
“Zero Dose” Children in the Democratic Republic of the Congo: How Many and Who Are They?

 ,
,  , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
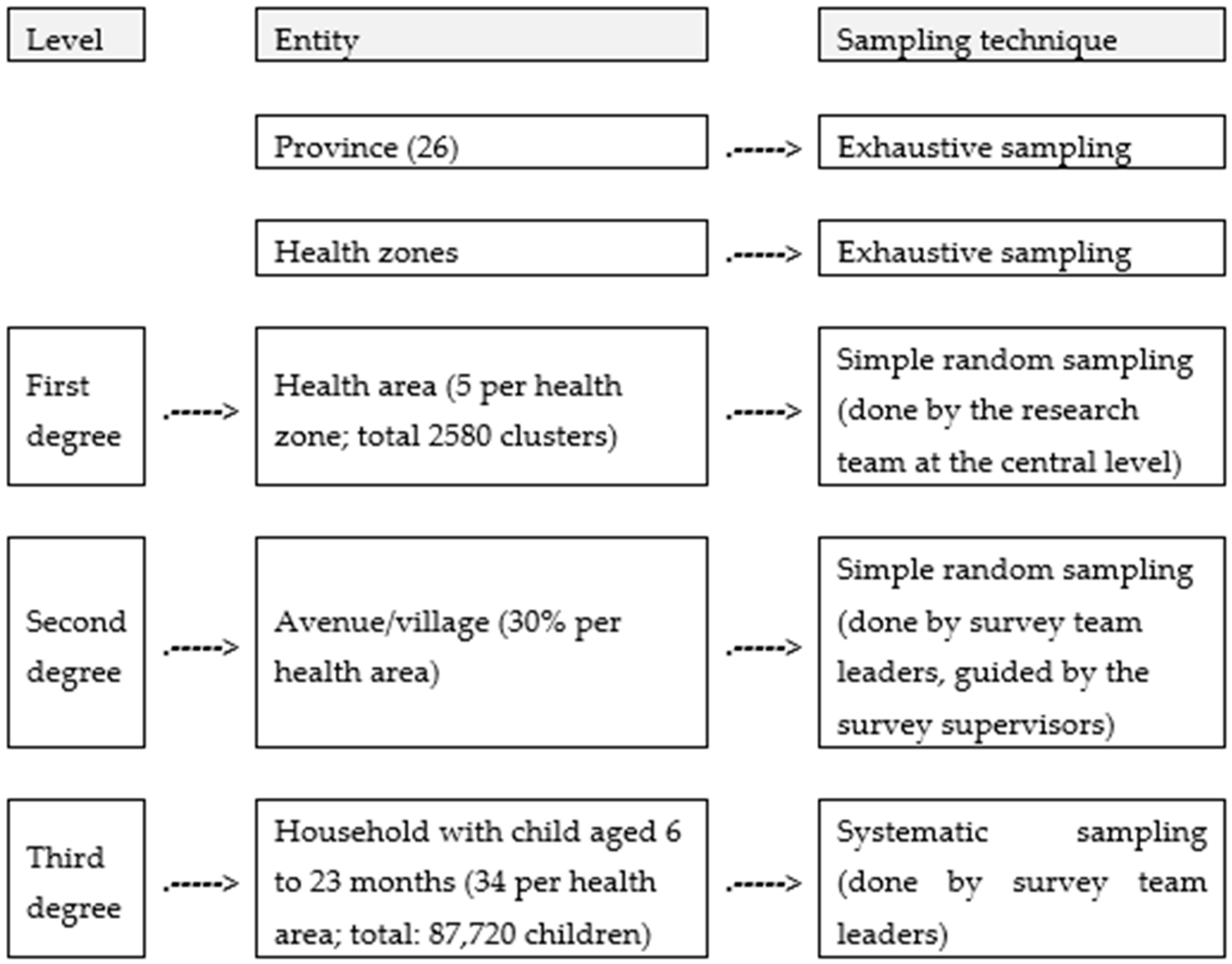
2.2. Sampling
2.3. Data Collection
2.4. Variables
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Description of the Sample
3.1.1. Characteristics of Mothers/Caregivers of 12–23 Month Old Children and Gender of the Child
3.1.2. Household Socio-Economic, Communicational, and System-Related Characteristics
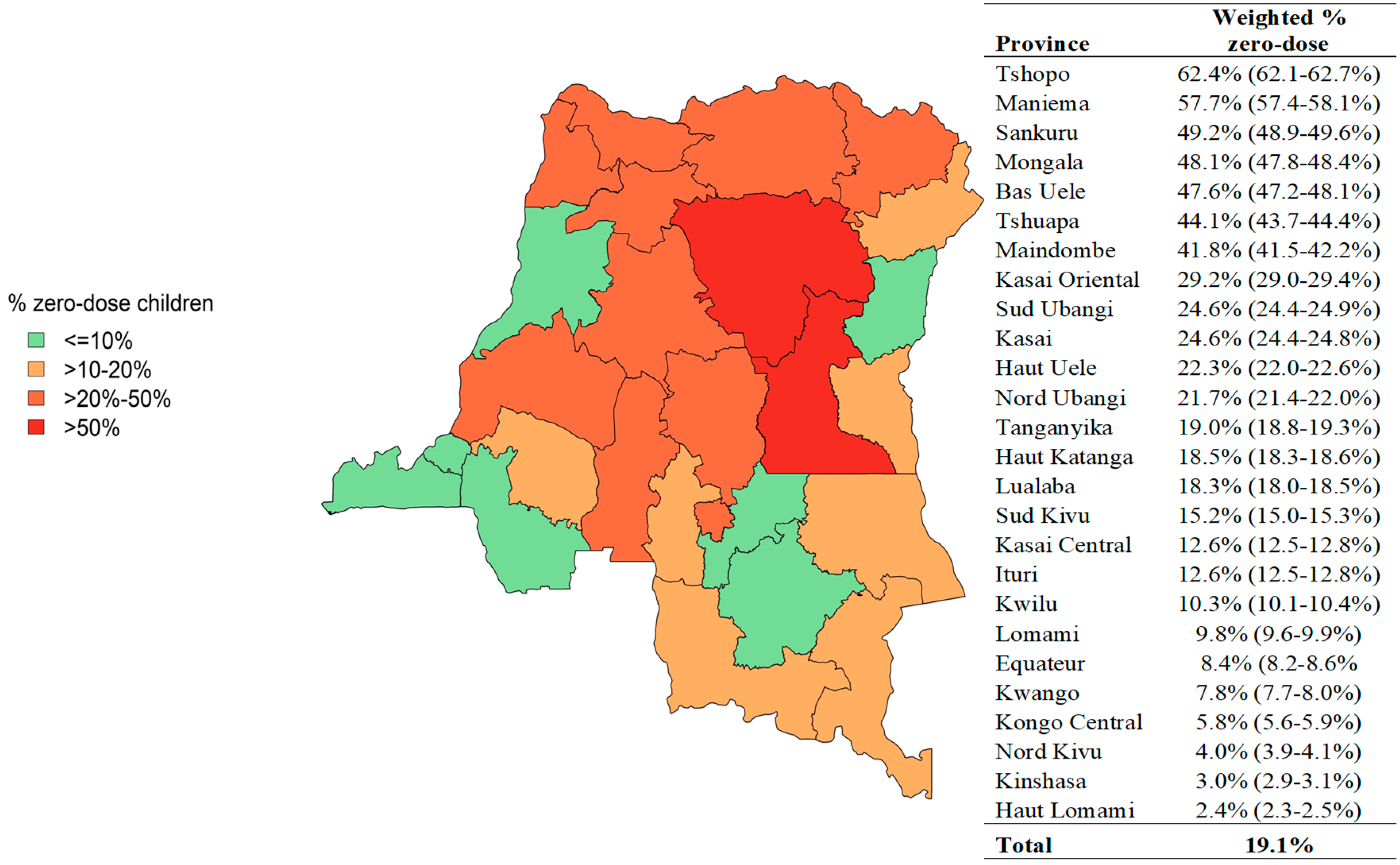
3.2. Proportion of ZD Children 12–23 Months in DRC
3.3. Factors Associated with Zero-Dose Vaccine in Children Aged 12 to 23 Months in the DRC
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Greenwood, B. The contribution of vaccination to global health: Past, present and future. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2014, 369, 20130433. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Immunization Coverage 2021 [Internet]; WHO: Geneva, Switzerland, 2021; (WHO Estimates of National Immunization Coverage (Data as of July 2022)); Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 10 November 2022).
