
Arising Concerns of Atypical Manifestations in Patients with Hand, Foot, and Mouth Disease

 ,
,  ,
, 

Abstract
1. Introduction
2. Literature Search Strategy
3. Inclusion and Exclusion Criteria
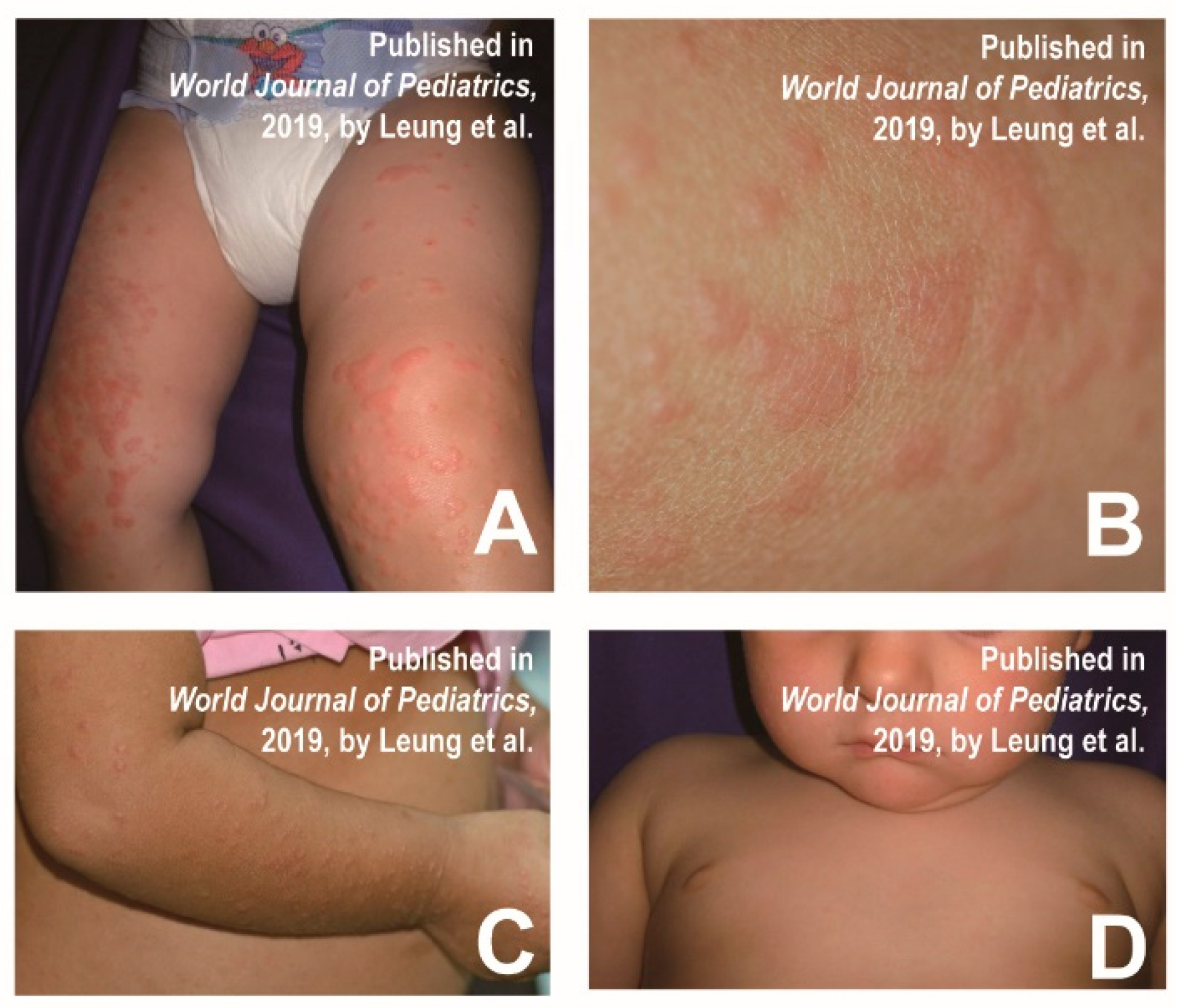
4. Gianotti Crosti-like eruptions
5. Eczema Coxsackium
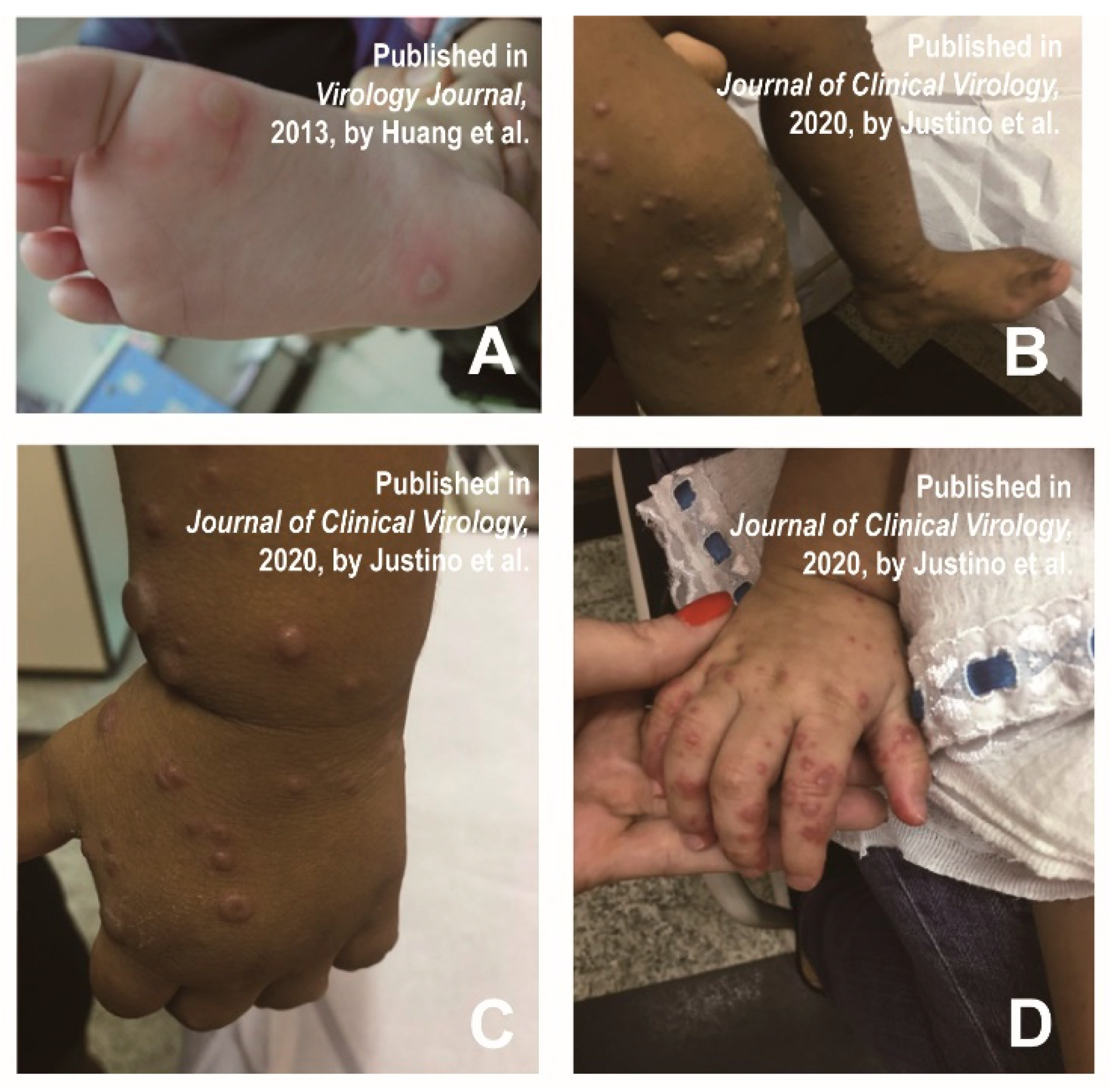
6. Petechial/Purpuric Eruptions
7. Vesiculobullous Exanthema
8. Tomato Flu
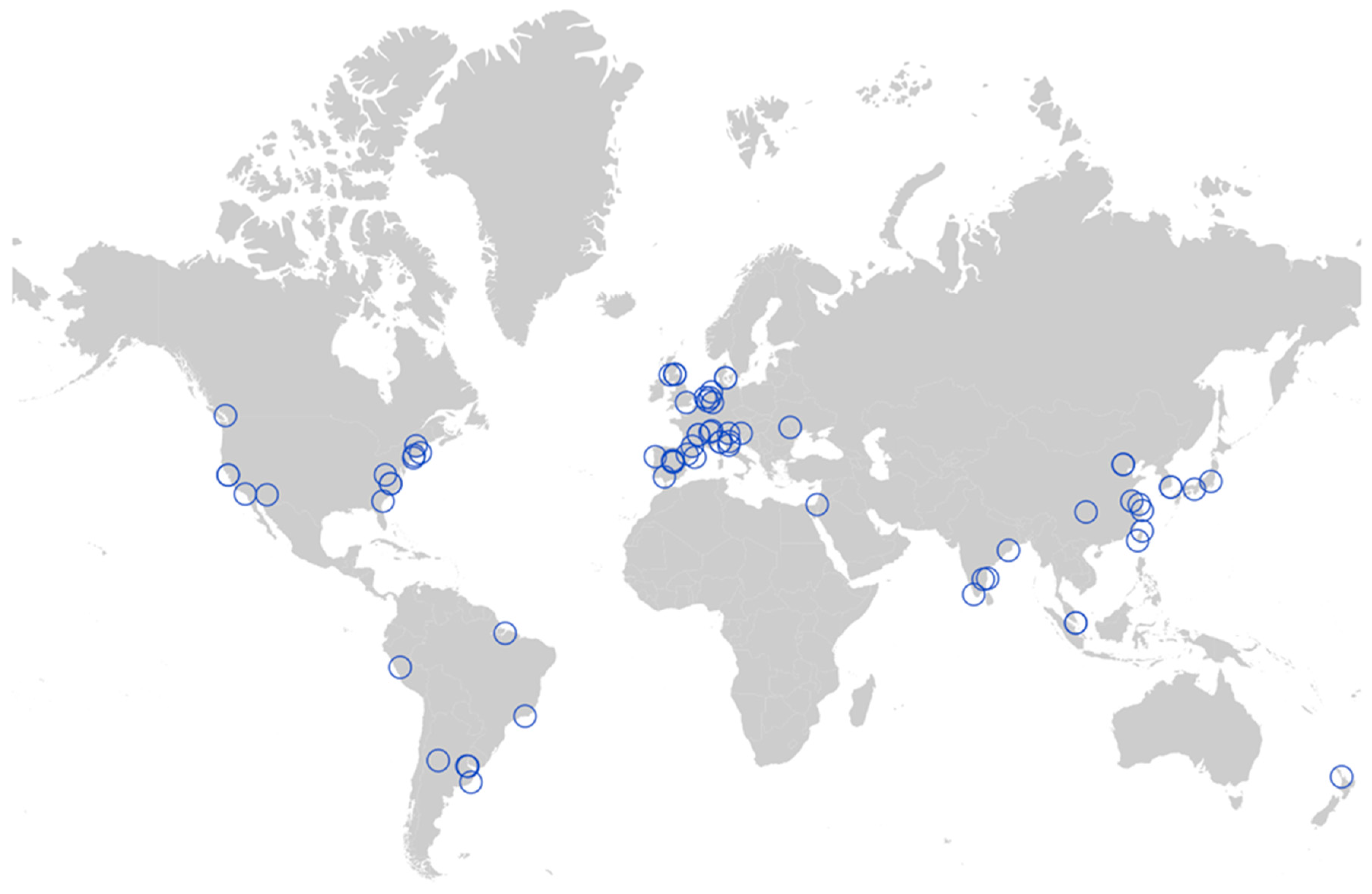
9. Geographical Distribution of Atypical HFMD
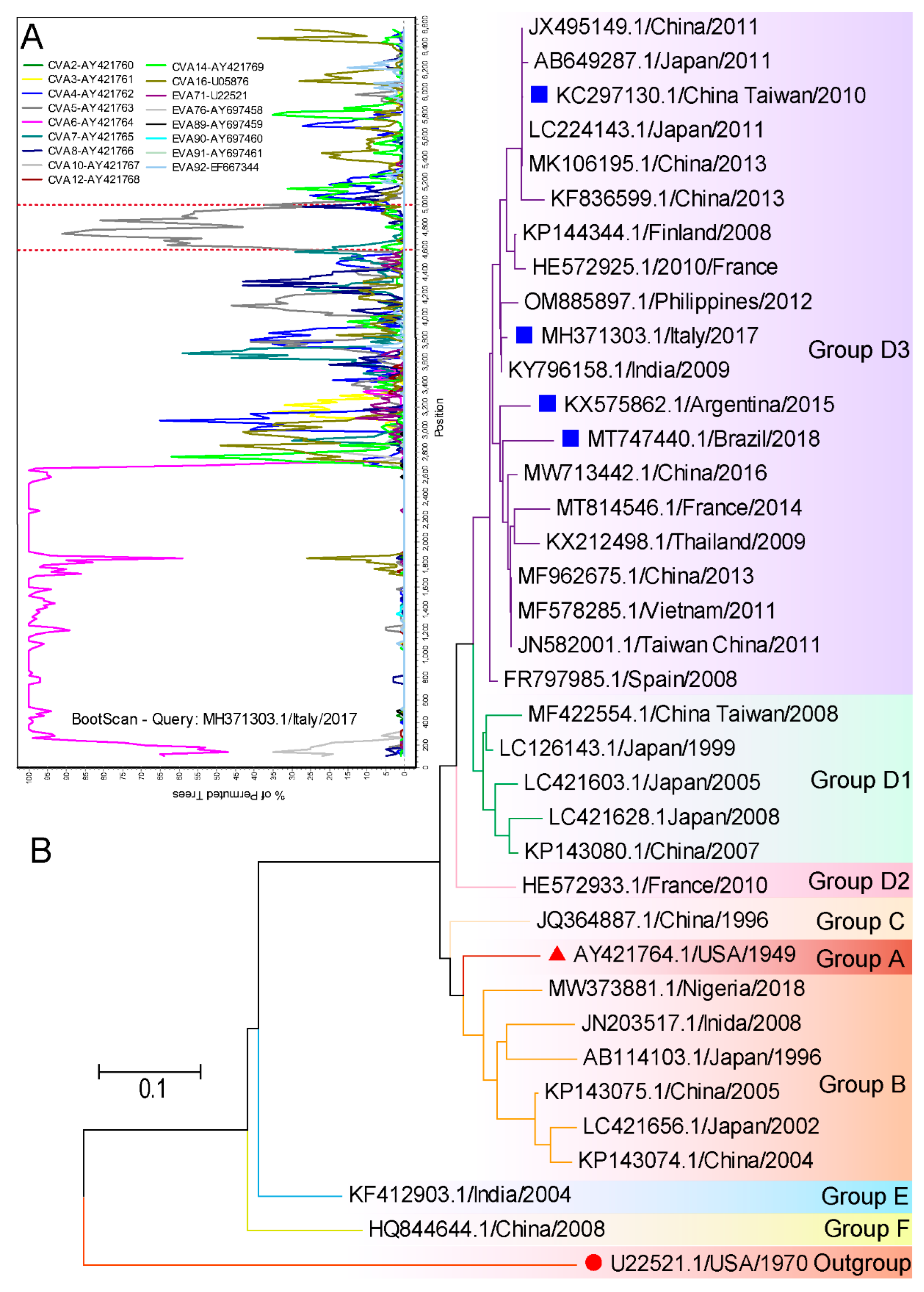
10. Evolutionary Characteristics of Virus Strains Causing Atypical HFMD
11. Summary and Prospective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Solomon, T.; Lewthwaite, P.; Perera, D.; Cardosa, M.J.; McMinn, P.; Ooi, M.H. Virology, epidemiology, pathogenesis, and control of enterovirus 71. Lancet Infect. Dis. 2010, 10, 778–790. [Google Scholar] [CrossRef]
- Ooi, M.H.; Wong, S.C.; Lewthwaite, P.; Cardosa, M.J.; Solomon, T. Clinical features, diagnosis, and management of enterovirus 71. Lancet Neurol. 2010, 9, 1097–1105. [Google Scholar] [CrossRef] [PubMed]
- Merzel Sabovic, E.K.; Tockova, O.; Ursic, T.; Zgavec, B.; Dolenc-Voljc, M. Atypical hand, foot, and mouth disease in an adult patient: A case report and literature review. Acta Derm. Alp. Pannonica Adriat. 2019, 28, 85–88. [Google Scholar] [CrossRef]
- Bruning, A.H.; van der Sanden, S.M.; ten Hoedt, A.E.; Wolthers, K.C.; van Kaam, A.H.; Pajkrt, D. An atypical course of coxsackievirus A6 associated hand, foot and mouth disease in extremely low birth weight preterm twins. J. Clin. Virol. 2015, 65, 20–22. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.C.; Jiang, S.W.; Gu, W.Z.; Hu, A.R.; Lu, C.T.; Liang, X.Y.; Hu, Y.R.; Zhu, D.D.; Xie, L. Clinicopathologic features and molecular analysis of enterovirus 71 infection: Report of an autopsy case from the epidemic of hand, foot and mouth disease in China. Pathol Int. 2012, 62, 565–570. [Google Scholar] [CrossRef]
- Lizasoain, A.; Piegas, S.; Victoria, M.; Da Silva, E.E.; Colina, R. Hand-foot-and-mouth disease in uruguay: Coxsackievirus A6 identified as causative of an outbreak in a rural childcare center. J. Med. Virol. 2020, 92, 167–173. [Google Scholar] [CrossRef]
- Mirand, A.; le Sage, F.V.; Pereira, B.; Cohen, R.; Levy, C.; Archimbaud, C.; Peigue-Lafeuille, H.; Bailly, J.L.; Henquell, C. Ambulatory Pediatric Surveillance of Hand, Foot and Mouth Disease as Signal of an Outbreak of Coxsackievirus A6 Infections, France, 2014-2015. Emerg. Infect. Dis. 2016, 22, 1884–1893. [Google Scholar] [CrossRef]
- Drago, F.; Ciccarese, G.; Gariazzo, L.; Cioni, M.; Parodi, A. Acute localized exanthem due to Coxsackievirus A4. Infez. Med. 2017, 25, 274–276. [Google Scholar]
- Brandt, O.; Abeck, D.; Gianotti, R.; Burgdorf, W. Gianotti-Crosti syndrome. J. Am. Acad. Derm. 2006, 54, 136–145. [Google Scholar] [CrossRef]
- Kimmis, B.D.; Downing, C.; Tyring, S. Hand-foot-and-mouth disease caused by coxsackievirus A6 on the rise. Cutis 2018, 102, 353–356. [Google Scholar]
- Zhao, T.S.; Du, J.; Sun, D.P.; Zhu, Q.R.; Chen, L.Y.; Ye, C.; Wang, S.; Liu, Y.Q.; Cui, F.; Lu, Q.B. A review and meta-analysis of the epidemiology and clinical presentation of coxsackievirus A6 causing hand-foot-mouth disease in China and global implications. Rev. Med. Virol. 2020, 30, e2087. [Google Scholar] [CrossRef] [PubMed]
