
Vaccine-Acquired SARS-CoV-2 Immunity versus Infection-Acquired Immunity: A Comparison of Three COVID-19 Vaccines
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Blood Samples, Specimen Processing, and Storage
2.3. ELISAs
2.4. IgG Avidity Assays
2.5. Memory B Cell ELISpot Assays
2.6. Immunofluorescence-Based SARS-CoV-2 Live Virus Microneutralization Assays
2.7. Activation-Induced Marker (AIM) and Intracellular Cytokine Staining (ICS) Analyses
3. Results
3.1. Study Participants
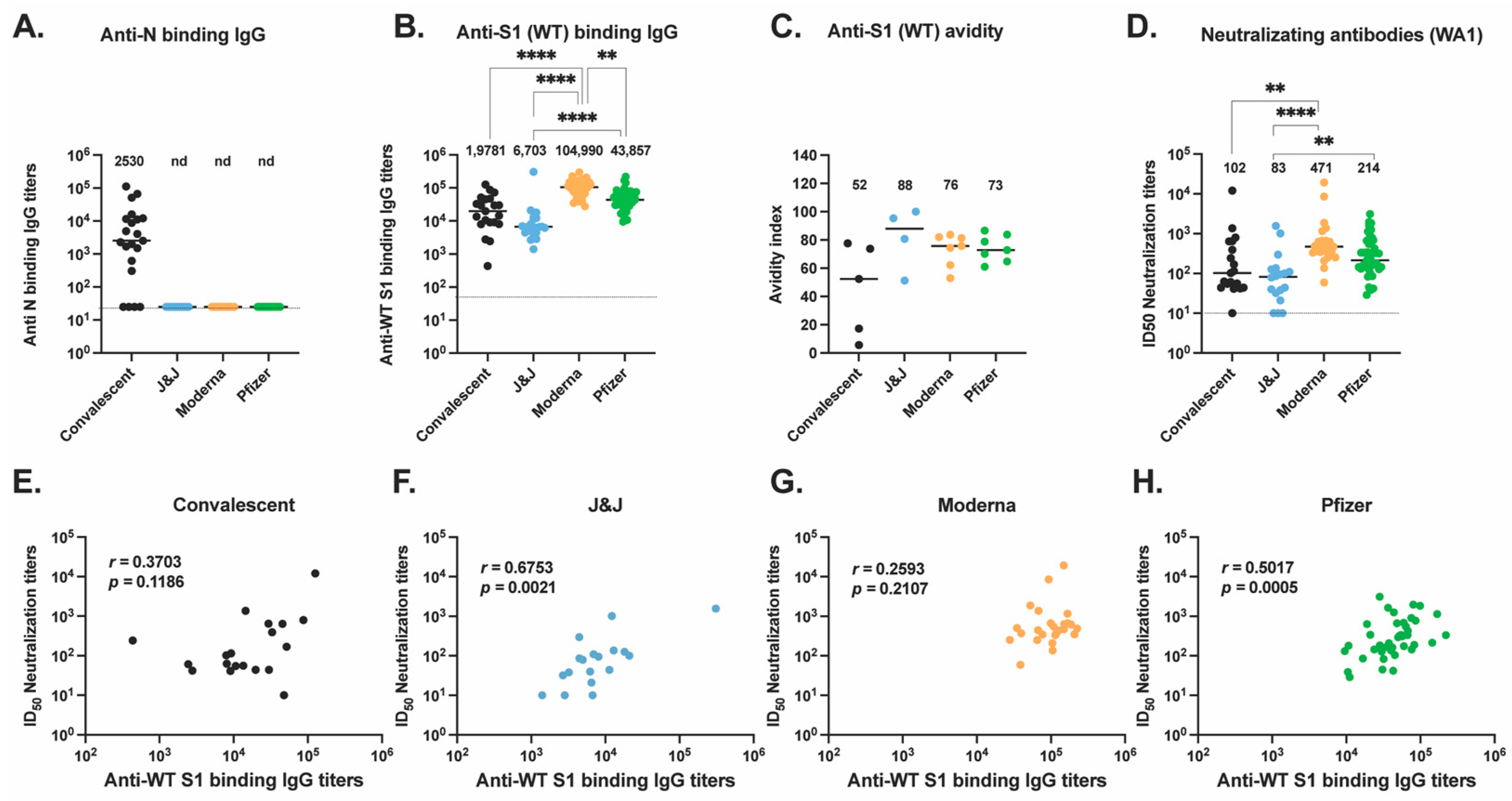
3.2. Anti-S Antibody Responses in Vaccinated and Convalescent Participants
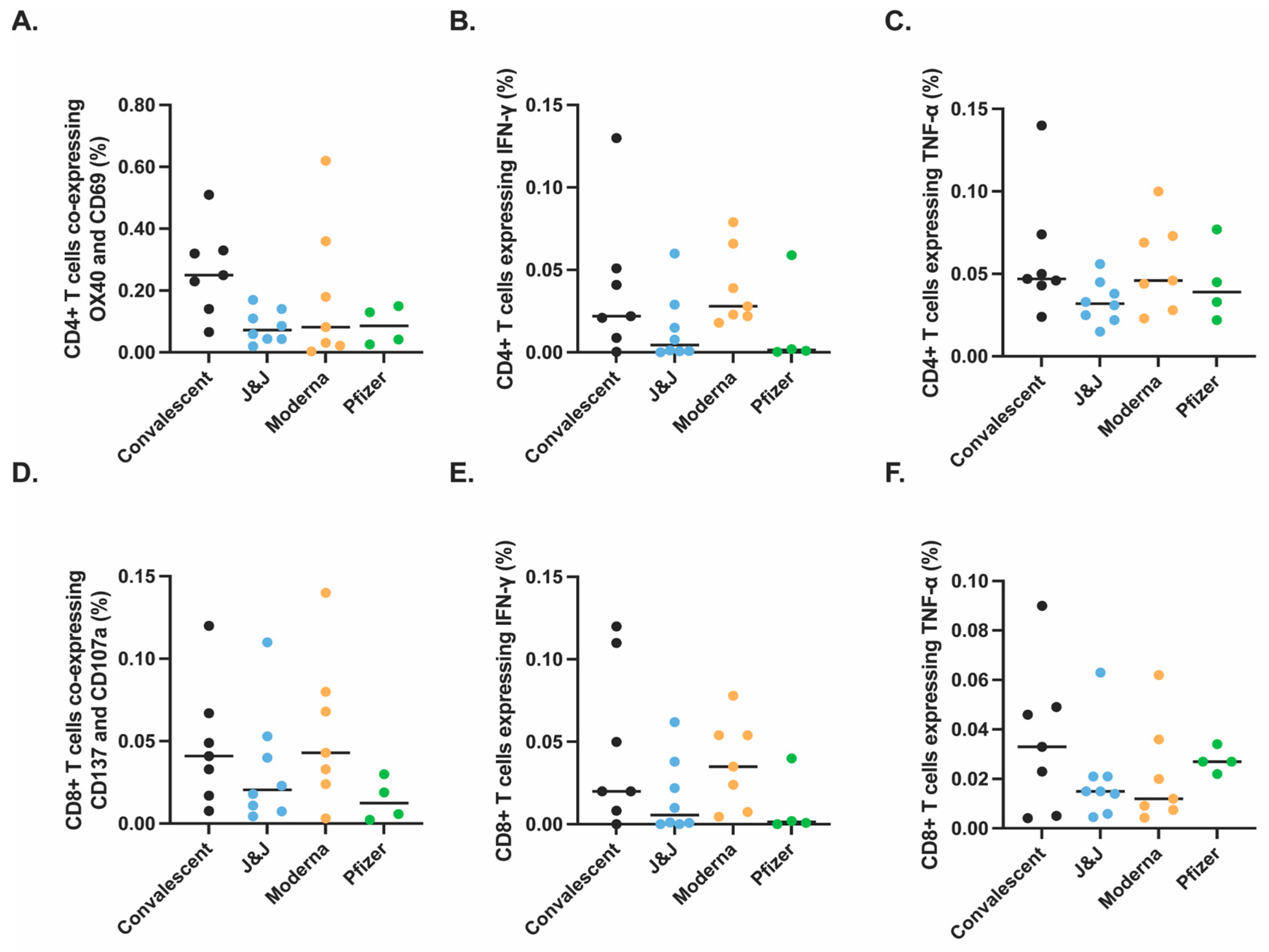
3.3. Spike-Specific T Cell Responses in Vaccinated and Convalescent Participants
