

Single-Stage Endovascular Management of Concurrent Intracranial Aneurysms and Arterial Stenoses: Clinical Outcomes, Procedural Strategies, and Predictive Factors

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria Were
- •
- Age ≥ 18 years.
- •
- Confirmed ≥70% extracranial ICA or VA stenosis based on digital subtraction angiography (DSA), CTA, or MRA, evaluated using NASCET criteria.
- •
- At least one saccular or fusiform intracranial aneurysm identified via CTA or DSA.
- •
- Either symptomatic ischemia (e.g., TIA, infarct on DWI) or aneurysm-related symptoms (e.g., headache, SAH).
- •
- Available pre- and post-procedural imaging and clinical records.
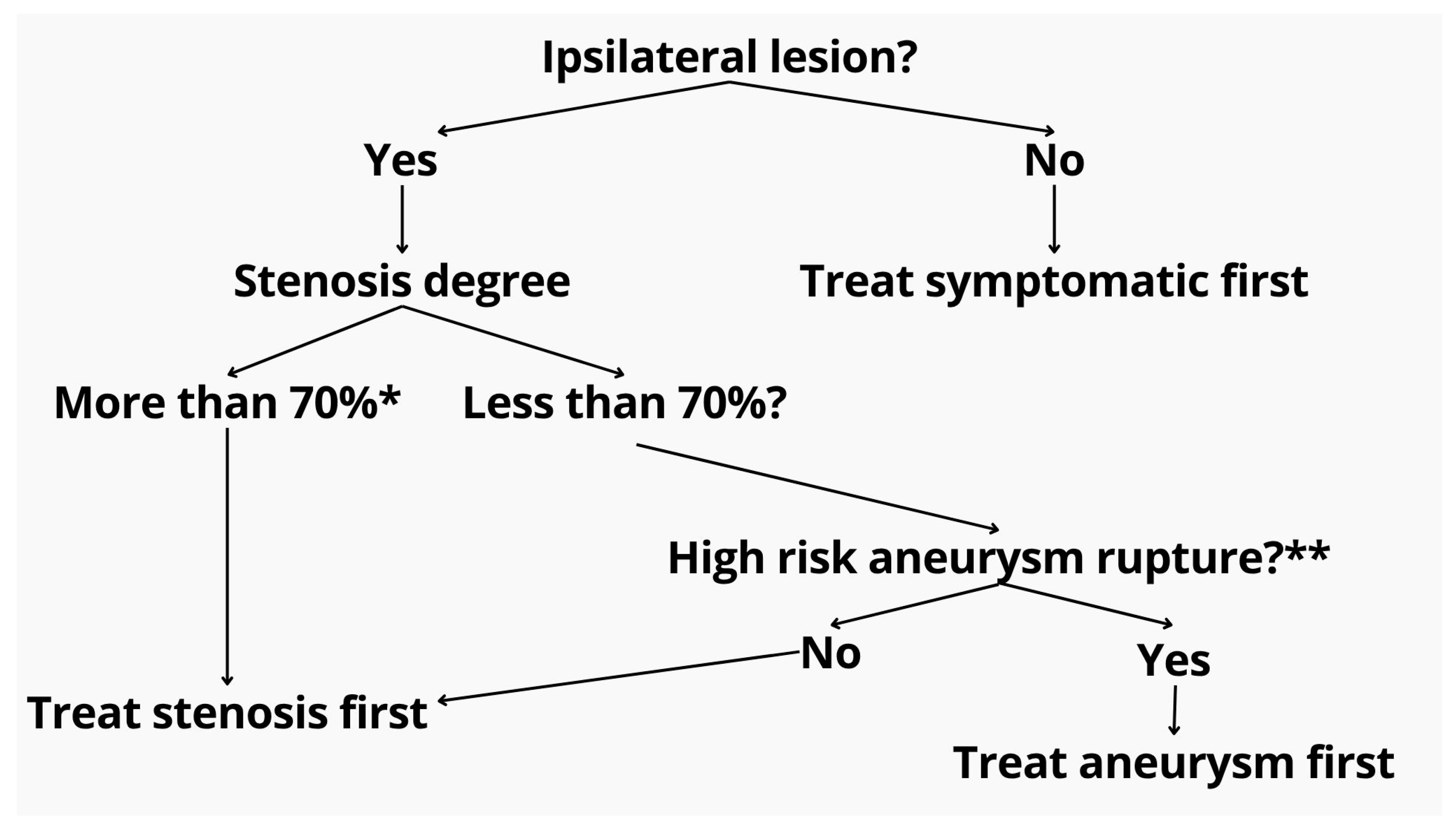
2.2. Imaging and Decision Protocol
2.3. Procedure
2.4. Periprocedural Management
2.5. Data Collection and Outcomes
2.6. Statistical Analysis
2.7. Ethics Statement
3. Results
3.1. Patient Characteristics and Vascular Lesion Profile
3.2. Risk Factors and Lesion Characteristics
3.3. Treatment Strategy
3.4. Functional Outcomes and Predictive Factors
3.5. Complications
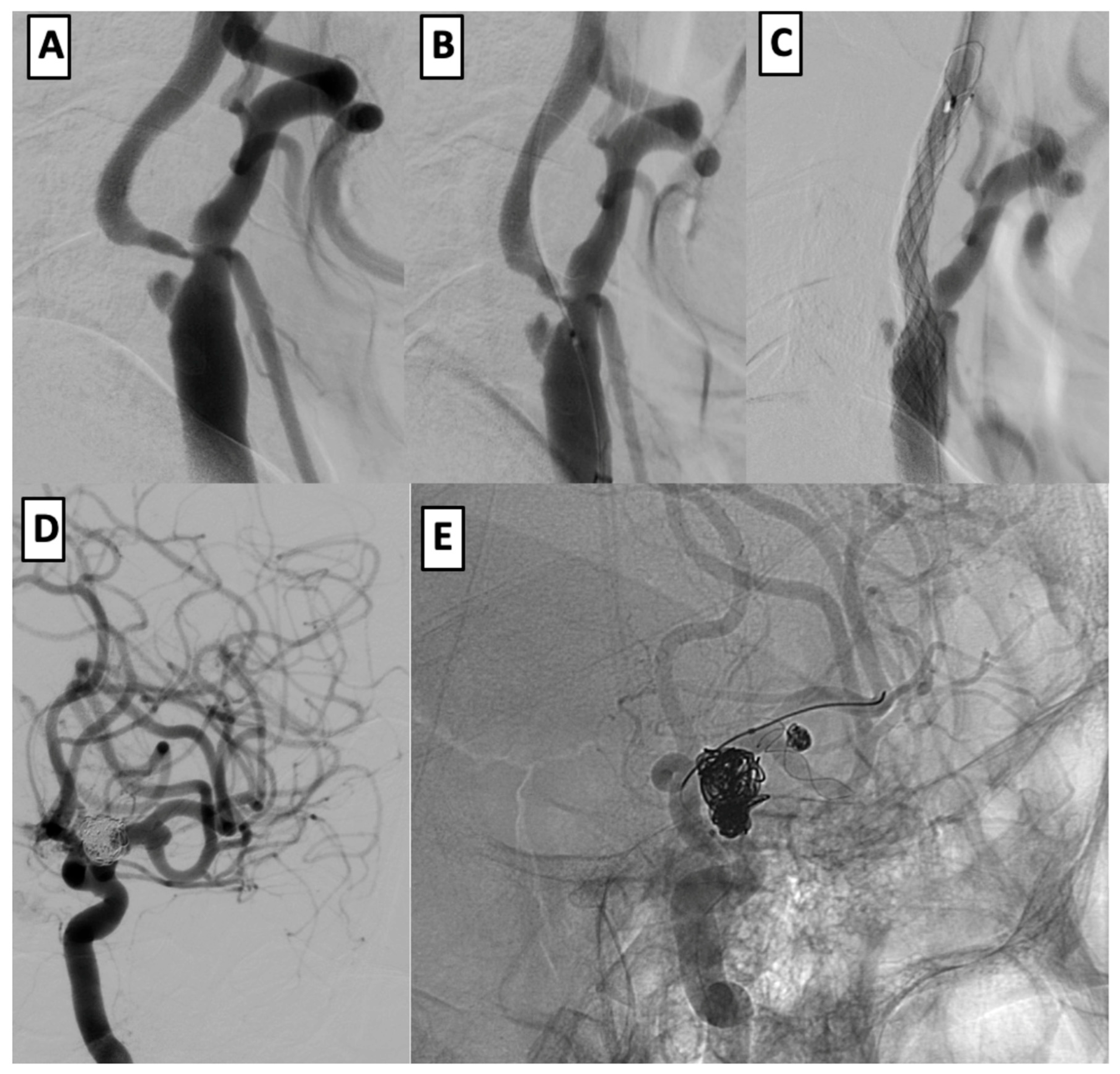
3.6. Case Examples
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACA | Anterior Cerebral Artery |
| Acom | Anterior Communicating Artery |
| BA | Basilar Artery |
| CAS | Carotid Artery Stenting |
| CTA | Computed Tomography Angiography |
| DAPT | Dual Antiplatelet Therapy |
| DSA | Digital Subtraction Angiography |
| DWI | Diffusion-Weighted Imaging |
| ICA | Internal Carotid Artery |
| IDH | Isocitrate Dehydrogenase |
| IHD | Ischemic Heart Disease |
| MCA | Middle Cerebral Artery |
| mRS | Modified Rankin Scale |
| MRI | Magnetic Resonance Imaging |
| SAH | Subarachnoid Hemorrhage |
| TIA | Transient Ischemic Attack |
| VA | Vertebral Artery |
References
- Hartmann, M.; Weber, R.; Zoubaa, S.; Schranz, C.; Knauth, M. Fatal subarachnoid hemorrhage after carotid stenting. J Neuroradiol. 2004, 31, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Pappada, G.; Fiori, L.; Marina, R.; Vaiani, S.; Gaini, S.M. Management of symptomatic carotid stenoses with coincidental intracranial aneurysms. Acta Neurochir. 1996, 138, 1386–1390. [Google Scholar] [CrossRef] [PubMed]