- Mathes, E.F.; Oza, V.; Frieden, I.J.; Cordoro, K.M.; Yagi, S.; Howard, R.; Kristal, L.; Ginocchio, C.C.; Schaffer, J.; Maguiness, S.; et al. “Eczema coxsackium” and unusual cutaneous findings in an enterovirus outbreak. Pediatrics 2013, 132, e149–e157. [Google Scholar] [CrossRef]
- Leung, A.K.C.; Sergi, C.M.; Lam, J.M.; Leong, K.F. Gianotti-Crosti syndrome (papular acrodermatitis of childhood) in the era of a viral recrudescence and vaccine opposition. World J. Pediatr. 2019, 15, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Marcassi, A.P.; Piazza, C.A.D.; Seize, M.; Cestari, S. Atypical Gianotti-Crosti syndrome. Bras Derm. 2018, 93, 265–267. [Google Scholar] [CrossRef] [PubMed]
- Losey, N.A.; Stevenson, B.S.; Busse, H.J.; Damste, J.S.S.; Rijpstra, W.I.C.; Rudd, S.; Lawson, P.A. Thermoanaerobaculum aquaticum gen. nov., sp. nov., the first cultivated member of Acidobacteria subdivision 23, isolated from a hot spring. Int. J. Syst. Evol. Microbiol. 2013, 63, 4149–4157. [Google Scholar] [CrossRef]
- Allmon, A.; Deane, K.; Martin, K.L. Common Skin Rashes in Children. Am. Fam. Physician 2015, 92, 211–216. [Google Scholar]
- Naimer, S.A.; Cohen, A.D.; Mumcuoglu, K.Y.; Vardy, D.A. Household papular urticaria. Isr. Med. Assoc. J. 2002, 4, 911–913. [Google Scholar]
- Millikan, L.E. Papular urticaria. Semin Derm. 1993, 12, 53–56. [Google Scholar]
- Vafaie, J.; Schwartz, R.A. Erythema infectiosum. J. Cutan Med. Surg. 2005, 9, 159–161. [Google Scholar] [CrossRef]
- Nahmias, A.J.; Froeschle, J.E.; Feorino, P.M.; McCord, G. Generalized eruption in a child with eczema due to coxsackievirus A16. Arch. Derm. 1968, 97, 147–148. [Google Scholar] [CrossRef]
- Ganguly, S.; Kuruvila, S. Eczema Coxsackium. Indian J. Derm. 2016, 61, 682–683. [Google Scholar] [CrossRef] [PubMed]
