
A Survey of Fear for Others, Fear for Self, and Pandemic Anxiety Predicting Intention to Take the First Booster Vaccine to Combat COVID-19


Abstract
:1. Introduction
1.1. Challenges Facing First Responders (FR) and Frontline Healthcare Professionals (FHP)
1.2. Second-Wave Threat of COVID-19
1.3. Experimental Fear Appeal Research Related to COVID-19
1.4. Altruistic Fear (FOTH)
Research on fear of crime in the United States has concentrated on personal fear while overlooking the fear that people have for others in their lives—children, spouses, friends—whose safety they value…. Altruistic fear (fear for others) has a distinctive structure in family households and is more common and often more intense than personal fear.(p. 551)
1.5. Distinct Nature of Anxiety
2. Materials and Methods
2.1. Research Questions
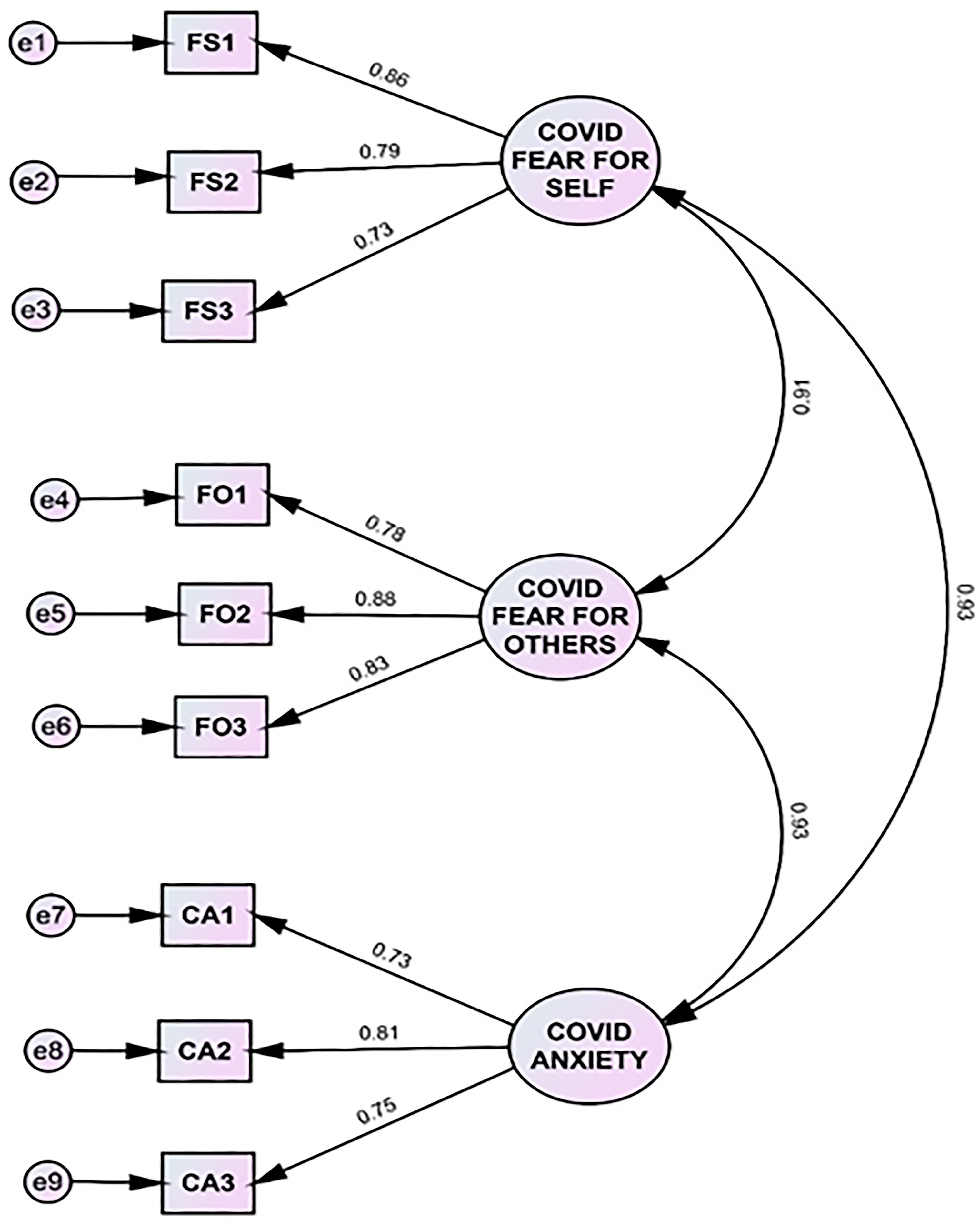
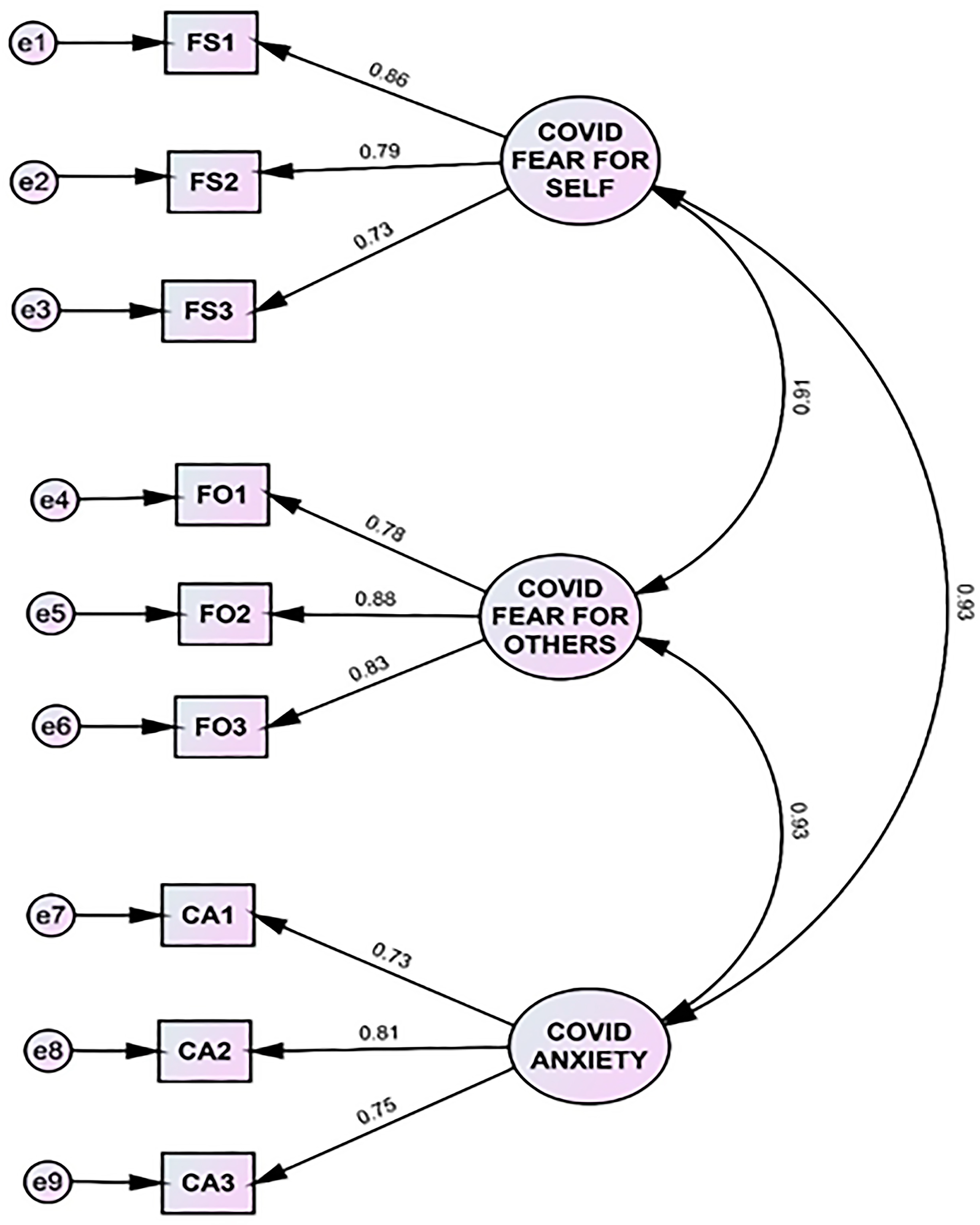
- RQ1: Are FSELF, FOTH and CANX unique independent measures?
