
Status of Routine Immunization Coverage in the World Health Organization African Region Three Years into the COVID-19 Pandemic

 , ,
, ,  , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Data Sources and Measurement
2.3. Data Analysis
- The percentage of difference in immunization coverage in 2022 compared to 2019 (pre-pandemic period): the coverage of the year under review divided by the 2019 coverage minus one and multiplied by one hundred. To calculate a percentage difference in the few countries in which coverage was null in 2019 but non-zero in 2022, coverage in 2019 was set to one.
- The number of zero-dose (ZD) children: the number of surviving infants (aged 0–11 months) for a given year (from the United Nations (UN) Population Estimates 2022 revision) [16] minus the number of children vaccinated with the DTP1 during the same year.
- The number of un-immunized children for vaccines other than the DTP: the number of the target population for a given year and antigen (from UN Population Estimates 2022 revision) [16] minus the number of children vaccinated with the related vaccine during the same year.
- The number of under-immunized children: the number of children vaccinated with the last dose of a given vaccine minus the number of children vaccinated with the first dose of the same vaccine.
- The percentage of ZD children: the number of zero-dose children divided by the number of surviving infants for the same period, multiplied by 100.
- The number ZD children per one thousand population: number of zero-dose children divided by the total population (UN population Estimates) for the same period, multiplied by 1000.
3. Results
3.1. Overview of Data Reported
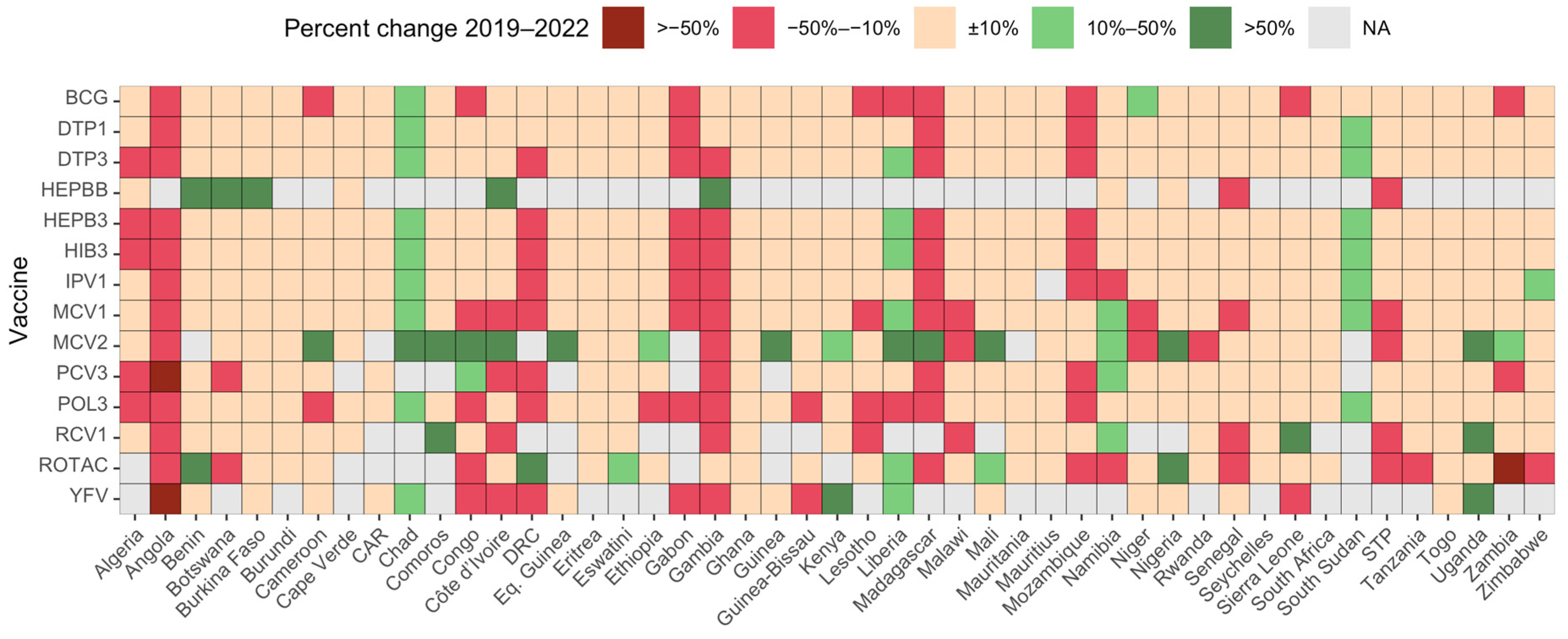
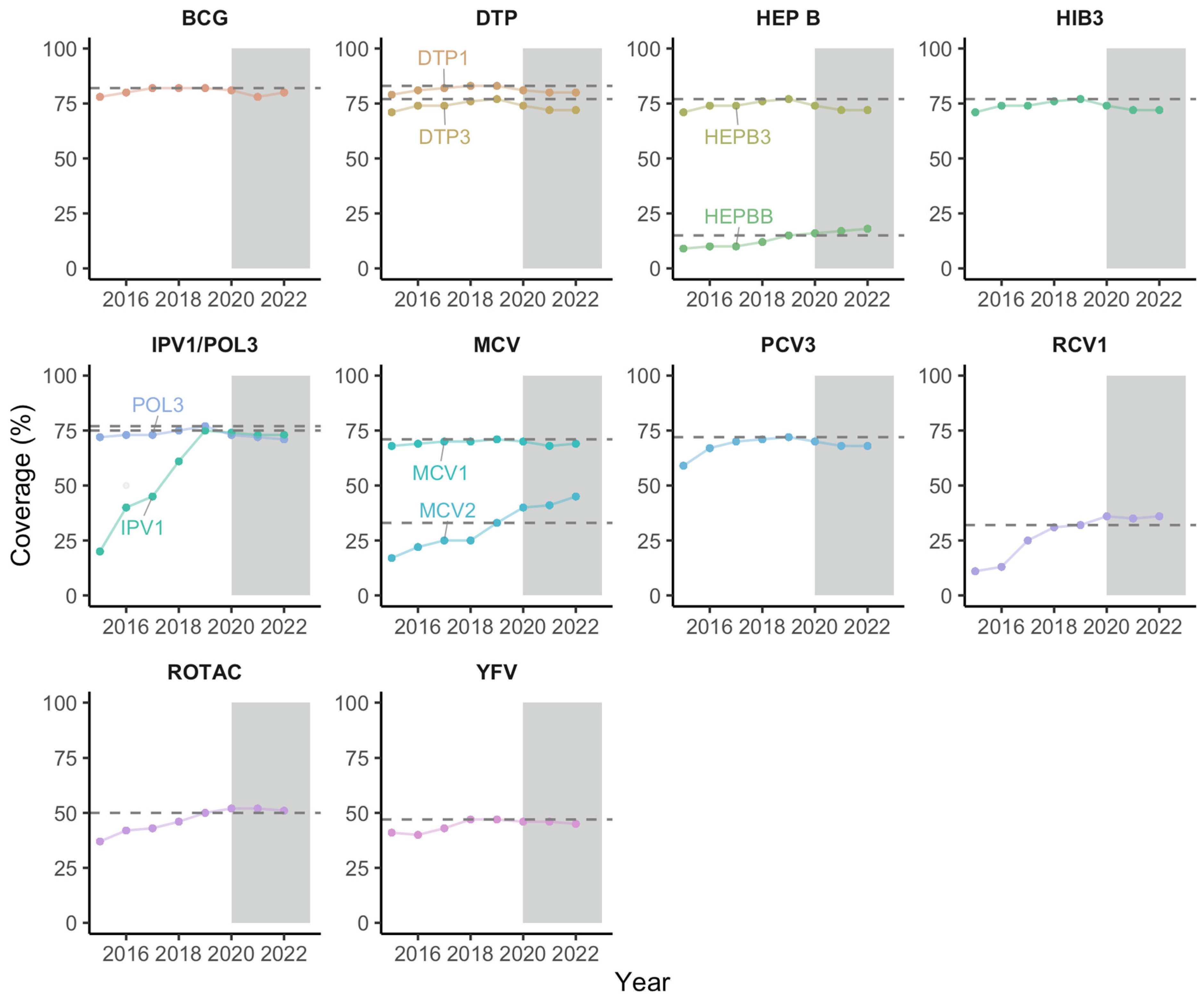
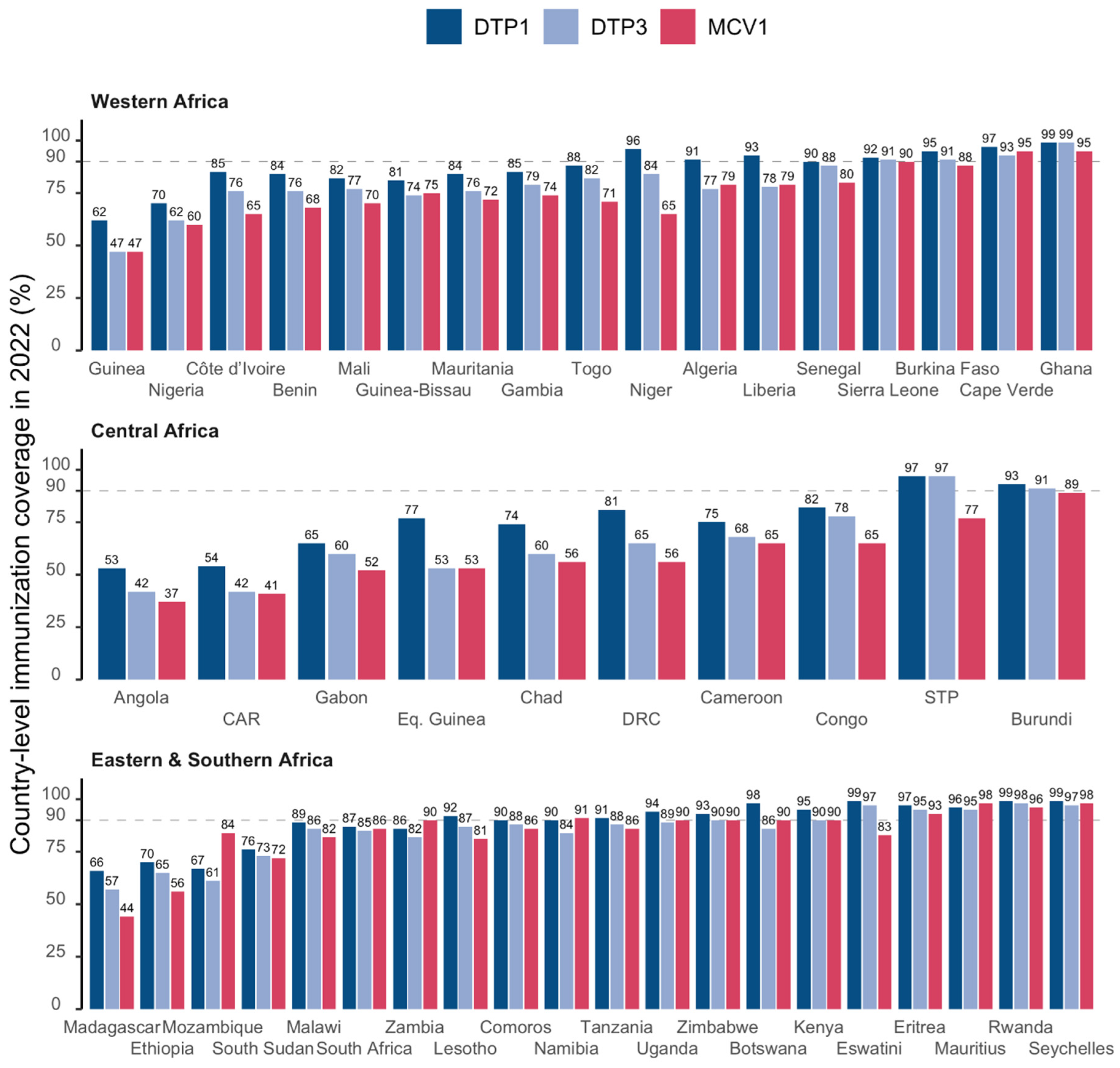
3.2. Immunization Coverage Trends
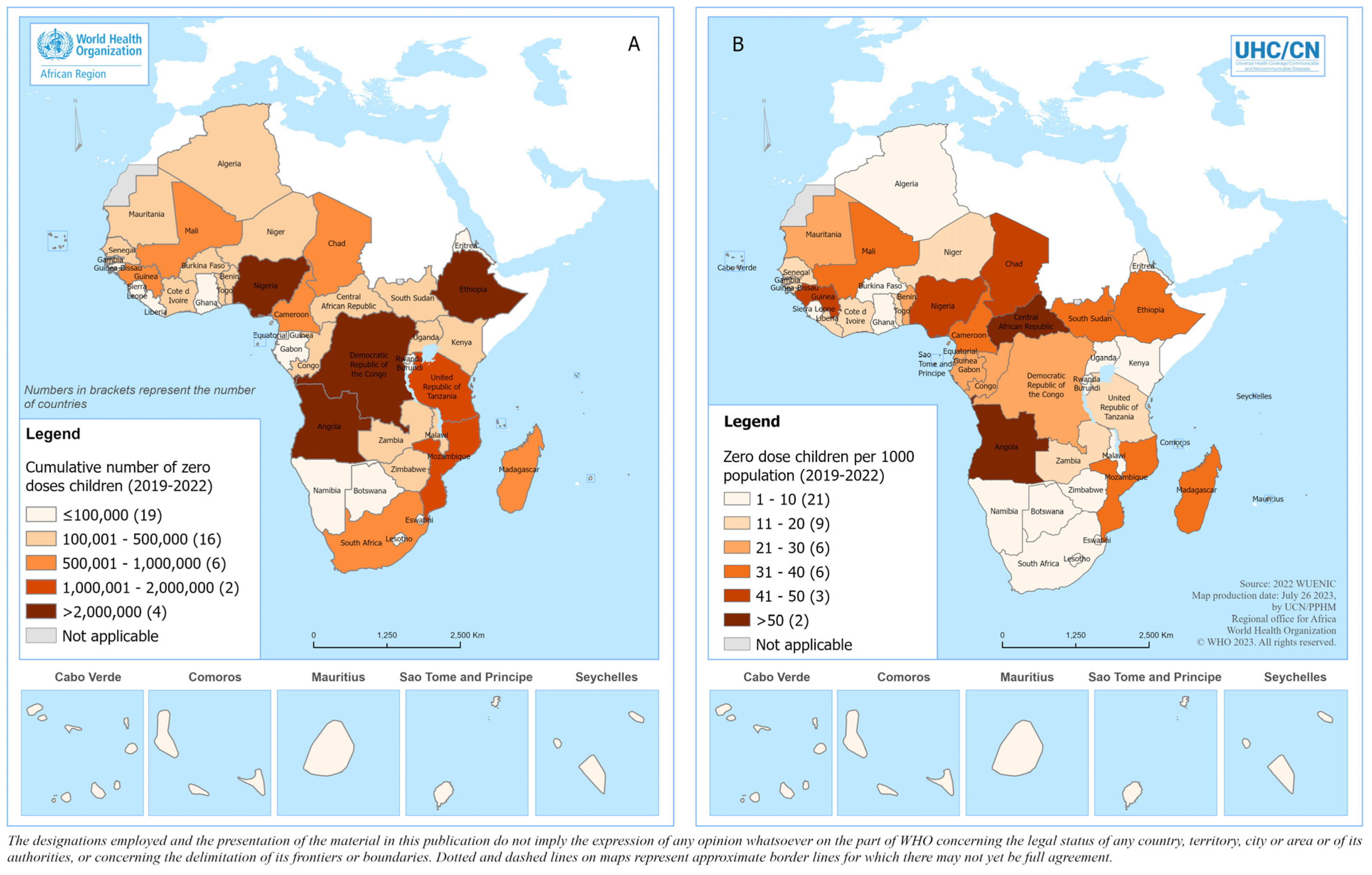
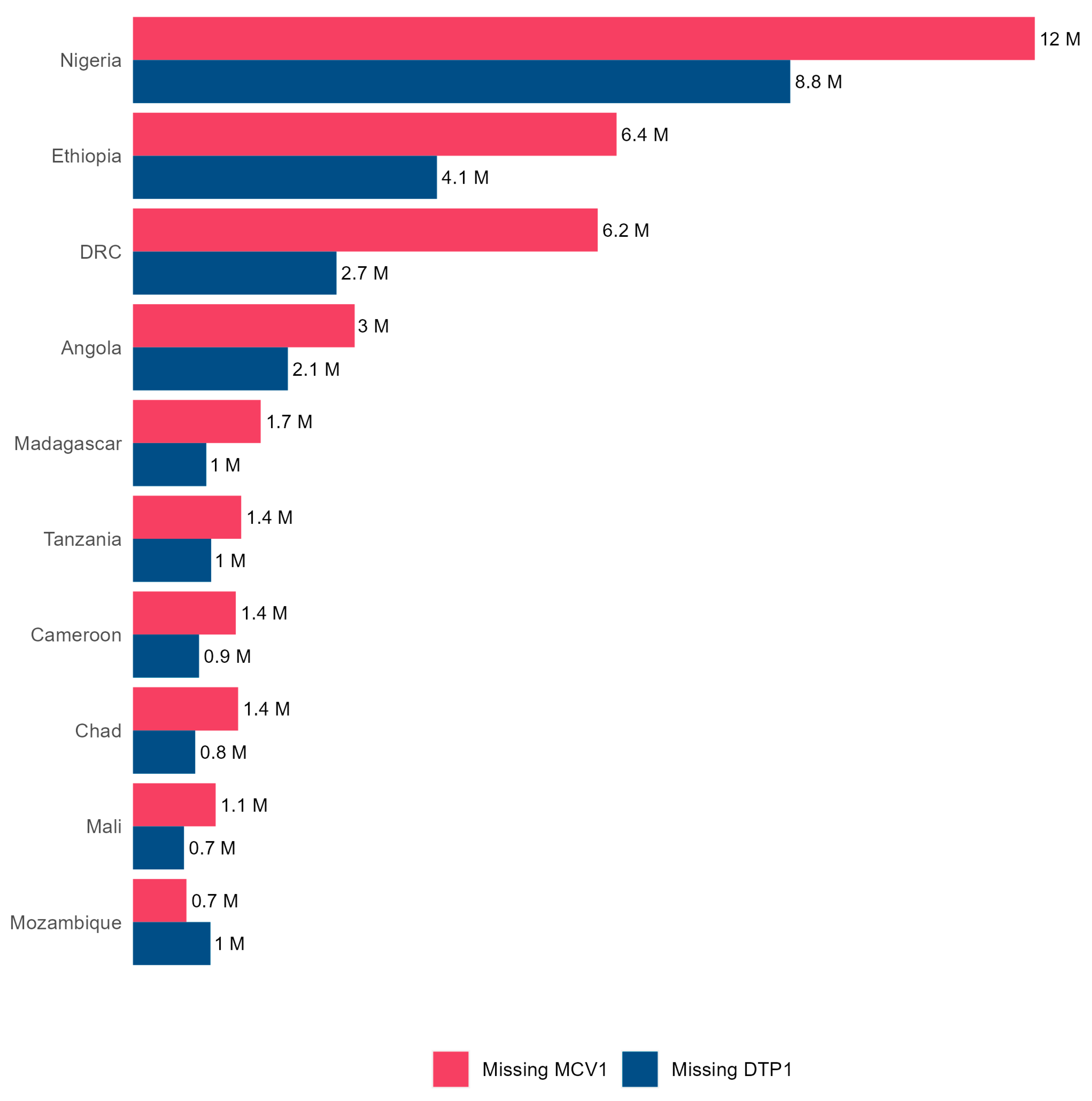
3.3. Un- and Under-Immunized Children
3.4. WUENIC and Administrative Coverage Data Comparison
