Safety of Co-Administration Versus Separate Administration of the Same Vaccines in Children: A Systematic Literature Review

Abstract
1. Introduction
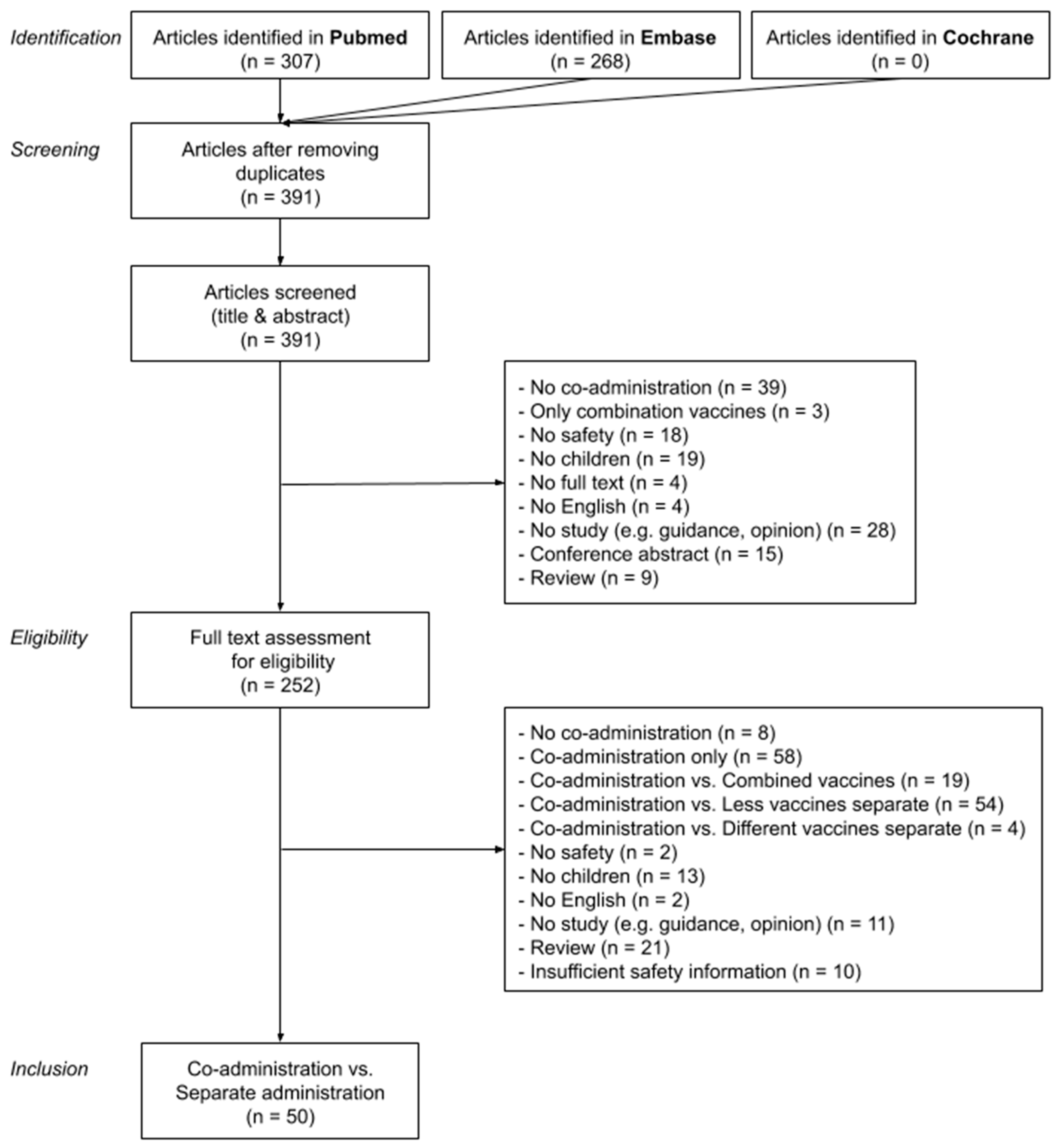
2. Methods
- Population: Infant OR child OR adolescent OR newborn OR minors OR teenager;
- Intervention: Vaccination OR vaccines OR immunization OR immunization schedule OR immunization OR immunization, secondary/trends OR mass vaccination/trends OR vaccines/administration & dosage OR vaccines/pharmacology; and
- Outcome: ((Safety drug-related side effects OR adverse reactions OR adverse effects OR vaccination/adverse effects OR vaccines/complications OR vaccines/adverse effects) OR safety OR tolerability) AND (co-administration OR co-administered OR concomitant administration OR simultaneous administration).