- Wigley, A.; Lorin, J.; Hogan, D.; Utazi, C.E.; Hagedorn, B.; Dansereau, E.; Tatem, A.J.; Tejedor-Garavito, N. Estimates of the number and distribution of zero-dose and under-immunised children across remote-rural, urban, and conflict-affected settings in low and middle-income countries. PLoS Glob. Public Health 2022, 2, e0001126. [Google Scholar] [CrossRef] [PubMed]
- Gavi, the Vaccine Alliance. The Zero-Dose Child: Explained. Vaccines Work, 26 April 2021. Available online: https://www.gavi.org/vaccineswork/zero-dose-child-explained (accessed on 12 November 2022).
- Ministère de la Santé Publique de RDC. Plan D’urgence Pour la Relance de la Vaccination de Routine Dit «Plan Marshall sur la Vaccination de Routine» (Plan MASHAKO). Programme Elargi de Vaccination; Ministère de la Santé Publique de RDC: Kinshasa, Democratic Republic of the Congo, July 2018. [Google Scholar]
- WHO/UNICEF. Estimates of National Immunization Coverage 2021 [Internet]; WHO/UNICEF: Geneva, Switzerland; Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/immunization-coverage/who-unicef-estimates-of-national-immunization-coverage (accessed on 12 November 2022).
- Dobiliti, Inc., USA. Available online: https://www.surveycto.com/ (accessed on 12 November 2022).
- Abebe, A.M.; Mengistu, T.; Mekuria, A.D. Measles case, immunization coverage and its determinant factors among 12–23 month children, in Bassona Worena Woreda, Amhara Region, Ethiopia, 2018. BMC Res. Notes 2019, 12, 71. [Google Scholar] [CrossRef]
- Negussie, A.; Kassahun, W.; Assegid, S.; Hagan, A.K. Factors associated with incomplete childhood immunization in Arbegona district, southern Ethiopia: A case—Control study. BMC Public Health 2015, 16, 27. [Google Scholar] [CrossRef] [PubMed]
- Mohamud, A.N.; Feleke, A.; Worku, W.; Kifle, M.; Sharma, H.R. Immunization coverage of 12–23 months old children and associated factors in Jigjiga District, Somali National Regional State, Ethiopia. BMC Public Health 2014, 14, 865. [Google Scholar] [CrossRef] [PubMed]
- Zewdie, A.; Letebo, M.; Mekonnen, T. Reasons for defaulting from childhood immunization program: A qualitative study from Hadiya zone, Southern Ethiopia. BMC Public Health 2016, 16, 1240. [Google Scholar] [CrossRef]
- Mekonnen, Z.A.; Gelaye, K.A.; Were, M.C.; Tilahun, B. Timely completion of vaccination and its determinants among children in northwest, Ethiopia: A multilevel analysis. BMC Public Health 2020, 20, 908. [Google Scholar] [CrossRef]
- Girmay, A.; Dadi, A.F. Full Immunization Coverage and Associated Factors among Children Aged 12–23 Months in a Hard-to-Reach Areas of Ethiopia. Int. J. Pediatr. 2019, 2019, 1924941. [Google Scholar] [CrossRef]
- Kinfe, Y.; Gebre, H.; Bekele, A. Factors associated with full immunization of children 12–23 months of age in Ethiopia: A multilevel analysis using 2016 Ethiopia Demographic and Health Survey. PLoS ONE 2019, 14, e0225639. [Google Scholar] [CrossRef]
- Tamirat, K.S.; Sisay, M.M. Full immunization coverage and its associated factors among children aged 12–23 months in Ethiopia: Further analysis from the 2016 Ethiopia demographic and health survey. BMC Public Health 2019, 19, 1019. [Google Scholar] [CrossRef]
