
Characteristics and Outcomes for Recipients of NVX-CoV2373: A Real-World Retrospective Study in Germany

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
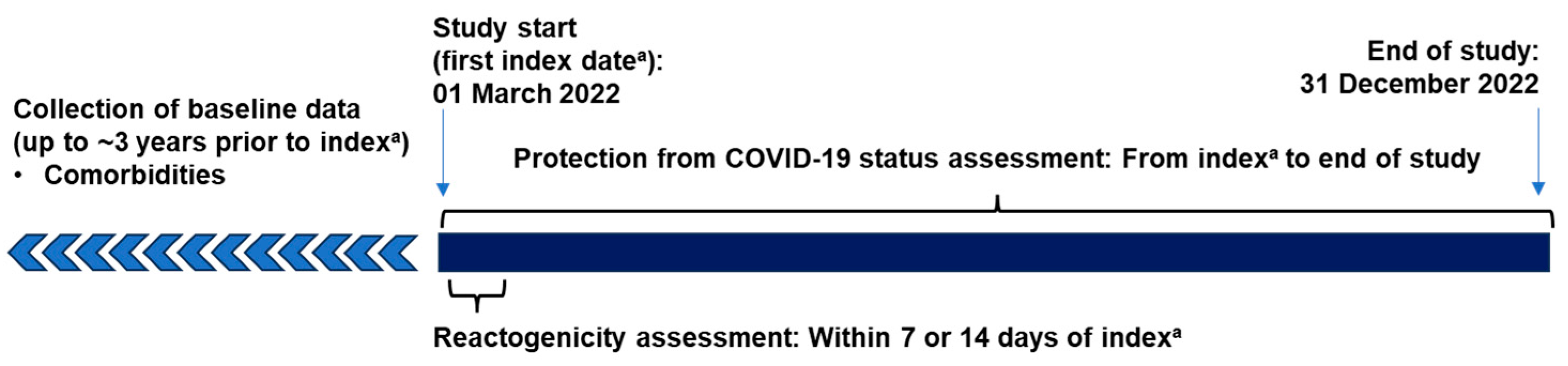
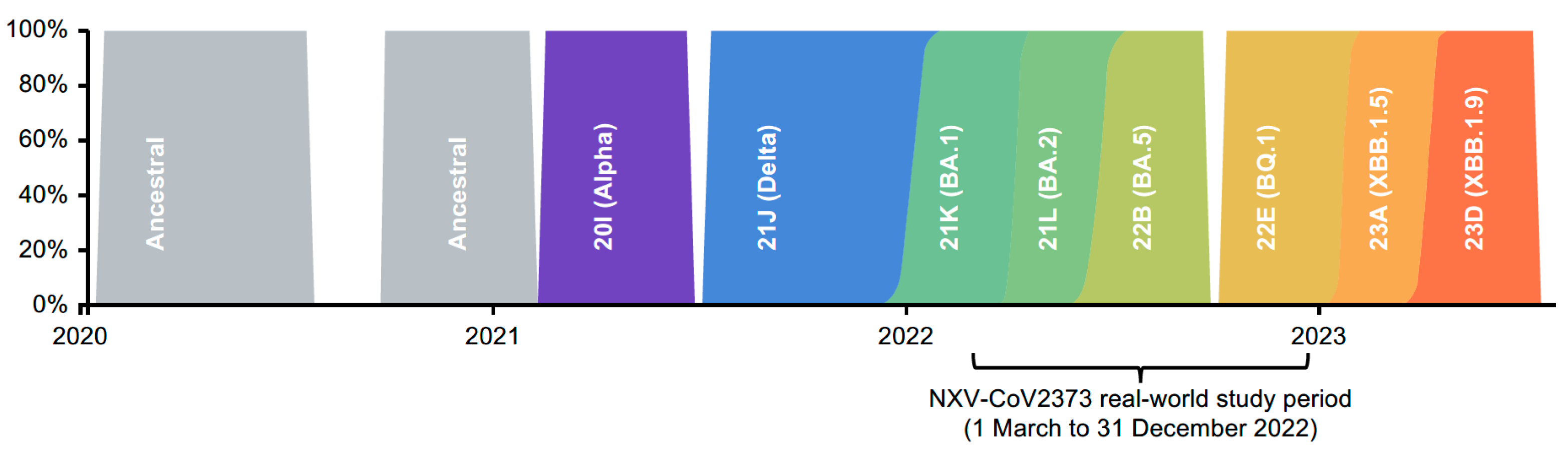
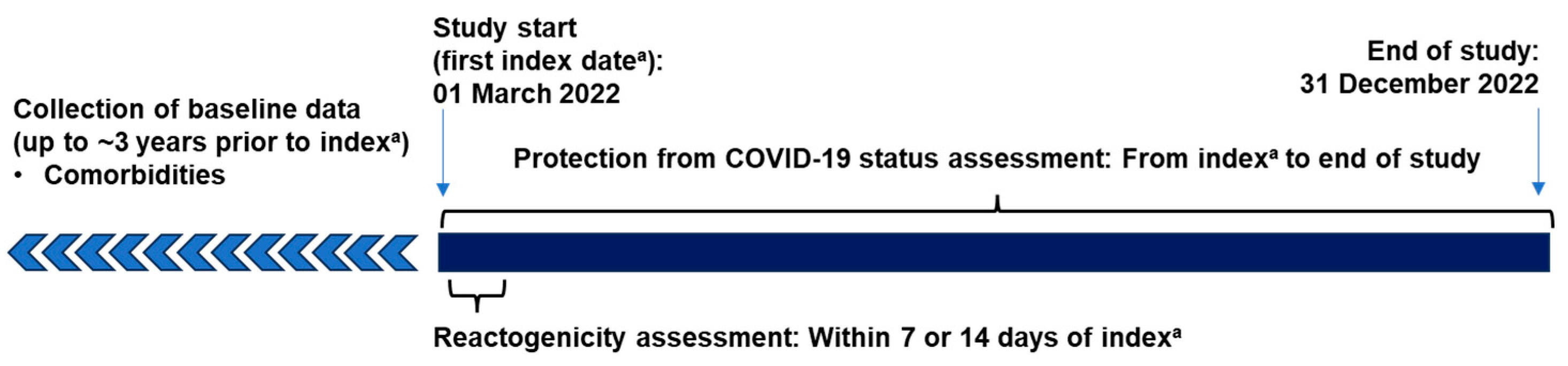
2.1. Study Design and Recipients
2.2. Study Objectives
2.3. Outcomes
2.4. Statistical Analysis
3. Results
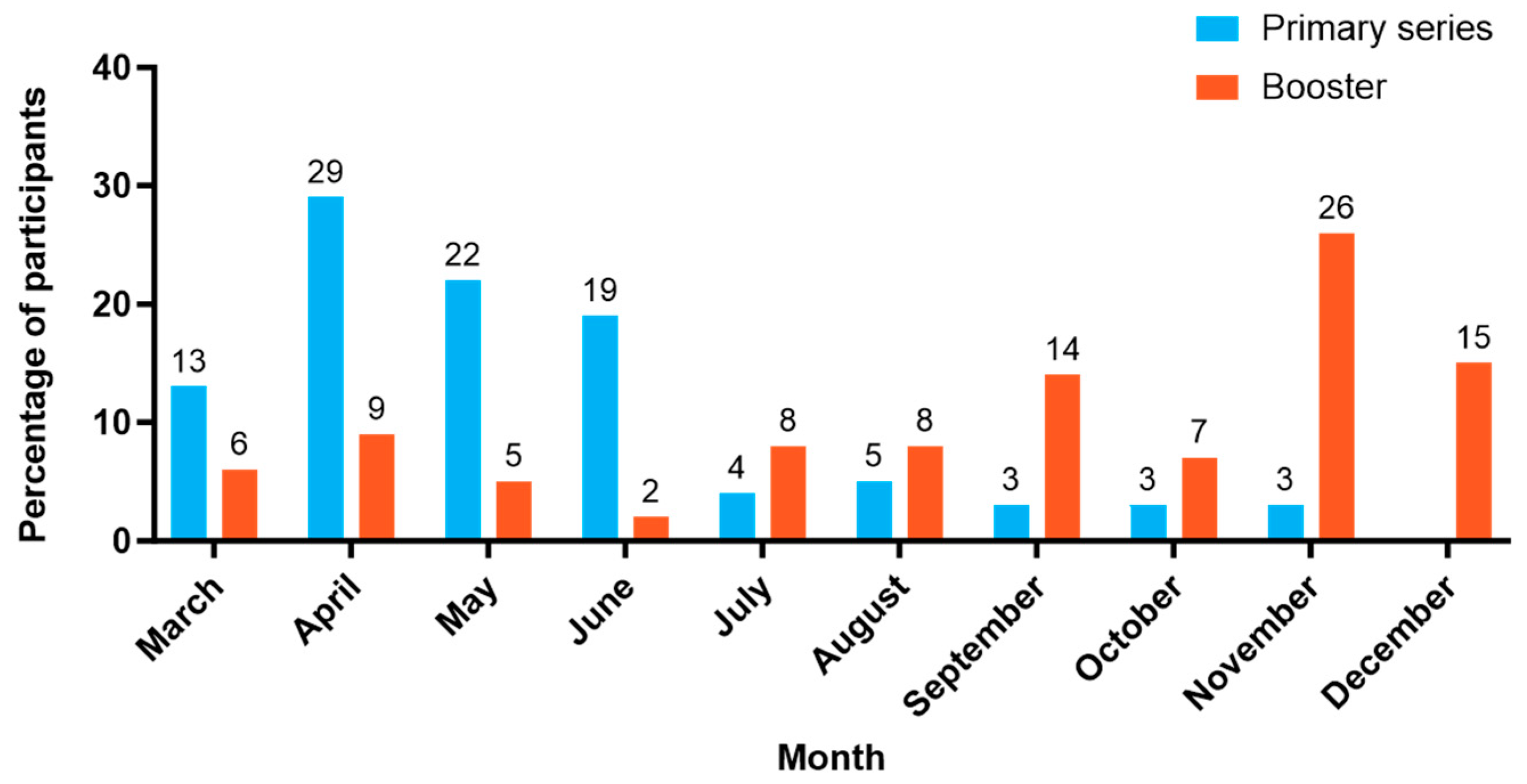
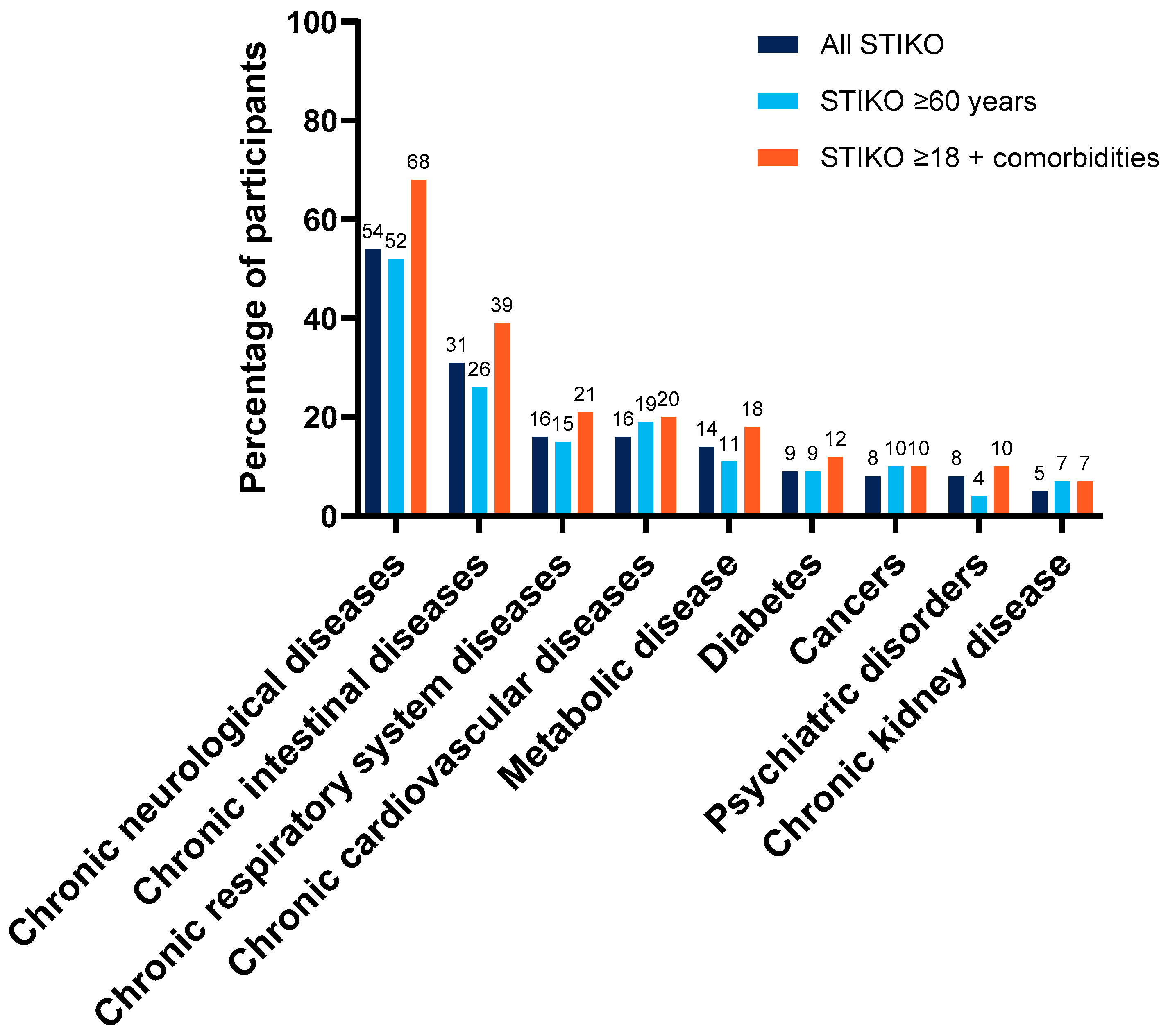
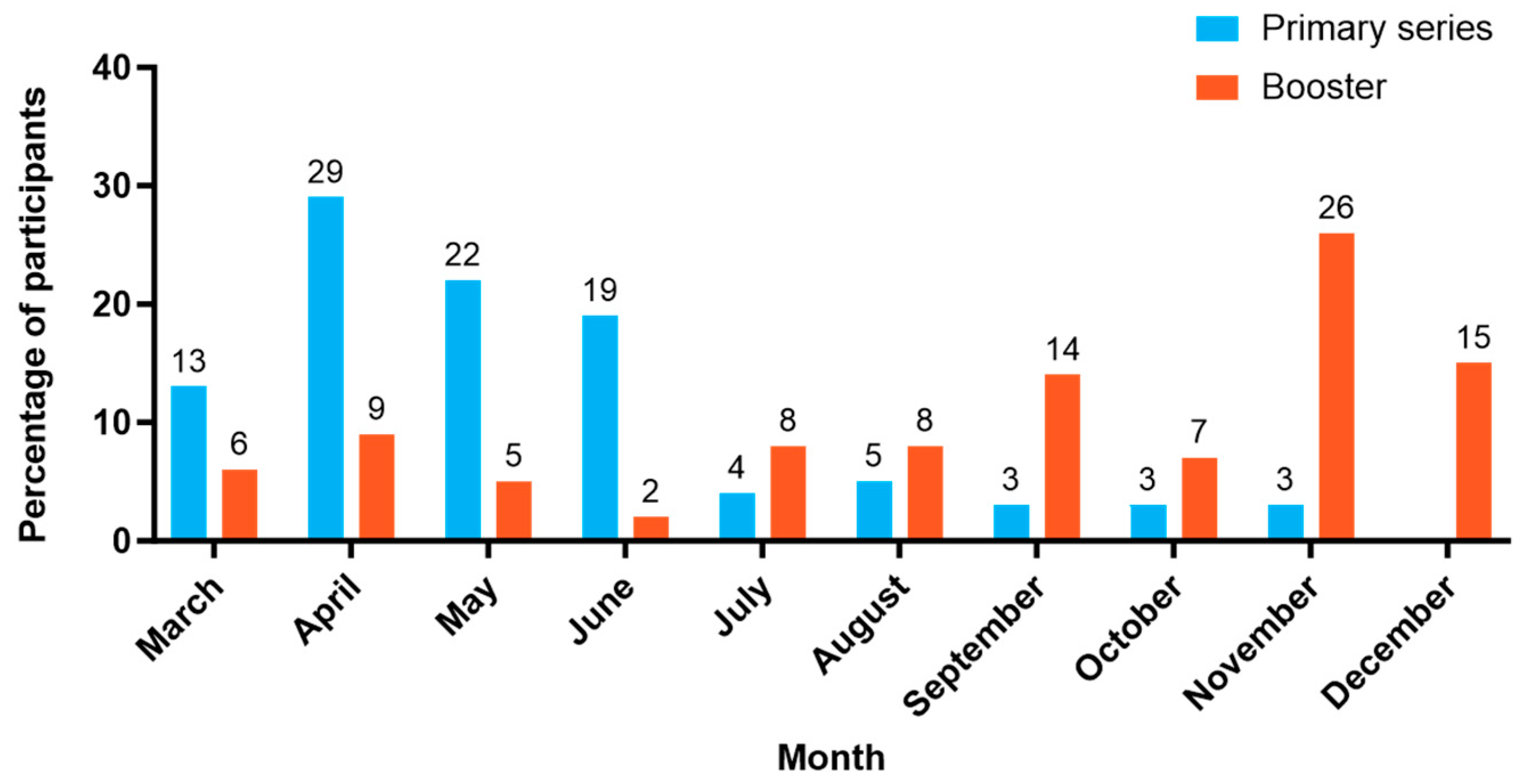
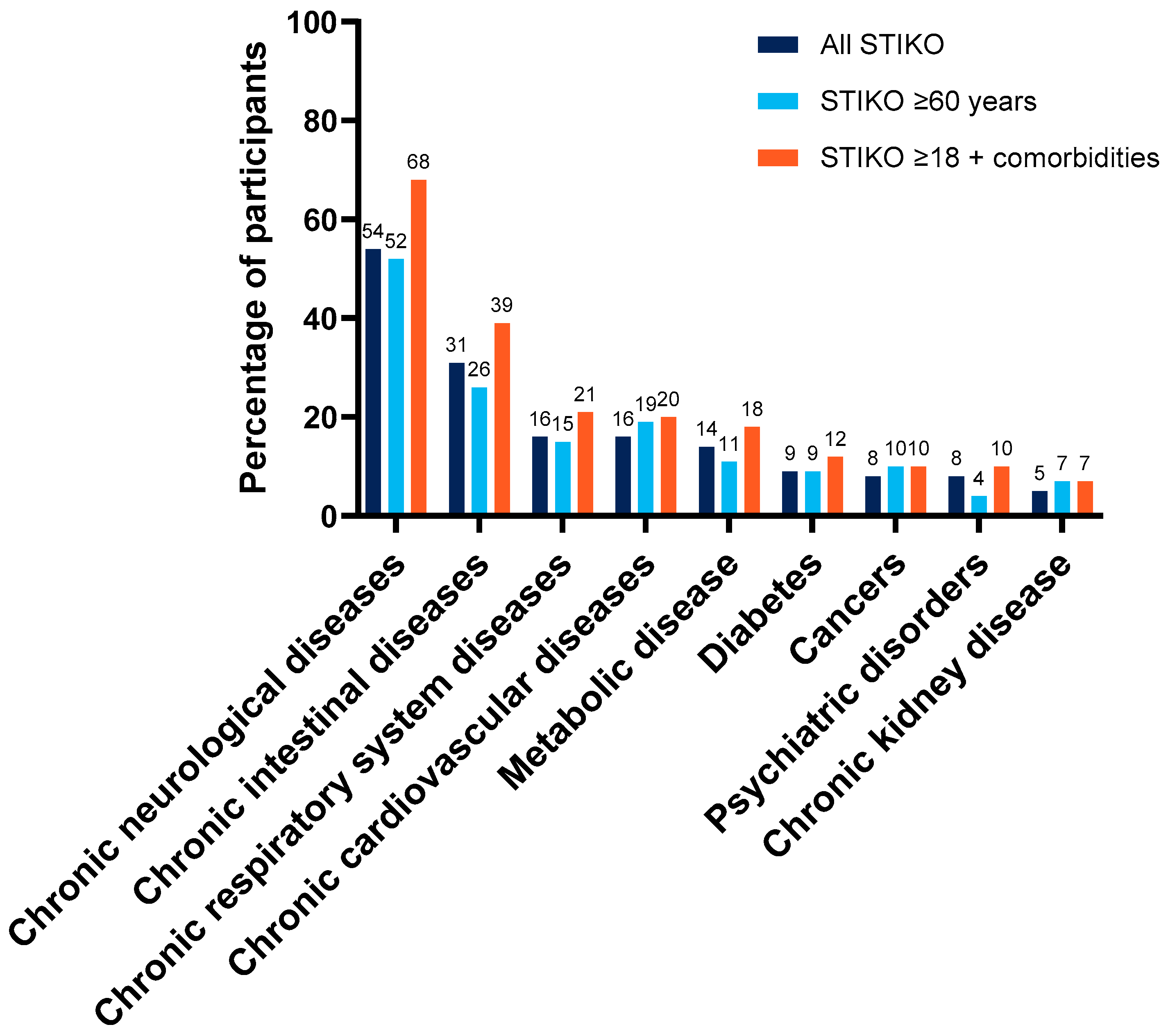
3.1. Recipient Characteristics
3.2. Tolerability-Related Outcomes
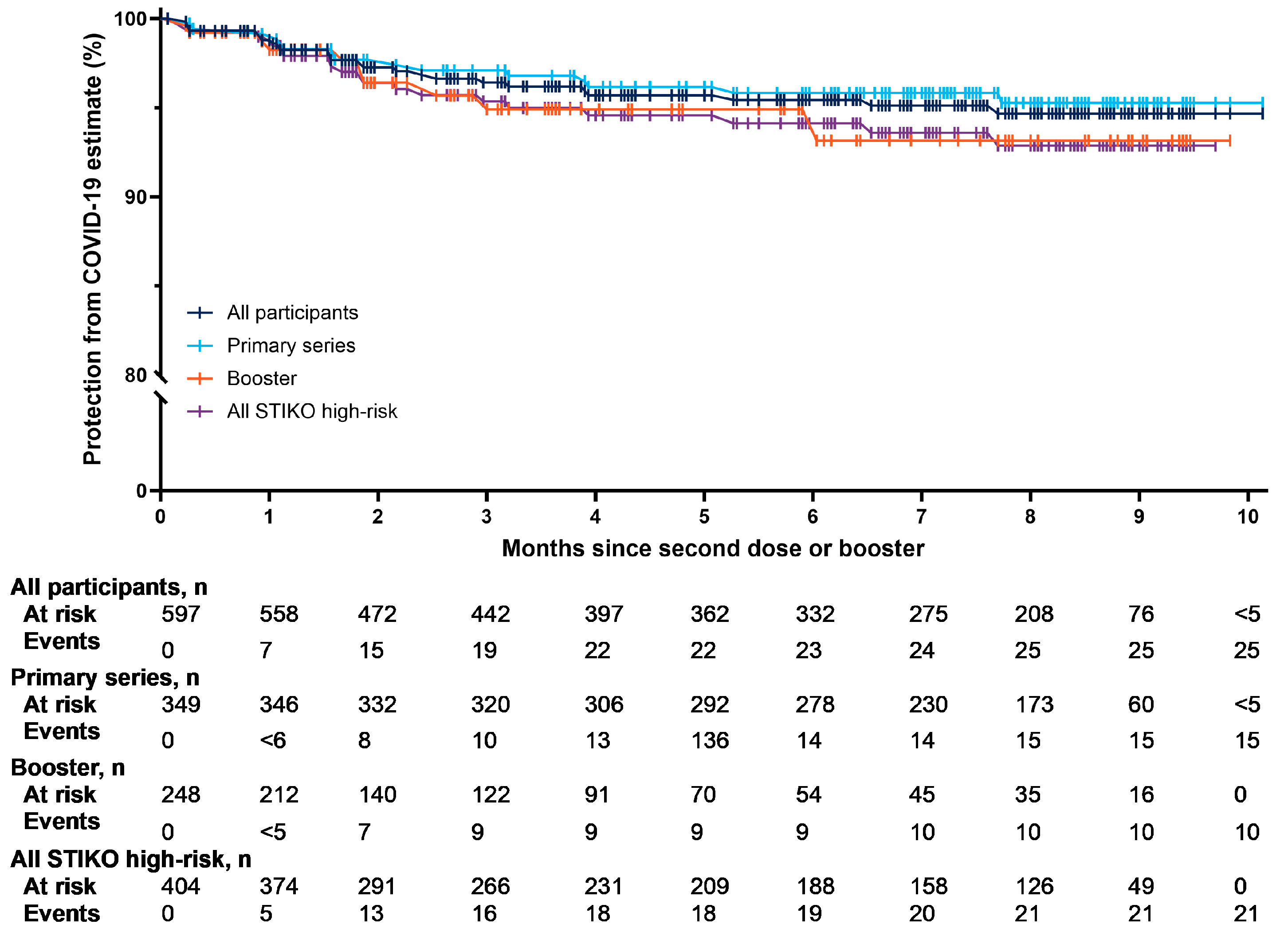
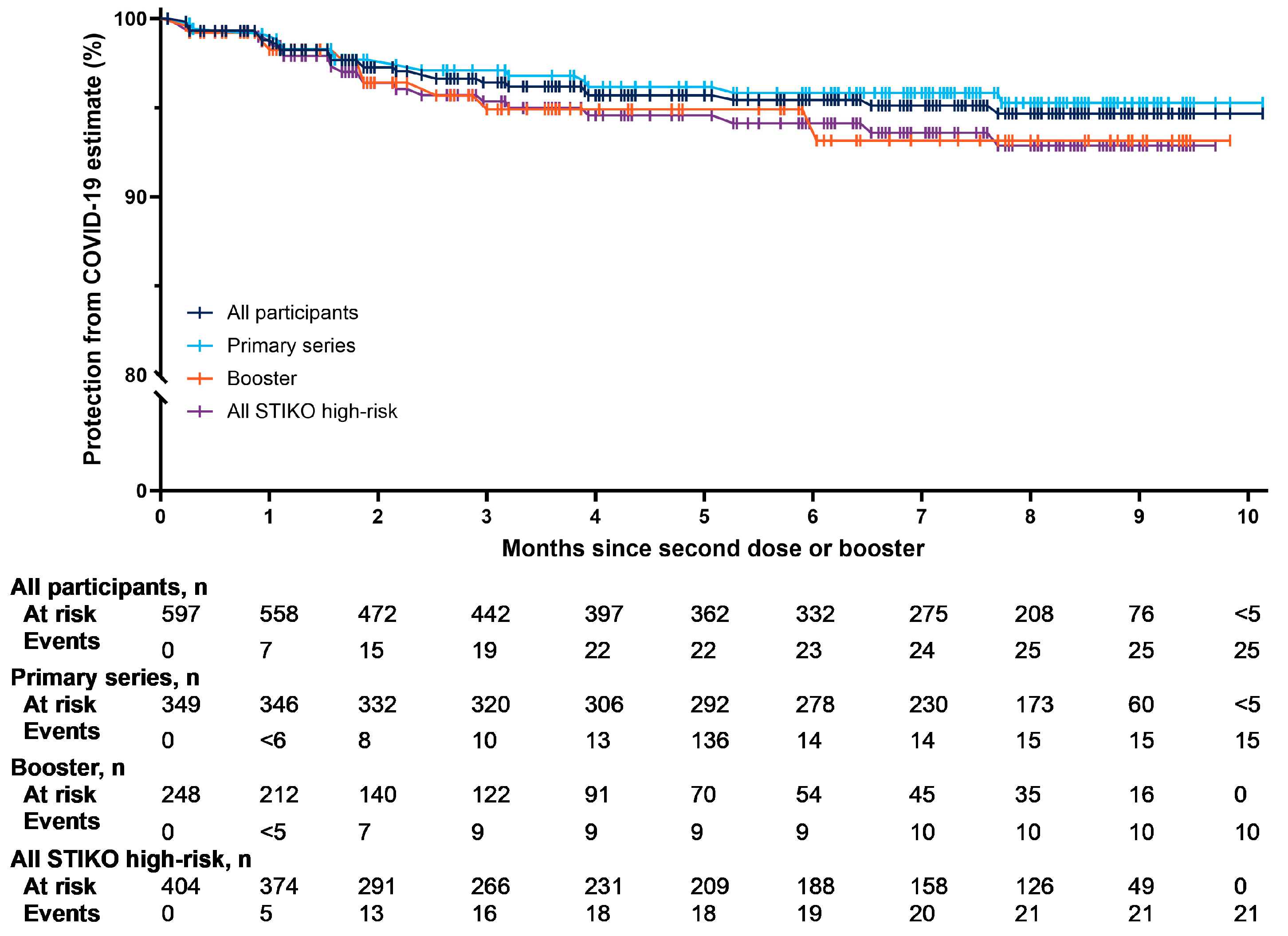
3.3. Protection from COVID-19
4. Discussion
5. Conclusions and Future Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carabelli, A.M.; Peacock, T.P.; Thorne, L.G.; Harvey, W.T.; Hughes, J.; Consortium, C.-G.U.; Peacock, S.J.; Barclay, W.S.; de Silva, T.I.; Towers, G.J.; et al. SARS-CoV-2 variant biology: Immune escape, transmission and fitness. Nat. Rev. Microbiol. 2023, 21, 162–177. [Google Scholar] [CrossRef] [PubMed]