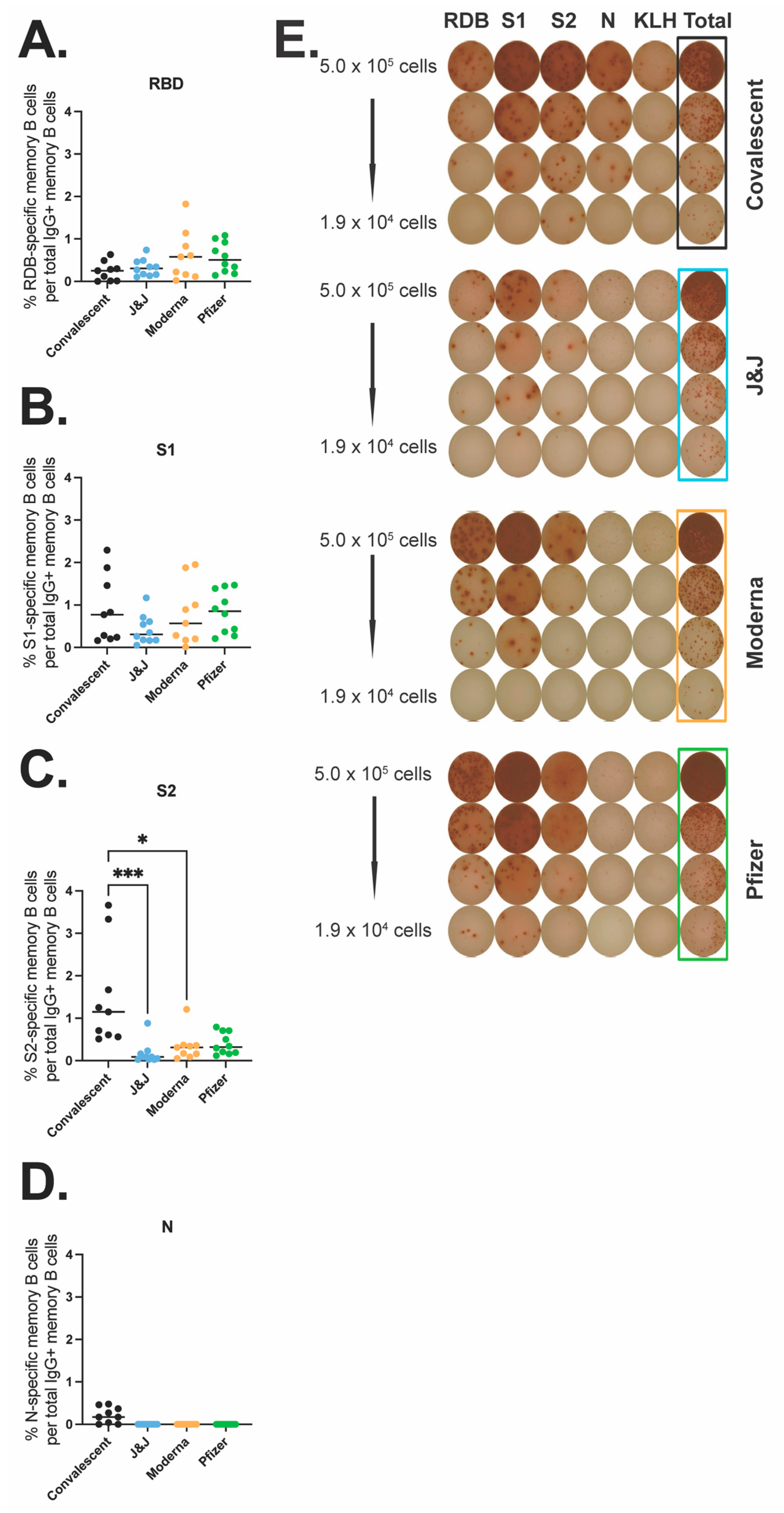
3.4. Spike- and N-Specific Memory B Cell Responses in Vaccinated and Convalescent Participants
3.5. Antibody Responses against Variants of Concern (VOC) in Vaccinated and Convalescent Participants
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 15 November 2022).