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Gaythorpe, K.A.; Abbas, K.; Huber, J.; Karachaliou, A.; Thakkar, N.; Woodruff, K.; Li, X.; Echeverria-Londono, S.; Ferrari, M. Impact of COVID-19-related disruptions to measles, meningococcal A, and yellow fever vaccination in 10 countries. eLife 2021, 10, e67023. [Google Scholar] [CrossRef]
- Masresha, B.G.; Luce, R., Jr.; Shibeshi, M.E.; Ntsama, B.; N’Diaye, A.; Chakauya, J.; Poy, A.; Mihigo, R. The performance of routine immunization in selected African countries during the first six months of the COVID-19 pandemic. Pan Afr. Med. J. 2020, 37, 12. [Google Scholar] [CrossRef]
- Saidu, Y.; Di Mattei, P.; Nchinjoh, S.C.; Edwige, N.N.; Nsah, B.; Muteh, N.J.; Ndoula, S.T.; Abdullahi, R.; Zamir, C.S.; Njoh, A.A.; et al. The Hidden Impact of the COVID-19 Pandemic on Routine Childhood Immunization Coverage in Cameroon. Vaccines 2023, 11, 645. [Google Scholar] [CrossRef] [PubMed]
- Babatunde, O.A.; Olatunji, M.B.; Omotajo, O.R.; Ikwunne, O.I.; Babatunde, A.M.; Nihinlola, E.T.; Patrick, G.F.; Dairo, D.M. Impact of COVID-19 on routine immunization in Oyo State, Nigeria: Trend analysis of immunization data in the pre-and post-index case period; 2019–2020. Pan Afr. Med. J. 2022, 41, 54. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. About WHO: Regional Office for Africa. Available online: https://www.afro.who.int/countries (accessed on 1 February 2023).
