
Systemic Adverse Effects Induced by the BNT162b2 Vaccine Are Associated with Higher Antibody Titers from 3 to 6 Months after Vaccination

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Population and Study Design
2.2. Structured Self-Report Questionnaire to Obtain Individual Variables
2.3. Data Analysis
3. Results
3.1. Incidence of Adverse Effects in Response to the BNT162b2 Vaccine
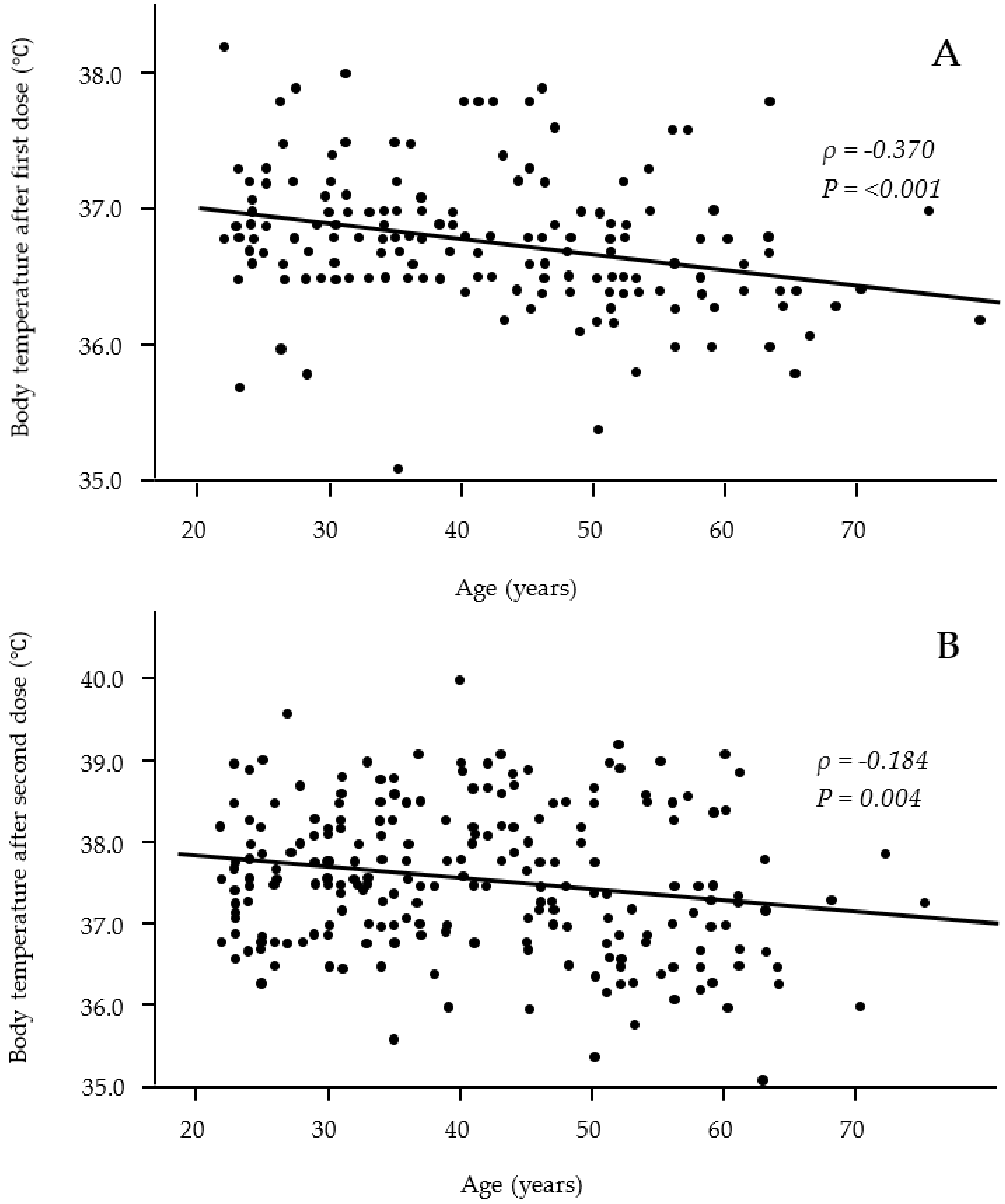
3.2. Relationship between Participants’ Characteristics and Vaccine-Related Systemic Adverse Effects
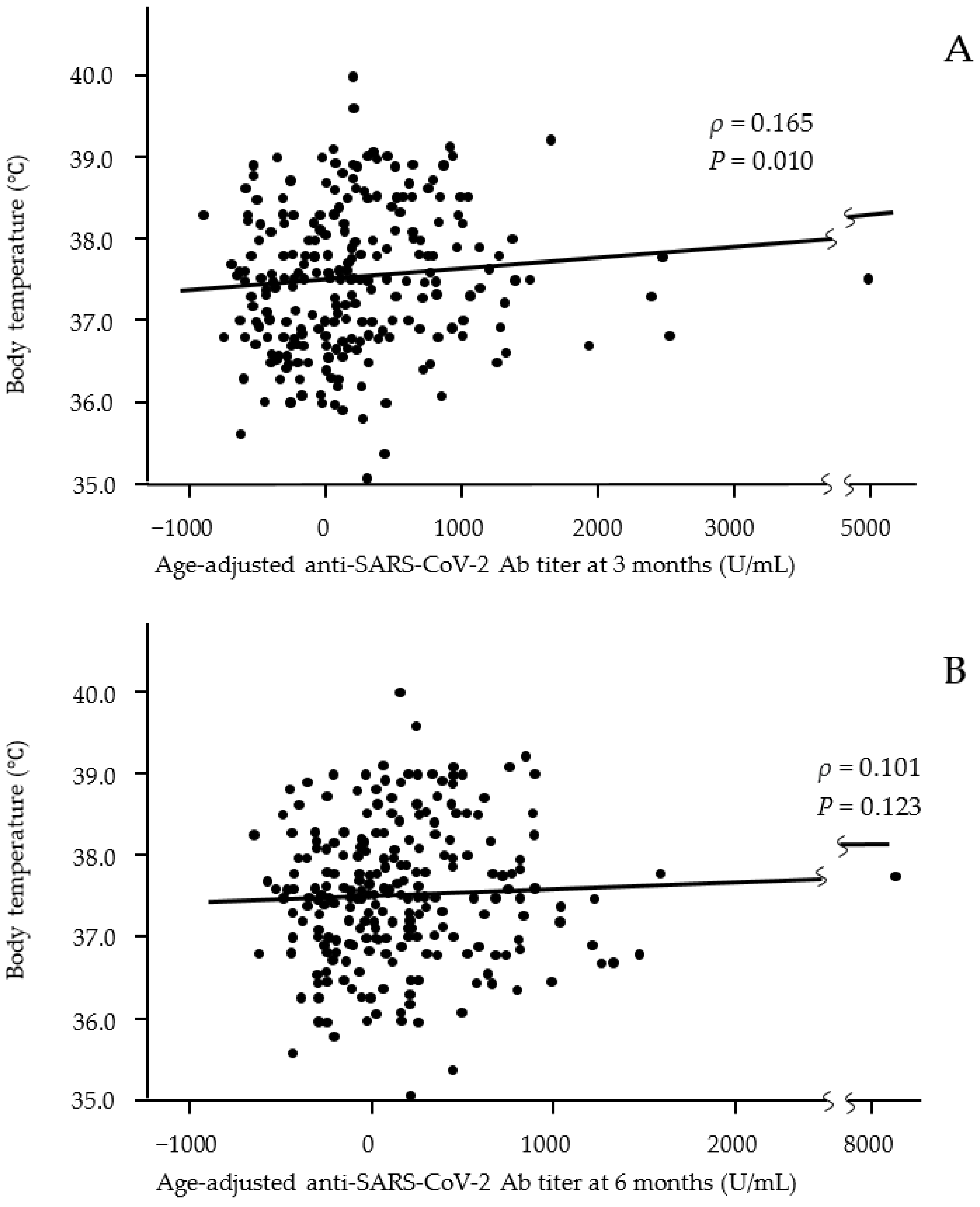
3.3. Association between Ab Titers and Vaccine-Related Adverse Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. COVID-19 breakthrough infections in vaccinated health care workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. C4591001 clinical trial group. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Kozakai, R.; Kushida, A.; Moumouni, P.F.; Okuma, S.; Takahashi, K.; Hoshi, K.; Sato, Y.; Takahashi, M.; Chida, N.; Takahashi, M.; et al. Assessment of COVID-19 mRNA vaccination titer and side effects in healthy volunteers. J. Lab. Med. 2021. [Google Scholar] [CrossRef]
- Izumo, T.; Kuse, N.; Awano, N.; Tone, M.; Sakamoto, K.; Takada, K.; Muto, Y.; Fujimoto, K.; Saiki, A.; Ito, Y.; et al. Side effects and antibody titer transition of the BNT162b2 messenger ribonucleic acid coronavirus disease 2019 vaccine in Japan. Respir. Investig. 2021, 59, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Coggins, S.A.; Laing, E.D.; Olsen, C.H.; Goguet, E.; Moser, M.; Jackson-Thompson, B.M.; Samuels, E.C.; Pollett, S.D.; Tribble, D.R.; Davies, J.; et al. Adverse effects and antibody titers in response to the BNT162b2 mRNA COVID-19 vaccine in a prospective study of healthcare workers. Open Forum Infect. Dis. 2021, 9, ofab575. [Google Scholar] [CrossRef] [PubMed]
