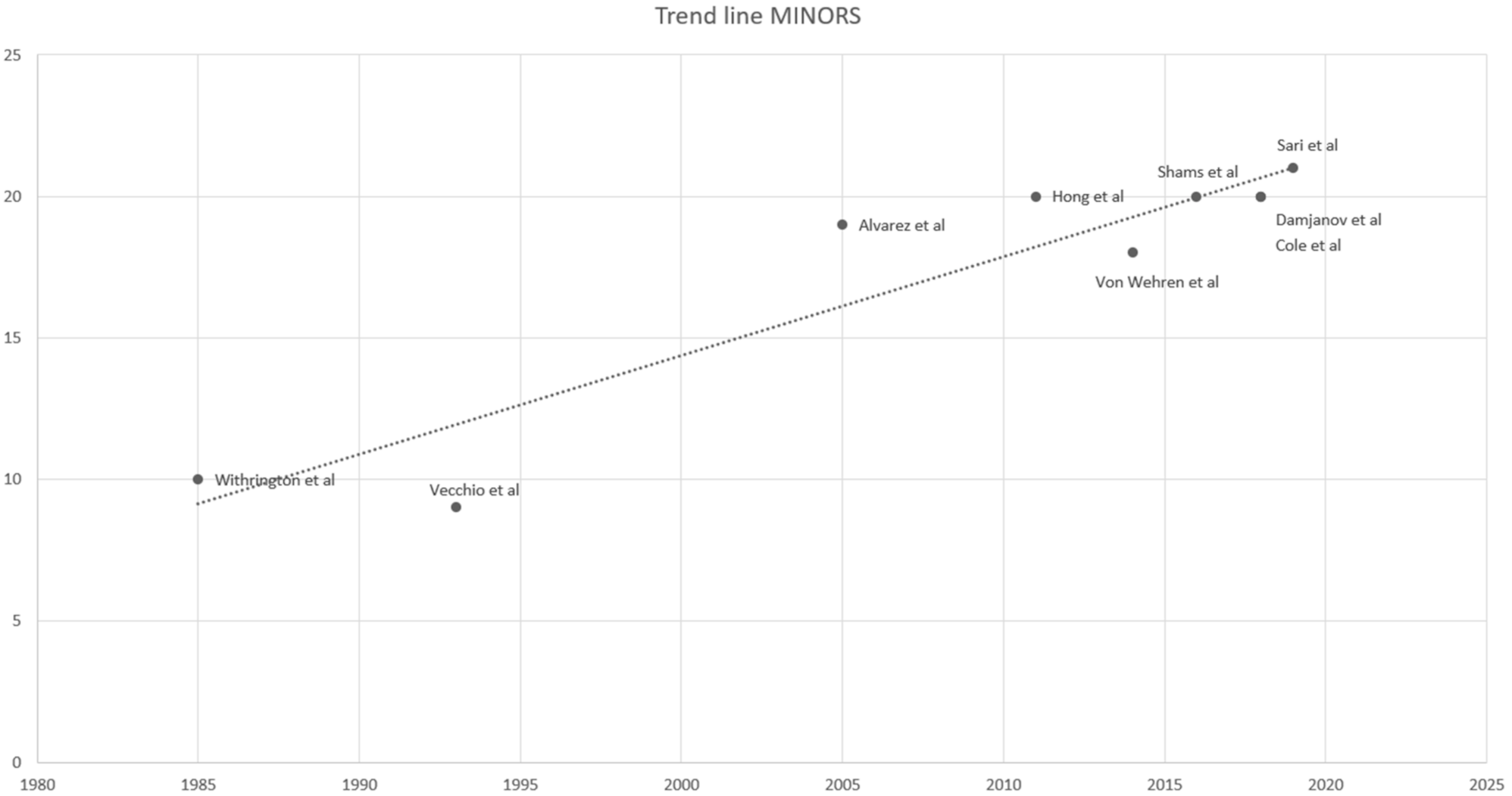
2.4. Study Quality
2.5. Statistical Analysis
3. Results
3.1. Interventions
3.2. Outcome Measures
3.3. Outcomes Data
3.4. Corticosteroids
3.5. PRP
3.6. Prolotherapy
3.7. Short-Term Follow-Up
3.8. Medium-Term Follow-Up
3.9. Long-Term Follow-Up
3.10. Complications
3.11. Methodological Quality
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lin, K.M.; Wang, D.; Dines, J.S. Injection Therapies for Rotator Cuff Disease. Orthop. Clin. North Am. 2018, 49, 231–239. [Google Scholar] [CrossRef]
- Sher, J.S.; Uribe, J.W.; Posada, A.; Murphy, B.J.; Zlatkin, M.B. Abnormal findings on magnetic resonance images of asymptomatic shoulders. J. Bone Joint Surg. Am. Vol. 1995, 77, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Reilly, P.; MacLeod, I.; Macfarlane, R.; Windley, J.; Emery, R.J.H. Dead Men and Radiologists Don’t Lie: A Review of Cadaveric and Radiological Studies of Rotator Cuff Tear Prevalence. Ann. R. Coll. Surg. Engl. 2006, 88, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Matthewson, G.; Beach, C.J.; Nelson, A.A.; Woodmass, J.M.; Ono, Y.; Boorman, R.S.; Lo, I.K.Y.; Thornton, G.M. Partial Thickness Rotator Cuff Tears: Current Concepts. Adv. Orthop. 2015, 2015, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, J.E. Exercise in the treatment of rotator cuff impingement: A systematic review and a synthesized evidence-based rehabilitation protocol. J. Shoulder Elb. Surg. 2009, 18, 138–160. [Google Scholar] [CrossRef] [PubMed]
- Desjardins-Charbonneau, A.; Roy, J.-S.; Dionne, C.E.; Frémont, P.; MacDermid, J.C.; Desmeules, F. The Efficacy of Manual Therapy for Rotator Cuff Tendinopathy: A Systematic Review and Meta-analysis. J. Orthop. Sports Phys. Ther. 2015, 45, 330–350. [Google Scholar] [CrossRef]
- Bertrand, H.; Reeves, K.D.; Bennett, C.J.; Bicknell, S.; Cheng, A.-L. Dextrose Prolotherapy Versus Control Injections in Painful Rotator Cuff Tendinopathy. Arch. Phys. Med. Rehabil. 2016, 97, 17–25. [Google Scholar] [CrossRef]
- Lin, M.-T.; Chiang, C.-F.; Wu, C.-H.; Huang, Y.-T.; Tu, Y.-K.; Wang, T.-G. Comparative Effectiveness of Injection Therapies in Rotator Cuff Tendinopathy: A Systematic Review, Pairwise and Network Meta-analysis of Randomized Controlled Trials. Arch. Phys. Med. Rehabil. 2019, 100, 336–349.e15. [Google Scholar] [CrossRef]
- Coombes, B.K.; Bisset, L.; Vicenzino, B. Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: A systematic review of randomised controlled trials. Lancet 2010, 376, 1751–1767. [Google Scholar] [CrossRef]
- De Palma, A. Surgery of the Shoulder; J.B. Lippincott & Co.: Philadelphia, PA, USA, 1983. [Google Scholar]