- Kagoné, M.; Yé, M.; Nébié, E.; Sie, A.; Schoeps, A.; Becher, H.; Muller, O.; Fisker, A.B. Vaccination coverage and factors associated with adherence to the vaccination schedule in young children of a rural area in Burkina Faso. Glob. Health Action 2017, 10, 1399749. [Google Scholar] [CrossRef]
- Kiptoo, E.; Esilaba, M.; Kobia, G.; Ngure, R. Factors Influencing Low Immunization Coverage Among Children Between 12–23 Months in East Pokot, Baringo Country, Kenya. Int. J. Vaccines Vaccin. 2015, 1, 00012. [Google Scholar] [CrossRef]
- Gidado, S.; Nguku, P.; Biya, O.; Waziri, N.E.; Mohammed, A.; Nsubuga, P.; Akpan, H.; Oyemakinde, A.; Nasidi, A.; Suleman, I.; et al. Determinants of routine immunization coverage in Bungudu, Zamfara State, Northern Nigeria, May 2010. Pan Afr. Med. J. 2014, 18, 9. [Google Scholar] [CrossRef]
- Adedokun, S.T.; Uthman, O.A.; Adekanmbi, V.T.; Wiysonge, C.S. Incomplete childhood immunization in Nigeria: A multilevel analysis of individual and contextual factors. BMC Public Health 2017, 17, 236. [Google Scholar] [CrossRef]
- Duru, C.B.; Iwu, A.C.; Uwakwe, K.A.; Diwe, K.C.; Merenu, I.A.; Emerole, C.A.; Adaeze, C.A.; Onyekuru, C.U.; Ihunnia, O. Assessment of Immunization Status, Coverage and Determinants among under 5-Year-Old Children in Owerri, Imo State, Nigeria. Open Access Libr. J. 2016, 3, e2753. [Google Scholar] [CrossRef]
- Legesse, E.; Dechasa, W. An assessment of child immunization coverage and its determinants in Sinana District, Southeast Ethiopia. BMC Pediatr. 2015, 15, 31. [Google Scholar] [CrossRef]
- Tadesse, H.; Deribew, A.; Woldie, M. Predictors of defaulting from completion of child immunization in south Ethiopia, May 2008—A case control study. BMC Public Health 2009, 9, 150. [Google Scholar] [CrossRef]
- Johri, M.; Rajpal, S.; Subramanian, S.V. Progress in reaching unvaccinated (zero-dose) children in India, 1992–2016: A multilevel, geospatial analysis of repeated cross-sectional surveys. Lancet Glob. Health 2021, 9, e1697–e1706. [Google Scholar] [CrossRef]
- Toirambe, S.E.; Camara, T.; Khalis, M.; Serhier, Z.; Darkaoui, N.; Hassouni, K.; Belouali, R.; Jallal, M. Facteurs prédictifs de la non-complétude vaccinale chez des enfants migrants de moins de 5 ans, Maroc. St. Publique 2021, 33, 435–443. [Google Scholar] [CrossRef]
- Ozigbu, C.E.; Olatosi, B.; Li, Z.; Hardin, J.W.; Hair, N.L. Correlates of Zero-Dose Vaccination Status among Children Aged 12–59 Months in Sub-Saharan Africa: A Multilevel Analysis of Individual and Contextual Factors. Vaccines 2022, 10, 1052. [Google Scholar] [CrossRef]
- Santos, T.M.; Cata-Preta, B.O.; Wendt, A.; Arroyave, L.; Hogan, D.R.; Mengistu, T.; Barros, A.J.D.; Victora, C.G. Religious Affiliation as a Driver of Immunization Coverage: Analyses of Zero-Dose Vaccine Prevalence in 66 Low- and Middle-Income Countries. Front. Public Health 2022, 10, 977512. [Google Scholar] [CrossRef] [PubMed]
- Balle, F. Les Médias. In Que Sais-Je? PUF: Paris, France, 2006. [Google Scholar]
- Corrêa, G.; Verstraete, P.; Soundardjee, R.; Shankar, M.; Paterson, C.; Hampton, L.; Jackson, D.; Muniz, M.; Mwamba, R.; Wenz, K.; et al. Immunization programmes and notifications of vital events. Bull. World Health Organ. 2019, 97, 306–308. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization (PAHO). Immunization and Birth Registration. Immun. Newsl. 2012, 34, 1–2. Available online: www.paho.org/immunization/newsletter (accessed on 20 November 2022).
