
Neuroanatomical and Neurocognitive Differences Between the Executive Functions in Child Sexual Offenders: A Systematic Review





Abstract

1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
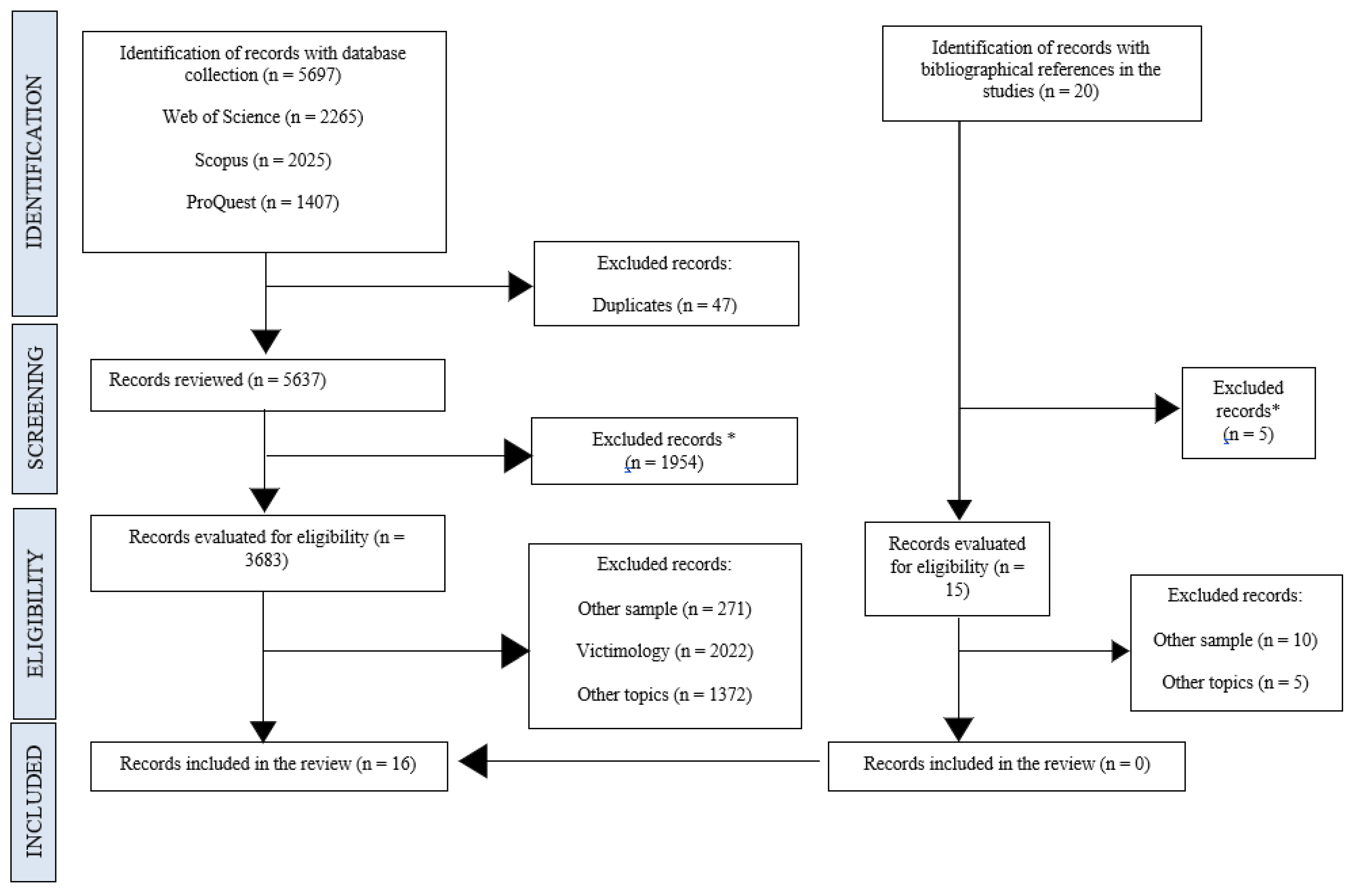
2.3. Study Selection Procedure
2.4. Data Extraction
2.5. Risk of Bias and Quality Assessment
3. Results
3.1. Characteristics of the Studies
3.2. Neurocognitive and Neuroanatomical Alterations
3.2.1. Neurocognitive Alterations
3.2.2. Neuroanatomical Alterations
4. Discussion
4.1. Limitations and Future Research
4.2. Implications for Clinical Practice and Social Policy
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Items | Item n. º | Item Location |
|---|---|---|
| Title. Identifies the publication as a systematic review | 1 | 1 |
| Abstract. Structured summary | 2 | 2 |
| Introduction. Justification | 3 | 3–6 |
| Introduction. Objectives | 4 | 6 |
| Methods. Eligibility criteria | 5 | 7 |
| Methods. Sources of information | 6 | 7 |
| Methods. Research strategy | 7 | 8–9 |
| Methods. Study selection process | 8 | 8–9 |
| Methods. Data extraction process | 9 | 9–10/34 |
| Methods. List of data | 10 a* | 10 |
| Methods. List of data (variables) | 10 b* | 10 |
| Methods. Bias ratio in individual studies | 11 | 10 |
| Methods. Measures of the effect | 12 | - |
| Methods. Results synthesis (selection criteria) | 13 a* | 10 |
| Methods. Results synthesis (required method) | 13 b* | 10 |
| Methods. Results synthesis (presentation method) | 13 c* | 9–10 |
| Methods. Results synthesis (justification) | 13 d* | 9–10 |
| Methods. Results synthesis (heterogeneity) | 13 e* | 10 |
| Methods. Results synthesis (robustness) | 13 f* | 10 |
| Methods. Assessment by publication | 14 | 10 |
| Methods. Assessment of the certainty of the evidence | 15 | 10 |
| Results. Selection of the studies (research) | 16 a* | 10–11 |
| Results. Selection of the studies (inclusive) | 16 b* | 10–11 |
| Results. Characteristics of the studies | 17 | 36–39 |
| Results. Individual studies bias ratio | 18 | - |
| Results. Results of individual studies | 19 | 40–42 |
| Results. Results of the synthesis (characteristics) | 20 a* | 12–14 |
| Results. Results of the synthesis (presentation) | 20 b* | 12–14 |
| Results. Results of the synthesis (heterogeneity) | 20 c* | 12–14 |
| Results. Results of the synthesis (robustness) | 20 d* | 12–14 |
| Results. Publication bias | 21 | - |