- Keyes, E.L. Observations on rupture of the supraspinatus tendon: Based upon a study of seventy-three cadavers. Ann. Surg. 2006, 97, 849–856. [Google Scholar] [CrossRef]
- Lindblom, K. On pathogenesis of ruptures of the tendon aponeurosis of the shoulder joint. Acta Radiol. 1939, 20, 563–577. [Google Scholar] [CrossRef]
- Uhthoff, H. The pathogenesis of the rotator cuff tears. In Proceedings of the 3rd International Conference on the Surgery of the Shoulder, Fukuoka, Japan, 1986; pp. 211–212. [Google Scholar]
- Pegreffi, F.; Paladini, P.; Campi, F.; Porcellini, G. Conservative management of rotator cuff tear. Sports Med. Arthrosc. Rev. 2011, 19, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Tillander, B.; Franzén, L.E.; Karlsson, M.H.; Norlin, R. Effect of steroid injections on the rotator cuff: An experimental study in rats. J. Shoulder Elb. Surg. 1999, 8, 271–274. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (MINORS): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Withrington, R.H.; Girgis, F.L.; Seifert, M.H. A Placebo-controlled Trial of Steroid Injections in the Treatment of Supraspinatus Tendonitis. Scand. J. Rheumatol. 1985, 14, 76–78. [Google Scholar] [CrossRef]
- Vecchio, P.; Hazleman, B.; King, R. A Double-Blind Trial Comparing Subacromial Methylprednisolone and Lignocalne in Acute Rotation Cuff Tendinits. Rheumatology 1993, 32, 743–745. [Google Scholar] [CrossRef]
- Alvarez, C.M.; Litchfield, R.; Jackowski, D.; Griffin, S.; Kirkley, A. A Prospective, Double-Blind, Randomized Clinical Trial Comparing Subacromial Injection of Betamethasone and Xylocaine to Xylocaine alone in Chronic Rotator Cuff Tendinosis. Am. J. Sports Med. 2005, 33, 255–262. [Google Scholar] [CrossRef]
- Hong, J.Y.; Yoon, S.-H.; Moon, D.J.; Kwack, K.-S.; Joen, B.; Lee, H.Y. Comparison of High- and Low-Dose Corticosteroid in Subacromial Injection for Periarticular Shoulder Disorder: A Randomized, Triple-Blind, Placebo-Controlled Trial. Arch. Phys. Med. Rehabil. 2011, 92, 1951–1960. [Google Scholar] [CrossRef]
- Von Wehren, L.; Blanke, F.; Todorov, A.; Heisterbach, P.; Sailer, J.; Majewski, M. The effect of subacromial injections of autologous conditioned plasma versus cortisone for the treatment of symptomatic partial rotator cuff tears. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3787–3792. [Google Scholar] [CrossRef]