- Kappelle, L.; Eliasziw, M.; Fox, A.J.; Barnett, H.J. Small, unruptured intracranial aneurysms and management of symptomatic carotid artery stenosis: North American Symptomatic Carotid Endarterectomy Trial Group. Neurology 2000, 55, 307–309. [Google Scholar] [PubMed]
- Ladowski, J.S.; Webster, M.W.; Yonas, H.O.; Steed, D.L. Carotid endarterectomy in patients with asymptomatic intracranial aneurysm. Ann. Surg. 1984, 200, 70–73. [Google Scholar] [PubMed]
- Adams, H.P., Jr. Carotid stenosis and coexisting ipsilateral intracranial aneurysm: A problem in management. Arch. Neurol. 1977, 34, 515–516. [Google Scholar] [CrossRef] [PubMed]
- Kaçar, E.; Nas, Ö.F.; Erdoğan, C.; Hakyemez, B. Single-stage endovascular treatment in patients with severe extracranial large vessel stenosis and concomitant ipsilateral unruptured intracranial aneurysm. Diagn. Interv. Radiol. 2015, 21, 476–482. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Iwata, T.; Mori, T.; Tajiri, H. Successful staged endovascular treatment of a symptomatic cervical bifurcation stenosis coupled with a coincidental unruptured cerebral aneurysm in the carotid distal segment. AJNR Am. J. Neuroradiol. 2008, 29, 1948–1950. [Google Scholar] [CrossRef] [PubMed]
- Badruddin, A.; Teleb, M.S.; Abraham, M.G.; Taqi, M.A.; Zaidat, O.O. Safety and feasibility of simultaneous ipsilateral proximal carotid artery stenting and cerebral aneurysm coiling. Front. Neurol. 2010, 1, 120. [Google Scholar] [CrossRef] [PubMed]
- Gallego León, J.I.; Concepción Aramendía, L.; Ballenilla Marco, F.; Vázquez Suárez, J.C. Concomitant endovascular treatment of concomitant extracranial carotid stenosis and intracranial aneurysm. Our experience. Interv. Neuroradiol. 2009, 15, 53–59. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- ACAS Trial Investigators. Endarterectomy for asymptomatic carotid artery stenosis: Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA 1995, 273, 1421–1428. [Google Scholar] [CrossRef]
- Campos, J.K.; Lin, L.M.; Beaty, N.B.; Bender, M.T.; Jiang, B.; Zarrin, D.A.; Coon, A.L. Tandem cervical carotid stenting for stenosis with flow diversion embolisation for the treatment of intracranial aneurysms. Stroke Vasc. Neurol. 2019, 4, e000187. [Google Scholar] [CrossRef]