- Gin, A.; King, E.; Scardamaglia, L.; Orchard, D. Eczema exacerbation caused by Coxsackie virus A6. Australas. J. Derm. 2018, 59, 64–65. [Google Scholar] [CrossRef] [PubMed]
- Su, H.J.; Chen, C.B. Eczema coxsackium. Med. J. Aust. 2021, 215, 403. [Google Scholar] [CrossRef] [PubMed]
- Feder, H.M., Jr.; Bennett, N.; Modlin, J.F. Atypical hand, foot, and mouth disease: A vesiculobullous eruption caused by Coxsackie virus A6. Lancet Infect Dis 2014, 14, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Schmader, K. Herpes Zoster. Ann. Intern. Med. 2018, 169, ITC19–ITC31. [Google Scholar] [CrossRef]
- Damour, A.; Garcia, M.; Seneschal, J.; Leveque, N.; Bodet, C. Eczema Herpeticum: Clinical and Pathophysiological Aspects. Clin. Rev. Allergy Immunol. 2020, 59, 1–18. [Google Scholar] [CrossRef]
- Ventarola, D.; Bordone, L.; Silverberg, N. Update on hand-foot-and-mouth disease. Clin. Derm. 2015, 33, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.H.; Huang, Y.P.; Liu, M.C.; Tsou, T.P.; Lin, H.C.; Lin, T.L.; Tsai, C.Y.; Chao, Y.N.; Chang, L.Y.; Hsu, C.M. An outbreak of coxsackievirus A6 hand, foot, and mouth disease associated with onychomadesis in Taiwan, 2010. BMC Infect. Dis. 2011, 11, 346. [Google Scholar] [CrossRef]
- Laga, A.C.; Shroba, S.M.; Hanna, J. Atypical hand, foot and mouth disease in adults associated with coxsackievirus A6: A clinico-pathologic study. J. Cutan Pathol. 2016, 43, 940–945. [Google Scholar] [CrossRef]
- Second, J.; Velter, C.; Cales, S.; Truchetet, F.; Lipsker, D.; Cribier, B. Clinicopathologic analysis of atypical hand, foot, and mouth disease in adult patients. J. Am. Acad. Derm. 2017, 76, 722–729. [Google Scholar] [CrossRef]
