

Comparative Analysis of Redox Homeostasis Biomarkers in Patients with Psoriasis and Atopic Dermatitis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
2.3. Statistical Analysis
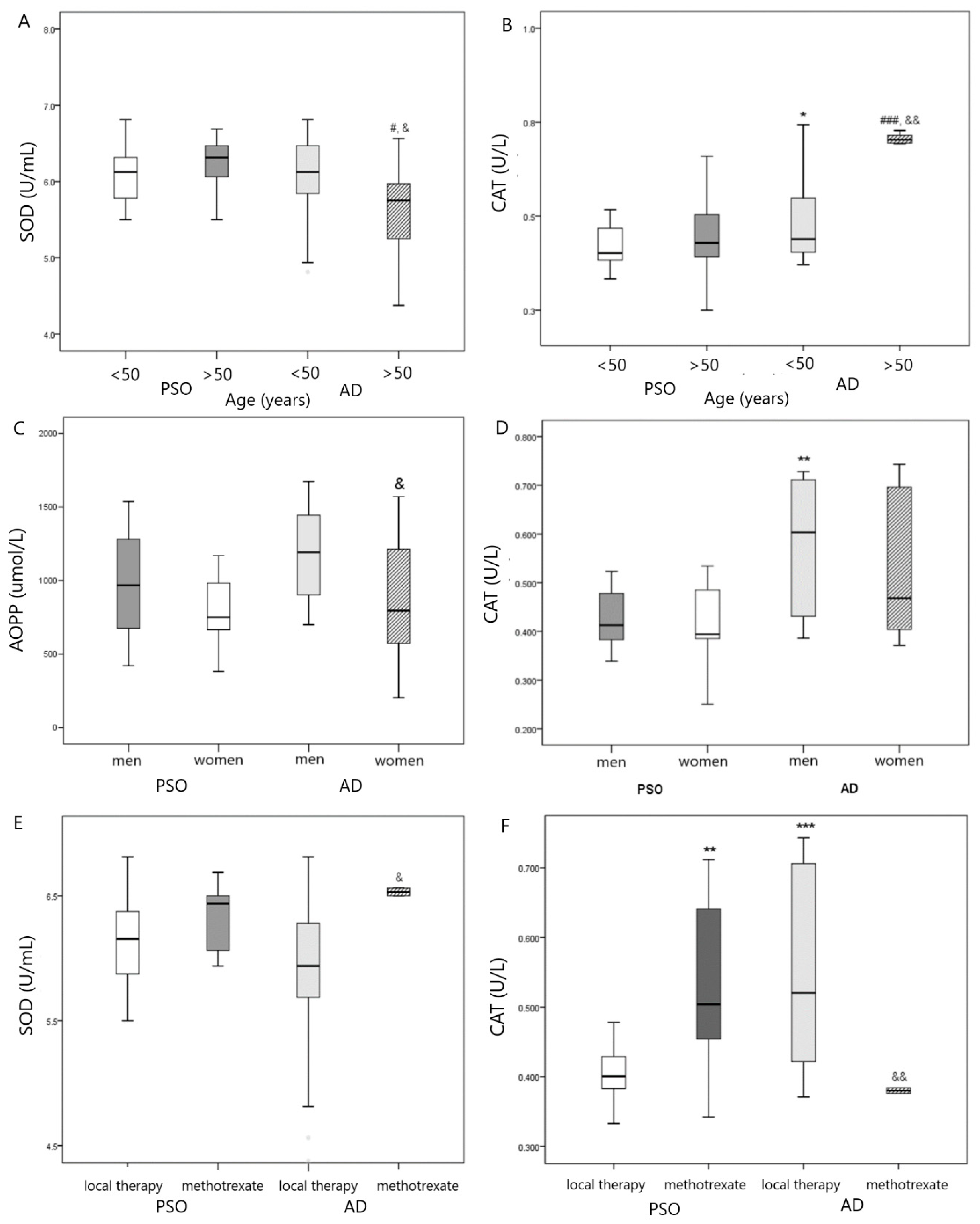
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Borgia, F.; Li Pomi, F.; Vaccaro, M.; Alessandrello, C.; Papa, V.; Gangemi, S. Oxidative Stress and Phototherapy in Atopic Dermatitis: Mechanisms, Role, and Future Perspectives. Biomolecules 2022, 12, 1904. [Google Scholar] [CrossRef] [PubMed]
- Guttman-Yassky, E.; Krueger, J.G.; Lebwohl, M.G. Systemic immune mechanisms in atopic dermatitis and psoriasis with implications for treatment. Exp. Dermatol. 2018, 27, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.; Guo, Y.; Chen, L.; Zhu, J.; Li, C. Crosstalk between cholesterol metabolism and psoriatic inflammation. Front. Immunol. 2023, 14, 1124786. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Yang, Y.; Liao, Y.; Shi, Y.; Zhang, L.J. Emerging Roles of Adipose Tissue in the Pathogenesis of Psoriasis and Atopic Dermatitis in Obesity. JID Innov. 2021, 2, 100064. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.Y.; Chen, S.C.; Hsu, S.Y.; Lin, Y.A.; Shih, C.M.; Huang, C.Y.; Wang, K.H.; Lee, A.W. Annoying Psoriasis and Atopic Dermatitis: A Narrative Review. Int. J. Mol. Sci. 2022, 23, 4898. [Google Scholar] [CrossRef] [PubMed]
- Dobrică, E.C.; Cozma, M.A.; Găman, M.A.; Voiculescu, V.M.; Găman, A.M. The Involvement of Oxidative Stress in Psoriasis: A Systematic Review. Antioxidants 2022, 11, 282. [Google Scholar] [CrossRef]
- Cannavò, S.P.; Riso, G.; Casciaro, M.; Di Salvo, E.; Gangemi, S. Oxidative stress involvement in psoriasis: A systematic review. Free Radic. Res. 2019, 53, 829–840. [Google Scholar] [CrossRef]
- Bakic, M.; Klisic, A.; Kocic, G.; Kocic, H.; Karanikolic, V. Oxidative stress and metabolic biomarkers in patients with psoriasis. J. Med. Biochem. 2023, 42, 1–9. [Google Scholar]
- Medovic, M.V.; Jakovljevic, V.L.; Zivkovic, V.I.; Jeremic, N.S.; Jeremic, J.N.; Bolevich, S.B.; Ravic Nikolic, A.B.; Milicic, V.M.; Srejovic, I.M. Psoriasis between Autoimmunity and Oxidative Stress: Changes Induced by Different Therapeutic Approaches. Oxid. Med. Cell. Longev. 2022, 2022, 2249834. [Google Scholar] [CrossRef]
- Balato, A.; Zink, A.; Babino, G.; Buononato, D.; Kiani, C.; Eyerich, K.; Ziehfreund, S.; Scala, E. The Impact of Psoriasis and Atopic Dermatitis on Quality of Life: A Literature Research on Biomarkers. Life 2022, 12, 2026. [Google Scholar] [CrossRef]