- Debes, A.K.; Xiao, S.; Colantuoni, E.; Egbert, E.R.; Caturegli, P.; Gadala, A.; Milstone, A.M. association of vaccine type and prior SARS-CoV-2 infection with symptoms and antibody measurements following vaccination among health care workers. JAMA Intern. Med. 2021, 181, 1660–1662. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, M.; Higa, Y.; Esaki, A.; Nabeshima, Y.; Nakazono, A. Does reactogenicity after a second injection of the BNT162b2 vaccine predict spike IgG antibody levels in healthy Japanese subjects? PLoS ONE 2021, 16, e0257668. [Google Scholar] [CrossRef] [PubMed]
- Maeda, K.; Amano, M.; Uemura, Y.; Tsuchiya, K.; Matsushima, T.; Noda, K.; Shimizu, Y.; Fujiwara, A.; Takamatsu, Y.; Ichikawa, Y.; et al. Correlates of neutralizing/SARS-CoV-2-S1-binding antibody response with adverse effects and immune kinetics in BNT162b2-vaccinated individuals. Sci. Rep. 2021, 11, 22848. [Google Scholar] [CrossRef] [PubMed]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jürjenson, V.; Adamson, A.; Haljasmägi, L.; Rumm, A.P.; Maruste, R.; Kärner, J.; et al. Dynamics of antibody response to BNT162b2 vaccine after six months: A longitudinal prospective study. Lancet Reg. Health Eur. 2021, 10, 100208. [Google Scholar] [CrossRef] [PubMed]
- Krammer, F.; Srivastava, K.; Alshammary, H.; Amoako, A.A.; Awawda, M.H.; Beach, K.F.; Bermúdez-González, M.C.; Bielak, D.A.; Carreño, J.M.; Chernet, R.L.; et al. Antibody responses in seropositive persons after a single dose of SARS-CoV-2 mRNA vaccine. N. Engl. J. Med. 2021, 384, 1372–1374. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Sawahata, M.; Nakamura, Y.; Kurihara, M.; Koike, R.; Katsube, O.; Hagiwara, K.; Niho, S.; Masuda, N.; Tanaka, T.; et al. Age and smoking predict antibody titres at 3 months after the second dose of the BNT162b2 COVID-19 vaccine. Vaccines 2021, 9, 1042. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Sawahata, M.; Nakamura, Y.; Koike, R.; Katsube, O.; Hagiwara, K.; Niho, S.; Masuda, N.; Tanaka, T.; Sugiyama, K. Attenuation of antibody titers from 3 to 6 months after the second dose of the BNT162b2 vaccine depends on sex, with age and smoking risk factors for lower antibody titers at 6 months. Vaccines 2021, 9, 1500. [Google Scholar] [CrossRef] [PubMed]
