






Geospatial Analyses of Recent Household Surveys to Assess Changes in the Distribution of Zero-Dose Children and Their Associated Factors before and during the COVID-19 Pandemic in Nigeria

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data and Sources
2.1.1. 2018 Nigeria Demographic and Health Survey (DHS)
2.1.2. 2021 Nigeria Multiple Indicator Cluster Survey—National Immunization Coverage Survey (MICS-NICS)
2.1.3. Outcome Indicators of Zero-Dose Children Included in the Study
2.1.4. Independent Variables and Geospatial Covariate Data
2.1.5. Population Data
2.2. Statistical Analysis
2.2.1. Descriptive and Bivariate Analysis
2.2.2. Multilevel Model
2.2.3. Geostatistical Model
3. Results
3.1. Outcome Indicators of Vaccination Coverage
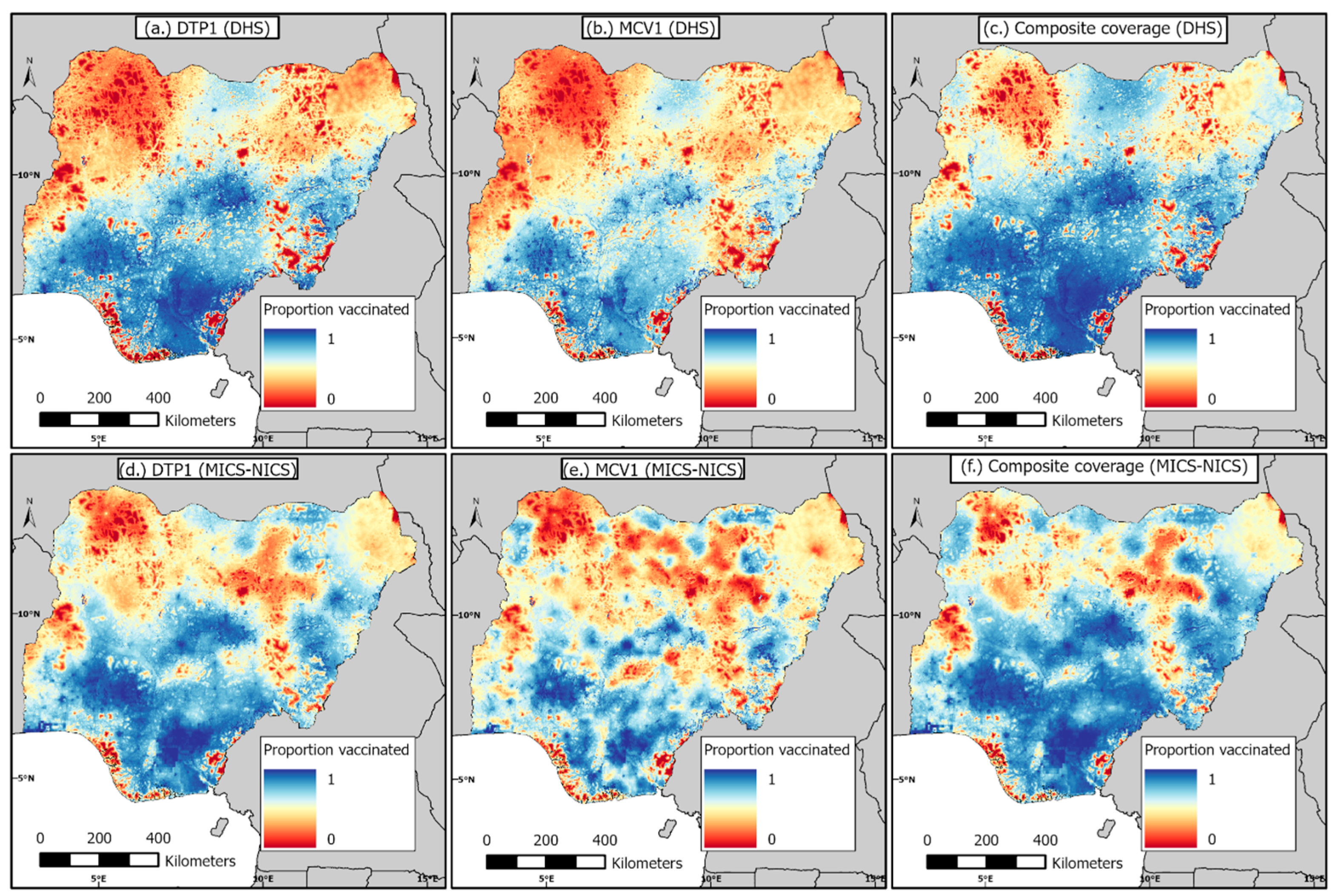
3.2. 1 km 1 km Modelled Estimates of Coverage and Associated Uncertainties before and during the Pandemic
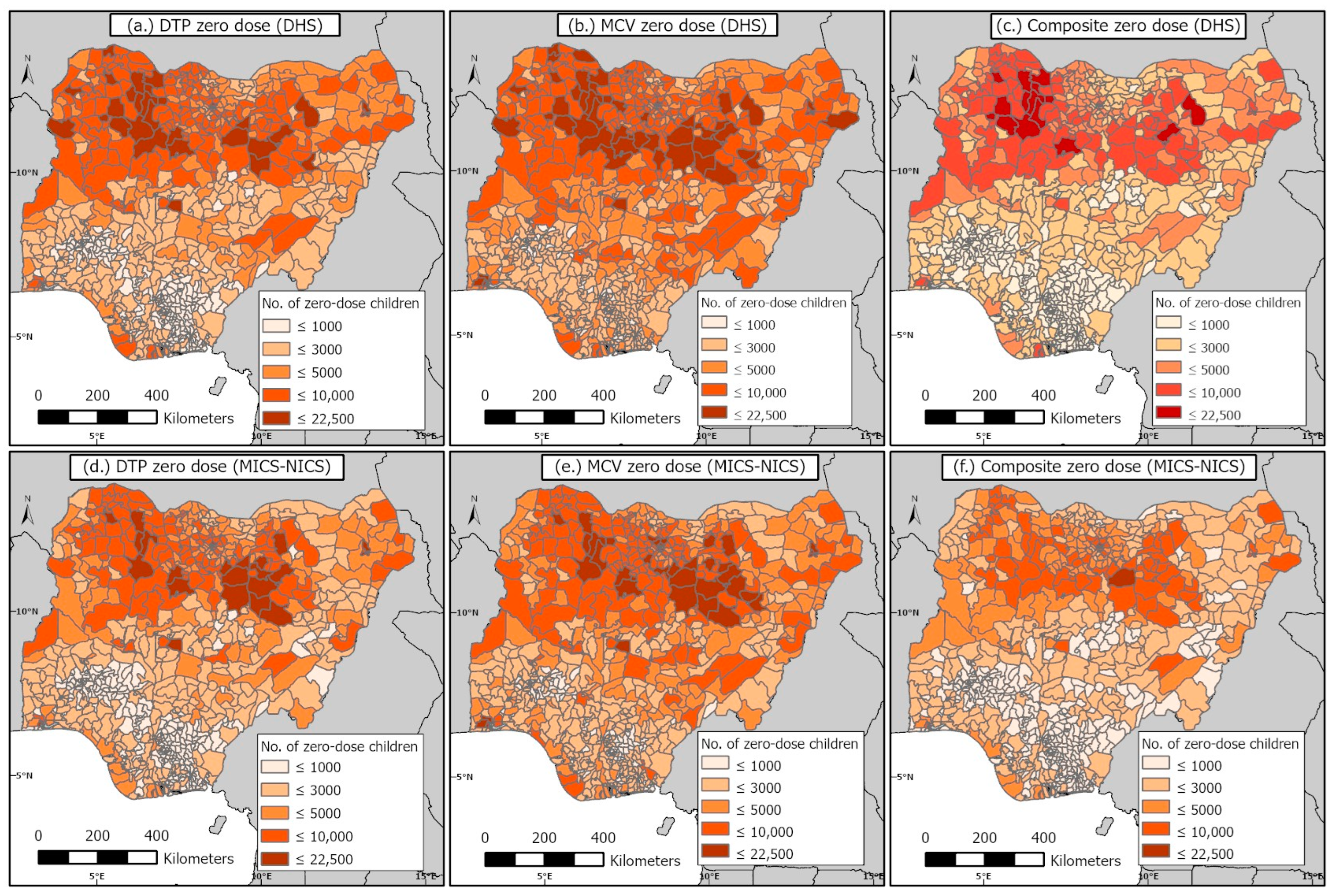
3.3. District-Level Estimates of the Numbers of Zero-Dose Children before and during the Pandemic
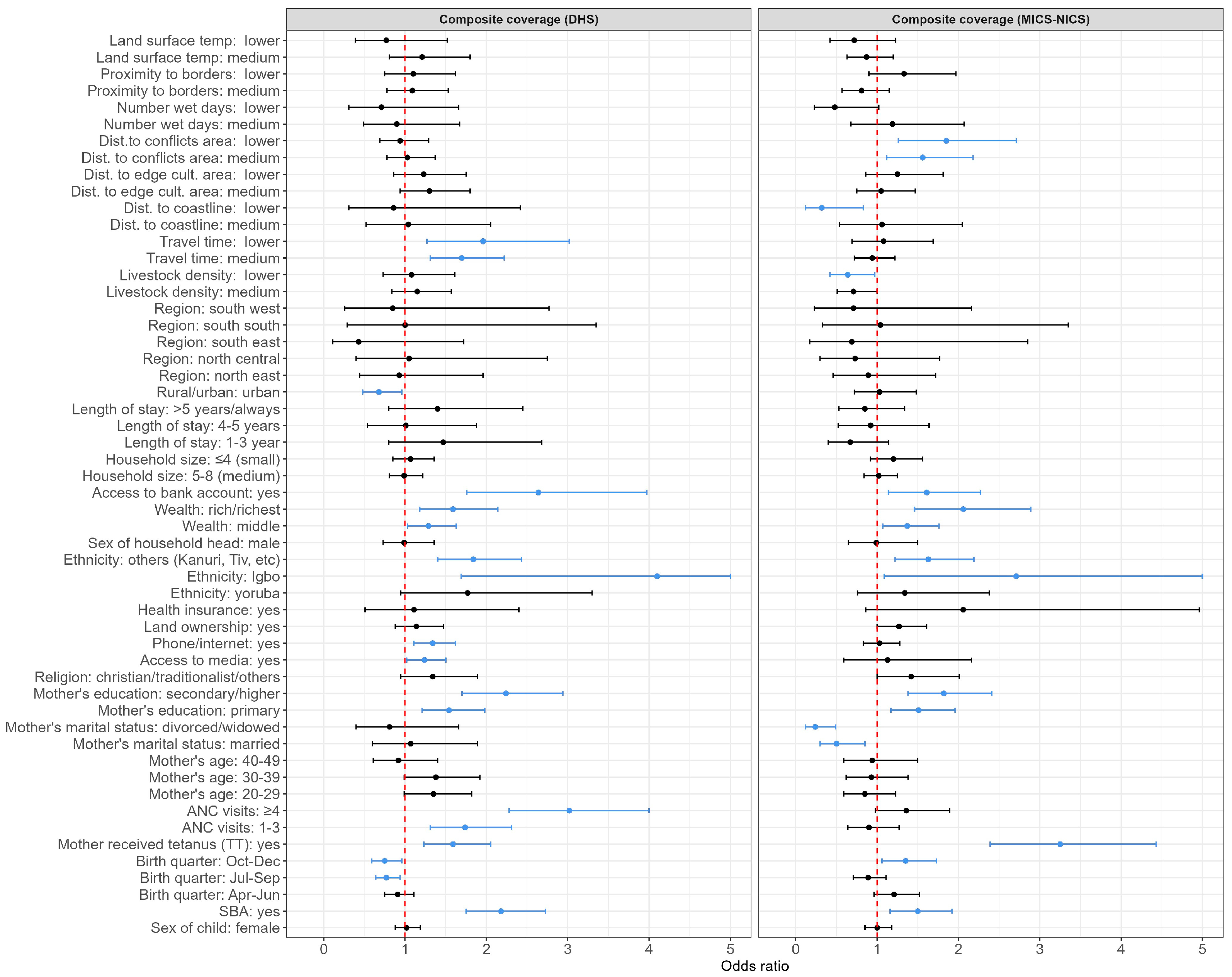
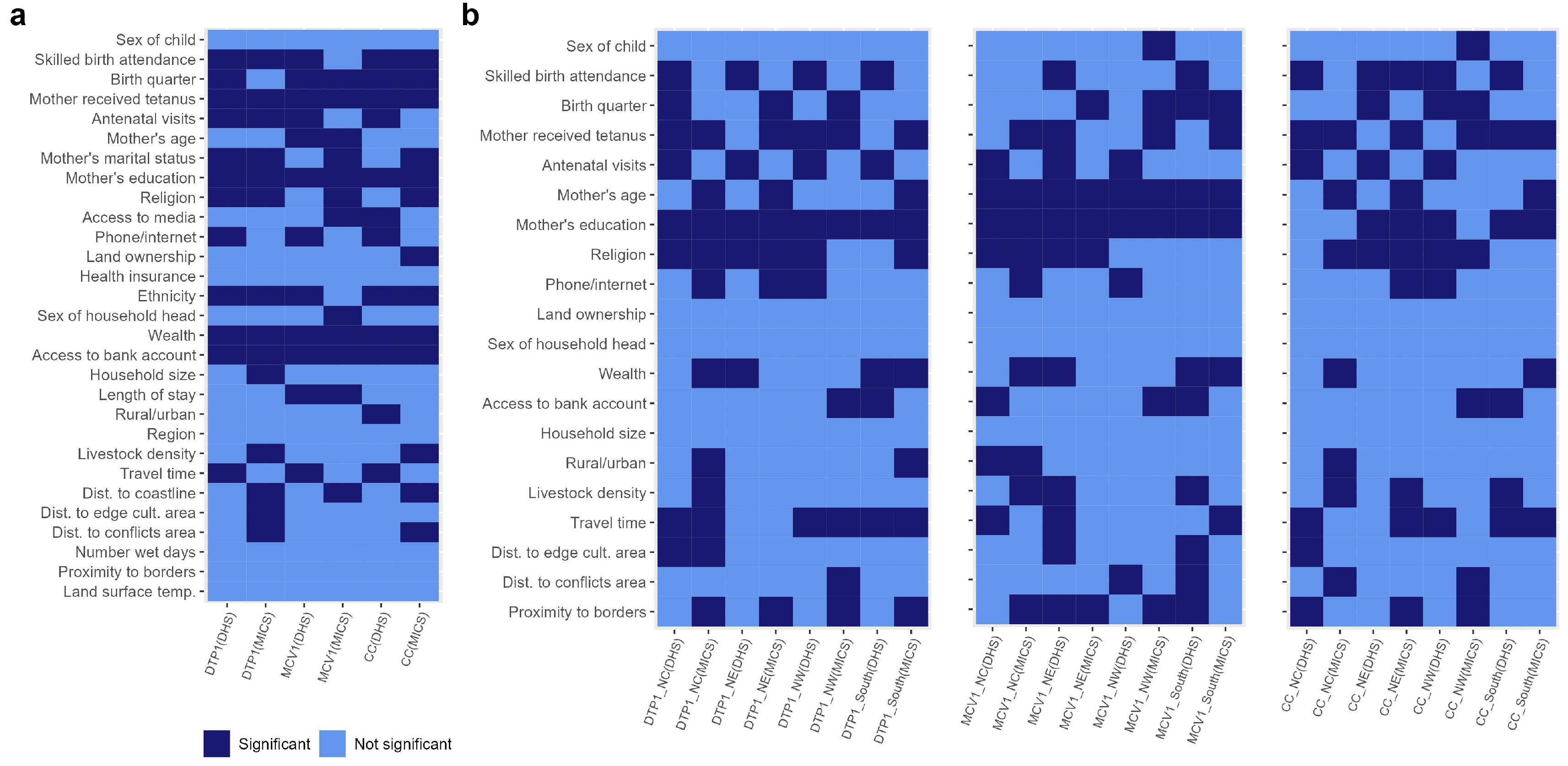
3.4. Risk Factors Associated with Zero Dose at the National and Regional Levels before and during the Pandemic