- Shams, A.; El-Sayed, M.M.H.; Gamal, O.; Ewes, W. Subacromial injection of autologous platelet-rich plasma versus corticosteroid for the treatment of symptomatic partial rotator cuff tears. Eur. J. Orthop. Surg. Traumatol. 2016, 26, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Cole, B.; Lam, P.; Hackett, L.; Murrell, G.A.C. Ultrasound-guided injections for supraspinatus tendinopathy: Corticosteroid versus glucose prolotherapy—A randomized controlled clinical trial. Shoulder Elb. 2018, 10, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Damjanov, N.; Barac, B.; Colic, J.; Stevanovic, V.; Zekovic, A.; Tulic, G. The efficacy and safety of autologous conditioned serum (ACS) injections compared with betamethasone and placebo injections in the treatment of chronic shoulder joint pain due to supraspinatus tendinopathy: A prospective, randomized, double-blind, controlled study. Med Ultrason. 2018, 20, 335. [Google Scholar] [CrossRef] [PubMed]
- Sari, A.; Eroglu, A. Comparison of ultrasound-guided platelet-rich plasma, prolotherapy, and corticosteroid injections in rotator cuff lesions. J. Back Musculoskelet. Rehabil. 2020, 33, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.U.; Sun, Z.; Liao, B.; Song, Z.; Xiao, T.; Zhu, P. Sodium Hyaluronate and Platelet-Rich Plasma for Partial-Thickness Rotator Cuff Tears. Med. Sci. Sports Exerc. 2019, 51, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, K.; Tetro, A.; Blam, O.; Evanoff, B.A.; Teefey, S.A.; Middleton, W.D. Natural history of asymptomatic rotator cuff tears: A longitudinal analysis of asymptomatic tears detected sonographically. J. Shoulder Elb. Surg. 2001, 10, 199–203. [Google Scholar] [CrossRef]
- Duckworth, D.G.; Smith, K.L.; Campbell, B.; Matsen, F.A. Self-assessment questionnaires document substantial variability in the clinical expression of rotator cuff tears. J. Shoulder Elb. Surg. 1999, 8, 330–333. [Google Scholar] [CrossRef]
- Diercks, R.; Bron, C.; Dorrestijn, O.; Meskers, C.; Naber, R.; de Ruiter, T.; Willems, J.; Winters, J.; van der Woude, H. Guideline for diagnosis and treatment of subacromial pain syndrome: A multidisciplinary review by the Dutch Orthopaedic Association. Acta Orthop. 2014, 85, 314–322. [Google Scholar] [CrossRef]
- Bergeson, A.G.; Tashjian, R.Z.; Greis, P.E.; Crim, J.; Stoddard, G.J.; Burks, R.T. Effects of Platelet-Rich Fibrin Matrix on Repair Integrity of At-Risk Rotator Cuff Tears. Am. J. Sports Med. 2011, 40, 286–293. [Google Scholar] [CrossRef]
- Merolla, G.; Bianchi, P.; Porcellini, G. Ultrasound-guided subacromial injections of sodium hyaluronate for the management of rotator cuff tendinopathy: A prospective comparative study with rehabilitation therapy. Musculoskelet. Surg. 2013, 97, 49–56. [Google Scholar] [CrossRef]