- Jiang, X.; Shang, X.; Lin, J.; Zhao, Y.; Wang, W.; Qiu, Y. Impacts of free vaccination policy and associated factors on influenza vaccination behavior of the elderly in China: A quasi-experimental study. Vaccine 2021, 39, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Fang, R.; Ma, Y.; Wu, J.; Lv, M.; Tian, L.; Xie, Z. Free influenza vaccination coverage and its influencing factors about cognition among elderly population in Beijing. Chin. Gen. Pract. 2013, 17, 1403–1406. [Google Scholar] [CrossRef]
- Crocker-Buque, T.; Mindra, G.; Duncan, R.; Mounier-Jack, S. Immunization, urbanization and slums—A systematic review of factors and interventions. BMC Public Health 2017, 17, 556. [Google Scholar] [CrossRef]
- Machado, A.A.; Edwards, S.A.; Mueller, M.; Saini, V. Effective interventions to increase routine childhood immunization coverage in low socioeconomic status communities in developed countries: A systematic review and critical appraisal of peer-reviewed literature. Vaccine 2021, 39, 2938–2964. [Google Scholar] [CrossRef]
- JSI Inc. Attendre les Enfants non Vaccinés: Leçons Tirées de L’assistance Technique de JSI au Gouvernement de RDC Pour L’amélioration de L’accès aux Services de Vaccination de Routine et Pour une Meilleure Utilisation de ces Services. 2020. Available online: https://publications.jsi.com/JSIInternet/Inc/Common/_download_pub.cfm?id=23343&lid=6 (accessed on 20 November 2022).
- Kaboré, L.; Méda, C.Z.; Sawadogo, F.; Bengue, M.M.; Kaboré, W.M.; Essoh, A.T.; Gervaix, A.; Galetto-Lacour, A.; Médah, I.; Betsem, E. Quality and reliability of vaccination documentation in the routine childhood immunization program in Burkina Faso: Results from a cross-sectional survey. Vaccine 2020, 38, 2808–2815. [Google Scholar] [CrossRef]
- Mansour, Z.; Brandt, L.; Said, R.; Fahmy, K.; Riedner, G.; Danovaro-Holliday, M.C. Home-based records’ quality and validity of caregivers’ recall of children’s vaccination in Lebanon. Vaccine 2019, 37, 4177–4183. [Google Scholar] [CrossRef]
- Dansereau, E.; Brown, D.; Stashko, L.; Danovaro-Holliday, M.C. A systematic review of the agreement of recall, home-based records, facility records, BCG scar, and serology for ascertaining vaccination status in low and middle-income countries. Gates Open Res. 2020, 3, 923. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Socio-Demographic Characteristics of the Mother/Guardian of the Child and Gender | Household Socio-Economic, Communicational, and System-Related Characteristics | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | n | Weighted % | Variable | n | Weighted % | Variable | n | Weighted % |
| Relationship between respondent and child | Occupation | Household wealth quintile | ||||||
| Child’s mother | 48,838 | 95.8 | No occupation | 15,034 | 32.2 | Lowest | 21,955 | 40.7 |
| Other caregiver | 2216 | 4.2 | Teacher | 1687 | 3.4 | Second | 24,500 | 49.0 |