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Global Immunization Coverage 2021; WHO Estimates of National Immunization Coverage: Geneva, Switzerland, 2021; Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 20 March 2023).
- World Health Organization (WHO); UNICEF. 2022 WHO/UNICEF Estimates of National Immunization Coverage (WUENIC). WHO and UNICEF. 2023. Available online: https://cdn.who.int/media/docs/default-source/immunization/wuenic-progress-and-challenges.pdf?sfvrsn=b5eb9141_12&download=true (accessed on 21 August 2023).
- Causey, K.; Fullman, N.; Sorensen, R.J.; Galles, N.C.; Zheng, P.; Aravkin, A.; Danovaro-Holliday, M.C.; Martinez-Piedra, R.; Sodha, S.V.; Velandia-González, M.P.; et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: A modelling study. Lancet 2021, 398, 522–534. [Google Scholar] [CrossRef] [PubMed]
- Ho, L.L.; Gurung, S.; Mirza, I.; Nicolas, H.D.; Steulet, C.; Burman, A.L.; Danovaro-Holliday, M.C.; Sodha, S.V.; Kretsinger, K. Impact of the SARS-CoV-2 pandemic on vaccine-preventable disease campaigns. Int. J. Infect. Dis. 2022, 119, 201–209. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO); UNICEF. 2021 WHO/UNICEF Estimates of National Immunization Coverage (WUENIC). 2022. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/immunization-coverage/who-unicef-estimates-of-national-immunization-coverage (accessed on 20 February 2023).