- Haraldsson, B.T.; Langberg, H.; Aagaard, P.; Zuurmond, A.-M.; van El, B.; de Groot, J.; Kjær, M.; Magnusson, S.P. Corticosteroids Reduce the Tensile Strength of Isolated Collagen Fascicles. Am. J. Sports Med. 2006, 34, 1992–1997. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.K.; Tipton, C.M.; Matthes, R.D.; Bedford, T.G.; A Maynard, J.; Walmer, H.C. An in situ study of the influence of a sclerosing solution in rabbit medial collateral ligaments and its junction strength. Connect. Tissue Res. 1983, 11, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Mohamadi, A.; Chan, J.J.; Claessen, F.M.; Ring, D.; Chen, N.C. Corticosteroid Injections Give Small and Transient Pain Relief in Rotator Cuff Tendinosis: A Meta-Analysis; Springer: Berlin/Hedielberg, Germany, 2017. [Google Scholar]
- Johansson, K.; Oberg, B.; Adolfsson, L.; Foldevi, M. A combination of systematic review and clinicians’ beliefs in interventions for subacromial pain. Br. J. Gen. Pr. 2002, 52, 145–152. [Google Scholar]
- Grant, H.J.; Arthur, A.; Pichora, D.R. Evaluation of interventions for rotator cuff pathology: A systematic review. J. Hand Ther. 2004, 17, 274–299. [Google Scholar] [CrossRef] [PubMed]
- Green, S.; Buchbinder, R.; Glazier, R.; Forbes, A. Systematic review of randomised controlled trials of interventions for painful shoulder: Selection criteria, outcome assessment, and efficacy. BMJ 1998, 316, 354–360. [Google Scholar] [CrossRef]
- Goupille, P.; Sibilia, J. Local corticosteroid injections in the treatment of rotator cuff tendinitis (except for frozen shoulder and calcific tendinitis). Groupe Rhumatologique Français de l’Epaule (G.R.E.P.). Clin. Exp. Rheumatol. 1996, 14, 561–566. [Google Scholar]
- Van der Heijden, G.J.; van Der Windt, D.A.; Kleijnen, J.; Koes, B.W.; Bouter, L.M. Steroid injections for shoulder disorders: A systematic review of randomized clinical trials. Br. J. Gen. Pr. 1996, 46, 309–316. [Google Scholar]
- Buchbinder, R.; Green, S.; Youd, J. Corticosteroid injections for shoulder pain. Cochrane Database System. Rev. 2003, 1. [Google Scholar] [CrossRef]
- Petri, M.; Ettinger, M.; Brand, S.; Stuebig, T.; Krettek, C.; Omar, M. M11: Non-Operative Management of Rotator Cuff Tears. Open Orthop. J. 2016, 10 (Suppl. 1), 349. [Google Scholar] [CrossRef]
- Gialanella, B.; Prometti, P. Effects of Corticosteroids Injection in Rotator Cuff Tears. Pain Med. 2011, 12, 1559–1565. [Google Scholar] [CrossRef]
- Reeves, K.D.; Sit, R.W.; Clinics, R. Dextrose prolotherapy: A narrative review of basic science, clinical research, and best treatment recommendations. Physical Med. Rehabil. Clin. 2016, 27, 783–823. [Google Scholar] [CrossRef] [PubMed]
- Nichols, A.W. Complications Associated With the Use of Corticosteroids in the Treatment of Athletic Injuries. Clin. J. Sport Med. 2005, 15, E370–E375. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study | LOE | Study | Year | Procedures | Inclusion Criteria | No. of Patients (Shoulders) | Disease Stage | MINORS Score |