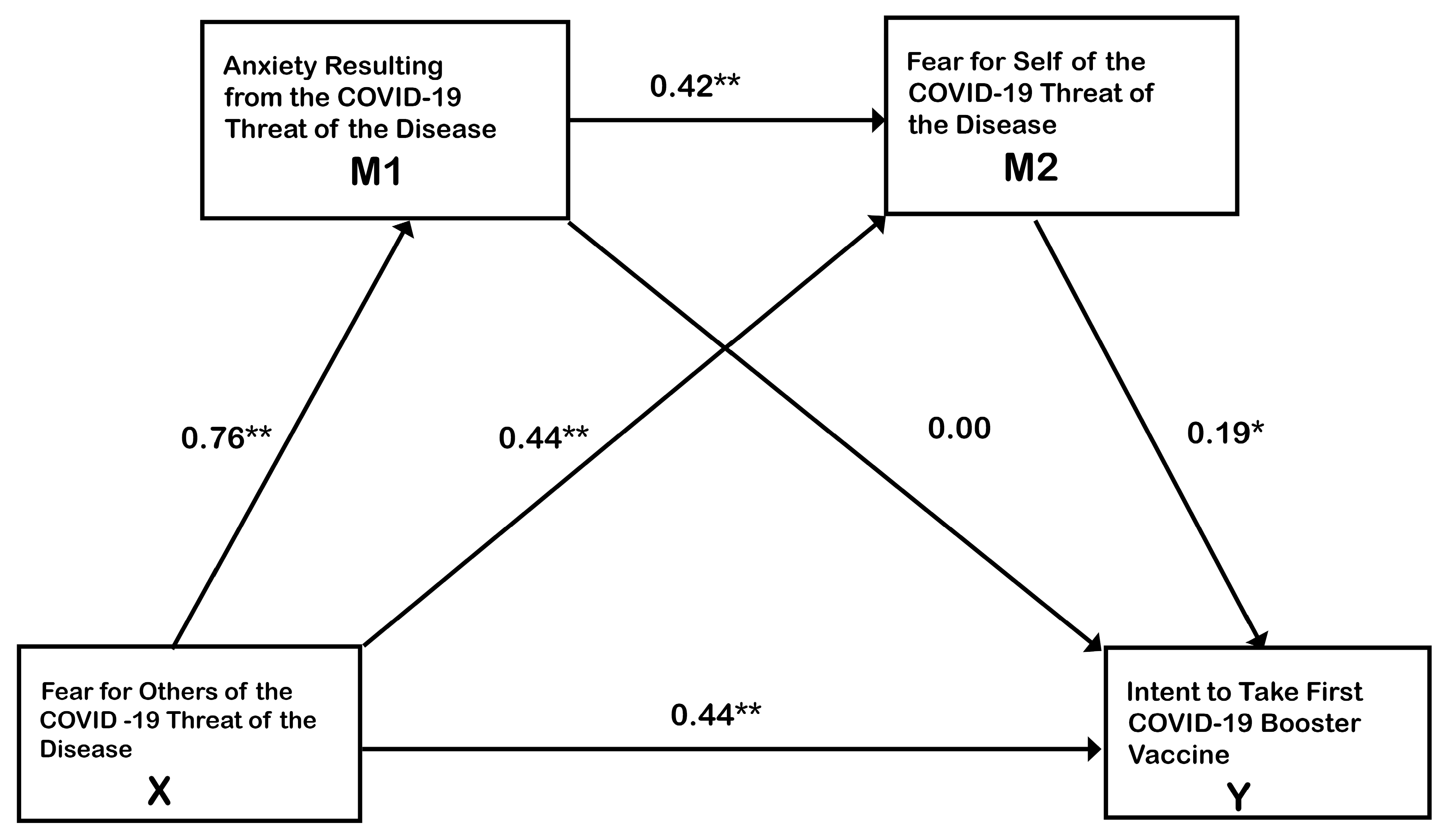
- RQ2: Which of FOTH, FSELF or CANX of COVID-19 are unique predictors of BINT?