- Hogan, D.; Gupta, A. Why Reaching Zero-Dose Children Holds the Key to Achieving the Sustainable Development Goals. Vaccines 2023, 11, 781. [Google Scholar] [CrossRef] [PubMed]
- Utazi, C.E.; Pannell, O.; Aheto, J.M.K.; Wigley, A.; Tejedor-Garavito, N.; Wunderlich, J.; Hagedorn, B.; Hogan, D.; Tatem, A.J. Assessing the characteristics of un- and under-vaccinated children in low- and middle-income countries: A multi-level cross-sectional study. PLOS Glob. Public Health 2022, 2, e0000244. [Google Scholar] [CrossRef] [PubMed]
- Wigley, A.; Lorin, J.; Hogan, D.; Utazi, C.E.; Hagedorn, B.; Dansereau, E.; Tatem, A.J.; Tejedor-Garavito, N. Estimates of the number and distribution of zero-dose and under-immunised children across remote-rural, urban, and conflict-affected settings in low and middle-income countries. PLoS Glob. Public Health 2022, 2, e0001126. [Google Scholar] [CrossRef]
- Chopra, M.; Bhutta, Z.; Blanc, D.C.; Checchi, F.; Gupta, A.; Lemango, E.T.; Levine, O.S.; Lyimo, D.; Nandy, R.; O’brien, K.L.; et al. Addressing the persistent inequities in immunization coverage. Bull World Health Organ. 2020, 98, 146–148. [Google Scholar] [CrossRef] [PubMed]
- WHO. Immunization Agenda 2030: A Global Strategy to Leave No One Behind; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/immunization/immunization_agenda_2030/en/ (accessed on 25 June 2021).
- O’Brien, K.L.; Lemango, E. The big catch-up in immunisation coverage after the COVID-19 pandemic: Progress and challenges to achieving equitable recovery. Lancet 2023, 402, 510–512. [Google Scholar] [CrossRef]
- Shuaib, F.; Garba, A.B.; Meribole, E.; Obasi, S.; Sule, A.; Nnadi, C.; Waziri, N.E.; Bolu, O.; Nguku, P.M.; Ghiselli, M.; et al. Implementing the routine immunisation data module and dashboard of DHIS2 in Nigeria, 2014–2019. BMJ Glob. Health 2020, 5, e002203. [Google Scholar] [CrossRef]
- District Health Information System, Version 2. 2019. Available online: https://www.dhis2.org/ (accessed on 19 March 2023).
- Sbarra, A.N.; Rolfe, S.; Nguyen, J.Q.; Earl, L.; Galles, N.C.; Marks, A.; Abbas, K.M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F. Mapping routine measles vaccination in low- and middle-income countries. Nature 2021, 589, 415–419. [Google Scholar]
- Utazi, C.E.; Thorley, J.; Alegana, V.A.; Ferrari, M.J.; Takahashi, S.; Metcalf, C.J.E.; Lessler, J.; Cutts, F.T.; Tatem, A.J. Mapping vaccination coverage to explore the effects of delivery mechanisms and inform vaccination strategies. Nat. Commun. 2019, 10, 1633. [Google Scholar] [CrossRef]
- Utazi, C.E.; Nilsen, K.; Pannell, O.; Dotse-Gborgbortsi, W.; Tatem, A.J. District-level estimation of vaccination coverage: Discrete vs continuous spatial models. Stat. Med. 2021, 40, 2197–2211. [Google Scholar] [CrossRef] [PubMed]
- United Nations (UN). Transforming Our World: The 2030 Agenda for Sustainable Development. UN. 2015. Available online: https://sustainabledevelopment.un.org/post2015/transformingourworld/publication (accessed on 20 August 2023).
- Gavi The Vaccine Alliance (GAVI). Gavi Strategy 5.0, 2021–2025; GAVI2020, 2020. Available online: https://www.gavi.org/our-alliance/strategy/phase-5-2021-2025 (accessed on 20 June 2023).
- Nigeria Centre for Disease Control and Prevention (NCDC). An Update of Measles Outbreak in Nigeria. 2023. Available online: https://ncdc.gov.ng/diseases/sitreps (accessed on 20 February 2023).