- Anez, G.; Dunkle, L.M.; Gay, C.L.; Kotloff, K.L.; Adelglass, J.M.; Essink, B.; Campbell, J.D.; Cloney-Clark, S.; Zhu, M.; Plested, J.S.; et al. Safety, Immunogenicity, and Efficacy of the NVX-CoV2373 COVID-19 Vaccine in Adolescents: A Randomized Clinical Trial. JAMA Netw. Open 2023, 6, e239135. [Google Scholar] [CrossRef] [PubMed]
- Dunkle, L.M.; Kotloff, K.L.; Gay, C.L.; Anez, G.; Adelglass, J.M.; Barrat Hernandez, A.Q.; Harper, W.L.; Duncanson, D.M.; McArthur, M.A.; Florescu, D.F.; et al. Efficacy and Safety of NVX-CoV2373 in Adults in the United States and Mexico. N. Engl. J. Med. 2022, 386, 531–543. [Google Scholar] [CrossRef] [PubMed]
- Heath, P.T.; Galiza, E.P.; Baxter, D.N.; Boffito, M.; Browne, D.; Burns, F.; Chadwick, D.R.; Clark, R.; Cosgrove, C.; Galloway, J.; et al. Safety and Efficacy of NVX-CoV2373 COVID-19 Vaccine. N. Engl. J. Med. 2021, 385, 1172–1183. [Google Scholar] [CrossRef] [PubMed]
- Heath, P.T.; Galiza, E.P.; Baxter, D.N.; Boffito, M.; Browne, D.; Burns, F.; Chadwick, D.R.; Clark, R.; Cosgrove, C.A.; Galloway, J.; et al. Safety and Efficacy of the NVX-CoV2373 Coronavirus Disease 2019 Vaccine at Completion of the Placebo-Controlled Phase of a Randomized Controlled Trial. Clin. Infect. Dis. 2023, 76, 398–407. [Google Scholar] [CrossRef] [PubMed]