- Fraticelli, P.; Benfaremo, D.; Gabrielli, A. Diagnosis and management of leukocytoclastic vasculitis. Intern. Emerg. Med. 2021, 16, 831–841. [Google Scholar] [CrossRef] [PubMed]
- Zelman, B.; Muhlbauer, A.; Kim, W.; Speiser, J. A rare case of papular-purpuric “gloves and socks” syndrome associated with influenza. J. Cutan Pathol. 2022, 49, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Halasz, C.L.; Cormier, D.; Den, M. Petechial glove and sock syndrome caused by parvovirus B19. J. Am. Acad. Derm. 1992, 27, 835–838. [Google Scholar] [CrossRef] [PubMed]
- Segura Saint-Gerons, R.; Ceballos Salobrena, A.; Gutierrez Torres, P.; Gonzalez Ruiz, A.; Gavilan Fernandez, I.; Martinez-Sahuquillo Marquez, A. Papular purpuric gloves and socks syndrome. Presentation of a clinical case. Med. Oral. Patol. Oral. Cir. Bucal 2007, 12, E4–E6. [Google Scholar]
- Huang, W.C.; Huang, L.M.; Lu, C.Y.; Cheng, A.L.; Chang, L.Y. Atypical hand-foot-mouth disease in children: A hospital-based prospective cohort study. Virol. J. 2013, 10, 209. [Google Scholar] [CrossRef]
- Justino, M.C.A.; da, S.M.D.; Souza, M.F.; Farias, F.P.; Dos, S.A.J.C.; Ferreira, J.L.; Lopes, D.P.; Tavares, F.N. Atypical hand-foot-mouth disease in Belem, Amazon region, northern Brazil, with detection of coxsackievirus A6. J. Clin. Virol. 2020, 126, 104307. [Google Scholar] [CrossRef]
- Hartman-Adams, H.; Banvard, C.; Juckett, G. Impetigo: Diagnosis and treatment. Am. Fam. Physician 2014, 90, 229–235. [Google Scholar]
- Arvin, A.M. Varicella-zoster virus. Clin. Microbiol. Rev. 1996, 9, 361–381. [Google Scholar] [CrossRef]
- Bagci, I.S.; Horvath, O.N.; Ruzicka, T.; Sardy, M. Bullous pemphigoid. Autoimmun. Rev. 2017, 16, 445–455. [Google Scholar] [CrossRef]