| Total | 51,054 | 100.0 | Official | 673 | 1.5 | Middle | 3949 | 8.9 |
| Age | Farmer/Breeder | 24,722 | 42.4 | Fourth | 630 | 1.3 | ||
| Median: 27 years | Fisherman | 277 | 0.5 | Highest | 20 | 0.1 | ||
| IQR: 22–33 years | Trader | 4806 | 11.6 | Total | 51,054 | 100.0 | ||
| Range: 13–81 years | Worker | 564 | 1.3 | Household location environment | ||||
| ≤19 years | 3643 | 7.0 | Others | 2081 | 4.7 | Rural | 41,041 | 73.2 |
| 20 to 29 years | 26,718 | 52.6 | Pupil/Student | 1210 | 2.5 | Urban | 10,013 | 26.8 |
| 30 to 39 years | 17,351 | 34.2 | Total | 51,054 | 100.0 | Total | 51,054 | 100.0 |
| 40 to 49 years | 2903 | 5.4 | Number of other children | Registration of birth with the civil authority | ||||
| ≥50 years | 429 | 0.8 | 0 | 17 | 0.1 | Yes | 12,863 | 29.4 |
| Total | 51,054 | 100.0 | 1 | 49,589 | 97.2 | No | 37,598 | 69.4 |
| Current marital status | 2 | 1347 | 2.5 | Do not know | 593 | 1.2 | ||
| Married | 25,066 | 52.5 | 3 | 101 | 0.2 | Total | 51,054 | 100.0 |
| Free union | 21,199 | 38.1 | Total | 51,054 | 100.0 | Having to pay for the vaccination card | ||
| Separated | 1082 | 1.9 | Religion | Yes | 16,174 | 39.8 | ||
| Single | 3004 | 6.1 | No religion | 826 | 1.5 | No | 27,697 | 59.7 |
| Divorced | 225 | 0.4 | Catholic | 14,964 | 28.9 | Do not know | 250 | 0.5 |
| Widow | 478 | 0.9 | Protestant | 13,711 | 25 | Total | 44,121 | 100.0 |
| Total | 51,054 | 100.0 | Kimbanguist | 1460 | 2.7 | Having to pay for another immunization-related service | ||
| Educational level | Muslim | 773 | 1.7 | Yes | 7712 | 21.2 | ||
| No level | 7156 | 12.7 | Revival Church | 17,063 | 35.5 | No | 36,066 | 78.1 |
| Primary | 20,851 | 38 | Other religion | 2158 | 4.5 | Do not know | 343 | 0.7 |
| Secondary | 21,493 | 45.5 | Do not know | 23 | 0.1 | Total | 44,121 | 100.0 |
| Superior | 1342 | 3.3 | Failure to disclose RA | 76 | 0.1 | Telephone use | ||
| Do not know | 40 | 0.1 | Total | 51,054 | 100.0 | Yes | 29,845 | 64.8 |
| No response | 172 | 0.4 | Gender of the child | No | 21,209 | 35.2 | ||
| Total | 51,054 | 100.0 | Male | 27,493 | 54 | Total | 51,054 | 100.0 |
| At least one vaccine-preventable | Female | 23,561 | 46 | Radio | ||||
| disease cited by the respondent | ||||||||
| Yes | 47,674 | 93.9 | Total | 51,054 | 100.0 | Yes | 25,883 | 54.2 |
| No | 3380 | 6.1 | No | 25,171 | 45.8 | |||
| Total | 51,054 | 100.0 | Total | 51,054 | 100.0 | |||
| Variables | Bivariate | Multivariate | |||
|---|---|---|---|---|---|
| Weighted % Zero-Doses | OR (95% CI) | p-Value | AOR (95% CI) | p-Value | |
| Age groups | |||||
| 20 to 29 years | 18.9 | 1.00 | 1.00 | ||
| 30 to 39 years | 17.9 | 0.94 (0.89 to 0.99) | 0.034 | 1.01 (0.93 to 1.11) | 0.760 |
| 40 to 49 years | 21.6 | 1.19 (1.07 to 1.32) | 0.002 | 0.97 (0.81 to 1.15) | 0.680 |
| ≥50 years | 29.3 | 1.79 (1.38 to 2.31) | <0.001 | 1.14 (0.74 to 1.75) | 0.561 |