- RQ3: Are significant indirect effects present among FOTH, FSELF or CANX as predictors of BINT?
2.2. Procedures
2.3. Participants
2.4. Measures
3. Results
3.1. Participants
3.2. Impact of Covariates and Overall Relationships of the Variables
3.3. Research Question One
4. Discussion
4.1. Limitations
4.1.1. Model Specifications
4.1.2. Sampling
4.2. Restricted Variable Ranges
4.3. Contributions of the Study
4.4. Shifting Conditions for the Latest COVID-19 Vaccines
4.5. Limitations
4.5.1. Lack of Connection to Message Design Strategy
4.5.2. Limited Sample and Narrow Range of Participants
4.5.3. Problem of Political Division
4.6. Future Research
4.6.1. Focus on Fear for Others and Fear for Self
4.6.2. Salient Features of Effective Advertisements
4.6.3. Clarification of the Role of Anxiety
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus disease 2019 |
| FOTH | Fear for others |
| FSELF | Fear for self |
| CANX | COVID-19 anxiety |
| BINT | Intent to take the first COVID-19 booster vaccine |
| CDC | Center for Disease Control |
| PPE | Personal Protective Equipment |
| AMT | Amazon Mechanical Turk |
References
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef] [PubMed]
- Scrima, F.; Miceli, S.; Caci, B.; Cardaci, M. The relationship between fear of COVID-19 and intention to get vaccinated. The serial mediation roles of existential anxiety and conspiracy beliefs. Pers. Individ. Differ. 2022, 184, 111188. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Coiado, O.C. COVID-19 vaccine and booster hesitation around the world: A literature review. Front. Med. 2023, 9, 1054557. [Google Scholar] [CrossRef] [PubMed]
- Seddig, D.; Maskileyson, D.; Davidov, E.; Ajzen, I.; Schmidt, P. Correlates of COVID-19 vaccination intentions: Attitudes, institutional trust, fear, conspiracy beliefs, and vaccine skepticism. Soc. Sci. Med. 2022, 302, 114981. [Google Scholar] [CrossRef] [PubMed]
- Crowe, S.; Howard, A.F.; Vanderspank-Wright, B.; Gillis, P.; McLeod, F.; Penner, C.; Haljan, G. The effect of COVID-19 pandemic on the mental health of Canadian critical care nurses providing patient care during the early phase pandemic: A mixed method study. Intensive Crit. Care Nurs. 2021, 63, 102999. [Google Scholar] [CrossRef] [PubMed]
- McAlearney, A.S.; Gaughan, A.A.; MacEwan, S.R.; Gregory, M.E.; Rush, L.J.; Volney, J.; Panchal, A.R. Pandemic Experience of First Responders: Fear, Frustration, and Stress. Int. J. Environ. Res. Public Health 2022, 19, 4693. [Google Scholar] [CrossRef] [PubMed]
- Gordon, J.M.; Magbee, T.; Yoder, L.H. The experiences of critical care nurses caring for patients with COVID-19 during the 2020 pandemic: A qualitative study. Appl. Nurs. Res. 2021, 59, 151418. [Google Scholar] [CrossRef]