- Park, J.C.; Kwon, B.J.; Kang, H.S.; Kim, J.E.; Kim, K.M.; Cho, Y.D.; Han, M.H. Single-stage extracranial carotid artery stenting and intracranial aneurysm coiling: Technical feasibility and clinical outcome. Interv. Neuroradiol. 2013, 19, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Laurent, D.; Lucke-Wold, B.; Leary, O.; Randall, M.H.; Porche, K.; Koch, M.; Chalouhi, N.; Polifka, A.; Hoh, B.L. The evolution of endovascular therapy for intracranial aneurysms: Historical perspective and next frontiers. Neurosci. Insights 2022, 17, 26331055221117560. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.S.; Lee, C.; Dhillon, P.S.; Kirollos, R.; Nga, V.D.W.; Yeo, T.T.; Henkes, H.; Arthur, A.S.; Yeo, L.L.L.; Bhogal, P. Antiplatelet therapy in aneurysmal subarachnoid hemorrhage: An updated meta-analysis. Neurosurg. Rev. 2023, 46, 221. [Google Scholar] [CrossRef] [PubMed]
- Qoorchi Moheb Seraj, F.; Mirbolouk, M.H.; Vaezi, M. Safety of dual antiplatelet therapy in the acute phase of aneurysmal subarachnoid. Focus 2023, 55, E10. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Patient # | Age | Gender | Presenting Symptoms | Aneurysm (#) and Localization | Stenosis Localization | Ipsilateral Lesion? | Aneurysm Size | Stenosis Length | Stenosis Degree | Stents Used | mRS Before | mRS FU |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 67 | m | Persistent headache | (2) A1 left, right MCA bif | M2 left | Yes | Small | 20 mm | 70% | Ultimaster 3.5× 9; | 2 | 2 |
| 2 | 70 | m | Left cerebellar stroke, persistent headache, sensorineural hearing loss | (1) A1 left | V1 left, Left ICA supraclinoid | Yes | Small | 15 mm | 80% | Destiny 3.0 × 15 | 1 | 1 |
| 3 | 75 | m | Persistent headache | (1) Right ICA, supraclinoid | V1 right | Yes | Small | 15 mm | 70% | Ultimaster 3.5 × 9; | 2 | 2 |
| 4 | 72 | m | Persistent headache | (1) Right MCA bif | V1 left, V1 right | Yes | Small | 30 mm | 70% | Ultimaster Nagomi 2.5 × 12; Orsiro 3.5 × 26 | 1 | 1 |
| 5 | 65 | f | Right frontal and parietal strokes with left-sided hemiparesis | (1) Right MCA bif | Left MCA bif | No | Small | 15 mm | 70% | LVIS EVO 3.0 × 18 | 3 | 3 |
| 6 | 65 | m | Left occipital stroke | (1) Right ICA, ophthalmic | V1 left | No | Small | 10 mm | 70% | Ultimaster 4.0 × 9; | 1 | 1 |