- WHO. COVID-19 Vaccine Tracker and Landscape. Available online: https://medbox.org/document/covid-19-vaccine-tracker-and-landscape#GO (accessed on 15 November 2022).
- WHO. COVID-19 Advice for the Public: Getting Vaccinated. Available online: https://heartcenter.kz/en/patients-visitors/covid-19/covid-19-advice-for-the-public-getting-vaccinated/ (accessed on 15 November 2022).
- FDA. Pfizer-BioNTech COVID-19 Vaccines. Available online: https://www.pfizer.com/products/product-detail/pfizer-biontech-covid-19-vaccine (accessed on 15 November 2022).
- FDA. Moderna COVID-19 Vaccines. Available online: https://www.cdc.gov/vaccines/covid-19/info-by-product/moderna/index.html (accessed on 15 November 2022).
- FDA. Janssen COVID-19 Vaccine. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/janssen-covid-19-vaccine (accessed on 15 November 2022).
- FDA. Novavax COVID-19 Vaccine, Adjuvanted. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/novavax-covid-19-vaccine-adjuvanted (accessed on 15 November 2022).
- CDC. Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Approved or Authorized in the United States. Available online: https://www.cdc.gov/vaccines/covid-19/clinical-considerations/covid-19-vaccines-us.html (accessed on 15 November 2022).
- El Sahly, H.M.; Baden, L.R.; Essink, B.; Doblecki-Lewis, S.; Martin, J.M.; Anderson, E.J.; Campbell, T.B.; Clark, J.; Jackson, L.A.; Fichtenbaum, C.J.; et al. Efficacy of the mRNA-1273 SARS-CoV-2 Vaccine at Completion of Blinded Phase. N. Engl. J. Med. 2021, 385, 1774–1785. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Van Dromme, I.; Spiessens, B.; et al. Final Analysis of Efficacy and Safety of Single-Dose Ad26.COV2.S. N. Engl. J. Med. 2022, 386, 847–860. [Google Scholar] [CrossRef]
- Huang, Y.; Yang, C.; Xu, X.-F.; Xu, W.; Liu, S.-W. Structural and functional properties of SARS-CoV-2 spike protein: Potential antivirus drug development for COVID-19. Acta Pharmacol. Sin. 2020, 41, 1141–1149. [Google Scholar] [CrossRef]
- Jackson, C.B.; Farzan, M.; Chen, B.; Choe, H. Mechanisms of SARS-CoV-2 entry into cells. Nat. Rev. Mol. Cell Biol. 2022, 23, 3–20. [Google Scholar] [CrossRef]
- Altarawneh, H.N.; Chemaitelly, H.; Hasan, M.R.; Ayoub, H.H.; Qassim, S.; AlMukdad, S.; Coyle, P.; Yassine, H.M.; Al-Khatib, H.A.; Benslimane, F.M.; et al. Protection against the Omicron Variant from Previous SARS-CoV-2 Infection. N. Engl. J. Med. 2022, 386, 1288–1290. [Google Scholar] [CrossRef]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 Covid-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus Pandemic (COVID-19). Our World in Data. 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 15 November 2022).