3. Results
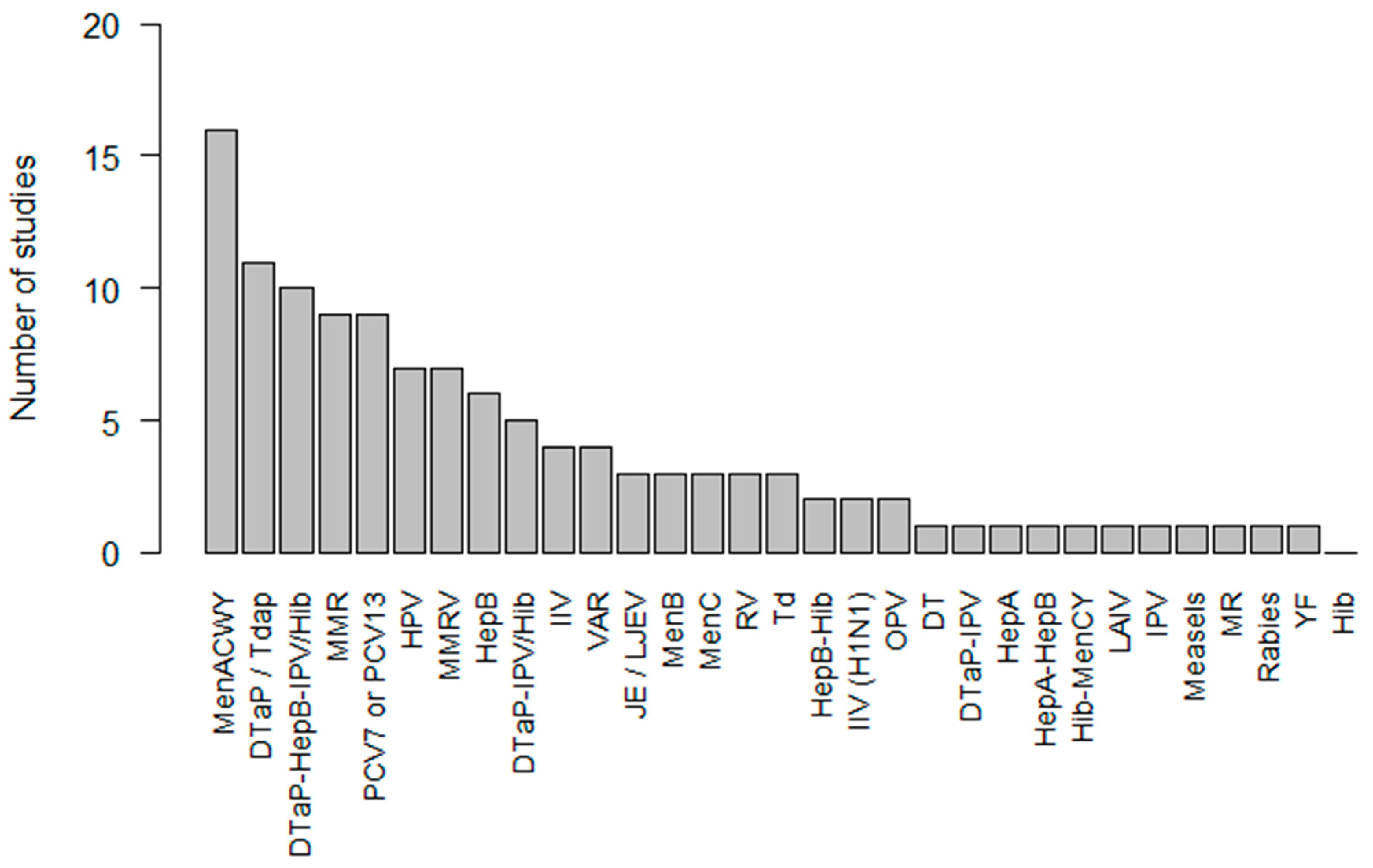
3.1. Vaccines Studied
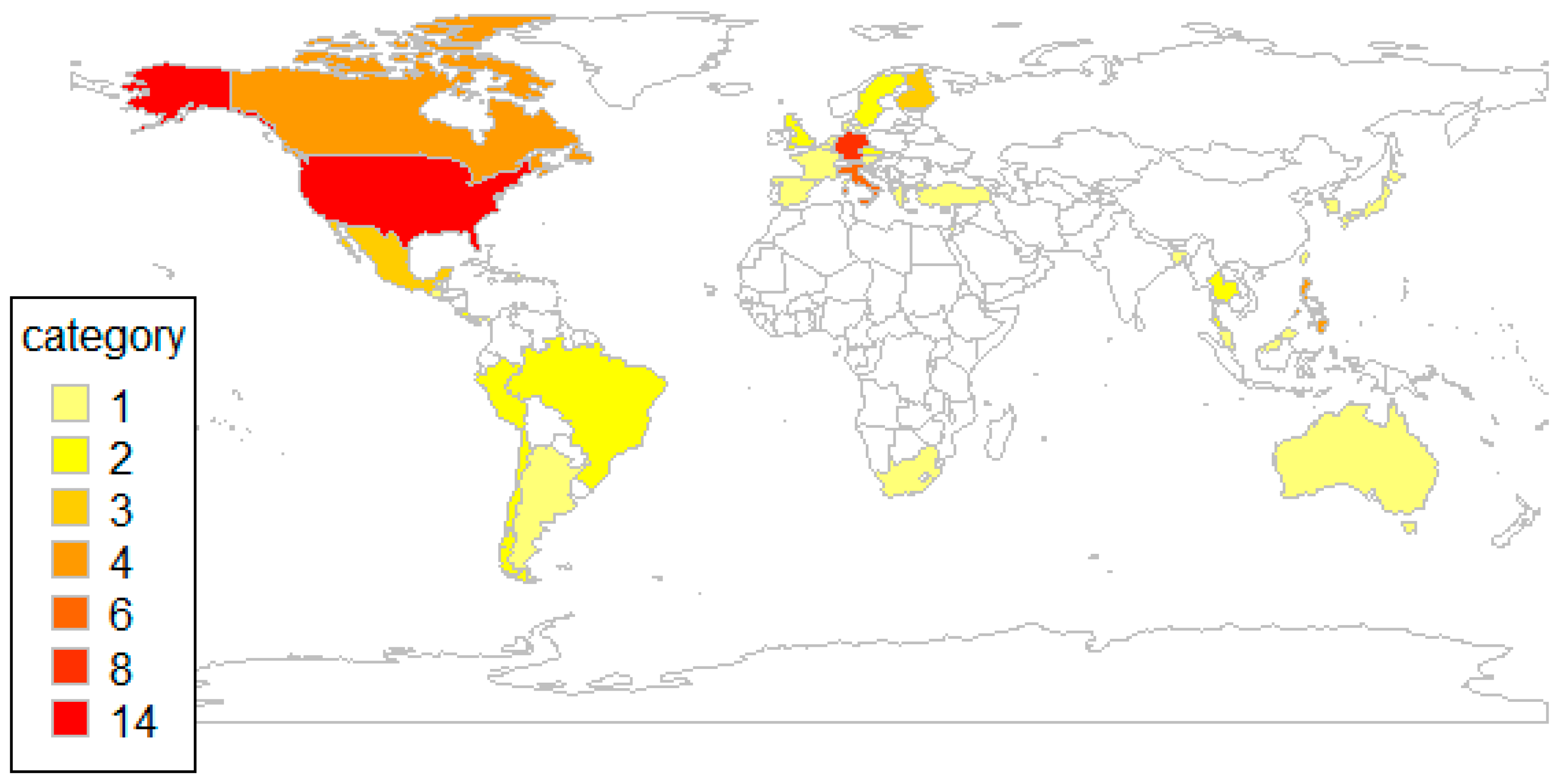
3.2. Study Characteristics
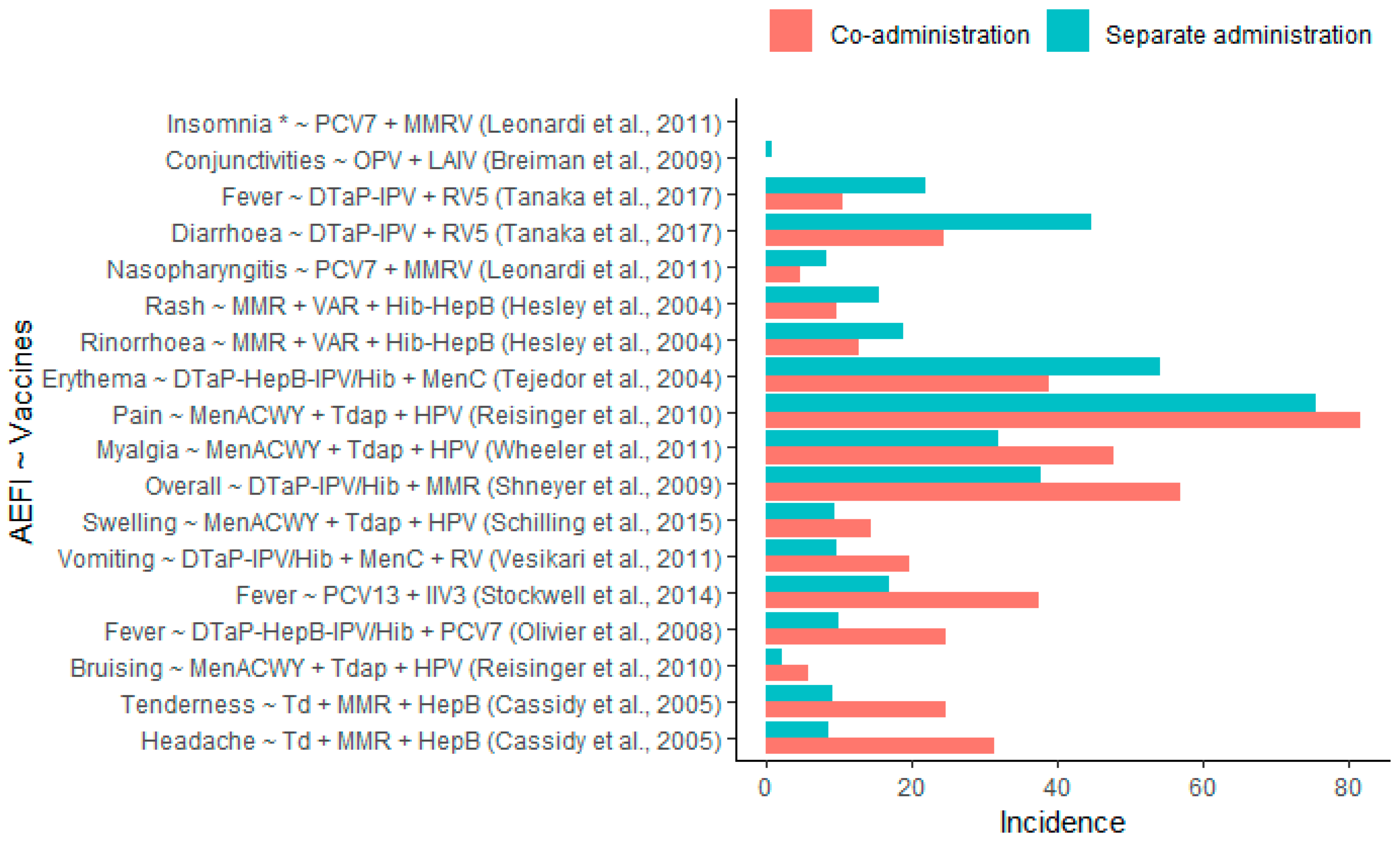
3.3. Safety Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Doshi, P.; Stahl-Timmins, W.; Merino, J.G.; Simpkins, C. Visualising childhood vaccination schedules across G8 countries. BMJ 2015, 351, h5966. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). Vaccine Scheduler. Solna, Sweden, 2017. Available online: https://vaccine-schedule.ecdc.europa.eu/ (accessed on 25 December 2017).