| ≤19 years | 24.0 | 1.36 (1.24 to 1.49) | <0.001 | 1.23 (1.06 to 1.44) | 0.007 |
| Relationship between respondent and child | |||||
| Child’s mother | 18.8 | 1.00 | |||
| Other caregiver | 27.8 | 1.67 (1.49 to 1.87) | <0.001 | ||
| Current marital status | |||||
| Married | 18.1 | 1.00 | |||
| Free union | 19.4 | 1.09 (1.03 to 1.15) | 0.002 | ||
| separated | 28.2 | 1.77 (1.51 to 2.08) | <0.001 | ||
| Single | 20.8 | 1.19 (1.07 to 1.32) | 0.002 | ||
| Divorced | 34.4 | 2.37 (1.70 to 3.32) | <0.001 | ||
| Widow | 28.8 | 1.83 (1.46 to 2.29) | <0.001 | ||
| Educational level | |||||
| Superior | 4.6 | 1.00 | 1.00 | ||
| No level | 22.8 | 6.18 (4.64 to 8.23) | <0.001 | 3.46 (1.99 to 5.99) | <0.001 |
| Primary | 14.6 | 3.59 (2.69 to 4.79) | <0.001 | 3.14 (1.81 to 5.42) | <0.001 |
| Secondary | 28.0 | 8.14 (6.09 to 10.89) | <0.001 | 3.87 (2.22 to 6.75) | <0.001 |
| Occupation | |||||
| No occupation | 17.5 | 1.00 | |||
| Teacher | 13.0 | 0.71 (0.60 to 0.83) | <0.001 | ||
| Official | 9.7 | 0.51 (0.38 to 0.67) | <0.001 | ||
| Farmer/Breeder | 22.7 | 1.38 (1.30 to 1.47) | <0.001 | ||
| Fisherman | 32.4 | 2.25 (1.66 to 3.05) | <0.001 | ||
| Trader | 13.7 | 0.75 (0.67 to 0.83) | <0.001 | ||
| Worker | 17.0 | 0.96 (0.75 to 1.24) | 0.777 | ||
| Others | 19.1 | 1.11 (0.98 to 1.27) | 0.103 | ||
| Pupil/Student | 18.4 | 1.06 (0.89 to 1.27) | 0.507 | ||
| Religion | |||||
| Catholic | 15.1 | 1.00 | 1.00 | ||
| No religion | 30.2 | 2.44 (2.02 to 2.95) | <0.001 | 1.12 (080 to 1.56) | 0.510 |
| Protestant | 19.7 | 1.39 (1.29 to 1.49) | <0.001 | 1.12 (1.01 to 1.25) | 0.031 |
| Kimbanguist | 20.7 | 1.47 (1.27 to 1.71) | <0.001 | 1.31 (1.03 to 1.66) | 0.026 |
| Muslim | 30.4 | 2.46 (2.05 to 2.96) | <0.001 | 1.71 (1.25 to 2.33) | 0.001 |
| Revival/Ind. Church | 20.5 | 1.45 (1.36 to 1.55) | <0.001 | 1.35 (1.22 to 1.50) | <0.001 |
| Other religion | 21.9 | 1.58 (1.39 to 1.80) | <0.001 | 1.13 (0.91 to 1.39) | 0.267 |
| Do not know | 14.8 | 0.98 (0.36 to 2.70) | 0.972 | 0.85 (0.23 to 3.12) | 0.804 |
| Failure to disclose RA | 52.0 | 6.12 (3.45 to 10.85) | <0.001 | 4.22 (1.63 to 10.94) | <0.001 |
| Household wealth quintile | |||||
| Lowest | 26.3 | 9.44 (1.23 to 72.29) | 0.031 | ||
| Second | 15.6 | 4.88 (0.64 to 37.50) | 0.127 | ||
| Middle | 8.1 | 2.34 (0.30 to 18.02) | 0.415 | ||
| Fourth | 6.6 | 1.86 (0.25 to 14.76) | 0.557 | ||
| Highest | 3.7 | 1.00 | |||
| Household location environment | |||||
| Urban | 12.7 | 1.00 | |||
| Rural | 21.5 | 1.89 (1.76 to 2.04) | <0.001 | ||
| Child’s gender | |||||
| Male | 19.4 | 1.00 | |||
| Female | 18.9 | 0.97 (0.92 to 1.02) | 0.241 | ||
| Registration of birth with the civil authority | |||||
| Yes | 6.2 | 1.00 | 1.00 | ||
| No | 24.5 | 4.91 (4.50 to 5.35) | <0.001 | 2.04 (1.81 to 2.29) | <0.001 |
| Do not know | 28.9 | 6.17 (4.83 to 7.86) | <0.001 | 2.36 (1.65 to 3.36) | <0.001 |
| Having to pay for the vaccination card | |||||
