
Factors That Impact Acceptance of COVID-19 Vaccination in Different Community-Dwelling Populations in China

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Study Sites
2.3. Sampling
2.4. Data Collection
2.4.1. Face-to-Face Survey
2.4.2. Online Survey
2.4.3. Statistical Analysis
3. Results
3.1. Face-to-Face Survey
3.1.1. Demographic Characteristics
3.1.2. Vaccine Acceptance in the Community
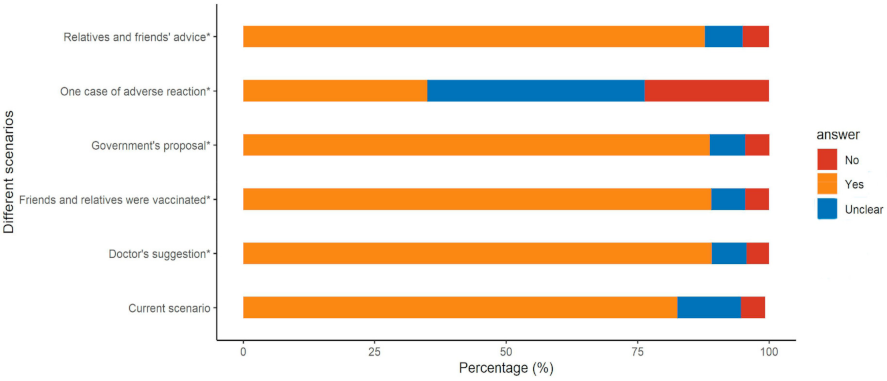
3.1.3. Methods to Improve Acceptance of Vaccination
3.2. Online Survey
3.2.1. Demographic Characteristics
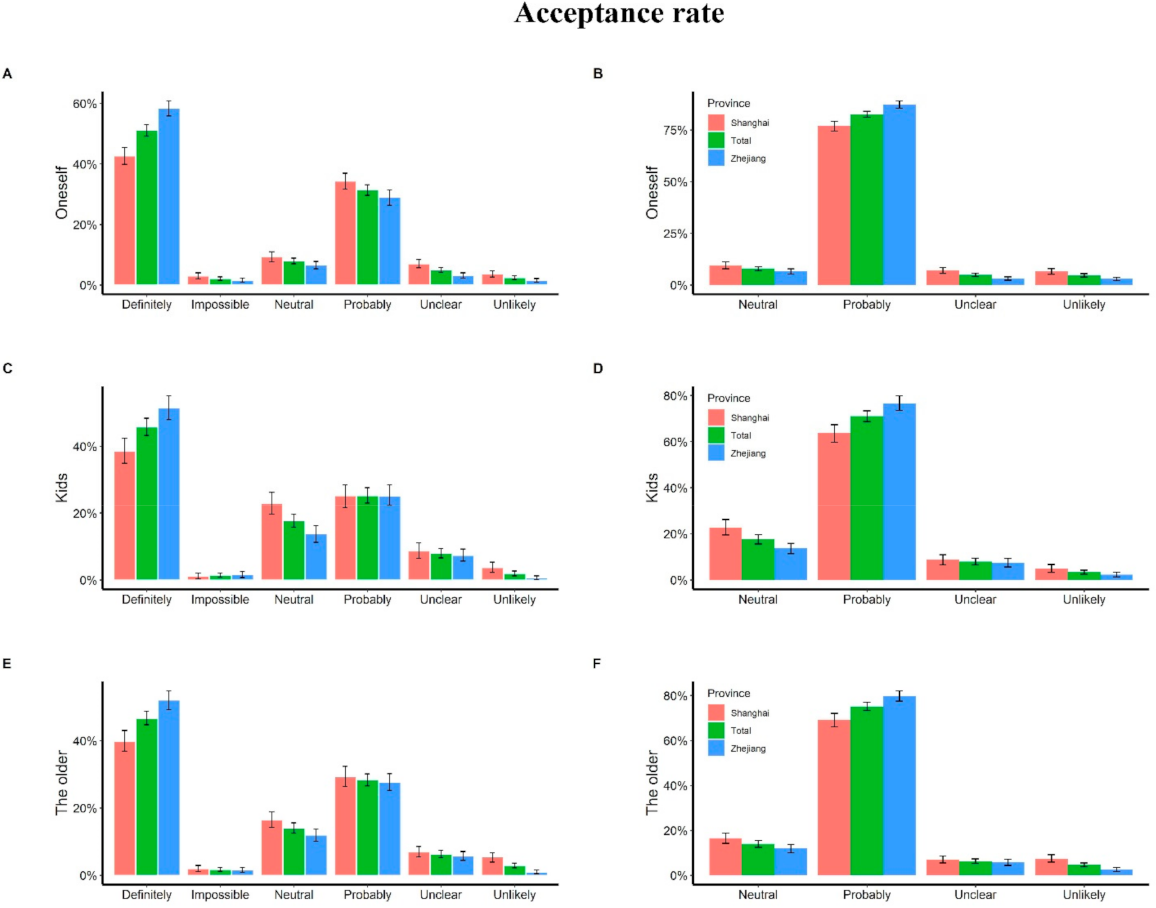
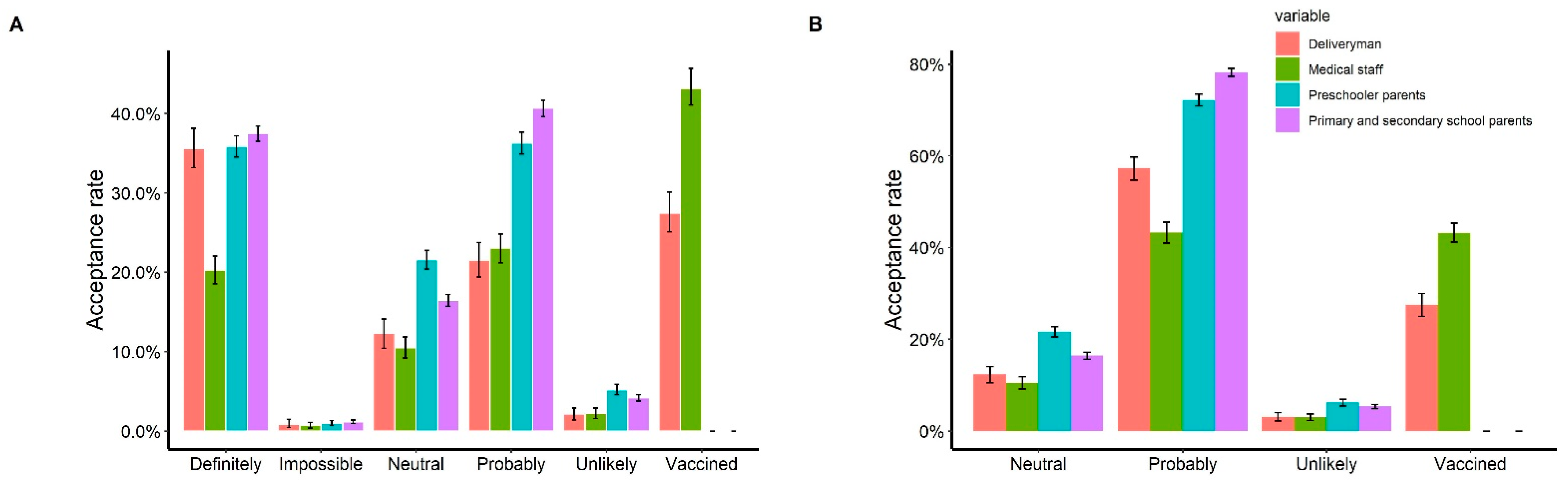
3.2.2. Vaccine Acceptance in the Four Key Populations
4. Discussion
4.1. Face-to-Face Survey
4.2. Online Survey
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yao, Y.; Pan, J.; Wang, W.; Liu, Z.; Kan, H.; Qiu, Y.; Meng, X.; Wang, W. Association of particulate matter pollution and case fatality rate of COVID-19 in 49 Chinese cities. Sci. Total Environ. 2020, 741, 140396. [Google Scholar] [CrossRef]
- Yao, Y.; Pan, J.; Liu, Z.; Meng, X.; Wang, W.; Kan, H.; Wang, W. No association of COVID-19 transmission with temperature or UV radiation in Chinese cities. Eur. Respir. J. 2020, 55, 2000517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, Y.; Pan, J.; Liu, Z.; Meng, X.; Wang, W.; Kan, H.; Wang, W. Ambient nitrogen dioxide pollution and spreadability of COVID-19 in Chinese cities. Ecotoxicol. Environ. Saf. 2021, 208, 111421. [Google Scholar] [CrossRef]
- Alqudeimat, Y.; Alenezi, D.; Al Hajri, B.; Alfouzan, H.; Almokhaizeem, Z.; Altamimi, S.; Almansouri, W.; Alzalzalah, S.; Ziyab, A.H. Acceptance of a COVID-19 Vaccine and Its Related Determinants among the General Adult Population in Kuwait. Med. Princ. Pract. 2021, 30, 262–271. [Google Scholar] [CrossRef]
- Devi, S. COVID-19 resurgence in Iran. Lancet 2020, 395, 1896. [Google Scholar] [CrossRef]
- Shimizu, K.; Wharton, G.; Sakamoto, H.; Mossialos, E. Resurgence of COVID-19 in Japan. BMJ 2020, 370, 3221. [Google Scholar] [CrossRef]