- Pellegrino, A.; Busellu, G.; Cucchi, A.; Cavallaro, A.; Gabutti, G. Vaccine co-administration in paediatric age: The experience of the local health unit of Cuneo-1 (ambito di cuneo), Italy. Acta Bio Med. Atenei Parm. 2010, 81, 204–209. [Google Scholar]
- Gilkey, M.B.; McRee, A.-L.; Magnus, B.E.; Reiter, P.L.; Dempsey, A.F.; Brewer, N.T. Vaccination confidence and parental refusal/delay of early childhood vaccines. PLoS ONE 2016, 11, e0159087. [Google Scholar] [CrossRef] [PubMed]
- Karafillakis, E.; Larson, H.J. The benefit of the doubt or doubts over benefits? A systematic literature review of perceived risks of vaccines in European populations. Vaccine 2017, 35, 4840–4850. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.; Kundi, M.; Zwiauer, K.; Wiedermann, U. Paediatricians require more information before they routinely co-administer the meningococcal B vaccine with routine infant vaccines. Acta Paediatr. 2015, 104, e439–e447. [Google Scholar] [CrossRef] [PubMed]
- Roy Rosenzweig Center for History and New Media. Zotero; Roy Rosenzweig Center for History and New Media, George Mason University: Fairfax, VA, USA, 2016. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Olivier, B.; Stojanov, B.; Petersen, L. Immunogenicity, reactogenicity, and safety of a seven-valent pneumococcal conjugate vaccine (PCV7) concurrently administered with a fully liquid DTPa-IPV-HBV-Hib combination vaccine in healthy infants. Vaccine 2008, 26, 3142–3152. [Google Scholar] [CrossRef]
- Stockwell, M.S.; Broder, K.; LaRussa, P.; Lewis, P.; Fernandez, N.; Sharma, D.; Barrett, A.; Sosa, J.; Vellozzi, C. Risk of fever after pediatric trivalent inactivated influenza vaccine. JAMA Pediatrics 2014, 168, 211–219. [Google Scholar] [CrossRef]
- Reisinger, K.S.; Block, S.L.; Collins-Ogle, M.; Marchant, C.; Catlett, M.; Radley, D.; Sings, H.L.; Haupt, R.M.; Garner, E.I.O. Safety, tolerability, and immunogenicity of gardasil given concomitantly with menactra and adacel. Pediatrics 2010, 125, 1142–1151. [Google Scholar] [CrossRef]
- Schilling, A.; Parra, M.M.; Gutierrez, M.; Restrepo, J.; Ucros, S.; Herrera, T.; Engel, E.; Huicho, L.; Shew, M.; Maansson, R.; et al. Coadministration of a 9-valent human papillomavirus vaccine with meningococcal and tdap vaccines. Pediatrics 2015, 136, e563–e572. [Google Scholar] [CrossRef]
- Wheeler, C.M.; Harvey, B.M.; Pichichero, M.E.; Simon, M.W.; Combs, S.P.; Blatter, M.M.; Marshall, G.S.; Catteau, G.; Dobbelaere, K.; Descamps, D.; et al. Immunogenicity and safety of human papillomavirus-16/18 AS04-adjuvanted vaccine coadministered with tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis vaccine and/or meningococcal conjugate vaccine to healthy girls 11 to 18 years of age: Results from a randomized open trial. Pediatrics Infect. Dis. J. 2011, 30, e225–e234. [Google Scholar] [CrossRef]
- Cassidy, W.M.; Jones, G.; Williams, K.; Deforest, A.; Forghani, B.; Virella, G.; Venters, C. Safety and immunogenicity of concomitant versus nonconcomitant administration of hepatitis, B.; tetanus-diphtheria, and measles-mumps-rubella vaccines in healthy eleven- to twelve-year-olds. J. Adolesc. Health 2005, 36, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Vesikari, T.; Karvonen, A.; Borrow, R.; Kitchin, N.; Baudin, M.; Thomas, S.; Fiquet, A. Results from a randomized clinical trial of coadministration of RotaTeq, a pentavalent rotavirus vaccine, and NeisVac-C, a meningococcal serogroup C conjugate vaccine. Clin. Vaccine Immunol. 2011, 18, 878–884. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Shneyer, E.; Strulov, A.; Rosenfeld, Y. Reduced rate of side effects associated with separate administration of MMR and DTaP-Hib-IPV vaccinations. Isr. Med. Assoc. J. IMAJ 2009, 11, 735–738. [Google Scholar] [PubMed]