- Impouma, B.; Mboussou, F.; Farham, B.; Wolfe, C.M.; Johnson, K.; Clary, C.; Mihigo, R.; Nsenga, N.; Talisuna, A.; Yoti, Z. The COVID-19 pandemic in the WHO African Region: The first year (February 2020 to February 2021). Epidemiol. Infect. 2021, 149, e263. [Google Scholar] [CrossRef] [PubMed]
- Mbow, M.; Lell, B.; Jochems, S.P.; Cisse, B.; Mboup, S.; Dewals, B.G.; Jaye, A.; Dieye, A.; Yazdanbakhsh, M. COVID-19 in Africa: Dampening the storm? Science 2020, 369, 624–626. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Singh, S.K.; Sharma, L.; Dwiwedi, M.K.; Agarwal, D.; Gupta, G.K.; Dhiman, R. Magnitude and causes of routine immunization disruptions during COVID-19 pandemic in developing countries. J. Fam. Med. Prim. Care 2021, 10, 3991. [Google Scholar] [CrossRef] [PubMed]
- Lai, X.; Zhang, H.; Pouwels, K.B.; Patenaude, B.; Jit, M.; Fang, H. Estimating global and regional between-country inequality in routine childhood vaccine coverage in 195 countries and territories from 2019 to 2021: A longitudinal study. eClinicalMedicine 2023, 60, 102042. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Big Catch-Up: An Essential Immunization Recovery Plan for 2023 and Beyond. Available online: https://www.who.int/publications/i/item/9789240075511 (accessed on 10 October 2023).
- World Health Organization. Immunization Agenda 2030: A Global Strategy to Leave No One behind. Available online: https://www.immunizationagenda2030.org (accessed on 16 October 2023).
- World Health Organization. Statement on the Fifteenth Meeting of the IHR (2005) Emergency Committee on the COVID-19 Pandemic. Available online: https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic (accessed on 7 September 2023).
- World Health Organization. WHO/UNICEF Joint Reporting Process. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/who-unicef-joint-reporting-process (accessed on 22 October 2023).
- Burton, A.; Monasch, R.; Lautenbach, B.; Gacic-Dobo, M.; Neill, M.; Karimov, R.; Wolfson, L.; Jones, G.; Birmingham, M. WHO and UNICEF estimates of national infant immunization coverage: Methods and processes. Bull. World Health Organ. 2009, 87, 535–541. [Google Scholar] [CrossRef]
- World Health Organization. Immunization Data. Available online: https://immunizationdata.who.int/listing.html?topic=coverage&location=afr (accessed on 22 October 2023).
- United Nations. World Population Prospects 2022. Available online: https://population.un.org/wpp/ (accessed on 3 October 2023).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Dalton, M.; Sanderson, B.; Robinson, L.J.; Homer, C.S.E.; Pomat, W.; Danchin, M.; Vaccher, S. Impact of COVID-19 on routine childhood immunisations in low- and middle-income countries: A scoping review. PLoS Glob. Public Health 2023, 3, e0002268. [Google Scholar] [CrossRef]
- Ota, M.O.C.; Badur, S.; Romano-Mazzotti, L.; Friedland, L.R. Impact of COVID-19 pandemic on routine immunization. Ann. Med. 2021, 53, 2286–2297. [Google Scholar] [CrossRef] [PubMed]
- Kaur, G. Routine Vaccination Coverage—Worldwide, 2022. MMWR Morb. Mortal Wkly. Rep. 2023, 72, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Immunization Coverage. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 6 November 2023).