- Utazi, C.E.; Aheto, J.M.; Wigley, A.; Tejedor-Garavito, N.; Bonnie, A.; Nnanatu, C.C.; Wagai, J.; Williams, C.; Setayesh, H.; Tatem, A.J.; et al. Mapping the distribution of zero-dose children to assess the performance of vaccine delivery strategies and their relationships with measles incidence in Nigeria. Vaccine 2023, 41, 170–181. [Google Scholar] [CrossRef] [PubMed]
- Baptiste, A.E.J.; Masresha, B.; Wagai, J.; Luce, R.; Oteri, J.; Dieng, B.; Bawa, S.; Ikeonu, O.C.; Chukwuji, M.; Braka, F.; et al. Trends in measles incidence and measles vaccination coverage in Nigeria, 2008–2018. Vaccine 2021, 39, C89–C95. [Google Scholar] [CrossRef] [PubMed]
- Akwataghibe, N.N.; Ogunsola, E.A.; Broerse, J.E.W.; Popoola, O.A.; Agbo, A.I.; Dieleman, M.A. Exploring Factors Influencing Immunization Utilization in Nigeria-A Mixed Methods Study. Front. Public Health 2019, 7, 392. [Google Scholar] [CrossRef] [PubMed]
- Aheto, J.M.K.; Pannell, O.; Dotse-Gborgbortsi, W.; Trimner, M.K.; Tatem, A.J.; Rhoda, D.A.; Cutts, F.T.; Utazi, C.E. Multilevel analysis of predictors of multiple indicators of childhood vaccination in Nigeria. PLoS ONE 2022, 17, e0269066. [Google Scholar] [CrossRef] [PubMed]
- Oku, A.; Oyo-Ita, A.; Glenton, C.; Fretheim, A.; Eteng, G.; Ames, H.; Muloliwa, A.; Kaufman, J.; Hill, S.; Cliff, J.; et al. Factors affecting the implementation of childhood vaccination communication strategies in Nigeria: A qualitative study. BMC Public Health 2017, 17, 200. [Google Scholar] [CrossRef] [PubMed]
- International Vaccine Access Center (IVAC). Landscape Analysis of Routine Immunization in Nigeria. IVAC; 2012. Available online: https://www.jhsph.edu/ivac/wp-content/uploads/2018/05/IVAC-Landscape-Analysis-Routine-Immunization-Nigeria-Brief.pdf (accessed on 10 March 2023).
- Obanewa, O.A.; Newell, M.L. The role of place of residency in childhood immunisation coverage in Nigeria: Analysis of data from three DHS rounds 2003–2013. BMC Public Health 2020, 20, 123. [Google Scholar] [CrossRef]
- Nigeria Centre for Disease Control (NCDC). First Case of Corona Virus Disease Confirmed in Nigeria. 2020. Available online: https://ncdc.gov.ng/news/227/first-case-of-corona-virus-disease-confirmed-in-nigeria (accessed on 24 March 2023).
- Presidential Task Force on COVID-19—Nigeria. Presidential Task Force on COVID-19: Mid-Term Report. Nigeria. 2020. Available online: https://statehouse.gov.ng/covid19/2020/10/02/presidential-task-force-on-covid-19-mid-term-report/ (accessed on 30 April 2023).
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; Ortiz-Ospina, E.; et al. Coronavirus Pandemic (COVID-19), Vaccinations by Country; Nigeria. Our World in Data. 2020. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 21 February 2023).
- Essoh, T.A.; Adeyanju, G.C.; Adamu, A.A.; Ahawo, A.K.; Aka, D.; Tall, H.; Aplogan, A.; Wiysonge, C.S. Early Impact of SARS-CoV-2 Pandemic on Immunization Services in Nigeria. Vaccines 2022, 10, 1107. [Google Scholar] [CrossRef]
- Ibrahim, D.; Alyssa, S.; Ismael, H.; Ricardo, I. Analysis of the impact of COVID-19 pandemic and response on routine childhood vaccination coverage and equity in Northern Nigeria: A mixed methods study. BMJ Open 2023, 13, e076154. [Google Scholar]
- Adelekan, B.; Goldson, E.; Abubakar, Z.; Mueller, U.; Alayande, A.; Ojogun, T.; Ntoimo, L.; Williams, B.; Muhammed, I.; Okonofua, F. Effect of COVID-19 pandemic on provision of sexual and reproductive health services in primary health facilities in Nigeria: A cross-sectional study. Reprod. Health 2021, 18, 166. [Google Scholar] [CrossRef]
- National Population Commission (NPC) [Nigeria]; ICF. Nigeria Demographic and Health Survey 2018—Final Report. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF. 2019. Available online: https://dhsprogram.com/publications/publication-fr359-dhs-final-reports.cfm (accessed on 16 March 2021).