- Kakkar, M.; Barmak, A.B.; Gajendra, S. Evaluation of fear, anxiety, and knowledge among dental providers during the COVID 19 pandemic. J. Dent. Sci. 2022, 17, 1648–1655. [Google Scholar] [CrossRef]
- Bigsby, E.; Albarracín, D. Self- and response efficacy information in fear appeals: A meta-analysis. J. Commun. 2022, 72, 241–263. [Google Scholar] [CrossRef]
- Tannenbaum, M.B.; Hepler, J.; Zimmerman, R.S.; Saul, L.; Jacobs, S.; Wilson, K.; Albarracín, D. Appealing to fear: A meta-analysis of fear appeal effectiveness and theories. Psychol. Bull. 2015, 141, 1178–1204. [Google Scholar] [CrossRef]
- Witte, K.; Allen, M. A Meta-analysis of fear appeals: Implications for effective public health campaigns. Health Educ. Behav. 2000, 27, 591–615. [Google Scholar] [CrossRef] [PubMed]
- Anthes, E. The Delta Variant: What Scientists Know; The New York Times: New York, NY, USA, 22 June 2021; Available online: https://www.nytimes.com/2021/06/22/health/delta-variant-covid.html (accessed on 14 November 2023).
- Yee, N.L. Three Charts Show How Far COVID Delta Variant Has Spread around the World. CNBC. Available online: https://www.cnbc.com/2021/08/06/covid-charts-show-how-far-delta-variant-has-spread-around-the-world.html (accessed on 20 December 2023).
- Dhawan, M.; Sharma, A.; Priyanka Thakur, N.; Rajkhowa, T.K.; Choudhary, O.P. Delta variant (B.1.617.2) of SARS-CoV-2: Mutations, impact, challenges and possible solutions. Hum. Vaccines Immunother. 2022, 18, 2068883. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Deng, A.; Li, K.; Hu, Y.; Li, Z.; Shi, Y.; Xiong, Q.; Liu, Z.; Guo, Q.; Zou, L.; et al. Viral infection and transmission in a large, well-traced outbreak caused by the SARS-CoV-2 Delta variant. Nat. Commun. 2022, 13, 460. [Google Scholar] [CrossRef] [PubMed]
- Roberto, A.J.; Zhou, X. Predicting college students’ COVID-19 vaccination behavior: An application of the extended parallel process model. J. Behav. Med. 2023, 46, 76–87. [Google Scholar] [CrossRef] [PubMed]
- Witte, K. Putting the fear back into fear appeals: The Extended Parallel Process Model. Commun. Monogr. 1992, 59, 329–349. [Google Scholar] [CrossRef]
- Roberto, A.J.; Mongeau, P.A.; Liu, Y.; Hashi, E.C. “Fear the Flu, Not the Flu Shot”: A test of the Extended Parallel Process Model. J. Health Com. 2019, 24, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Hochbaum, G.M. Public Participation in Medical Screening Programs: A Sociopsychological Study; United States Government Printing Office: Washington, DC, USA, 1958; Available online: https://books.google.com/books?hl=en&lr=&id=7O44ljhQkrsC&oi=fnd&pg=PA6&dq=Hochbaum,+G.&ots=bNmymlN2BW&sig=dDc_Jd3XCpk8zKamOIS7QoX_mV8#v=onepage&q=Hochb aum%2C%20G.&f=false (accessed on 29 December 2023).