- Brussow, H. COVID-19: Vaccine’s progress. Microb. Biotechnol. 2021, 14, 1246–1257. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in Southeast Asia: A Cross-Sectional Study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020, 27, 225–228. [Google Scholar] [CrossRef]
- Gan, L.; Chen, Y.; Hu, P.; Wu, D.; Zhu, Y.; Tan, J.; Li, Y.; Zhang, D. Willingness to Receive SARS-CoV-2 Vaccination and Associated Factors among Chinese Adults: A Cross Sectional Survey. Int. J. Environ. Res. Public Health 2021, 18, 1993. [Google Scholar] [CrossRef]
- Harapan, H.; Anwar, S.; Setiawan, A.M.; Sasmono, R.T. Dengue vaccine acceptance and associated factors in Indonesia: A community-based cross-sectional survey in Aceh. Vaccine 2016, 34, 3670–3675. [Google Scholar] [CrossRef]
- Hadisoemarto, P.F.; Castro, M.C. Public acceptance and willingness-to-pay for a future dengue vaccine: A communi-ty-based survey in Bandung, Indonesia. PLoS Negl. Trop. Dis. 2013, 7, e2427. [Google Scholar] [CrossRef] [Green Version]
- Kruiroongroj, S.; Chaikledkaew, U.; Thavorncharoensap, M. Knowledge, Acceptance, and Willingness to Pay for Human Papilloma Virus (HPV) Vaccination among Female Parents in Thailand. Asian Pac. J. Cancer Prev. 2014, 15, 5469–5474. [Google Scholar] [CrossRef] [Green Version]
- Ughasoro, M.D.; Esangbedo, D.O.; Tagbo, B.N.; Mejeha, I.C. Acceptability and Willingness-to-Pay for a Hypothetical Ebola Virus Vaccine in Nigeria. PLoS Negl. Trop. Dis. 2015, 9, e0003838. [Google Scholar] [CrossRef] [Green Version]
- Zhong, B.-L.; Luo, W.; Li, H.-M.; Zhang, Q.-Q.; Liu, X.-G.; Li, W.-T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Biol. Sci. 2020, 16, 1745–1752. [Google Scholar] [CrossRef]
- Muslih, M.; Susanti, H.; Rias, Y.; Chung, M.-H. Knowledge, Attitude, and Practice of Indonesian Residents toward COVID-19: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2021, 18, 4473. [Google Scholar] [CrossRef]
- Kasemy, Z.A.; Bahbah, W.A.; Zewain, S.K.; Haggag, M.G.; Alkalash, S.H.; Zahran, E.; Desouky, D.E. Knowledge, Attitude and Practice toward COVID-19 among Egyptians. J. Epidemiol. Glob. Health 2020, 10, 378–385. [Google Scholar] [CrossRef]