- World Health Organization. WHO South-East Asia Region Lauds Countries for Routine Immunization Coverage Scale-Up, Says Accelerated Efforts Must Continue. Available online: https://www.who.int/southeastasia/news/detail/18-07-2023-who-south-east-asia-region-lauds-countries-for-routine-immunization-coverage-scale-up--says-accelerated-efforts-must-continue. (accessed on 6 November 2023).
- Borba, R.C.; Vidal, V.M.; Moreira, L.O. The re-emergency and persistence of vaccine preventable diseases. An. Acad. Bras. Cienc. 2015, 87, 1311–1322. [Google Scholar] [CrossRef] [PubMed]
- IntraAction. Global Rise in Vaccine-Preventable Diseases Highlights Urgent Actions Needed to Save Lives and Alleviate Future Suffering. Available online: https://www.interaction.org/blog/global-rise-in-vaccine-preventable-diseases-highlights-urgent-actions-needed-to-save-lives-and-alleviate-future-suffering/ (accessed on 6 November 2023).
- Adegboye, O.A.; Alele, F.O.; Pak, A.; Castellanos, M.E.; Abdullahi, M.A.S.; Okeke, M.I.; Emeto, T.I.; McBryde, E.S. A resurgence and re-emergence of diphtheria in Nigeria, 2023. Ther. Adv. Infect. Dis. 2023, 10, 20499361231161936. [Google Scholar] [CrossRef] [PubMed]
- Hogan, D.; Gupta, A. Why Reaching Zero-Dose Children Holds the Key to Achieving the Sustainable Development Goals. Vaccines 2023, 11, 781. [Google Scholar] [CrossRef] [PubMed]
- Gavi, the Vaccine Alliance. Reaching Zero-Dose Children. Available online: https://www.gavi.org/our-alliance/strategy/phase-5-2021-2025/equity-goal/zero-dose-children-missed-communities (accessed on 7 November 2023).
- Gavi, the Vaccine Alliance. The Zero-Dose Child: Explained. Available online: https://www.gavi.org/vaccineswork/zero-dose-child-explained (accessed on 7 November 2023).
- O’Brien, K.L.; Lemango, E. The big catch-up in immunisation coverage after the COVID-19 pandemic: Progress and challenges to achieving equitable recovery. Lancet 2023, 402, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Ingle, E.A.; Shrestha, P.; Seth, A.; Lalika, M.S.; Azie, J.I.; Patel, R.C. Interventions to Vaccinate Zero-Dose Children: A Narrative Review and Synthesis. Viruses 2023, 15, 2092. [Google Scholar] [CrossRef]
- Kirkby, K.; Bergen, N.; Schlotheuber, A.; Sodha, S.V.; Danovaro-Holliday, M.C.; Hosseinpoor, A.R. Subnational Inequalities in Diphtheria–Tetanus–Pertussis Immunization in 24 Countries in the African Region. Bull. World Health Organ. 2021, 99, 627. [Google Scholar] [CrossRef]
- IQVIA Middle-East and Africa. Removing the Immunization Barriers for Zero-Dose Children: How to Make It Work. Available online: https://www.iqvia.com/locations/middle-east-and-africa/blogs/2023/02/removing-immunization-barriers-for-zero-dose-children-how-to-make-it-work. (accessed on 7 November 2023).
- World Health Organization. Leave No One Behind: Guidance for Planning and Implementing Catch-Up Vaccination. Available online: https://www.who.int/publications/i/item/9789240016514 (accessed on 10 October 2023).
- World Bank Blogs. How to Finance “The Big Catch-Up”, Allowing More children and Communities to Be Protected from Vaccine-Preventable Diseases. Available online: https://blogs.worldbank.org/health/how-finance-big-catch-allowing-more-children-and-communities-be-protected-vaccine (accessed on 8 November 2023).
- World Health Organization; Regional Office for Africa. African Leaders Call for Urgent Action to Revitalize Routine Immunization. Available online: https://www.afro.who.int/news/african-leaders-call-urgent-action-revitalize-routine-immunization (accessed on 8 November 2023).