| 7 | 45 | f | Persistent headache | (1) Right ICA, supraclinoid | Right ICA, cervical | Yes | Medium | 35 mm | 80% | X.ACT 8-6 × 30; Carotid WALLSTENT 7–30 × 135 | 1 | 1 |
| 8 | 40 | f | Persistent headache | (2) Right ICA, supraclinoid, Left ICA ophthalmic | Left ICA supraclinoid | Yes | Small | 20 mm | 70% | pEGASUS 4.5 × 20 | 1 | 1 |
| 9 | 72 | f | Persistent headache | (1) Left ICA, communicant | BA | N/A | Small | 20 mm | 80% | CREDO 5.0 × 20 | 1 | 1 |
| 10 | 60 | m | Persistent headache | (2) Left M2, left ICA supraclinoid | Right ICA, supraclinoid, cavernous | No | Small | 30 mm | 80% | Credo 5.0 × 25; Ultimaster 4.0 × 12 | 2 | 2 |
| 11 | 69 | m | Right frontal and parietal strokes with left-sided hemiparesis | (1) Right ICA, cavernous | Right ICA, supraclinoid | Yes | Small | 20 mm | 70% | CREDO 4.0 × 20 | 2 | 2 |
| 12 | 57 | m | Persistent headache | (2) Left ICA, communicant, Left MCA bif | Left ICA, cervical | Yes | Medium | 40 mm | 99% | X.ACT 10-10 × 30 CASPER 9 × 20 × 143 | 2 | 2 |
| 13 | 38 | m | Right cerebellar stroke | (1) Left MCA bif | V1 right | No | Small | 20 mm | 80% | Ultimaster 3.5 × 12 | 2 | 1 |
| 14 | 64 | f | Left frontal stroke with right-sided hemiparesis | (1) Left MCA bif | Left М2 | Yes | Small | 20 mm | 99% | CREDO 4.0 × 20 | 2 | 2 |
| 15 | 60 | f | Persistent headache | (1) Right ICA, communicant | Right ICA supraclinoid | Yes | Small | 25 mm | 75% | CASPER 7 × 30 × 143 | 1 | 1 |
| 16 | 43 | m | Ruptured aneurysm, left-sided hemiparesis | (3) Right MCA bif, left MCA bif, left ICA choroidal | V1 left, left ICA cervical, right ICA, cervical | Yes | Medium | 50 mm | 99% | Ultimaster 2.75–9; BioMatrix 3.5 × 9; Wallaby 3.0 × 40; Wallaby 2.5 × 40 | 3 | 3 |
| 17 | 56 | f | Persistent headache, sensorineural hearing loss | (1) Left MCA bif | Left ICA cervical, right ICA, cervical | Yes | Medium | 40 mm | 75% | CGuard 10 × 40; CGuard 9 × 30; LEO 2.5 × 25 | 1 | 1 |
| 18 | 59 | m | Ruptured aneurysm, right parietal strokes, left-sided hemiparesis | (1) BA fusiform | Right ICA, cervical | N/A | Fusiform | 25 mm | 80% | Mozec 4.5 × 23; СGuard 9 × 40; LEO + 4.5 × 75 | 3 | 3 |
| 19 | 68 | f | Persistent headache | (1) Right ICA, supraclinoid | V1 left | No | Small | 10 mm | 90% | Ultimaster Terumo 4.0 × 9.0 | 1 | 1 |
| 20 | 57 | f | Left temporal stroke | (1) Left MCA bif | Left M1-M2 | Yes | Medium | 20 mm | 70% | Acclino flex 5.0 × 20 | 2 | 2 |