- Alves, K.; Plested, J.S.; Galbiati, S.; Chau, G.; Cloney-Clark, S.; Zhu, M.; Kalkeri, R.; Patel, N.; Smith, K.; Marcheschi, A.; et al. Immunogenicity and safety of a fourth homologous dose of NVX-CoV2373. Vaccine 2023, 41, 4280–4286. [Google Scholar] [CrossRef] [PubMed]
- Mallory, R.M.; Formica, N.; Pfeiffer, S.; Wilkinson, B.; Marcheschi, A.; Albert, G.; McFall, H.; Robinson, M.; Plested, J.S.; Zhu, M.; et al. Safety and immunogenicity following a homologous booster dose of a SARS-CoV-2 recombinant spike protein vaccine (NVX-CoV2373): A secondary analysis of a randomised, placebo-controlled, phase 2 trial. Lancet Infect. Dis. 2022, 22, 1565–1576. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Nuvaxovid. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/nuvaxovid#authorisation-details-section (accessed on 4 December 2023).
- Robert Koch Institute. Decision on the Implementation of the COVID-19 Vaccination into the General Recommendations of the STIKO 2023: STIKO Recommendation on COVID-19 Vaccination. Available online: https://www.rki.de/EN/Content/infections/Vaccination/recommandations/implementation_covid-19_vaccination.pdf?__blob=publicationFile (accessed on 2 November 2023).
- Robert Koch Institute. Aktualisierung der COVID-19-Impfempfehlung Epidemiologisches Bulletin 8/2023. Available online: https://www.rki.de/DE/Content/Infekt/EpidBull/Archiv/2023/Ausgaben/08_23.pdf?__blob=publicationFile (accessed on 2 November 2023).
- Rathmann, W.; Bongaerts, B.; Carius, H.J.; Kruppert, S.; Kostev, K. Basic characteristics and representativeness of the German Disease Analyzer database. Int. J. Clin. Pharmacol. Ther. 2018, 56, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Kang, M.; Zhao, N.; Zhuang, Y.; Li, S.; Song, T. Comprehensive narrative review of real-world COVID-19 vaccines: Viewpoints and opportunities. Med. Rev. 2022, 2, 169–196. [Google Scholar] [CrossRef] [PubMed]
- Marchese, A.M.; Beyhaghi, H.; Orenstein, W.A. With established safe and effective use, protein vaccines offer another choice against COVID-19. Vaccine 2022, 40, 6567–6569. [Google Scholar] [CrossRef] [PubMed]