- Rau, C.; Lüdecke, D.; Dumolard, L.B.; Grevendonk, J.; Wiernik, B.M.; Kobbe, R.; Gacic-Dobo, M.; Danovaro-Holliday, M.C. Data quality of reported child immunization coverage in 194 countries between 2000 and 2019. PLoS Glob. Public Health 2022, 2, e0000140. [Google Scholar] [CrossRef]
- Mihigo, R.; Okeibunor, J.; Anya, B.; Mkanda, P.; Zawaira, F. Challenges of immunization in the African Region. Pan Afr. Med. J. 2017, 27, 12. [Google Scholar] [CrossRef]
- World Health Organization. Assessing and Improving the Accuracy of Target Population Estimates for Immunization Coverage. Available online: https://www.who.int/publications/m/item/assessing-and-improving-the-accuracy-of-target-population-estimates-for-immunization-coverage (accessed on 2 November 2023).
- Ziema, S.A.; Asem, L. Assessment of immunization data quality of routine reports in Ho municipality of Volta region, Ghana. BMC Health Serv. Res. 2020, 20, 1013. [Google Scholar] [CrossRef]
- Danovaro-Holliday, M.C.; Gacic-Dobo, M.; Diallo, M.S.; Murphy, P.; Brown, D.W. Compliance of WHO and UNICEF Estimates of National Immunization Coverage (WUENIC) with Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) Criteria. Gates Open Res. 2021, 5, 77. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | # Surviving Children | Estimated Number of Vaccinated with DTP1 | Estimated Number of Zero-Dose Children | % Zero-Dose Children |
|---|---|---|---|---|
| 2019 | 36,995,277 | 30,763,363 | 6,231,914 | 16.8 |
| 2020 | 37,521,132 | 30,463,727 | 7,057,405 | 18.8 |
| 2021 | 38,080,516 | 30,439,539 | 7,640,977 | 20.1 |
| 2022 | 38,567,250 | 30,791,574 | 7,775,676 | 20.2 |
| Cumulative 2019–2022 | 151,164,175 | 122,458,203 | 28,705,972 | 19.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© World Health Organization 2024. Licensee MDPI. This article is distributed under the terms of the Creative Commons Attribution IGO License. (https://creativecommons.org/licenses/by/3.0/igo/) which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any reproduction of this article there should not be any suggestion that WHO or this article endorse any specific organization or products. The use of the WHO logo is not permitted.
Share and Cite
Mboussou, F.; Kada, S.; Danovaro-Holliday, M.C.; Farham, B.; Gacic-Dobo, M.; Shearer, J.C.; Bwaka, A.; Amani, A.; Ngom, R.; Vuo-Masembe, Y.; et al. Status of Routine Immunization Coverage in the World Health Organization African Region Three Years into the COVID-19 Pandemic. Vaccines 2024, 12, 168. https://doi.org/10.3390/vaccines12020168
Mboussou F, Kada S, Danovaro-Holliday MC, Farham B, Gacic-Dobo M, Shearer JC, Bwaka A, Amani A, Ngom R, Vuo-Masembe Y, et al. Status of Routine Immunization Coverage in the World Health Organization African Region Three Years into the COVID-19 Pandemic. Vaccines. 2024; 12(2):168. https://doi.org/10.3390/vaccines12020168
Chicago/Turabian StyleMboussou, Franck, Sarah Kada, Maria Carolina Danovaro-Holliday, Bridget Farham, Marta Gacic-Dobo, Jessica C. Shearer, Ado Bwaka, Adidja Amani, Roland Ngom, Yolande Vuo-Masembe, and et al. 2024. "Status of Routine Immunization Coverage in the World Health Organization African Region Three Years into the COVID-19 Pandemic" Vaccines 12, no. 2: 168. https://doi.org/10.3390/vaccines12020168
APA StyleMboussou, F., Kada, S., Danovaro-Holliday, M. C., Farham, B., Gacic-Dobo, M., Shearer, J. C., Bwaka, A., Amani, A., Ngom, R., Vuo-Masembe, Y., Wiysonge, C. S., & Impouma, B. (2024). Status of Routine Immunization Coverage in the World Health Organization African Region Three Years into the COVID-19 Pandemic. Vaccines, 12(2), 168. https://doi.org/10.3390/vaccines12020168