- Perkmann, T.; Perkmann-Nagele, N.; Breyer, M.K.; Breyer-Kohansal, R.; Burghuber, O.C.; Hartl, S.; Aletaha, D.; Sieghart, D.; Quehenberger, P.; Marculescu, R.; et al. Side-by-side comparison of three fully automated SARS-CoV-2 antibody assays with a focus on specificity. Clin. Chem. 2020, 66, 1405–1413. [Google Scholar] [CrossRef] [PubMed]
- Roman, M.J.; Shanker, B.A.; Davis, A.; Lockshin, M.D.; Sammaritano, L.; Simantov, R.; Crow, M.K.; Schwartz, J.E.; Paget, S.A.; Devereux, R.B.; et al. Prevalence and correlates of accelerated atherosclerosis in systemic lupus erythematosus. N. Engl. J. Med. 2003, 349, 2399–2406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodson, N.; Marks, J.; Lunt, M.; Symmons, D. Cardiovascular admissions and mortality in an inception cohort of patients with rheumatoid arthritis with onset in the 1980s and 1990s. Ann. Rheum. 2005, 64, 1595–1601. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Adverse Effects | After First Dose | After Second Dose | Rate of Concordance between 1st and 2nd |
|---|---|---|---|
| Systemic reactions | |||
| Fever ≥ 37.0 °C | 17.0% (56/274/48) | 56.8% (191/145/42) | 83.9% (47/56) |
| General fatigue | 35.0% (132/245/1) | 73.3% (277/101/0) | 93.9% (124/132) |
| Headache | 20.7% (78/299/1) | 46.0% (173/203/2) | 79.5% (62/78) |
| Muscle pain | 18.6% (70/307/1) | 35.7% (135/243/0) | 80.0% (56/70) |
| Joint pain | 7.7% (29/348/1) | 33.2% (125/252/1) | 86.2% (25/29) |
| Nausea | 2.4% (9/368/1) | 7.0% (26/347/5) | 66.7% (6/9) |
| Diarrhea | 1.1% (4/373/1) | 3.7% (14/362/2) | 50.0% (2/4) |
| Local reactions | |||
| Pain | 89.6% (337/39/2) | 83.3% (310/62/6) | 87.2% (294/337) |