- Marchese, A.M.; Kalkeri, R.; Vadivale, M.; Suntronwong, N.; Toback, S.; Poovorawan, Y. Pivoting to protein: The immunogenicity and safety of protein-based NVX-CoV2373 as a heterologous booster for inactivated and viral vector COVID-19 vaccines. Expert Rev. Vaccines 2023, 22, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Bauernfeind, S.; Huppertz, G.; Mueller, K.; Hitzenbichler, F.; Hardmann, L.; Pemmerl, S.; Hollnberger, H.; Sieber, W.; Wettstein, M.; Seeliger, S.; et al. Health Care Workers’ Sick Leave due to COVID-19 Vaccination in Context With SARS-CoV-2 Infection and Quarantine-A Multicenter Cross-Sectional Survey. Open Forum Infect. Dis. 2022, 9, ofac203. [Google Scholar] [CrossRef] [PubMed]
- Faramarzi, A.; Javan-Noughabi, J.; Tabatabaee, S.S.; Najafpoor, A.A.; Rezapour, A. The lost productivity cost of absenteeism due to COVID-19 in health care workers in Iran: A case study in the hospitals of Mashhad University of Medical Sciences. BMC Health Serv. Res. 2021, 21, 1169. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Recipients (n = 597) | Primary Series (n = 349) | Booster (n = 248) |
|---|---|---|---|