| Results. Certainty of the evidence | 22 | 34 |
| Discussion. Interpretation of results | 23 a* | 14–19 |
| Discussion. Limitations of the evidence | 23 b* | 19 |
| Discussion. Limitations of the review process | 23 | 19–22 |
| Discussion. Implications and future lines of action | 23 d* | 22 |
| Other information. Registry and protocol (registry) | 24 a* | - |
| Other information. Registry and protocol (access) | 24 b* | - |
| Other information. Registry and protocol (amendment) | 24 c* | - |
| Other information. Funding | 25 | 23 |
| Other information. Conflict of interest | 26 | 23 |
| Availability of data, codes and other materials | 27 | 23 |
Appendix B
| Quality Level | Study Design | Directness | Consistence | Precision | Risk of Bias | |
|---|---|---|---|---|---|---|
| [45] | Moderate | * | Mod. | High | Mod. | Mod. |
| [35] | Moderate | * | Mod. | High | Mod. | Mod. |
| [36] | Moderate | * | Mod. | High | Mod. | Mod. |
| [37] | Moderate | * | Mod. | High | Mod. | Mod. |
| [48] | Moderate | * | Mod. | High | Mod. | Mod. |
| [49] | Moderate | * | Mod. | High | Mod. | Mod. |
| [50] | Moderate | * | Mod. | High | Mod. | Mod. |
| [38] | Moderate | * | Mod. | High | Mod. | Mod. |
| [39] | Moderate | * | Mod. | High | Mod. | Mod. |
| [40] | Moderate | * | Mod. | High | Mod. | Mod. |
| [41] | Moderate | * | Mod. | High | Mod. | Mod. |
| [42] | Moderate | * | Mod. | High | Mod. | Mod. |
| [46] | Moderate | * | Mod. | High | Mod. | Mod. |
| [47] | Moderate | * | Mod. | High | Mod. | Mod. |
| [43] | Moderate | * | Mod. | High | Mod. | Mod. |
| [44] | Moderate | * | Mod. | High | Mod. | Mod. |
References
- Quintero, D.M. ¿Las parafilias, un paradigma o un problema de salud pública? Salud Arte Cuid. 2023, 16, 43–50. [Google Scholar] [CrossRef]
- Morrison, J. DSM-5® Guía Para el Diagnóstico Clínico; Editorial El Manual Moderno: Ciudad De León, Gto, Mexico, 2015. [Google Scholar]
- Seto, M.C. Pedophilia and Sexual Offending Against Children: Theory, Assessment, and Intervention; American Psychological Association: Washington, DC, USA, 2008. [Google Scholar] [CrossRef]
- Seto, M.C. Pedophilia. Annu. Rev. Clin. Psychol. 2009, 5, 391–407. [Google Scholar] [CrossRef] [PubMed]
- Seto, M.C. Defining pedophilia. In Pedophilia and Sexual Offending Against Children: Theory, Assessment, and Intervention; Seto, M.C., Ed.; American Psychological Association: Washington, DC, USA, 2018; pp. 9–30. [Google Scholar] [CrossRef]