- Addis, S.G.; Nega, A.D.; Miretu, D.G. Knowledge, attitude and practice of patients with chronic diseases towards COVID-19 pandemic in Dessie town hospitals, Northeast Ethiopia. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 847–856. [Google Scholar] [CrossRef]
- Galbadage, T.; Peterson, B.M.; Awada, J.; Buck, A.S.; Ramirez, D.A.; Wilson, J.; Gunasekera, R.S. Systematic Review and Meta-Analysis of Sex-Specific COVID-19 Clinical Outcomes. Front. Med. 2020, 7, 348. [Google Scholar] [CrossRef]
- Verger, P.; Scronias, D.; Dauby, N.; Adedzi, K.A.; Gobert, C.; Bergeat, M.; Gagneur, A.; Dubé, E. Attitudes of healthcare workers towards COVID-19 vaccination: A survey in France and French-speaking parts of Belgium and Canada, 2020. Eurosurveillance 2021, 26, 2002047. [Google Scholar] [CrossRef]
- Lucia, V.C.; Kelekar, A.; Afonso, N.M. COVID-19 vaccine hesitancy among medical students. J. Public Health 2021, 43, 445–449. [Google Scholar] [CrossRef]
- Shaw, J.; Stewart, T.; Anderson, K.B.; Hanley, S.; Thomas, S.J.; Salmon, D.A.; Morley, C. Assessment of U.S. health care personnel (HCP) attitudes towards COVID-19 vaccination in a large university health care system. Clin. Infect. Dis. 2021, 2021, ciab054. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Community Residents | Deliverymen | Health Workers | Parents of Preschoolers | Parents of School Students * | |
|---|---|---|---|---|---|
| n = 2769 | n = 1335 | n = 2001 | n = 4847 | n = 9017 | |
| Age (mean (SD)) | 45.95 (19.29) | 31.52 (7.45) | 34.70 (9.46) | 4.61 (1.51) | 11.21 (3.55) |
| Province (%) | |||||
| Zhejiang | 1283 (46.3) | 317 (23.7) | 534 (26.7) | 2127 (43.9) | 1206 (13.4) |
| Qinghai | 1486 (53.7) | 68 (5.1) | 779 (38.9) | 1996 (41.2) | 7251 (80.4) |
| Shanghai | 950 (71.2) | 688 (34.4) | 724 (14.9) | 560 (6.2) | |
| Sex (%) | |||||
| Female | 1483 (53.6) | 232 (17.3) | 1539 (76.9) | 2305 (47.5) | 4341 (48.1) |
| Education (%) | |||||
| Low | 1390 (50.2) | 520 (39.0) | 35 (1.7) | N/A | N/A |
| Median | 542 (19.6) | 558 (41.8) | 156 (7.8) | N/A | N/A |