| Swelling | 31.6% (119/257/2) | 31.1% (117/259/2) | 74.8% (89/119) |
| Induration | 23.4% (88/288/2) | 21.0% (79/297/2) | 72.7% (64/88) |
| Itching | 16.5% (62/314/2) | 17.2% (65/313/0) | 72.6% (45/62) |
| Acetaminophen use | 21.1% (76/284/18) | 57.1% (210/158/10) | 76.3% (58/76) |
| Risk Factors | After the First Dose | After the Second Dose | ||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Sex (female) | 1.862 | 0.789–4.392 | 2.139 | 1.185–3.859 |
| Age (older) | 0.962 | 0.931–0.994 | 0.957 | 0.936–0.979 |
| BMI (obesity) | 1.054 | 0.966–1.149 | 0.995 | 0.929–1.066 |
| Smoking | 0.677 | 0.303–1.510 | 1.616 | 0.913–2.863 |
| Drinking | 0.738 | 0.349–1.563 | 0.584 | 0.338–1.010 |
| Any allergic history | 0.702 | 0.268–1.842 | 1.312 | 0.629–2.736 |
| Food | 0.748 | 0.207–2.700 | 1.088 | 0.411–2.879 |
| Drug or chemical | 0.955 | 0.247–3.696 | 1.018 | 0.368–2.813 |
| Any allergic disease | 0.804 | 0.155–4.183 | 3.125 | 0.918–10.64 |
| Allergic rhinitis | 3.368 | 0.751–15.12 | 0.455 | 0.145–1.428 |
| Asthma | 1.695 | 0.602–4.768 | 0.955 | 0.389–2.347 |
| Atopic dermatitis/Urticaria | 1.869 | 0.703–4.968 | 0.757 | 0.323–1.774 |
| Diabetes mellitus | 5.979 | 0.953–37.50 | 1.457 | 0.287–7.411 |
| Hypertension | 0.522 | 0.085–3.193 | 0.525 | 0.159–1.732 |
| Dyslipidemia | 8.750 | 1.814–42.20 | 2.284 | 0.593–8.804 |
| Collagen diseases | 2.727 | 0.629–11.83 | 3.501 | 0.690–17.76 |
| Adverse Effects | After the First Dose | After the Second Dose | ||
|---|---|---|---|---|
| Median (IQR) U/mL | p-Value | Median (IQR) U/mL | p-Value | |
| Systemic reactions | ||||
| Fever (≥37.0 °C) | 153 (−242 to 529)/−28 (−306 to 293) | 0.042 | 110 (−259 to 511)/−69 (−335 to 263) | 0.002 |
| General fatigue * | 22 (−337 to 369)/0 (−279 to 334) | 0.841 | 60 (−287 to 430)/−109 (−327 to 130) | 0.010 |
| Headache * | −30 (−416 to 334)/0 (−285 to 355) | 0.289 | 70 (−309 to 481)/−47 (−293 to 297) | 0.120 |