- Tanaka, Y.; Yokokawa, R.; Rong, H.S.; Kishino, H.; Stek, J.E.; Nelson, M.; Lawrence, J. Concomitant administration of diphtheria, tetanus, acellular pertussis and inactivated poliovirus vaccine derived from Sabin strains (DTaP-sIPV) with pentavalent rotavirus vaccine in Japanese infants. Hum. Vaccines Immunother. 2017, 13, 1–7. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Tejedor, J.C.; Omenaca, F.; Garcia-Sicilia, J.; Verdaguer, J.; Van Esso, D.; Esporrin, C.; Molina, V.; Muro, M.; Mares, J.; Enrubia, M.; et al. Immunogenicity and reactogenicity of a three-dose primary vaccination course with a combined diphtheria-tetanus-acellular pertussis-hepatitis B-inactivated polio-Haemophilus influenzae type b vaccine coadministered with a meningococcal C conjugate vaccine. Pediatric Infect. Dis. J. 2004, 23, 1109–1115. [Google Scholar]
- Hesley, T.M.; Reisinger, K.S.; Sullivan, B.J.; Jensen, E.H.; Stasiorowski, S.; Meechan, C.; Chan, C.Y.; West, D.J. Concomitant administration of a bivalent Haemophilus influenzae type b-hepatitis B vaccine, measles-mumps-rubella vaccine and varicella vaccine: Safety, tolerability and immunogenicity. Pediatric Infect. Dis. J. 2004, 23, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, M.; Bromberg, K.; Baxter, R.; Gardner, J.L.; Klopfer, S.; Nicholson, O.; Brockley, M.; Trammel, J.; Leamy, V.; Williams, W.; et al. Immunogenicity and safety of MMRV and PCV-7 administered concomitantly in healthy children. Pediatrics 2011, 128, e1387–e1394. [Google Scholar] [CrossRef]
- Breiman, R.F.; Brooks, W.A.; Goswami, D.; Lagos, R.; Borja-Tabora, C.; Lanata, C.F.; Londono, J.A.C.; Lum, L.C.S.; Rappaport, R.; Razmpour, A.; et al. A multinational, randomized, placebo-controlled trial to assess the immunogenicity, safety, and tolerability of live attenuated influenza vaccine coadministered with oral poliovirus vaccine in healthy young children. Vaccine 2009, 27, 5472–5479. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Monitoring Processes to R&D 2019. Available online: https://www.who.int/research-observatory/monitoring/processes/clinical_trials_1/en/ (accessed on 20 December 2019).
- Arguedas, A.; Soley, C.; Loaiza, C.; Rincon, G.; Guevara, S.; Perez, A.; Porras, W.; Alvarado, O.; Aguilar, L.; Abdelnour, A.; et al. Safety and immunogenicity of one dose of MenACWY-CRM, an investigational quadrivalent meningococcal glycoconjugate vaccine, when administered to adolescents concomitantly or sequentially with Tdap and HPV vaccines. Vaccine 2010, 28, 3171–3179. [Google Scholar] [CrossRef]
- Gasparini, R.; Conversano, M.; Bona, G.; Gabutti, G.; Anemona, A.; Dull, P.M.; Ceddia, F. Randomized trial on the safety, tolerability, and immunogenicity of MenACWY-CRM, an investigational quadrivalent meningococcal glycoconjugate vaccine, administered concomitantly with a combined tetanus, reduced diphtheria, and acellular pertussis vaccine in adolescents and young adults. Clin. Vaccine Immunol. CVI 2010, 17, 537–544. [Google Scholar] [CrossRef][Green Version]
- Jackson, L.A.; Yu, O.; Nelson, J.; Belongia, E.A.; Hambidge, S.J.; Baxter, R.; Naleway, A.; Nordin, J.; Baggs, J.; Iskander, J. Risk of medically attended local reactions following diphtheria toxoid containing vaccines in adolescents and young adults: A Vaccine Safety Datalink study. Vaccine 2009, 27, 4912–4916. [Google Scholar] [CrossRef] [PubMed]
- Rivera, L.; Schwarz, T.F.; Kim, K.-H.; Kim, Y.-K.; Behre, U.; Cha, S.-H.; Jo, D.S.; Lee, J.; Lee, J.-S.; Cheuvart, B.; et al. Immunogenicity and safety of the quadrivalent meningococcal vaccine MenACWY-TT co-administered with a combined diphtheria-tetanus-acellular pertussis vaccine versus their separate administration in adolescents and young adults: A phase III, randomized study. Vaccine 2018, 36, 4750–4758. [Google Scholar] [CrossRef] [PubMed]