|---|---|---|---|---|---|---|---|---|
| Withrington et al. [18] | I | RCT | 1985 | Corticosteroid vs. placebo | Clinical supraspinatus tendonitis | 12(12)/13(13) | - | 10 |
| Vecchio et al. [19] | I | RCT | 1993 | Corticosteroid vs. placebo | Clinical diagnosed acute RC tendinitis | 28(28)/27(27) | - | 9 |
| Alvarez et al. [20] | I | RCT | 2005 | Corticosteroid vs. placebo | Chronic tendinosis or partial cuff tear | 30(30)/28(28) | - | 19 |
| Hong et al. [21] | I | RCT | 2011 | Corticosteroid (double dose) vs. corticosteroid vs. placebo | Clinically or ultrasound diagnosed RC lesion | 27(27)/25(25)/27(27) | - | 20 |
| Von Wehren et al. [22] | III | CT | 2014 | Corticosteroid vs. PRP | MRI evidence of partial supraspinatus tear | 25(25)/25(25) | II-III-IV | 18 |
| Shams et al. [23] | I | RCT | 2016 | Corticosteroid vs. PRP | Painful partial RC tears diagnosed by MRI | 20(20)/20(20) | II-III-IV | 20 |
| Cole et al. [24] | I | RCT | 2018 | Corticosteroid vs. Prolotherapy | Ultrasound evidence of supraspinatus tendinopathy | 19(19)/17(17) | - | 20 |
| Damjanov et al. [25] | I | RCT | 2018 | Corticosteroid vs. ACS | Ultrasonography evidence of supraspinatus tendinopathy | 16(16)/15(15) | - | 20 |
| Sari et al. [26] | I | RCT | 2019 | Corticosteroid vs. PRP vs. Prolotherapy vs. placebo | RC pathology (bursitis, RC tendinosis, or partial tears) | 30(30)/30(30)/ 30(30)/30(30) | - | 21 |
| Study | Follow-Up (wk) | Outcome Measure | Procedures/Rx Dose |
|---|---|---|---|
| Withrington et al. [18] | 2, 8 | VAS, paracetamol count | Steroid vs. Placebo |
| Vecchio et al. [19] | 2, 4, 12 | VAS, ROM | Steroid vs. Placebo |
| Alvarez et al. [20] | 2, 6, 12, 24 | VAS, DASH, ASES, WORC, ROM | Steroid vs. Placebo |
| Hong et al. [21] | 2, 4, 8 | VAS, SDQ, ROM | Steroid (double dose) vs. Steroid vs. Placebo |
| Von Wehren et al. [22] | 6, 12, 24 | VAS, CSS, ASES, SST | Steroid vs. PRP |
| Shams et al. [23] | 6, 12, 24 | VAS, CSS, ASES, SST | Steroid vs. PRP |
| Cole et al. [24] | 6, 12, 24 | Pain calculated with a 5 pt Likert scale, ROM | Steroid vs. Prolotherapy |
| Damjanov et al. [25] | 0, 4, 24 | VAS, CSS | Steroid vs. PRP |
| Sari et al. [26] | 3, 12, 24 | VAS, ASES, WORC | Steroid vs. PRP vs. Prolotherapy vs. Placebo |
| Study | Follow-up (wk) | Procedures/Rx Dose | VAS for Pain | ASES | CS | WORC/SST | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | |||
| Withrington et al. [18] | 2, 8 | Steroid: 80 mg methylprednisolone plus 2 mL of 2% lignocaine | 2.72 variation | |||||||