| Yes | 3.8 | 1.00 | 1.00 | ||
| No | 11.0 | 3.10 (2.81 to 3.42) | <0.001 | 2.02 (1.81 to 2.24) | <0.001 |
| Do not know | 38.0 | 15.44 (11.29 to 21.12) | <0.001 | 5.14 (3.46 to 7.65) | <0.001 |
| Having to pay for another immunization-related service | |||||
| Yes | 1.8 | 1.00 | 1.00 | ||
| No | 9.8 | 5.81 (4.76 to 7.10) | <0.001 | 3.22 (2.57 to 4.03) | <0.001 |
| Do not know | 28.9 | 21.75 (15.58 to 30.37) | <0.001 | 5.80 (3.82 to 8.82) | <0.001 |
| Telephone use | |||||
| Yes | 13.8 | 1.00 | 1.00 | ||
| No | 28.9 | 2.54 (2.41 to 2.67) | <0.001 | 1.59 (1.45 to 1.75) | <0.001 |
| Radio | |||||
| Yes | 13.2 | 1.00 | 1.00 | ||
| No | 26.2 | 2.33 (2.21 to 2.45) | <0.001 | 1.48 (1.34 to 1.63) | <0.001 |
| At least one vaccine-preventable disease cited by the respondent | |||||
| Yes | 16.7 | 1.0 | 1.00 | ||
| No | 56.4 | 6.44 (5.90 to 7.03) | <0.001 | 3.37 (2.94 to 3.87) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© World Health Organization 2023. Licensee MDPI. This article is distributed under the terms of the Creative Commons Attribution IGO License. (https://creativecommons.org/licenses/by/3.0/igo/) which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any reproduction of this article there should not be any suggestion that WHO or this article endorse any specific organization or products. The use of the WHO logo is not permitted.
Share and Cite
Ishoso, D.K.; Danovaro-Holliday, M.C.; Cikomola, A.M.-W.; Lungayo, C.L.; Mukendi, J.-C.; Mwamba, D.; Ngandu, C.; Mafuta, E.; Lusamba Dikassa, P.S.; Lulebo, A.; et al. “Zero Dose” Children in the Democratic Republic of the Congo: How Many and Who Are They? Vaccines 2023, 11, 900. https://doi.org/10.3390/vaccines11050900
Ishoso DK, Danovaro-Holliday MC, Cikomola AM-W, Lungayo CL, Mukendi J-C, Mwamba D, Ngandu C, Mafuta E, Lusamba Dikassa PS, Lulebo A, et al. “Zero Dose” Children in the Democratic Republic of the Congo: How Many and Who Are They? Vaccines. 2023; 11(5):900. https://doi.org/10.3390/vaccines11050900
Chicago/Turabian StyleIshoso, Daniel Katuashi, M. Carolina Danovaro-Holliday, Aimé Mwana-Wabene Cikomola, Christophe Luhata Lungayo, Jean-Crispin Mukendi, Dieudonné Mwamba, Christian Ngandu, Eric Mafuta, Paul Samson Lusamba Dikassa, Aimée Lulebo, and et al. 2023. "“Zero Dose” Children in the Democratic Republic of the Congo: How Many and Who Are They?" Vaccines 11, no. 5: 900. https://doi.org/10.3390/vaccines11050900
APA StyleIshoso, D. K., Danovaro-Holliday, M. C., Cikomola, A. M.-W., Lungayo, C. L., Mukendi, J.-C., Mwamba, D., Ngandu, C., Mafuta, E., Lusamba Dikassa, P. S., Lulebo, A., Manirakiza, D., Mboussou, F.-F., Yapi, M. D., Ngabo, G. F., Riziki, R. B., Mwanga, C., Otomba, J., & Nimpa, M. M. (2023). “Zero Dose” Children in the Democratic Republic of the Congo: How Many and Who Are They? Vaccines, 11(5), 900. https://doi.org/10.3390/vaccines11050900