- National Bureau of Statistics (NBS); United Nations Children’s Fund (UNICEF). Multiple Indicator Cluster Survey 2021—Survey Findings Report; NBS and UNICEF: Abuja, Nigeria, 2022. [Google Scholar]
- World Health Organization (WHO). Vaccination Schedule for Nigeria. WHO: 2023. Available online: https://immunizationdata.who.int/pages/schedule-by-country/nga.html?DISEASECODE=&TARGETPOP_GENERAL= (accessed on 19 February 2023).
- Utazi, C.E.; Wagai, J.; Pannell, O.; Cutts, F.T.; Rhoda, D.A.; Ferrari, M.J.; Dieng, B.; Oteri, J.; Danovaro-Holliday, M.C.; Adeniran, A.; et al. Geospatial variation in measles vaccine coverage through routine and campaign strategies in Nigeria: Analysis of recent household surveys. Vaccine 2020, 38, 3062–3071. [Google Scholar] [CrossRef] [PubMed]
- Utazi, C.E.; Thorley, J.; Alegana, V.A.; Ferrari, M.J.; Takahashi, S.; Metcalf, C.J.E.; Lessler, J.; Tatem, A.J. High resolution age-structured mapping of childhood vaccination coverage in low and middle income countries. Vaccine 2018, 36, 1583–1591. [Google Scholar] [CrossRef] [PubMed]
- WorldPop. Open Spatial Demographic Data and Research. WorldPop. 2021. Available online: https://www.worldpop.org/ (accessed on 20 February 2023).
- United Nations; Department of Economic and Social Affairs, Population Division. World Population Prospects 2022: Release note. Available online: https://population.un.org/wpp/ (accessed on 19 October 2023).
- Leckie, G.; Charlton, C. Runmlwin—A Program to Run the MLwiN Multilevel Modelling Software from within Stata. J. Stat. Softw. 2013, 52, 1–40. [Google Scholar]
- Hedeker, D.; Gibbons, R.D. MIXOR: A computer program for mixed-effects ordinal regression analysis. Comput. Methods Programs Biomed. 1996, 49, 157–176. [Google Scholar] [CrossRef] [PubMed]
- Lindgren, F.; Rue, H. Bayesian Spatial Modelling with R-INLA. J. Stat. Softw. 2015, 63, 25. [Google Scholar] [CrossRef]
- Diggle, P.; Ribeiro, P.J.; MyiLibrary. Model-based geostatistics. In Springer Series in Statistics; Springer: New York, NY, USA, 2007. [Google Scholar]
- Matérn, B. Spatial Variation, 2nd ed.; Springer: Berlin, Germany, 1986. [Google Scholar]
- Lindgren, F.; Rue, H.; Lindström, J. An explicit link between Gaussian fields and Gaussian Markov random fields: The stochastic partial differential equation approach. J. R. Stat. Soc. Ser. B 2011, 73, 423–498. [Google Scholar] [CrossRef]
- Rue, H.; Martino, S.; Lindgren, F.; Simpson, D.; Riebler, A.; Krainski, E.T. INLA: Functions which allow to perform full Bayesian analysis of latent Gaussian models using Integrated Nested Laplace approximation. R Package Version 0.0-1440400394. 2019. Available online: https://rdrr.io/github/andrewzm/INLA/ (accessed on 11 February 2023).
- Mosser, J.F.; Gagne-Maynard, W.; Rao, P.C.; Osgood-Zimmerman, A.; Fullman, N.; Graetz, N.; Burstein, R.; Updike, R.L.; Liu, P.Y.; Ray, S.E.; et al. Mapping diphtheria-pertussis-tetanus vaccine coverage in Africa, 2000–2016: A spatial and temporal modelling study. Lancet 2019, 393, 1843–1855. [Google Scholar] [CrossRef]
- Ludlow, L.; Klein, K. Suppressor Variables: The Difference between ‘is’ Versus ‘Acting As’. J. Stat. Educ. 2014, 22. [Google Scholar] [CrossRef]
- Nigeria Centre for Disease Control and Prevention (NCDC). COVID-19 NIGERIA. Nigeria. Available online: https://covid19.ncdc.gov.ng/ (accessed on 20 April 2023).