| 21 | 66 | m | Left frontal stroke | (1) Right MCA bif | Left ICA, cervical | No | Medium | 30 mm | 70% | Protege 8 × 6–30 | 1 | 1 |
| 22 | 64 | f | Persistent headache | (1) Right M1 | Right ICA, cervical | Yes | Small | 30 mm | 70% | Protege 8 × 6–30 | 1 | 1 |
| 23 | 69 | m | Left frontal stroke with right-sided hemiparesis | (1) BA bif | Left ICA, cervical | N/A | Small | 30 mm | 85% | Protege 8 × 6–30 | 3 | 3 |
| 24 | 59 | f | Right occipital, cerebellar, and basal ganglia strokes | (1) Acom | V1 Right | N/A | Small | 30 mm | 95% | AclinoFlex 3.0 × 15 | 4 | 4 |
| 25 | 69 | m | Right frontal stroke | (1) Left MCA bif | Right ICA cervical | No | Small | 40 mm | 80% | Protege 8 × 6–40 | 2 | 2 |
| 26 | 66 | m | Ruptured aneurysm | (1) Left MCA bif | Right ICA supraclinoid | No | Small | 30 mm | 85% | Protege 8 × 6–30 | 2 | 2 |
| 27 | 58 | f | Persistent headache | (1) Right ICA supraclinoid | Left ICA, cervical | No | Small | 30 mm | 80% | Protege 7 × 10–30 | 2 | 2 |
| 28 | 61 | m | Left occipital and cerebellar strokes | (1) Right M2 | V1 Left | No | Small | 30 mm | 80% | Ultimaster 4.0 × 9; Ultimaster 2.5 × 9; Ultimaster 3.0 × 9 | 2 | 2 |
| 29 | 70 | f | Right frontal and parietal strokes | (1) Right ICA supraclinoid | Right ICA, cervical | Yes | Small | 40 mm | 70% | Protege 8-6 × 30 | 2 | 2 |
| 30 | 77 | f | Right frontal and parietal strokes | (1) Right MCA bif | Right ICA, cervical | Yes | Small | 40 mm | 85% | Protege 8-6 × 40 | 2 | 2 |
| 31 | 65 | m | Ruptured aneurysm, left frontal and parietal strokes | (2) Left ICA, ophtalmic, terminus | Left ICA, cervical | Yes | Small | 40 mm | 80% | Protege 8-6 × 40; LEO 2.0 × 18 | 2 | 2 |
| 32 | 75 | f | Ruptured aneurysm, right frontal and parietal strokes | (2) Right ICA, communicant, right MCA bif | Right ICA, cervical, left ICA ophtalmic | Yes | Medium | 25 mm | 70% | Protege 6 × 8–30 | 3 | 3 |
| 33 | 56 | f | Left temporal stroke | (1) Acom | Left ICA, cervical | N/A | Medium | 30 mm | 70% | Protege 8-6 × 30 | 2 | 2 |
| 34 | 60 | f | Ruptured aneurysm, right frontal and parietal strokes | (1) Right MCA bif | Right ICA, cervical | Yes | Small | 15 mm | 85% | AclinoFlex 3.0 × 15 | 3 | 5 |