- Weston, W.M.; Friedland, L.R.; Wu, X.; Howe, B. Immunogenicity and reactogenicity of co-administered tetanus-diphtheria-acellular pertussis (Tdap) and tetravalent meningococcal conjugate (MCV4) vaccines compared to their separate administration. Vaccine 2011, 29, 1017–1022. [Google Scholar] [CrossRef] [PubMed]
- Trotta, F.; Santuccio, C.; Felicetti, P.; Bella, A.; Rizzo, C.; Conti, V.; Monaco, G.; Russo, F.; Zanoni, G.; Osbello, L.; et al. Comparative safety evaluation of 7-valent and 13-valent pneumococcal vaccines in routine paediatric vaccinations in four Italian regions, 2009 to 2011. Eurosurveillance 2015, 20, 21041. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Halperin, S.A.; Tapiero, B.; Dionne, M.; Meekison, W.; Diaz-Mitoma, F.; Zickler, P.; Rubin, E.; Embree, J.; Bhuyan, P.; Lee, A.; et al. Safety and immunogenicity of a toddler dose following an infant series of a hexavalent diphtheria, tetanus, acellular pertussis, inactivated poliovirus, Haemophilus influenzae type b, hepatitis B vaccine administered concurrently or at separate visits with a heptavalent pneumococcal conjugate vaccine. Pediatric Infect. Dis. J. 2014, 33, 73–80. [Google Scholar] [CrossRef]
- Zepp, F.; Behre, U.; Kindler, K.; Laakmann, K.-H.; Pankow-Culot, H.; Mannhardt-Laakmann, W.; Beckers, F.; Descamps, D.; Willems, P. Immunogenicity and safety of a tetravalent measles-mumps-rubella-varicella vaccine co-administered with a booster dose of a combined diphtheria-tetanus-acellular pertussis-hepatitis B-inactivated poliovirus-Haemophilus influenzae type b conjugate vaccine in healthy children aged 12-23 months. Eur. J. Pediatrics 2007, 166, 857–864. [Google Scholar] [CrossRef]
- Deichmann, K.A.; Ferrera, G.; Tran, C.; Thomas, S.; Eymin, C.; Baudin, M. Immunogenicity and safety of a combined measles, mumps, rubella and varicella live vaccine (ProQuad (R)) administered concomitantly with a booster dose of a hexavalent vaccine in 12-23-month-old infants. Vaccine 2015, 33, 2379–2386. [Google Scholar] [CrossRef]
- Kiely, M.; Billard, M.-N.; Toth, E.; Zafack, J.G.; Landry, M.; Skowronski, D.M.; De Serres, G. Investigation of an increase in large local reactions following vaccine schedule change to include DTaP-HB-IPV-Hib (Infanrix-hexa) and MMRV (ProQuad) at 18months of age. Vaccine 2018, 36, 6688–6694. [Google Scholar] [CrossRef]
- Gatchalian, S.; Leboulleux, D.; Desauziers, E.; Bermal, N.; Borja-Tabora, C. Immunogenicity and safety of a varicella vaccine, Okavax, and a trivalent measles, mumps and rubella vaccine, MMR-II, administered concomitantly in healthy Filipino children aged 12–24 months. Southeast Asian J. Trop. Med. Public Health 2003, 34, 589–597. [Google Scholar]
- Gatchalian, S.; Tabora, C.; Bermal, N.; Leboulleux, D.; Desauziers, E. Immunogenicity and safety of a varicella vaccine (Okavax) and a trivalent measles, mumps, and rubella vaccine (Trimovax) administered concomitantly in healthy Filipino children 12-24 months old. Am. J. Trop. Med. Hyg. 2004, 70, 273–277. [Google Scholar] [CrossRef]
- Shinefield, H.; Black, S.; Thear, M.; Coury, D.; Reisinger, K.; Rothstein, E.; Xu, J.; Hartzel, J.; Evans, B.; Digilio, L.; et al. Safety and immunogenicity of a measles, mumps, rubella and varicella vaccine given with combined Haemophilus influenzae type b conjugate/hepatitis B vaccines and combined diphtheria-tetanus-acellular pertussis vaccines. Pediatric Infect. Dis. J. 2006, 25, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Vesikari, T.; Borrow, R.; Da Costa, X.; Thomas, S.; Eymin, C.; Boisnard, F.; Lockhart, S. Concomitant administration of a fully liquid ready-to-use DTaP-IPV-HB-PRP-T hexavalent vaccine with a meningococcal ACWY conjugate vaccine in toddlers. Vaccine 2018, 36, 8019–8027. [Google Scholar] [CrossRef] [PubMed]
- Knuf, M.; Pantazi-Chatzikonstantinou, A.; Pfletschinger, U.; Tichmann-Schumann, I.; Maurer, H.; Maurer, L.; Fischbach, T.; Zinke, H.; Pankow-Culot, H.; Papaevangelou, V.; et al. An investigational tetravalent meningococcal serogroups, A.; C, W-135 and Y-tetanus toxoid conjugate vaccine co-administered with Infanrix hexa is immunogenic, with an acceptable safety profile in 12-23-month-old children. Vaccine 2011, 29, 4264–4273. [Google Scholar] [CrossRef] [PubMed]