- Finkelhor, D. Child Sexual Abuse: New Theory and Research; Free Press: New York, NY, USA, 1984. [Google Scholar]
- Gómez, A. Análisis Documental del Perfil del Abusador Sexual Infantil. Tesis de Grado Universidad de Antioquia. 2018. Available online: https://repository.ucc.edu.co/bitstream/20.500.12494/7300/1/2019_abusador_sexual_caracteristicas.pdf (accessed on 27 November 2022).
- Kruger, T.H.; Schiffer, B. Neurocognitive and personality factors in homo- and heterosexual pedophiles and controls. J. Sex. Med. 2011, 8, 1650–1659. [Google Scholar] [CrossRef]
- Joyal, C.C.; Beaulieu-Plante, J.; de Chantérac, A. The neuropsychology of sex offenders: A meta-analysis. Sex. Abus. 2014, 26, 149–177. [Google Scholar] [CrossRef]
- Dillien, T.; Brazil, I.A.; Sabbe, B.; Goethals, K. Personality features of sexual offenders who committed offences against children. J. Sex. Aggress. 2023, 29, 34–50. [Google Scholar] [CrossRef]
- Strassberg, D.S.; Eastvold, A.; Kenney, J.W.; Suchy, Y. Psychopathy among pedophilic and nonpedophilic child molesters. Child Abus. Negl. 2012, 36, 379–382. [Google Scholar] [CrossRef]
- Mohnke, S.; Müller, S.; Amelung, T.; Krüger, T.H.; Ponseti, J.; Schiffer, B.; Walter, M.; Beier, K.B.; Walter, H. Brain alterations in pedophilia: A critical review. Prog. Neurobiol. 2014, 122, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.M.; Swerdlow, R.H. Right orbitofrontal tumor with pedophilia symptom and constructional apraxia sign. Arch. Neurol. 2003, 60, 437–440. [Google Scholar] [CrossRef]
- Flor-Henry, P.; Lang, R.A.; Koles, Z.J.; Frenzel, R.R. Quantitative EEG studies of pedophilia. Int. J. Psychophysiol. 1991, 10, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Graber, B.; Hartmann, K.; Coffman, J.A.; Huey, C.J.; Golden, C.J. Brain damage among mentally disordered sex offenders. J. Forensic Sci. 1982, 27, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Schiffer, B.; Krueger, T.; Paul, T.; de Greiff, A.; Forsting, M.; Leygraf, N.; Schedlowski, M.; Gizewski, E. Brain response to visual sexual stimuli in homosexual pedophiles. J. Psychiatry Neurosci. 2008, 33, 23–33. [Google Scholar]