| Age, median years (IQR) | 58 (44–73) | 51 (39–63) | 71 (56–81) |
| Gender, % | |||
| Male | 46 | 42 | 51 |
| Female | 54 | 58 | 49 |
| Unknown | NA | NA | 0 |
| Median follow-up, months (IQR) | 7 (3–8) | 8 (7–9) | 3 (2–6) |
| Treating physician, % | |||
| General practitioner | 81 | 81 | 82 |
| Specialist | 19 | 19 | 18 |
| Geographical region, % | |||
| East Germany | 56 | 39 | 81 |
| West Germany | 44 | 61 | 19 |
| STIKO high-risk group, % | 68 | 58 | 81 |
| Age ≥ 60 years | 46 | 29 | 69 |
| Age ≥ 18 years + comorbidity | 53 | 45 | 65 |
| Care-facility resident | 3 | NA | NA |
| Characteristic | Age 12–35 (n = 78) | Age 36–59 (n = 245) | Age ≥ 60 (n = 274) |
|---|---|---|---|
| Age, median (IQR) years | 28 (23–33) | 49 (43–56) | 74 (67–82) |
| Gender, % | |||
| Female | 53 | 58 | 51 |
| Male | 47 | 42 | 49 |
| Unknown | 0 | 0 | NA |
| Median follow-up, months (IQR) | 8 (6–9) | 7 (6–8) | 4 (2–8) |
| Treating physician, % | |||
| General practitioner | 72 | 73 | 91 |
| Specialist | 28 | 27 | 9 |
| Geographical region, % | |||
| East Germany | 40 | 50 | 67 |
| West Germany | 60 | 50 | 33 |
| STIKO high-risk group, % | 24 | 45 | 100 |