| High | 755 (27.3) | 257 (19.0) | 1810 (90.5) | N/A | N/A |
| Income (thousand CNY, %) | |||||
| <10 | 574 (20.7) | 545 (40.8) | 376 (18.8) | 959 (19.8) | 3490 (38.7) |
| 10–30 | 587 (21.2) | 192 (14.4) | 277 (13.8) | 759 (15.7) | 2065 (22.9) |
| 30–50 | 648 (23.4) | 239 (17.9) | 266 (13.3) | 746 (15.4) | 1472 (16.3) |
| 50–100 | 711 (25.7) | 288 (21.6) | 544 (27.2) | 1096 (22.6) | 1165 (12.9) |
| 100–200 | 195 (7.0) | 59 (4.4) | 456 (22.8) | 781 (16.1) | 530 (5.9) |
| >200 | 54 (2.0) | 12 (0.9) | 82 (4.1) | 506 (10.4) | 295 (3.3) |
| Univariate Logistic Model | Multivariate Logistic Model | |||
|---|---|---|---|---|
| Adjusted OR (95% CI) | Crude OR (95% CI) | Adjusted OR (95% CI) | Crude OR (95% CI) | |
| Sex: female vs. male | 1.48 (1.12, 1.96) † | 1.56 (1.28, 1.91) † | 1.49 (1.12, 1.98) † | 1.55 (1.27, 1.90) † |
| Age | ||||
| 30–39 vs. <30 | 0.77 (0.48, 1.23) | 0.84 (0.61, 1.16) | 0.76 (0.47, 1.22) | 0.86 (0.62, 1.18) |
| 40–49 vs. <30 | 0.82 (0.49, 1.35) | 0.72 (0.51, 1.00) | 0.78 (0.47, 1.30) | 0.80 (0.57, 1.12) |
| 50–59 vs. <30 | 0.88 (0.53, 1.48) | 0.60 (0.43, 0.84) † | 0.83 (0.49, 1.40) | 0.66 (0.47, 0.92) † |
| 60–69 vs. <30 | 0.58 (0.32, 1.02) | 0.78 (0.56, 1.08) | 0.52 (0.29, 0.92) * | 0.75 (0.54, 1.05) |
| >69 vs. <30 | 0.66 (0.38, 1.15) | 0.78 (0.57, 1.05) | 0.63 (0.36, 1.11) | 0.78 (0.58, 1.06) |
| Region: rural vs. urban | 0.59 (0.44, 0.79) † | 0.57 (0.47, 0.70) † | 0.87 (0.58, 1.3) | 0.91 (0.67, 1.25) |
| Overseas experience Last month | 15.6 (2.51, 127.66) † | 2.16 (0.68, 5.98) | 14.66 (2.25, 95.41) † | 1.74 (0.60, 5.07) |
| Education | ||||
| Medium vs. low | 1.64 (1.13, 2.38) † | 1.41 (1.09, 1.8) † | 1.5 (1.05, 2.23) * | 1.19 (0.92, 1.54) |
| High vs. low | 1.13 (0.74, 1.71) | 1.20 (0.95, 1.51) | 1.07 (0.7, 1.62) | 1.02 (0.80, 1.29) |
| Marriage: others vs. married | 1.19 (0.84, 1.69) | 1.50 (1.19, 1.88) † | 1.13 (0.79, 1.62) | 1.39 (1.10, 1.75) † |
| Employment: unemployed vs. employed | 1.15 (0.81, 1.65) | 1.13 (0.91, 1.39) | 1.09 (0.76, 1.56) | 0.97 (0.78, 1.21) |