- Shimamoto, J.; Kurokawa, T.; Tanizaki, H.; Moriwaki, S. The evaluation of oxidative stress in patients with psoriasis vulgaris and atopic dermatitis by measuring the urinary level of 8-hydroxy2′-deoxyguanosine. J. Cutan. Immunol. Allergy 2019, 2, 163–168. [Google Scholar] [CrossRef]
- Chen, P.Y.; Chen, C.W.; Su, Y.J.; Chang, W.H.; Kao, W.F.; Yang, C.C.; Wang, I.J. Associations between Levels of Urinary Oxidative Stress of 8-OHdG and Risk of Atopic Diseases in Children. Int. J. Environ. Res. Public Health 2020, 17, 8207. [Google Scholar] [CrossRef] [PubMed]
- Bakic, M.; Klisic, A.; Karanikolic, V. Comparative study of hematological parameters and biomarkers of immunity and inflammation in patients with psoriasis and atopic dermatitis. Medicina 2023, 59, 1622. [Google Scholar] [CrossRef]
- Skoie, I.M.; Dalen, I.; Omdal, R.; Jonsson, G. Malondialdehyde and advanced oxidation protein products are not increased in psoriasis: A controlled study. Arch. Dermatol. Res. 2019, 311, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Andreeva, L.I.; Kozhemiakin, L.A.; Kishkun, A.A. Modification of the method of determining lipid peroxidation in a test using thiobarbituric acid. Lab. Delo. 1988, 11, 41–43. [Google Scholar]
- Yazici, C.; Köse, K.; Utaş, S.; Tanrikulu, E.; Taşlidere, N. A novel approach in psoriasis: First usage of known protein oxidation markers to prove oxidative stress. Arch. Dermatol. Res. 2016, 308, 207–212. [Google Scholar] [CrossRef]
- Witko-Sarsat, V.; Friedlander, M.; Capeillere-Blandin, C.; Nguyen-Khoa, T.; Nguyen, A.T.; Zingraff, J.; Jungers, P.; Descamps-Latscha, B. Advanced oxidation protein products as a novel marker of oxidative stress in uremia. Kidney Int. 1996, 49, 1304–1313. [Google Scholar] [CrossRef]
- Góth, L. A simple method for determination of serum catalase activity and revision of reference range. Clin. Chim. Acta 1991, 196, 143–151. [Google Scholar] [CrossRef]
- Misra, H.P.; Fridovich, I. The role of superoxide anion in the autooxidation of epinephrine and a simple assay for superoxide dismutase. J. Biol. Chem. 1972, 247, 3170–3175. [Google Scholar] [CrossRef]
- Schisterman, E.F.; Perkins, N.J.; Liu, A.; Bondell, H. Optimal cut-point and its corresponding Youden Index to discriminate individuals using pooled blood samples. Epidemiology 2005, 16, 73–81. [Google Scholar] [CrossRef]
- Klisic, A.; Kavaric, N.; Vujcic, S.; Spasojevic-Kalimanovska, V.; Kotur-Stevuljevic, J.; Ninic, A. Factorial analysis of the cardiometabolic risk influence on redox status components in adult population. Oxid. Med. Cell. Longev. 2021, 2021, 6661940. [Google Scholar] [CrossRef] [PubMed]