| 35 | 59 | f | Ruptured aneurysm, multiple strokes | (6) Acom, right MCA bif, right ICA ophtalmic, communicant, supraclinoid, left ICA ophtalmic | Right ICA, cervical | Yes | Small | 30 mm | 80% | Protege 8 × 6–30 | 3 | 3 |
| 36 | 55 | m | Ruptured aneurysm | (1) Right ICA, communicant | Right ICA cervical | Yes | Medium | 30 mm | 70% | Protege 8 × 6–30 | 2 | 2 |
| 37 | 56 | f | Ruptured aneurysm | (1) BA bif | Left ICA cavernous | N/A | Small | 30 mm | 75% | Orsiro 3.50 × 1; Solitaire AB 6 × 30 | 2 | 2 |
| 38 | 63 | m | Left frontal stroke | (1) Left MCA bif | Left ICA, cervical | Yes | Small | 40 mm | 80% | Protege 6 × 8–40 (2) | 2 | 2 |
| 39 | 40 | f | Persistent headache | (1) Left ICA, ophtalmic | Left ICA, cervical | Yes | Medium | 40 mm | 70% | Protege 8 × 6–40; Protege 8 × 6–30 | 2 | 2 |
| 40 | 59 | f | Right occipital and cerebellar strokes | (1) Right ICA, communicant | V1 right | No | Medium | 40 mm | 80% | Protege 6 × 8–40 | 3 | 4 |
| 41 | 64 | f | Left cerebellar stroke | (1) V1 left | V1 left | Yes | Small | 10 mm | 70% | Resolute ONYX 2.0 × 8 | 2 | 2 |
| 42 | 53 | m | Right frontal stroke | (2) Acom, left ICA, cavernous | Left ICA, cervical, V1 right, V1 left | Yes | Medium | 30 mm | 70% | Protege 6 × 8–40 | 2 | 2 |
| 43 | 82 | f | Persistent headache | (1) Right ICA, cavernous | Right ICA, cervical | Yes | Fusiform | 30 mm | 70% | Protege 8 × 6–30, Pipeline with Shield 4.5 × 25 | 2 | 2 |
| 44 | 63 | f | Repeated pontine ischemia, Millard–Gubler syndrome | (1) BA bif | V1 left | N/A | Medium | 15 mm | 80% | Ultimaster 3.5 × 15 | 2 | 2 |
| 45 | 66 | m | Right frontal and parietal strokes | (1) Right MCA bif | Right ICA, cervical | Yes | Small | 30 mm | 85% | CASPER 7-30 × 143 | 2 | 2 |
| 46 | 67 | f | Persistent headache | (1) Right ICA, ophthalmic | Right ICA, cervical | Yes | Small | 40 mm | 90% | Protege 6 × 8–40 | 1 | 1 |
| 47 | 30 | f | Left occipital and cerebellar strokes | (1) V2 right | V3-V4 left | Yes | Small | 15 mm | 80% | XIENCE Xpedition 4 × 12 | 3 | 3 |
| One Stenosis Localization | Multiple Stenosis Localization | Total | p-Value Fisher’s | |
|---|---|---|---|---|
| Smoking | ||||
| No | 28 (71.79%) | 2 (25.00%) | 30 | 0.0191 |
| Yes | 11 (28.21%) | 6 (75.00%) | 17 | |
| AH | ||||
| AH1 | 3 (7.69%) | 0 (0.00%) | 3 | 0.1217 |