- Johnson, M.K. Impetigo. Adv. Emerg. Nurs. J. 2020, 42, 262–269. [Google Scholar] [CrossRef]
- Cole, C.; Borradori, L.; Amber, K.T. Deciphering the Contribution of BP230 Autoantibodies in Bullous Pemphigoid. Antibodies 2022, 11, 44. [Google Scholar] [CrossRef] [PubMed]
- Brazel, M.; Desai, A.; Are, A.; Motaparthi, K. Staphylococcal Scalded Skin Syndrome and Bullous Impetigo. Medicina 2021, 57, 1157. [Google Scholar] [CrossRef]
- Chavda, V.P.; Patel, K.; Apostolopoulos, V. Tomato flu outbreak in India. Lancet Respir. Med. 2023, 11, e1–e2. [Google Scholar] [CrossRef] [PubMed]
- Broccolo, F.; Drago, F.; Ciccarese, G.; Genoni, A.; Puggioni, A.; Rosa, G.M.; Parodi, A.; Manukyan, H.; Laassri, M.; Chumakov, K.; et al. Severe atypical hand-foot-and-mouth disease in adults due to coxsackievirus A6: Clinical presentation and phylogenesis of CV-A6 strains. J. Clin. Virol. 2019, 110, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Aswathyraj, S.; Arunkumar, G.; Alidjinou, E.K.; Hober, D. Hand, foot and mouth disease (HFMD): Emerging epidemiology and the need for a vaccine strategy. Med. Microbiol. Immunol. 2016, 205, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Zhang, J. Surveillance on other infectious diarrheal diseases in China from 2014 to 2015. Zhonghua Liu Xing Bing Xue Za Zhi 2017, 38, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.; Zhang, N.; Zhu, B.; Liu, J.; He, R. A descriptive analysis of the Spatio-temporal distribution of intestinal infectious diseases in China. BMC Infect. Dis. 2019, 19, 766. [Google Scholar] [CrossRef]