- Schmeink, C.E.; Bekkers, R.L.M.; Josefsson, A.; Richardus, J.H.; Berndtsson Blom, K.; David, M.-P.; Dobbelaere, K.; Descamps, D. Co-administration of human papillomavirus-16/18 AS04-adjuvanted vaccine with hepatitis B vaccine: Randomized study in healthy girls. Vaccine 2011, 29, 9276–9283. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, C.M.; Bautista, O.M.; Tomassini, J.E.; Nelson, M.; Sattler, C.A.; Barr, E. Safety and immunogenicity of co-administered quadrivalent human papillomavirus (HPV)-6/11/16/18 L1 virus-like particle (VLP) and hepatitis B (HBV) vaccines. Vaccine 2008, 26, 686–696. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Meregalli, E.; Daleno, C.; Ghio, L.; Tagliabue, C.; Valzano, A.; Serra, D.; Galeone, C.; Edefonti, A.; Principi, N. An open-label, randomized clinical trial assessing immunogenicity, safety and tolerability of pandemic influenza A/H1N1 MF59-adjuvanted vaccine administered sequentially or simultaneously with seasonal virosomal-adjuvanted influenza vaccine to paediatric kidney transplant recipients. Nephrol. Dial. Transplant. 2011, 26, 2018–2024. [Google Scholar] [CrossRef]
- Esposito, S.; Tagliaferri, L.; Daleno, C.; Valzano, A.; Picciolli, I.; Tel, F.; Prunotto, G.; Serra, D.; Galeone, C.; Plebani, A.; et al. Pandemic influenza A/H1N1 vaccine administered sequentially or simultaneously with seasonal influenza vaccine to HIV-infected children and adolescents. Vaccine 2011, 29, 1677–1682. [Google Scholar] [CrossRef]
- Rivera, L.; Chanthavanich, P.; Poder, A.; Suryakiran, P.V.; Jastorff, A.; Van der Wielen, M. MenACWY-TT is immunogenic when co-administered with Tdap and AS04-HPV16/18 in girls and young women: Results from a phase III randomized trial. Vaccine 2018, 36, 3967–3975. [Google Scholar] [CrossRef]
- Knuf, M.; Habermehl, P.; Cimino, C.; Petersen, G.; Schmitt, H.-J. Immunogenicity, reactogenicity and safety of a 7-valent pneumococcal conjugate vaccine (PCV7) concurrently administered with a DTPa-HBV-IPV/Hib combination vaccine in healthy infants. Vaccine 2006, 24, 4727–4736. [Google Scholar] [CrossRef]
- Martinon-Torres, F.; Gimenez-Sanchez, F.; Gurtman, A.; Bernaola, E.; Diez-Domingo, J.; Carmona, A.; Sidhu, M.; Sarkozy, D.A.; Gruber, W.C.; Emini, E.A. 13-valent pneumococcal conjugate vaccine given with meningococcal C-tetanus toxoid conjugate and other routine pediatric vaccinations: Immunogenicity and safety. Pediatric Infect. Dis. J. 2012, 31, 392–399. [Google Scholar] [CrossRef]
- Tichmann-Schumann, I.; Soemantri, P.; Behre, U.; Disselhoff, J.; Mahler, H.; Maechler, G.; Sanger, R.; Jacquet, J.-M.; Schuerman, L. Immunogenicity and reactogenicity of four doses of diphtheria-tetanus-three-component acellular pertussis-hepatitis B-inactivated polio virus-Haemophilus influenzae type b vaccine coadministered with 7-valent pneumococcal conjugate vaccine. Pediatric Infect. Dis. J. 2005, 24, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Vesikari, T.; Esposito, S.; Prymula, R.; Ypma, E.; Kohl, I.; Toneatto, D.; Dull, P.; Kimura, A. Immunogenicity and safety of an investigational multicomponent, recombinant, meningococcal serogroup B vaccine (4CMenB) administered concomitantly with routine infant and child vaccinations: Results of two randomised trials. Lancet 2013, 381, 825–835. [Google Scholar] [CrossRef]
- Vesikari, T.; Karvonen, A.; Prymula, R.; Schuster, V.; Tejedor, J.C.; Thollot, F.; Garcia-Corbeira, P.; Damaso, S.; Han, H.H.; Bouckenooghe, A. Immunogenicity and safety of the human rotavirus vaccine Rotarix co-administered with routine infant vaccines following the vaccination schedules in Europe. Vaccine 2010, 28, 5272–5279. [Google Scholar] [CrossRef] [PubMed]