| Placebo: 4 mL 0.9% saline | 1.16 variation | |||||||||
| Vecchio et al. [19] | 2, 4, 12 | Steroid: 40 mg methylprednisolone plus 1 mL of 1% lignocaine | 14 (12–19) a | 8 decrease | ||||||
| Placebo: 1% lignocaine 1 mL | 15 (12–18) a | 8 decrease | ||||||||
| Alvarez et al. [20] | 2, 6, 12, 24 | Steroid: 4 mL of 2% xylocaine plus 6 mg of betamethasone | 54.8 (0–100) | 45.2 (0–100) | 46.9 ± 18.3 | 62.3 ± 22.9 | 38.1 ± 17 ** | 59 ± 26 ** | ||
| Placebo: 5 mL of 2% xylocaine alone | 61.9 (0–100) | 42.6 (0–100) | 41.7 ± 16 | 60.4 ± 24.2 | 35.4 ± 19 ** | 51 ± 32 ** | ||||
| Hong et al. [21] | 2, 4, 8 | Steroid: 4 mL of triamcinolone acetonide (40 mg) | 5.5 ± 1.8 | 2.0 ± 2.3 | ||||||
| Steroid: 2 mL of 20 mg of triamcinolone acetonide + 2 mL of 1% lidocaine | 6.0 ± 1.4 | 3.2 ± 1.9 | ||||||||
| Placebo: 4 mL of 1% lidocaine | 5.3 ± 1.6 | 4.7 ± 2.2 | ||||||||
| Von Wehren et al. [22] | 6, 12, 24 | Steroid: 40 mg triamcinolone acetonide | N.a. | N.a. | 50.6 ± 14 | 82.5 ± 25.4 | 69.9 ± 19.5 | 87.5 ± 12.3 | 5.8 ± 3.2 * | 9.3 ± 2.6 * |
| PRP: 5 mL of autologous conditioned blood | N.a. | N.a. | 50.7 ± 15 | 77.1 ± 19.3 | 66.2 ± 21.1 | 90.7 ± 9.4 | 6.5 ± 3.1 * | 10.3 ± 2.1 * | ||
| Shams et al. [23] | 6, 12, 24 | Steroid: 40 mg triamcinolone acetonide | N.a. | N.a. | 52.5 ± 15 | 78.9 ± 13.2 | 69.7 ± 19.4 | 87.3 ± 12.2 | 5.6 ± 3.1 * | 9.2 ± 2.7 * |
| PRP: 2–2.5 mL of autologous conditioned blood | N.a. | N.a. | 52.6 ± 16 | 83.4 ± 16.1 | 66 ± 21 | 90.5 ± 8.3 | 6.3 ± 3 * | 10.2 ± 1.8 * | ||
| Cole et al. [24] | 6, 12, 24 | Steroid: 1 mL of 40 mg/mL methylprednisolone acetate plus 1 mL of 1% lignocaine hydrochloride | 1.8 † | 2.4† | ||||||
| Prolo: 1 mL of 50% glucose (25 g/50 mL) + 1 mL of 1% lignocaine hydrochloride giving a 25% glucose prolotherapy solution. | 1.9 † | 2.8 † | ||||||||
| Damjanov et al. [25] | 0, 4, 24 | Steroid: 2 mL of bethametasone injection | 65 | 40 | 87.5% poor; 12.5% fair; †† | 53.3% poor; 13.3% fair; 20% good; 13.3% excellent; †† | ||||
| PRP: 2 mL of autologous conditioned serum | 70 | 15 | 86.7% poor; 13.3% excellent; †† | 6.7% poor-fair-good; 80% excellent; †† | ||||||
| Sari et al. [26] | 3, 12, 24 | Steroid: 2 mL of 40 mg triamcinolone acetonide plus 2 mL 1% lidocaine and 1 mL saline. | 5.63 ± 0.93 | 3.77 ± 1.41 | 40.13 ± 8.18 | 55.63 ± 11 | 51.4 ± 7.73 ** | 93.90 ± 17.94 ** | ||
| PRP: 5 mL of autologous conditioned blood plus 1 mL 10% calcium chloride | 5.63 ± 1.00 | 2.57 ± 1.19 | 46.28 ± 8.61 | 63.87 ± 11.96 | 50.79 ± 6.48 ** | 79.46 ± 24.09 ** | ||||
| Prolotherapy: 5 mL of a mixture of 4 mL 20%dextrose and 1 mL lidocaine | 5.9 ± 0.88 | 3.1 ± 1.52 | 45 ± 9.42 | 60.37 ± 11.4 | 53.67 ± 8.43 ** | 91.27 ± 21.79 ** | ||||