- Samanovic, M.I.; Cornelius, A.R.; Gray-Gaillard, S.L.; Allen, J.R.; Karmacharya, T.; Wilson, J.P.; Hyman, S.W.; Tuen, M.; Koralov, S.B.; Mulligan, M.J.; et al. Robust immune responses are observed after one dose of BNT162b2 mRNA vaccine dose in SARS-CoV-2–experienced individuals. Sci. Transl. Med. 2022, 14, eabi8961. [Google Scholar] [CrossRef]
- Assadiasl, S.; Fatahi, Y.; Zavvar, M.; Nicknam, M.H. COVID-19: Significance of antibodies. Hum. Antibodies 2020, 28, 287–297. [Google Scholar] [CrossRef]
- Young, C.; Brink, R. The unique biology of germinal center B cells. Immunity 2021, 54, 1652–1664. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, L.A.; de Góis Filho, P.G.; Silva, A.M.F.; Santos, J.V.G.; Santos, D.S.; Aquino, M.M.; de Jesus, R.M.; Almeida, M.L.D.; da Silva, J.S.; Altmann, D.M.; et al. Recurrent COVID-19 including evidence of reinfection and enhanced severity in thirty Brazilian healthcare workers. J. Infect. 2021, 82, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Ren, X.; Zhou, J.; Guo, J.; Hao, C.; Zheng, M.; Zhang, R.; Huang, Q.; Yao, X.; Li, R.; Jin, Y. Reinfection in patients with COVID-19: A systematic review. Glob. Health Res. Policy 2022, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Toro-Huamanchumo, C.J.; Hilario-Gomez, M.M.; Pinedo-Castillo, L.; Zumarán-Nuñez, C.J.; Espinoza-Gonzales, F.; Caballero-Alvarado, J.; Rodriguez-Morales, A.J.; Barboza, J.J. Clinical and epidemiological features of patients with COVID-19 reinfection: A systematic review. New Microbes New Infect. 2022, 48, 101021. [Google Scholar] [CrossRef]
- Steensels, D.; Pierlet, N.; Penders, J.; Mesotten, D.; Heylen, L. Comparison of SARS-CoV-2 Antibody Response Following Vaccination with BNT162b2 and mRNA-1273. JAMA 2021, 326, 1533. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Malcangi, G.; Ceci, S.; Patano, A.; Corriero, A.; Azzollini, D.; Marinelli, G.; Coloccia, G.; Piras, F.; Barile, G.; et al. Antispike Immunoglobulin-G (IgG) Titer Response of SARS-CoV-2 mRNA-Vaccine (BNT162b2): A Monitoring Study on Healthcare Workers. Biomedicines 2022, 10, 2402. [Google Scholar] [CrossRef] [PubMed]
- Lagousi, T.; Routsias, J.; Mavrouli, M.; Papadatou, I.; Geropeppa, M.; Spoulou, V. Comparative Characterization of Human Antibody Response Induced by BNT162b2 Vaccination vs. SARS-CoV-2 Wild-Type Infection. Vaccines 2022, 10, 1210. [Google Scholar] [CrossRef]
- Barbeau, D.J.; Martin, J.M.; Carney, E.; Dougherty, E.; Doyle, J.D.; Dermody, T.S.; Hoberman, A.; Williams, J.V.; Michaels, M.G.; Alcorn, J.F.; et al. Comparative analysis of human immune responses following SARS-CoV-2 vaccination with BNT162b2, mRNA-1273, or Ad26.COV2.S. npj Vaccines 2022, 7, 77. [Google Scholar] [CrossRef]