| Age ≥ 60 years | – | – | 100 |
| Age ≥ 18 years + comorbidity | 24 | 45 | 68 |
| Care-facility resident | 0 | 0 | 7 |
| Baseline Comorbidity a, % | All Recipients (n = 597) | Primary Series (n = 349) | Booster (n = 248) |
|---|---|---|---|
| ≥1 STIKO high-risk comorbidity | 53 | 45 | 65 |
| ≥2 STIKO high-risk comorbidity | 30 | 23 | 40 |
| ≥3 STIKO high-risk comorbidity | 17 | 13 | 23 |
| Chronic neurological disease | 36 | 29 | 47 |
| Chronic intestinal disease | 21 | 19 | 24 |
| Chronic respiratory disease | 11 | 9 | 13 |
| Chronic cardiovascular disease | 11 | 6 | 17 |
| Metabolic disease (including obesity and diabetes mellitus) | 10 | 9 | 10 |
| Diabetes | 6 | 6 | 4 |
| Psychiatric disorder | 5 | 6 | 4 |
| Cancer | 5 | 2 | 10 |
| Chronic kidney disease | 4 | 2 | 5 |
| Dementia or intellectual disability | 2 | NA | NA |
| Chronic liver disease (including cirrhosis) | 1 | NA | NA |
| Autoimmune disease (including rheumatologic diseases) | NA | NA | NA |