- Boehncke, W.H.; Boehncke, S.; Tobin, A.M.; Kirby, B. The ‘psoriatic march’: A concept of how severe psoriasis may drive cardiovascular comorbidity. Exp. Dermatol. 2011, 20, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Mohamed Haris, N.H.; Krishnasamy, S.; Chin, K.-Y.; Mariappan, V.; Arumugam, M. Metabolic Syndrome Screening and Nutritional Status of Patients with Psoriasis: A Scoping Review. Nutrients 2023, 15, 2707. [Google Scholar] [CrossRef] [PubMed]
- Heitmann, J.; Frings, V.G.; Geier, A.; Goebeler, M.; Kerstan, A. Non-alcoholic fatty liver disease and psoriasis—Is there a shared proinflammatory network? J. Dtsch. Dermatol. Ges. 2021, 19, 517–528. [Google Scholar] [CrossRef] [PubMed]
- Thyssen, J.P.; Halling, A.S.; Schmid-Grendelmeier, P.; Guttman-Yassky, E.; Silverberg, J.I. Comorbidities of atopic dermatitis-what does the evidence say? J. Allergy Clin. Immunol. 2023, 151, 1155–1162. [Google Scholar] [CrossRef]
- Egeberg, A.; Griffiths, C.E.M.; Williams, H.C.; Andersen, Y.M.F.; Thyssen, J.P. Clinical characteristics, symptoms and burden of psoriasis and atopic dermatitis in adults. Br. J. Dermatol. 2020, 183, 128–138. [Google Scholar] [CrossRef]
- Brunner, P.M.; Suárez-Fariñas, M.; He, H.; Malik, K.; Wen, H.C.; Gonzalez, J.; Chan, T.C.; Estrada, Y.; Zheng, X.; Khattri, S.; et al. The atopic dermatitis blood signature is characterized by increases in inflammatory and cardiovascular risk proteins. Sci. Rep. 2017, 7, 8707, Erratum in Sci. Rep. 2018, 8, 8439. [Google Scholar] [CrossRef]
- Galiniak, S.; Mołoń, M.; Biesiadecki, M.; Bożek, A.; Rachel, M. The Role of Oxidative Stress in Atopic Dermatitis and Chronic Urticaria. Antioxidants 2022, 11, 1590. [Google Scholar] [CrossRef]
- Klisic, A.; Isakovic, A.; Kocic, G.; Kavaric, N.; Jovanovic, M.; Zvrko, E.; Skerovic, V.; Ninic, A. Relationship between Oxidative Stress, Inflammation and Dyslipidemia with Fatty Liver Index in Patients with Type 2 Diabetes Mellitus. Exp. Clin. Endocrinol. Diabetes. 2018, 126, 371–378. [Google Scholar] [CrossRef]
- Piskin, G.; Heydendael, V.M.; de Rie, M.A.; Bos, J.D.; Teunissen, M.B. Cyclosporin A and methotrexate are equally effective in reducing T cell numbers in psoriatic skin lesions but have no consistent effect on IFN-gamma and IL-4 expression in psoriatic skin in situ. Arch. Dermatol. Res. 2003, 294, 559–562. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Parameter | PsO | AD | p |
|---|---|---|---|
| Sex | |||
| men, n (%) | 22 (55) | 18 (45) | 0.251 |
| women, n (%) | 18 (45) | 22 (55) | |
| Age (years) | 50 (39–67) | 42 (34–51) | 0.011 |
| BMI (kg/m2) | 27.0 (24.0–30.8) | 23.8 (21.7–25.0) | <0.001 |
| Smoking, n (%) | |||
| No | 22 (55) | 23 (58) | 0.500 |
| Yes | 18 (45) | 17 (42) | |
| Disease duration (years) | 8.0 (5.0–13.5) | 10 (5.0–17.5) | 0.284 |
| Intensity of itch | 6.0 (5.0–8.0) | 8.0 (7.5–9.0) | 0.004 |