| Placebo: 5 mL solution containing 3 mL 1% lidocaine plus 2 mL saline solution | 5.47 ± 0.86 | 3.2 ± 1.19 | 47.27 ± 7.44 | 47.27 ± 7.44 | 52.13 ± 7.92 ** | 96.55 ± 20.43 ** | ||||
| Score | Corticosteroids | PRP | Prolotherapy | p Value (ANOVA) | |
|---|---|---|---|---|---|
| VAS | Pre-op. | 5.6 ± 0.66 | 6.2 ± 1.2 | 5.3 ± 0.81 | 0.56 |
| Short term | 2.73 ± 1.08 | 3.51 ± 1.86 | 4.37 ± 1.16 | 0.19 | |
| Mid term | 2.93 ± 0.89 | 3.9 | 4.27 ± 1.36 | 0.13 | |
| Long term | 4.09 ± 0.38 | 2.04 ± 0.76 | 3.1 ± 1.52 | 0.02 * | |
| ASES | Pre-op. | 48 ± 5.5 | 50 ± 3.2 | 45 ± 9.42 | 0.65 |
| Short term | 64.70 ± 6.71 | 63.89 ± 15.38 | 52.60 ± 11.25 | 0.36 | |
| Mid term | 63.60 ± 4.98 | 76.59 ± 18.03 | 56.10 ± 9.62 | 0.18 | |
| Long term | 68.48 ± 11.35 | 76.59 ± 11.03 | 60.37 ± 11.40 | 0.28 | |
| COSTANT | Pre-op. | 69 ± 2.8 | 68 ± 2.5 | - | 0.89 |
| Short term | 80.70 ± 0.14 | 81.50 ± 0.14 | - | 0.03 * | |
| Mid term | 77.50 ± 0.14 | 91 ± 0.14 | - | <0.01 * | |
| Long term | 87.40 ± 0.14 | 90.60 ± 0.14 | - | <0.01 * | |
| WORC | Pre-op. | 45 ± 9.4 | 51 ± 6.48 | 54 ± 8.43 | 0.77 |
| Short term | 50.52 ± 7.41 | 51.65 | 52.03 ± 7.79 | 0.06 | |
| Mid term | 51.22 ± 7.18 | 42.83 | 46.38 ± 9.01 | 0.27 | |
| Long term | 76.45 ± 24.68 | 79.46 | 91.27 ± 21.79 | 0.60 | |
| SST | Pre-op. | 6.2 ± 0.49 | 6.0 ± 0.49 | - | 0.72 |
| Short term | 8.6 ± 0.14 | 8.3 ± 0.14 | - | 0.16 | |
| Mid term | 8.25 ± 0.07 | 10.25 ± 0.07 | - | <0.01 * | |
| Long term | 9.25 ± 0.07 | 10.25 ± 0.07 | - | <0.01 * |
| Study | Procedures | Active abduction (°) | Active Forward Flexion (°) | Active External Rotation (°) | Active Internal Rotation (°) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post (Last Follow-Up) | Pre | Post (Last Follow-Up) | Pre | Post (Last Follow-Up) | Pre | Post (Last Follow-Up) | ||
| Withrington et al. [18] | Steroid | 64.6° | N.a. | ||||||
| Placebo | 61.9° | N.a. | |||||||
| Vecchio et al. [19] | Steroid | 155 (105-180) * | 0 (-10-50) ** | 45 (15-55) * | 0("5-^0) ** | ||||
| Placebo | 160(130-180) * | 0 (0-20) ** | 40 (20-60) * | 20(0-40) ** | |||||
| Alvarez et al. [20] | Steroid | 138.9° ± 23.7° | 139.0° ± 21.8° | 75.3° ± 16° | 75.7° ± 23.6° | 45.3° ± 23° | 46.4° ± 24° | ||
| Placebo | 136.3° ± 28.8° | 143.7° ± 27.8° | 80.4° ± 26.5° | 63.7° ± 25° | 40.9° ± 30° | 49.2° ± 27.4° | |||
| Hong et al. [21] | Steroid (double dose) | 141.7° ± 27.4° | 161.1° ± 25.0° | 153.0° ± 17.3° | 164.9° ± 15.7° | 64.3° ± 16.9° | 84.6° ± 15.2° | 44.0° ± 14.7° | 64.7° ± 15.0° |
| Steroid | 137.8° ± 26.8° | 162.7° ± 20.6° | 151.7° ± 19.1° | 163.0° ± 16.9° | 59.0° ± 16.6° | 84.6° ± 11.9° | 42.7° ± 19.3° | 59.7° ± 19.3° | |