- Israel, A.; Shenhar, Y.; Green, I.; Merzon, E.; Golan-Cohen, A.; Schäffer, A.A.; Ruppin, E.; Vinker, S.; Magen, E. Large-Scale Study of Antibody Titer Decay following BNT162b2 mRNA Vaccine or SARS-CoV-2 Infection. Vaccines 2021, 10, 64. [Google Scholar] [CrossRef]
- Iyer, A.S.; Jones, F.K.; Nodoushani, A.; Kelly, M.; Becker, M.; Slater, D.; Mills, R.; Teng, E.; Kamruzzaman, M.; Garcia-Beltran, W.F.; et al. Persistence and decay of human antibody responses to the receptor binding domain of SARS-CoV-2 spike protein in COVID-19 patients. Sci. Immunol. 2020, 5. [Google Scholar] [CrossRef]
- Sette, A.; Crotty, S. Immunological memory to SARS-CoV -2 infection and COVID-19 vaccines. Immunol. Rev. 2022, 310, 27–46. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Doyle, J.; Barbeau, D.; Le Sage, V.; Wells, A.; Duprex, W.; Shurin, M.; Wheeler, S.; McElroy, A. A Cross-Sectional Study of SARS-CoV-2 Seroprevalence between Fall 2020 and February 2021 in Allegheny County, Western Pennsylvania, USA. Pathogens 2021, 10, 710. [Google Scholar] [CrossRef] [PubMed]
- Zacks, N.; Bar-Shai, A.; Levi, H.; Breslavsky, A.; Maayan, S.; Evgenia, T.; Feitelovich, S.; Wand, O.; Schaffer, M.; Sherer, Y.; et al. Assessment of Predictors for SARS-CoV-2 Antibodies Decline Rate in Health Care Workers after BNT162b2 Vaccination—Results from a Serological Survey. Vaccines 2022, 10, 1443. [Google Scholar] [CrossRef] [PubMed]
- Naranbhai, V.; Garcia-Beltran, W.F.; Chang, C.C.; Mairena, C.B.; Thierauf, J.C.; Kirkpatrick, G.; Onozato, M.L.; Cheng, J.; Denis, K.J.S.; Lam, E.C.; et al. Comparative Immunogenicity and Effectiveness of mRNA-1273, BNT162b2, and Ad26.COV2.S COVID-19 Vaccines. J. Infect. Dis. 2021, 225, 1141–1150. [Google Scholar] [CrossRef]
- Barouch, D.H.; Stephenson, K.E.; Sadoff, J.; Yu, J.; Chang, A.; Gebre, M.; McMahan, K.; Liu, J.; Chandrashekar, A.; Patel, S.; et al. Durable Humoral and Cellular Immune Responses 8 Months after Ad26.COV2.S Vaccination. N. Engl. J. Med. 2021, 385, 951–953. [Google Scholar] [CrossRef] [PubMed]
- Jacot, D.; von Rotz, U.; Pellaton, C.; Blondet, F.; Aebischer, O.; Perreau, M.; De Rham, M.; Pantaleo, G.; Marchetti, O.; Greub, G. SARS-CoV-2 neutralizing antibody response in vaccinated and non-vaccinated hospital healthcare workers with or without history of infection. Microbes Infect. 2022, 25, 105077. [Google Scholar] [CrossRef]
- Cho, A.; Muecksch, F.; Schaefer-Babajew, D.; Wang, Z.; Finkin, S.; Gaebler, C.; Ramos, V.; Cipolla, M.; Mendoza, P.; Agudelo, M.; et al. Anti-SARS-CoV-2 receptor-binding domain antibody evolution after mRNA vaccination. Nature 2021, 600, 517–522. [Google Scholar] [CrossRef]