| AH2 | 3 (7.69%) | 3 (37.50%) | 6 | |
| AH3 | 33 (84.62%) | 5 (62.50%) | 38 | |
| Diabetes | ||||
| No | 31 (79.49%) | 5 (62.50%) | 36 | 0.3673 |
| Yes | 8 (20.51%) | 3 (37.50%) | 11 | |
| IHD | ||||
| No | 13 (33.33%) | 0 (0.00%) | 13 | 0.0855 |
| Yes | 26 (66.67%) | 8 (100.00%) | 34 | |
| Obesity | ||||
| Non-obese | 29 (74.36%) | 7 (87.50%) | 36 | 0.6593 |
| Obese | 10 (25.64%) | 1 (12.50%) | 11 | |
| One Aneurysm | Multiple Aneurysms | Total | p -V alue Fisher’s | |
| Smoking | ||||
| No | 26 (68.42%) | 4 (44.44%) | 30 | 0.2516 |
| Yes | 12 (31.58%) | 5 (55.56%) | 17 | |
| AH | ||||
| AH1 | 1 (2.63%) | 2 (22.22%) | 3 | 0.1201 |
| AH2 | 5 (13.16%) | 1 (11.11%) | 6 | |
| AH3 | 32 (84.21%) | 6 (66.67%) | 38 | |
| Diabetes | ||||
| No | 28 (73.68%) | 8 (88.89%) | 36 | 0.6631 |
| Yes | 10 (26.32%) | 1 (11.11%) | 11 | |
| IHD | ||||
| No | 11 (28.95%) | 2 (22.22%) | 13 | 1 |
| Yes | 27 (71.05%) | 7 (77.78%) | 34 | |
| Obesity | ||||
| Non-obese | 28 (73.68%) | 8 (88.89%) | 36 | 0.6631 |
| Obese | 10 (26.32%) | 1 (11.11%) | 11 |
| mRS 1–2 | mRS 3–6 | Total | p-Value Fisher’s | |
|---|---|---|---|---|
| Aneurysm side | ||||
| Left | 14 (37.84%) | 0 (0.00%) | 14 | 0.019 |
| Bilateral | 6 (16.22%) | 5 (50.00%) | 11 | |
| Right | 17 (45.95%) | 5 (50.00%) | 22 | |
| Aneurysm arteries | ||||
| ACA | 1 (2.70%) | 0 (0.00%) | 1 | 0.0761 |
| Acom | 1 (2.70%) | 1 (10.00%) | 2 | |
| BA | 2 (5.41%) | 2 (20.00%) | 4 | |
| ICA | 15 (40.54%) | 1 (10.00%) | 16 | |
| MCA | 13 (35.14%) | 2 (20.00%) | 15 | |
| Bilateral | 4 (10.81%) | 3 (30.00%) | 7 | |
| VA | 1 (2.70%) | 1 (10.00%) | 2 | |
| Stenosis side | ||||
| Left | 17 (45.95%) | 3 (30.00%) | 20 | 0.7017 |
| Bilateral | 5 (13.51%) | 2 (20.00%) | 7 | |
| Right | 15 (40.54%) | 5 (50.00%) | 20 | |
| Stenosis arteries | ||||
| BA | 1 (2.70%) | 0 (0.00%) | 1 | 0.9497 |
| ICA | 22 (59.46%) | 5 (50.00%) | 27 | |
| MCA | 3 (8.11%) | 1 (10.00%) | 4 | |
| Multiple | 3 (8.11%) | 1 (10.00%) | 4 | |
| VA | 8 (21.62%) | 3 (30.00%) | 11 | |
| The stenosis side and aneurysm side coincide | ||||
| N/A | 4 (10.81%) | 3 (30.00%) | 7 | 0.3108 |
| No | 9 (24.32%) | 2 (20.00%) | 11 | |
| Yes | 24 (64.86%) | 5 (50.00%) | 29 |
| mRS 1–2 | mRS 3–6 | Total | p-Value Fisher’s | |
|---|---|---|---|---|
| Aneurysm Size | ||||