| Placebo | 140.7° ± 21.4° | 137.6° ± 21.1° | 155.4° ± 12.3° | 157.9° ± 13.5° | 63.7° ± 18.5° | 63.9° ± 23.0° | 40.7° ± 13.3° | 41.9° ± 14.4° | |
| Von Wehren et al. [22] | Steroid | ||||||||
| PRP | |||||||||
| Shams et al. [23] | Steroid | ||||||||
| PRP | |||||||||
| Cole et al. [24] | Steroid | 153° | 163° | 161° | 165° | 60° | 63° | ||
| Prolotherapy | 166° | 175° | 167° | 172° | 67° | 61° | |||
| Damjanov et al. [25] | Steroid | ||||||||
| PRP | |||||||||
| Sari et al. [26] | Steroid | ||||||||
| PRP | |||||||||
| Prolotherapy | |||||||||
| Placebo | |||||||||
| Study | Follow-Up (wk) | No. of Patients (Shoulders) | Complications |
|---|---|---|---|
| Withrington et al. [18] | 2, 8 | 12(12)/13(13) | No mention |
| Vecchio et al. [19] | 2, 4, 12 | 28(28)/27(27) | No mention |
| Alvarez et al. [20] | 2, 6, 12, 24 | 30(30)/28(28) | No mention |
| Hong et al. [21] | 2, 4, 8 | 27(27)/25(25)/ 27(27) | Steroid (x2): Transient diarrhea (1) |
| Steroid: Facial flushing (1) | |||
| Placebo: Dizziness (1) | |||
| Von Wehren et al. [22] | 6, 12, 24 | 25(25)/25(25) | No infection reported |
| Shams et al. [23] | 6, 12, 24 | 20(20)/20(20) | No infection reported |
| Cole et al. [24] | 6, 12, 24 | 19(19)/17(17) | No mention |
| Damjanov et al. [25] | 0, 4, 24 | 16(16)/15(15) | Steroid: Arterial hypertension (2); Facial erythema (2); Facies lunata (1); Headache (3); Total = 8 AE; |
| PRP: No complications reported | |||
| Sari et al. [26] | 3, 12, 24 | 30(30)/30(30)/ 30(30)/30(30) | No mention |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giovannetti de Sanctis, E.; Franceschetti, E.; De Dona, F.; Palumbo, A.; Paciotti, M.; Franceschi, F. The Efficacy of Injections for Partial Rotator Cuff Tears: A Systematic Review. J. Clin. Med. 2021, 10, 51. https://doi.org/10.3390/jcm10010051
Giovannetti de Sanctis E, Franceschetti E, De Dona F, Palumbo A, Paciotti M, Franceschi F. The Efficacy of Injections for Partial Rotator Cuff Tears: A Systematic Review. Journal of Clinical Medicine. 2021; 10(1):51. https://doi.org/10.3390/jcm10010051
Chicago/Turabian StyleGiovannetti de Sanctis, Edoardo, Edoardo Franceschetti, Ferdinando De Dona, Alessio Palumbo, Michele Paciotti, and Francesco Franceschi. 2021. "The Efficacy of Injections for Partial Rotator Cuff Tears: A Systematic Review" Journal of Clinical Medicine 10, no. 1: 51. https://doi.org/10.3390/jcm10010051
APA StyleGiovannetti de Sanctis, E., Franceschetti, E., De Dona, F., Palumbo, A., Paciotti, M., & Franceschi, F. (2021). The Efficacy of Injections for Partial Rotator Cuff Tears: A Systematic Review. Journal of Clinical Medicine, 10(1), 51. https://doi.org/10.3390/jcm10010051