- Cisterna, D.M.; Lema, C.L.; Martinez, L.M.; Veron, E.; Contarino, L.P.; Acosta, D.; Freire, M.C. Atypical hand, foot, and mouth disease caused by Coxsackievirus A6 in Argentina in 2015. Rev. Argent Microbiol. 2019, 51, 140–143. [Google Scholar] [CrossRef]
- Chiu, H.H.; Liu, M.T.; Chung, W.H.; Ko, Y.S.; Lu, C.F.; Lan, C.E.; Lu, C.W.; Wei, K.C. The Mechanism of Onychomadesis (Nail Shedding) and Beau’s Lines Following Hand-Foot-Mouth Disease. Viruses 2019, 11, 522. [Google Scholar] [CrossRef]
- De Sousa, I.P., Jr.; Giamberardino, H.I.; Raboni, S.M.; Debur, M.C.; de Lourdes Aguiar Oliveira, M.; Burlandy, F.M.; da Silva, E.E. Simultaneous enterovirus EV-D68 and CVA6 infections causing acute respiratory distress syndrome and hand, foot and mouth disease. Virol. J. 2021, 18, 88. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Differential Points | Gianotti–Crosti-Like Eruptions | Gianotti–Crosti Eruptions | Papulosquamous Urticaria | Erythema Infectiosum |
|---|---|---|---|---|
| Fever |
|
|
|
|
| Skin rash |
|
|
|
|
| Itching |
|
|
|
|
| Blisters |
|
|
|
|
| Recurrence |
|
|
|
|
| Duration |
|
|
|
|
| Pathogens |
|
|
| |
| Prevalence age |
|
|
|
|
| Differential Points | Eczema Coxsackium | Herpes Zoster | Herpetic Eczema |
|---|---|---|---|
| Fever |
|
|
|
| Skin rash |
|
|
|
| Pain or itching |
|
|
|
| Complications |
|
|
|
| Recurrence |
|
|
|
| Duration |
|
|
|
| Pathogens |
|
|
|
| Prevalence age |
|
|
|
| Differential Points | Petechial/Purpuric Eruptions | Leukocytoclastic Vasculitis | Glove and Stocking Purpura |
|---|---|---|---|
| Fever |
|
|
|
| Skin rash |
|
|
|
| Itching |
|
|
|
| Recurrence |
|
|
|
| Duration |
|
|
|
| Histopathological features |
|
|
|
| Pathogens |
|
|
|
| Prevalence age |
|
|
|