| Fusiform | 1 (2.70%) | 1 (10.00%) | 2 | 0.4291 |
| Medium | 10 (27.03%) | 3 (30.00%) | 13 | |
| Small | 26 (70.27%) | 6 (60.00%) | 32 | |
| Stenosis length | ||||
| 10 mm | 3 (8.11%) | 0 (0.00%) | 3 | 0.0469 |
| 15 mm | 3 (8.11%) | 3 (30.00%) | 6 | |
| 20 mm | 7 (18.92%) | 0 (0.00%) | 7 | |
| 25 mm | 1 (2.70%) | 2 (20.00%) | 3 | |
| 30 mm | 13 (35.14%) | 3 (30.00%) | 16 | |
| 35 mm | 1 (2.70%) | 0 (0.00%) | 1 | |
| 40 mm | 9 (24.32%) | 1 (10.00%) | 10 | |
| 50 mm | 0 (0.00%) | 1 (10.00%) | 1 | |
| Stenosis degree | ||||
| 70 | 16 (43.24%) | 2 (20.00%) | 18 | 0.2588 |
| 75 | 3 (8.11%) | 0 (0.00%) | 3 | |
| 80 | 11 (29.73%) | 4 (40.00%) | 15 | |
| 85 | 3 (8.11%) | 2 (20.00%) | 5 | |
| 90 | 2 (5.41%) | 0 (0.00%) | 2 | |
| 95 | 0 (0.00%) | 1 (10.00%) | 1 | |
| 99 | 2 (5.41%) | 1 (10.00%) | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarshayev, M.; Makhanbetkhan, S.; Maidan, A.; Pons, R.B.; Davletov, D.; Zhumabekov, A.; Berdikhojayev, M. Single-Stage Endovascular Management of Concurrent Intracranial Aneurysms and Arterial Stenoses: Clinical Outcomes, Procedural Strategies, and Predictive Factors. Brain Sci. 2025, 15, 744. https://doi.org/10.3390/brainsci15070744
Sarshayev M, Makhanbetkhan S, Maidan A, Pons RB, Davletov D, Zhumabekov A, Berdikhojayev M. Single-Stage Endovascular Management of Concurrent Intracranial Aneurysms and Arterial Stenoses: Clinical Outcomes, Procedural Strategies, and Predictive Factors. Brain Sciences. 2025; 15(7):744. https://doi.org/10.3390/brainsci15070744
Chicago/Turabian StyleSarshayev, Marat, Shayakhmet Makhanbetkhan, Aiman Maidan, Roger Barranco Pons, Dimash Davletov, Abzal Zhumabekov, and Mynzhylky Berdikhojayev. 2025. "Single-Stage Endovascular Management of Concurrent Intracranial Aneurysms and Arterial Stenoses: Clinical Outcomes, Procedural Strategies, and Predictive Factors" Brain Sciences 15, no. 7: 744. https://doi.org/10.3390/brainsci15070744
APA StyleSarshayev, M., Makhanbetkhan, S., Maidan, A., Pons, R. B., Davletov, D., Zhumabekov, A., & Berdikhojayev, M. (2025). Single-Stage Endovascular Management of Concurrent Intracranial Aneurysms and Arterial Stenoses: Clinical Outcomes, Procedural Strategies, and Predictive Factors. Brain Sciences, 15(7), 744. https://doi.org/10.3390/brainsci15070744