- Warr, M. Altruistic fear of victimization in households. Soc. Sci. Q. 1992, 73, 723–736. [Google Scholar]
- Warr, M.; Ellison, C.G. Rethinking social reactions to crime: Personal and altruistic fear in family households. Am. J. Sociol. 2000, 106, 551–578. [Google Scholar] [CrossRef]
- Chen, M.; Chen, L. Promoting smoking cessation in China: Using an expansion of the EPPM with other-oriented threat. J. Health Commun. 2021, 26, 174–183. [Google Scholar] [CrossRef]
- Cori, L.; Curzio, O.; Adorni, F.; Prinelli, F.; Noale, M.; Trevisan, C.; Fortunato, L.; Giacomelli, A.; Bianchi, F. Fear of COVID-19 for Individuals and Family Members: Indications from the National Cross-Sectional Study of the EPICOVID19 Web-Based Survey. Int. J. Environ. Res. Public Health 2021, 18, 3248. [Google Scholar] [CrossRef]
- Ravindra, K.; Malik, V.S.; Padhi, B.K.; Goel, S.; Gupta, M. Asymptomatic infection and transmission of COVID-19 among clusters: Systematic review and meta-analysis. Public Health 2022, 203, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, F.; Sequeira, C.; Teixeira, L. Impact of COVID-19 outbreak on nurses’ mental health: A prospective cohort study. Environ. Res. 2021, 194, 110620. [Google Scholar] [CrossRef] [PubMed]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and initial validation. Int. J. Ment. Health Addict. 2022, 20, 1537–1545. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.J.; Perkins, A.M.; Corr, P.J. A confirmatory factor analytic study of anxiety, fear, and behavioral inhibition system measures. J. Individ. Differ. 2007, 728, 179–187. [Google Scholar] [CrossRef]
- Lang, P.J.; Davis, M.; Ohman, A. Fear and anxiety: Animal models and human cognitive psychophysiology. J. Affect. Disord. 2000, 61, 137–159. [Google Scholar] [CrossRef] [PubMed]
- So, J.; Kuang, K.; Cho, H. Re-examining fear appeal models from cognitive appraisal theory and functional emotion theory perspectives. Commun. Monogr. 2016, 83, 120–144. [Google Scholar] [CrossRef]
- Heeren, A. On the distinction between fear and anxiety in a (post)pandemic world: A commentary. Clin. Neuropsychiatry 2020, 17, 189–191. [Google Scholar] [CrossRef]
- Schimmenti, A.; Billieux, J.; Starcevic, V. The four horsemen of fear: An integrated model of understanding fear experiences during the COVID-19 pandemic. Clin. Neuropsychiatry 2020, 17, 41–45. [Google Scholar] [CrossRef]
- Öhman, A. Fear and anxiety: Overlaps and dissociations. In Handbook of Emotions, 3rd ed.; Lewis, M., Jones, J.M., Barrett, L.F., Eds.; Guilford Press: New York, NY, USA, 2008; pp. 709–729. [Google Scholar]
- Jeffs, E.; Lucas, N.; Walls, T. COVID-19: Parent and caregiver concerns about reopening New Zealand schools. J. Paediatr. Child Health 2021, 57, 403–408. [Google Scholar] [CrossRef]
- Barzilay, R.; Moore, T.M.; Greenberg, D.M.; DiDomenico, G.E.; Brown, L.A.; White, L.K.; Gur, R.C.; Gur, R.E. Resilience, COVID-19-related stress, anxiety and depression during the pandemic in a large population enriched for healthcare providers. Transl. Psychiatry 2020, 10, 291. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis, 3rd ed.; Guilford Press: New York, NY, USA, 2022. [Google Scholar]
- Crowston, K. Amazon Mechanical Turk: A research tool for organizations and information systems scholars. In Shaping the Future of ICT 2012 Research. Methods and Approaches; Bhattacherjee, A., Fitzgerald, B., Eds.; Springer: Chambersburg, PA, USA, 2012; pp. 210–221. [Google Scholar] [CrossRef]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social Learning Theory and the Health Belief Model. Health Educ. Q. 1988, 15, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 5th ed.; Guilford Press: New York, NY, USA, 2023. [Google Scholar]
- IBM Corporation. IBM SPSS for Windows, Version 28.; IBM Corporation: Armonk, NY, USA, 2021. [Google Scholar]
- Hayes, A.F.; Rockwood, N.J. Conditional Process Analysis: Concepts, computation, and advances in the modeling of the contingencies of mechanisms. Am. Behav. Sci. 2020, 64, 19–54. [Google Scholar] [CrossRef]
- Rattner, N.U.S. Heads into Second Christmas with COVID as Cases Rise and Americans Rush to Get Booster Shots. CNBC, 22 December 2021. Available online: https://www.cnbc.com/2021/12/22/us-covid-cases-booster-shots-on-the-rise-as-country-nears-christmas.html (accessed on 8 November 2023).