| Differential Points | Vesiculobullous Exanthema | Bullous Impetigo | Varicella | Primary Immune Bullous (Take Bullous Pemphigoid, for Example) |
|---|---|---|---|---|
| Fever |
|
|
|
|
| Clinical Presentation |
|
|
|
|
| Preferred site |
|
|
|
|
| Itching |
|
|
|
|
| Recurrence |
|
|
|
|
| Duration |
|
|
|
|
| Pathogens |
|
|
|
|
| Prevalence age |
|
|
|
|
| Serotype | Atypical Presentation | Accession Number | Time | Country | References |
|---|---|---|---|---|---|
| CVA6 |
| KX575862 - KX575865 | 2015 | Argentina | [48] |
| CVA6 |
| KC297130 - KC297135 | 2010 | Taiwan, China | [35] |
| CVA6 |
| TW910141 - TW910142 | 2015 | Taiwan, China | [49] |
| CVA6 |
| MT747440 | 2018 | Brazil | [50] |
| CVA6 |
| MH371303 | 2017 | Italy | [44] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Dai, B.; Han, S.; Duan, G.; Yang, H.; Chen, S.; Ji, W.; Jin, Y. Arising Concerns of Atypical Manifestations in Patients with Hand, Foot, and Mouth Disease. Vaccines 2023, 11, 405. https://doi.org/10.3390/vaccines11020405
Chen Y, Dai B, Han S, Duan G, Yang H, Chen S, Ji W, Jin Y. Arising Concerns of Atypical Manifestations in Patients with Hand, Foot, and Mouth Disease. Vaccines. 2023; 11(2):405. https://doi.org/10.3390/vaccines11020405
Chicago/Turabian StyleChen, Yu, Bowen Dai, Shujie Han, Guangcai Duan, Haiyan Yang, Shuaiyin Chen, Wangquan Ji, and Yuefei Jin. 2023. "Arising Concerns of Atypical Manifestations in Patients with Hand, Foot, and Mouth Disease" Vaccines 11, no. 2: 405. https://doi.org/10.3390/vaccines11020405
APA StyleChen, Y., Dai, B., Han, S., Duan, G., Yang, H., Chen, S., Ji, W., & Jin, Y. (2023). Arising Concerns of Atypical Manifestations in Patients with Hand, Foot, and Mouth Disease. Vaccines, 11(2), 405. https://doi.org/10.3390/vaccines11020405