| Quarantined: yes vs. no | 0.24 (0.08, 0.58) † | 0.81 (0.44, 1.40) | 0.25 (0.09, 0.64) † | 0.86 (0.48, 1.53) |
| Health | ||||
| Good vs. low | 0.35 (0.15, 0.88) * | 0.43 (0.24, 0.79) † | 0.36 (0.15, 0.88) * | 0.46 (0.25, 0.82) † |
| Medium vs. low | 0.42 (0.17, 1.07) | 0.53 (0.29, 0.99) * | 0.41 (0.16, 1.01) | 0.50 (0.27, 0.94) * |
| Preference of imported or domestic vaccines | ||||
| Both fine vs. domestic | 1.12 (0.80, 1.55) | 1.48 (1.15, 1.9) † | 1.09 (0.78, 1.52) | 1.43 (1.11, 1.85) † |
| Imported vs. domestic | 1.52 (0.92, 2.43) | 1.6 (1.07, 2.34) * | 1.5 (0.92, 2.43) | 1.71 (1.15, 2.53) † |
| Unclear vs. domestic | 7.52 (4.99, 11.37) † | 9.65 (7.05, 13.29) † | 7.68 (5.08, 11.61) † | 10.22 (7.39, 14.13) † |
| Behavior | 0.74 (0.61, 0.91) † | 0.65 (0.57, 0.73) † | 0.73 (0.60, 0.90) † | 0.65 (0.57, 0.74) † |
| Attitude | 0.14 (0.10, 0.19) † | 0.10 (0.08, 0.13) † | 0.14 (0.10, 0.20) † | 0.10 (0.08, 0.13) † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, J.; A, K.; Liu, Z.; Zhang, P.; Xu, Z.; Guo, X.; Liu, G.; Xu, A.; Wang, J.; Wang, X.; et al. Factors That Impact Acceptance of COVID-19 Vaccination in Different Community-Dwelling Populations in China. Vaccines 2022, 10, 91. https://doi.org/10.3390/vaccines10010091
Pan J, A K, Liu Z, Zhang P, Xu Z, Guo X, Liu G, Xu A, Wang J, Wang X, et al. Factors That Impact Acceptance of COVID-19 Vaccination in Different Community-Dwelling Populations in China. Vaccines. 2022; 10(1):91. https://doi.org/10.3390/vaccines10010091
Chicago/Turabian StylePan, Jinhua, Kezhong A, Zhixi Liu, Peng Zhang, Zhiyin Xu, Xiaoqin Guo, Guangtao Liu, Ao Xu, Jing Wang, Xinyu Wang, and et al. 2022. "Factors That Impact Acceptance of COVID-19 Vaccination in Different Community-Dwelling Populations in China" Vaccines 10, no. 1: 91. https://doi.org/10.3390/vaccines10010091
APA StylePan, J., A, K., Liu, Z., Zhang, P., Xu, Z., Guo, X., Liu, G., Xu, A., Wang, J., Wang, X., & Wang, W. (2022). Factors That Impact Acceptance of COVID-19 Vaccination in Different Community-Dwelling Populations in China. Vaccines, 10(1), 91. https://doi.org/10.3390/vaccines10010091