- Goel, R.R.; Painter, M.M.; Apostolidis, S.A.; Mathew, D.; Meng, W.; Rosenfeld, A.M.; Lundgreen, K.A.; Reynaldi, A.; Khoury, D.S.; Pattekar, A.; et al. mRNA vaccines induce durable immune memory to SARS-CoV-2 and variants of concern. Science 2021, 374, abm0829. [Google Scholar] [CrossRef]
- Sokal, A.; Barba-Spaeth, G.; Fernández, I.; Broketa, M.; Azzaoui, I.; de La Selle, A.; Vandenberghe, A.; Fourati, S.; Roeser, A.; Meola, A.; et al. mRNA vaccination of naive and COVID-19-recovered individuals elicits potent memory B cells that recognize SARS-CoV-2 variants. Immunity 2021, 54, 2893–2907.e5. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Convalescents | J&J | Moderna | Pfizer- BioNTech |
|---|---|---|---|---|
| n = 21 | n = 20 | n = 28 | n = 47 | |
| Sex-no. (%) | ||||
| Female | 10 (48%) | 16 (80%) | 22 (79%) | 28 (60%) |
| Male | 11 (52%) | 4 (20%) | 6 (21%) | 19 (40%) |
| Age-yr. | 41.1 ± 11.2 | 36.3 ± 12.5 | 34.3 ± 9.8 | 38.7 ± 9.8 |
| Race or ethnic group-no. (%) 1 | ||||
| White | 15 (71%) | 16 (80%) | 19 (68%) | 22 (47%) |
| Asian | 3 (14%) | 1 (5%) | 3 (11%) | 20 (43%) |
| Black or African-American | 0 (0%) | 1 (5%) | 1 (4%) | 3 (6%) |
| Native | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Other | 3 (14%) | 2 (10%) | 5 (18%) | 2 (4%) |
| Hispanic or Latino-no. (%) | 2 (10%) | 0 (0%) | 4 (14%) | 5 (11%) |
| Plus-minus values are median ± SD | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samanovic, M.I.; Oom, A.L.; Cornelius, A.R.; Gray-Gaillard, S.L.; Karmacharya, T.; Tuen, M.; Wilson, J.P.; Tasissa, M.F.; Goins, S.; Herati, R.S.; et al. Vaccine-Acquired SARS-CoV-2 Immunity versus Infection-Acquired Immunity: A Comparison of Three COVID-19 Vaccines. Vaccines 2022, 10, 2152. https://doi.org/10.3390/vaccines10122152
Samanovic MI, Oom AL, Cornelius AR, Gray-Gaillard SL, Karmacharya T, Tuen M, Wilson JP, Tasissa MF, Goins S, Herati RS, et al. Vaccine-Acquired SARS-CoV-2 Immunity versus Infection-Acquired Immunity: A Comparison of Three COVID-19 Vaccines. Vaccines. 2022; 10(12):2152. https://doi.org/10.3390/vaccines10122152
Chicago/Turabian StyleSamanovic, Marie I., Aaron L. Oom, Amber R. Cornelius, Sophie L. Gray-Gaillard, Trishala Karmacharya, Michael Tuen, Jimmy P. Wilson, Meron F. Tasissa, Shelby Goins, Ramin Sedaghat Herati, and et al. 2022. "Vaccine-Acquired SARS-CoV-2 Immunity versus Infection-Acquired Immunity: A Comparison of Three COVID-19 Vaccines" Vaccines 10, no. 12: 2152. https://doi.org/10.3390/vaccines10122152
APA StyleSamanovic, M. I., Oom, A. L., Cornelius, A. R., Gray-Gaillard, S. L., Karmacharya, T., Tuen, M., Wilson, J. P., Tasissa, M. F., Goins, S., Herati, R. S., & Mulligan, M. J. (2022). Vaccine-Acquired SARS-CoV-2 Immunity versus Infection-Acquired Immunity: A Comparison of Three COVID-19 Vaccines. Vaccines, 10(12), 2152. https://doi.org/10.3390/vaccines10122152