| Congenital/acquired immunodeficiency or immunosuppression b | NA | NA | – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kutikova, L.; Brash, J.T.; Helme, K.; Brewster, J.; Brand, M.; Adam, A.; Seager, S.; Kostev, K.; Schelling, J. Characteristics and Outcomes for Recipients of NVX-CoV2373: A Real-World Retrospective Study in Germany. Vaccines 2024, 12, 387. https://doi.org/10.3390/vaccines12040387
Kutikova L, Brash JT, Helme K, Brewster J, Brand M, Adam A, Seager S, Kostev K, Schelling J. Characteristics and Outcomes for Recipients of NVX-CoV2373: A Real-World Retrospective Study in Germany. Vaccines. 2024; 12(4):387. https://doi.org/10.3390/vaccines12040387
Chicago/Turabian StyleKutikova, Lucie, James T. Brash, Kawitha Helme, Jack Brewster, Milou Brand, Atif Adam, Sarah Seager, Karel Kostev, and Jörg Schelling. 2024. "Characteristics and Outcomes for Recipients of NVX-CoV2373: A Real-World Retrospective Study in Germany" Vaccines 12, no. 4: 387. https://doi.org/10.3390/vaccines12040387
APA StyleKutikova, L., Brash, J. T., Helme, K., Brewster, J., Brand, M., Adam, A., Seager, S., Kostev, K., & Schelling, J. (2024). Characteristics and Outcomes for Recipients of NVX-CoV2373: A Real-World Retrospective Study in Germany. Vaccines, 12(4), 387. https://doi.org/10.3390/vaccines12040387