| Muscle pain * | 32 (−329 to 395)/0 (−293 to 341) | 0.770 | 90 (−246 to 340)/−39 (−336 to 352) | 0.058 |
| Joint pain * | 189 (−133 to 751)/−13 (−308 to 321) | 0.014 | 147 (−140 to 510)/−72 (−370 to 275) | <0.001 |
| Nausea * | 145 (−516 to 369)/0 (−299 to 340) | 0.926 | −249 (−441 to 171)/9 (−285 to 353) | 0.088 |
| Diarrhea * | 418(120 to 691)/0 (−299 to 340) | 0.295 | −91 (−413 to 376)/1 (−296 to 341) | 0.430 |
| Local reactions | ||||
| Pain * | 2 (−308 to 369)/−88 (−256 to 237) | 0.498 | −1 (−317 to 341)/26 (−226 to 335) | 0.528 |
| Swelling * | 0 (−307 to 395)/−3 (−299 to 317) | 0.822 | 0 (−312 to 411)/−11 (−293 to 322) | 0.780 |
| Induration * | 38 (−293 to 510)/−1 (−299 to 318) | 0.289 | −18 (−311 to 316)/0 (−299 to 339) | 0.902 |
| Itching * | 81 (−174 to 451)/−17 (−309 to 339) | 0.265 | 9 (−273 to 269)/0 (−301 to 364) | 0.896 |
| Acetaminophen use * | 108 (−281 to 632)/−17 (−299 to 292) | 0.136 | 82 (−256 to 517)/−84 (−371 to 226) | <0.001 |
| Adverse Effects | After the First Dose | After the Second Dose | ||
|---|---|---|---|---|
| Median (IQR) U/mL | p-Value | Median (IQR) U/mL | p-Value | |
| Systemic reactions | ||||
| Fever (≥37.0 °C) | 60 (−181 to 343)/−11 (−227to 256) | 0.187 | 57 (−201 to 359)/−25 (−229 to 207) | 0.065 |
| General fatigue * | 0 (−242 to 286)/1 (−223 to 263) | 0.853 | 35 (−217 to 328)/−117 (−241 to 174) | 0.015 |
| Headache * | −28 (−290 to 290)/8 (−214 to 263) | 0.278 | 30 (−240 to 336)/−20 (−224 to 254) | 0.425 |
| Muscle pain * | −4 (−256 to 248)/7 (−222 to 274) | 0.635 | 33 (−178 to 288)/−19 (−241 to 265) | 0.237 |
| Joint pain * | 142 (−71 to 461)/−7 (−240 to 256) | 0.023 | 54 (−92 to 339)/−58 (−264 to 244) | 0.001 |
| Nausea * | −56 (−339 to 314)/6 (−224 to 270) | 0.580 | −188 (−303 to −7)/14 (−221 to 283) | 0.013 |
| Diarrhea * | 695 (169 to 1036)/0 (−225 to 268) | 0.181 | −148 (−308 to 295)/1 (−224 to 271) | 0.294 |
| Local reactions | ||||