- Centers for Disease Control and Prevention. Leading Causes of Death [in the USA]. Available online: https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm (accessed on 2 November 2023).
- Centers for Disease Control and Prevention. COVID-19 Vaccinations in the United State. Available online: https://covid.cdc.gov/covid-data-tracker/#vaccinations_vacc-people-fully-percent-total (accessed on 2 November 2023).

{kind=link}
{kind=link}
| M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|---|---|
| 1. Fear for Others | 5.09 | 1.40 | 1 | 0.78 ** | 0.78 ** | 0.14 ** | −0.03 | −0.11 * | 0.63 ** |
| 2. Fear for Self | 4.72 | 1.52 | 0.78 ** | 1 | 0.77 ** | 0.17 ** | −0.12 | −0.15 ** | 0.57 ** |
| 3. COVID Anxiety | 4.81 | 1.42 | 0.78 ** | 0.77 ** | 1 | 0.13 ** | −0.01 | −0.11 * | 0.52 ** |
| 4. Political Affiliation (Democrat) | 0.61 | 0.49 | 0.14 ** | 0.17 ** | 0.13 ** | 1 | −0.60 ** | −0.57 ** | 0.24 ** |
| 5. Political Affiliation (Republican) | 0.19 | 0.39 | −0.03 * | −0.12 | −0.01 | −0.60 ** | 1 | −0.22 ** | −0.12 * |
| 6. Political Affiliation (Independent) | 0.17 | 0.38 | −0.11 * | −0.15 ** | −0.11 * | −0.57 ** | −0.22 ** | 1 | −0.14 ** |
| 7. Booster Indent | 5.27 | 1.48 | 0.63 ** | 0.57 ** | 0.52 ** | 0.24 ** | −0.12 * | −0.14 ** | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scudder, J.N.; DeBeck, D.P. A Survey of Fear for Others, Fear for Self, and Pandemic Anxiety Predicting Intention to Take the First Booster Vaccine to Combat COVID-19. Vaccines 2024, 12, 47. https://doi.org/10.3390/vaccines12010047
Scudder JN, DeBeck DP. A Survey of Fear for Others, Fear for Self, and Pandemic Anxiety Predicting Intention to Take the First Booster Vaccine to Combat COVID-19. Vaccines. 2024; 12(1):47. https://doi.org/10.3390/vaccines12010047
Chicago/Turabian StyleScudder, Joseph N., and Dennis P. DeBeck. 2024. "A Survey of Fear for Others, Fear for Self, and Pandemic Anxiety Predicting Intention to Take the First Booster Vaccine to Combat COVID-19" Vaccines 12, no. 1: 47. https://doi.org/10.3390/vaccines12010047
APA StyleScudder, J. N., & DeBeck, D. P. (2024). A Survey of Fear for Others, Fear for Self, and Pandemic Anxiety Predicting Intention to Take the First Booster Vaccine to Combat COVID-19. Vaccines, 12(1), 47. https://doi.org/10.3390/vaccines12010047