| Therapy local, n (%) | 30 (75.0) | 38 (95.0) | 0.013 |
| Methotrexate, n (%) | 10 (25.0) | 2 (5%) | |
| Comorbidities | |||
| No | 19 (47.5) | 20 (50.0) | 0.500 |
| Yes | 21 (52.5) | 20 (50.0) | |
| Glucose (mmol/L) | 5.3 (4.9–5.9) | 5.2 (4.9–5.4) | 0.178 |
| TC (mmol/L) | 5.02 (4.39–6.12) | 4.60 (4.06–5.26) | 0.227 |
| HDL-c (mmol/L) | 1.37 (1.09–1.63) | 1.54 (1.22–1.63) | 0.233 |
| LDL-c (mmol/L) | 2.88 (2.14–3.62) | 2.47 (2.14–3.54) | 0.564 |
| TG (mmol/L) | 1.68 (0.93–2.34) | 1.13 (0.75–1.90) | 0.114 |
| MDA (μmol/L) | 4.00 (1.67–7.49) | 5.15 (2.85–8.62) | 0.146 |
| AOPP (μmol/L) | 909 (676–1035) | 1086 (724–1300) | 0.145 |
| SOD (U/mL) | 6.19 (5.94–6.44) | 6.00 (5.75–6.38) | 0.162 |
| CAT (U/L) | 0.412 (0.383–0.478) | 0.521 (0.420–0.706) | <0.001 |
| Comorbidity | PsO | AD | p |
|---|---|---|---|
| Without comorbidities, n (%) | 19 (48.7) | 20 (50.0) | 0.261 |
| Hypertension, n (%) | 6 (15.4) | 5 (12.5) | |
| Diabetes, n (%) | 3 (7.7) | 0 (0) | |
| Obesity, n (%) | 2 (5.1) | 4 (10.0) | |
| Asthma, n (%) | 1 (2.6) | 2 (5.0) | |
| Hypertension + asthma, n (%) | 1 (2.6) | 5 (12.5) | |
| Hypertension + diabetes, n (%) | 5 (12.8) | 4 (10.0) | |
| Hypertension + fatty liver disease, n (%) | 2 (5.1) | 0 (0) | |
| Hypertension (total *), n (%) | 14 (35) | 14 (35) | 0.129 |
| Diabetes (total), n (%) | 8 (20) | 4 (10) | |
| Asthma (total), n (%) | 2 (5) | 7 (17.5) |
| Parameter | Local Therapy n = 68 | METHOTREXATE n = 12 | p |
|---|---|---|---|
| SOD (U/mL) | 6.06 (5.75–6.34) | 6.50 (6.09–6.53) | 0.036 |
| CAT (U/L) | 0.43 (0.39–0.68) | 0.46 (0.41–0.59) | 0.848 |
| MDA (μmol/L) | 4.83 (2.60–8.64) | 4.33 (1.92–5.36) | 0.553 |
| AOPP (μmol/L) | 971 (681–1250) | 976 (761–1064) | 0.856 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klisic, A.; Bakic, M.; Karanikolic, V. Comparative Analysis of Redox Homeostasis Biomarkers in Patients with Psoriasis and Atopic Dermatitis. Antioxidants 2023, 12, 1875. https://doi.org/10.3390/antiox12101875
Klisic A, Bakic M, Karanikolic V. Comparative Analysis of Redox Homeostasis Biomarkers in Patients with Psoriasis and Atopic Dermatitis. Antioxidants. 2023; 12(10):1875. https://doi.org/10.3390/antiox12101875
Chicago/Turabian StyleKlisic, Aleksandra, Mirjana Bakic, and Vesna Karanikolic. 2023. "Comparative Analysis of Redox Homeostasis Biomarkers in Patients with Psoriasis and Atopic Dermatitis" Antioxidants 12, no. 10: 1875. https://doi.org/10.3390/antiox12101875
APA StyleKlisic, A., Bakic, M., & Karanikolic, V. (2023). Comparative Analysis of Redox Homeostasis Biomarkers in Patients with Psoriasis and Atopic Dermatitis. Antioxidants, 12(10), 1875. https://doi.org/10.3390/antiox12101875