- Sato, R. Pattern of vaccination delivery around COVID-19 lockdown in Nigeria. Hum. Vaccines Immunother. 2021, 17, 2951–2953. [Google Scholar] [CrossRef]
- Amouzou, A.; Maïga, A.; Faye, C.M.; Chakwera, S.; Melesse, D.Y.; Mutua, M.K.; Thiam, S.; Abdoulaye, I.B.; Afagbedzi, S.K.; Iknane, A.A.; et al. Health service utilisation during the COVID-19 pandemic in sub-Saharan Africa in 2020: A multicountry empirical assessment with a focus on maternal, newborn and child health services. BMJ Glob. Health 2022, 7, e008069. [Google Scholar] [CrossRef]
- Utazi, C.E.; Aheto, J.M.K.; Chan, H.M.T.; Tatem, A.J.; Sahu, S.K. Conditional probability and ratio-based approaches for mapping the coverage of multi-dose vaccines. Stat. Med. 2022, 41, 5662–5678. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). States Adopt Integrated Vaccination Strategy to Reach Unimmunized Children, Nigeria. 2022. Available online: https://www.afro.who.int/countries/nigeria/news/states-adopt-integrated-vaccination-strategy-reach-unimmunized-children (accessed on 19 February 2023).
- Burgert, C.R.; Colston, J.; Roy, T.; Zachary, B. Geographic displacement procedure and georeferenced data release policy for the Demographic and Health Surveys. In DHS Spatial Analysis Reports No 7; ICF International: Calverton, MD, USA, 2013. [Google Scholar]
- Leasure, D.R.; Jochem, W.C.; Weber, E.M.; Tatem, A.J. National population mapping from sparse survey data: A hierarchical Bayesian modeling framework to account for uncertainty. Proc. Natl. Acad. Sci. USA 2020, 117, 24173–24179. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, K.; Tejedor-Garavito, N.; Leasure, D.R.; Utazi, C.E.; Ruktanonchai, C.W.; Wigley, A.S.; Dooley, C.A.; Matthews, Z.; Tatem, A.J. A review of geospatial methods for population estimation and their use in constructing reproductive, maternal, newborn, child and adolescent health service indicators. BMC Health Serv. Res. 2021, 21, 370. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aheto, J.M.K.; Olowe, I.D.; Chan, H.M.T.; Ekeh, A.; Dieng, B.; Fafunmi, B.; Setayesh, H.; Atuhaire, B.; Crawford, J.; Tatem, A.J.; et al. Geospatial Analyses of Recent Household Surveys to Assess Changes in the Distribution of Zero-Dose Children and Their Associated Factors before and during the COVID-19 Pandemic in Nigeria. Vaccines 2023, 11, 1830. https://doi.org/10.3390/vaccines11121830
Aheto JMK, Olowe ID, Chan HMT, Ekeh A, Dieng B, Fafunmi B, Setayesh H, Atuhaire B, Crawford J, Tatem AJ, et al. Geospatial Analyses of Recent Household Surveys to Assess Changes in the Distribution of Zero-Dose Children and Their Associated Factors before and during the COVID-19 Pandemic in Nigeria. Vaccines. 2023; 11(12):1830. https://doi.org/10.3390/vaccines11121830
Chicago/Turabian StyleAheto, Justice Moses K., Iyanuloluwa Deborah Olowe, Ho Man Theophilus Chan, Adachi Ekeh, Boubacar Dieng, Biyi Fafunmi, Hamidreza Setayesh, Brian Atuhaire, Jessica Crawford, Andrew J. Tatem, and et al. 2023. "Geospatial Analyses of Recent Household Surveys to Assess Changes in the Distribution of Zero-Dose Children and Their Associated Factors before and during the COVID-19 Pandemic in Nigeria" Vaccines 11, no. 12: 1830. https://doi.org/10.3390/vaccines11121830
APA StyleAheto, J. M. K., Olowe, I. D., Chan, H. M. T., Ekeh, A., Dieng, B., Fafunmi, B., Setayesh, H., Atuhaire, B., Crawford, J., Tatem, A. J., & Utazi, C. E. (2023). Geospatial Analyses of Recent Household Surveys to Assess Changes in the Distribution of Zero-Dose Children and Their Associated Factors before and during the COVID-19 Pandemic in Nigeria. Vaccines, 11(12), 1830. https://doi.org/10.3390/vaccines11121830