| Pain * | 9 (−240 to 274)/−55 (−186 to 144) | 0.441 | −9 (−317 to 341)/42 (−226 to 335) | 0.257 |
| Swelling * | 31 (−210 to 306)/−9 (−238 to 268) | 0.543 | −4 (−212 to 256)/3 (−232 to 273) | 0.785 |
| Induration * | 0 (−203 to 334)/6 (−233 to 268) | 0.697 | −49(−244 to 244)/11 (−226 to 280) | 0.476 |
| Itching * | 37 (−169 to 358)/−9 (−239 to 268) | 0.304 | 1 (−239 to 200)/0 (−224 to 281) | 0.735 |
| Acetaminophen use * | 78 (−224 to 446)/−8 (−233 to 251) | 0.191 | 46 (−208 to 334)/−58 (−246 to 209) | 0.019 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koike, R.; Sawahata, M.; Nakamura, Y.; Nomura, Y.; Katsube, O.; Hagiwara, K.; Niho, S.; Masuda, N.; Tanaka, T.; Sugiyama, K. Systemic Adverse Effects Induced by the BNT162b2 Vaccine Are Associated with Higher Antibody Titers from 3 to 6 Months after Vaccination. Vaccines 2022, 10, 451. https://doi.org/10.3390/vaccines10030451
Koike R, Sawahata M, Nakamura Y, Nomura Y, Katsube O, Hagiwara K, Niho S, Masuda N, Tanaka T, Sugiyama K. Systemic Adverse Effects Induced by the BNT162b2 Vaccine Are Associated with Higher Antibody Titers from 3 to 6 Months after Vaccination. Vaccines. 2022; 10(3):451. https://doi.org/10.3390/vaccines10030451
Chicago/Turabian StyleKoike, Ryousuke, Michiru Sawahata, Yosikazu Nakamura, Yushi Nomura, Otohiro Katsube, Koichi Hagiwara, Seiji Niho, Norihiro Masuda, Takaaki Tanaka, and Kumiya Sugiyama. 2022. "Systemic Adverse Effects Induced by the BNT162b2 Vaccine Are Associated with Higher Antibody Titers from 3 to 6 Months after Vaccination" Vaccines 10, no. 3: 451. https://doi.org/10.3390/vaccines10030451
APA StyleKoike, R., Sawahata, M., Nakamura, Y., Nomura, Y., Katsube, O., Hagiwara, K., Niho, S., Masuda, N., Tanaka, T., & Sugiyama, K. (2022). Systemic Adverse Effects Induced by the BNT162b2 Vaccine Are Associated with Higher Antibody Titers from 3 to 6 Months after Vaccination. Vaccines, 10(3), 451. https://doi.org/10.3390/vaccines10030451