- Wysocki, J.; Tansey, S.; Brachet, E.; Baker, S.; Gruber, W.; Giardina, P.; Arora, A. Randomised, controlled trial of concomitant pneumococcal and meningococcal conjugate vaccines. Vaccine 2010, 28, 7779–7786. [Google Scholar] [CrossRef] [PubMed]
- Alicino, C.; Merlano, C.; Zappettini, S.; Schiaffino, S.; Della Luna, G.; Accardo, C.; Gasparini, R.; Durando, P.; Icardi, G. Routine surveillance of adverse events following immunization as an important tool to monitor vaccine safety. Hum. Vaccines Immunother. 2015, 11, 91–94. [Google Scholar] [CrossRef]
- Baggio, S.; Gétaz, L. Current gaps in vaccination coverage: A need to improve prevention and care. Int. J. Public Health 2019, 64, 311–312. [Google Scholar] [CrossRef]
- Masters, N.B.; Wagner, A.L.; Carlson, B.F.; Boulton, M.L. Vaccination timeliness and co-administration among Kenyan children. Vaccine 2018, 36, 1353–1360. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Type | n | Minimum | Sample Size Median | Maximum |
|---|---|---|---|---|
| RCT (no phase specified) | 27 | 64 | 550 | 2503 |
| RCT phase 2 | 3 | 200 | 2499 | 2648 |
| RCT phase 2b | 1 | 460 | ||
| RCT phase 3 | 9 | 312 | 802 | 1620 |
| RCT phase 3b | 2 | 716 | 730 | 744 |
| RCT phase 4 | 3 | 376 | 1341 | 1504 |
| Case Control | 1 | 590 | ||
| Prospective Observational Cohort | 1 | 530 | ||
| Retrospective Observational Cohort | 1 | 36,844 | ||
| Surveillance report | 1 | 128,297 | ||
| Case Reports | 1 | 833 |
| Vaccines Co-Administered | Number of Studies | AEFI | Stat. Sign. More AEFI | Stat. Sign. Fewer AEFI | No Stat. Sign. Difference |
|---|---|---|---|---|---|
| DTaP-HepB-IPV/Hib + MenC | 1 | Injection site erythema | 0 (0%) | 1 (100%) | 0 (0%) |
| DTaP-HepB-IPV/Hib + PCV7 | 3 | Pyrexia | 1 (33%) | 0 (0%) | 2 (67%) |
| DTaP-IPV + RV5 | 1 | Diarrhoea | 0 (0%) | 1 (100%) | 0 (0%) |
| Pyrexia | 0 (0%) | 1 (100%) | 0 (0%) | ||
| DTaP-IPV/Hib + MenC + RV | 1 | Vomiting | 1 (100%) | 0 (0%) | 0 (0%) |
| DTaP-IPV/Hib + MMR | 1 | Overall | 1 (100%) | 0 (0%) | 0 (0%) |
| MenACWY + Tdap + HPV | 4 | Injection site bruising | 1 (25%) | 0 (0%) | 3 (75%) |
| Injection site pain | 1 (25%) | 0 (0%) | 3 (75%) | ||
| Injection site swelling | 1 (25%) | 0 (0%) | 3 (75%) | ||
| Myalgia | 1 (25%) | 0 (0%) | 3 (75%) | ||
| MMR + VAR + Hib-HepB | 1 | Rash | 0 (0%) | 1 (100%) | 0 (0%) |
| Rhinorrhoea | 0 (0%) | 1 (100%) | 0 (0%) | ||
| OPV + LAIV | 1 | Conjunctivitis | 0 (0%) | 1 (100%) | 0 (0%) |
| PCV7 + MMRV | 1 | Insomnia | 0 (0%) | 1 (100%) | 0 (0%) |
| Nasopharyngitis | 0 (0%) | 1 (100%) | 0 (0%) | ||
| PCV13 + IIV3 | 1 | Pyrexia | 1 (100%) | 0 (0%) | 0 (0%) |
| Td + MMR + HepB | 1 | Headache | 1 (100%) | 0 (0%) | 0 (0%) |
| Injection site tenderness | 1 (100%) | 0 (0%) | 0 (0%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bauwens, J.; Saenz, L.-H.; Reusser, A.; Künzli, N.; Bonhoeffer, J. Safety of Co-Administration Versus Separate Administration of the Same Vaccines in Children: A Systematic Literature Review. Vaccines 2020, 8, 12. https://doi.org/10.3390/vaccines8010012
Bauwens J, Saenz L-H, Reusser A, Künzli N, Bonhoeffer J. Safety of Co-Administration Versus Separate Administration of the Same Vaccines in Children: A Systematic Literature Review. Vaccines. 2020; 8(1):12. https://doi.org/10.3390/vaccines8010012
Chicago/Turabian StyleBauwens, Jorgen, Luis-Henri Saenz, Annina Reusser, Nino Künzli, and Jan Bonhoeffer. 2020. "Safety of Co-Administration Versus Separate Administration of the Same Vaccines in Children: A Systematic Literature Review" Vaccines 8, no. 1: 12. https://doi.org/10.3390/vaccines8010012
APA StyleBauwens, J., Saenz, L.-H., Reusser, A., Künzli, N., & Bonhoeffer, J. (2020). Safety of Co-Administration Versus Separate Administration of the Same Vaccines in Children: A Systematic Literature Review. Vaccines, 8(1), 12. https://doi.org/10.3390/vaccines8010012