- Schiffer, B.; Peschel, T.; Paul, T.; Gizewski, E.; Forsting, M.; Leygraf, N.; Schedlowski, M.; Krueger, T.H. Structural brain abnormalities in the frontostriatal system and cerebellum in pedophilia. J. Psychiatr. Res. 2007, 41, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Scarpazza, C.; Finos, L.; Genon, S.; Masiero, L.; Bortolato, E.; Cavaliere, C.; Pezzaioli, J.; Monaro, M.; Navarin, N.; Battaglia, U.; et al. Idiopathic and acquired pedophilia as two distinct disorders: An insight from neuroimaging. Brain Imaging Behav. 2021, 15, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Tenbergen, G.; Wittfoth, M.; Frieling, H.; Ponseti, J.; Walter, M.; Walter, H.; Beier, K.M.; Schiffer, B.; Kruger, T.H. The neurobiology and psychology of pedophilia: Recent advances and challenges. Front. Hum. Neurosci. 2015, 9, 344. [Google Scholar] [CrossRef]
- Seto, M.C. The motivation-facilitation model of sexual offending. Sex. Abus. 2019, 31, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Cantor, J.M.; Kabani, N.; Christensen, B.K.; Zipursky, R.B.; Barbaree, H.E.; Dickey, R.; Klassen, P.E.; Mikulis, D.J.; Kuban, M.E.; Blak, T.; et al. Cerebral white matter deficiencies in pedophilic men. J. Psychiatr. Res. 2008, 42, 167–183. [Google Scholar] [CrossRef]
- Dillien, T.; Goethals, K.; Sabbe, B.; Brazil, I.A. The neuropsychology of child sexual offending: A systematic review. Aggress. Violent Behav. 2020, 54, 101406. [Google Scholar] [CrossRef]
- Turner, D.; Rettenberger, M. Neuropsychological functioning in child sexual abusers: A systematic review. Aggress. Violent Behav. 2020, 54, 101405. [Google Scholar] [CrossRef]
- Gerwinn, H.; Weiß, S.; Tenbergen, G.; Amelung, T.; Födisch, C.; Pohl, A.; Massau, C.; Kneer, J.; Mohnke, S.; Kärgel, C.; et al. Clinical characteristics associated with pedophilia and child sex offending–Differentiating sexual preference from offence status. Eur. Psychiatry 2018, 51, 74–85. [Google Scholar] [CrossRef]
- Picard, E.H.; Bopp, L.L.; Rosenfeld, B. Neuropsychological Functioning in Sexual Offenders With and Without Pedophilic Disorder. Arch. Sex. Behav. 2024, 53, 43–56. [Google Scholar] [CrossRef]
- Storch, M.; Kanthack, M.; Amelung, T.; Beier, K.M.; Krueger, T.H.; Sinke, C.; Schoenknecht, P. Hypothalamic volume in pedophilia with or without child sexual offense. Eur. Arch. Psychiatry Clin. Neurosci. 2023, 273, 1295–1306. [Google Scholar] [CrossRef] [PubMed]
- Cock, M.R.; Matute, E.; Jurado, M.B. Las funciones ejecutivas a través de la vida. Rev. Neuropsicol. Neuropsiquiatría Neurocienc. 2008, 8, 23–46. [Google Scholar] [CrossRef]
- Kennedy, M.R.T.; Coelho, C.; Turkstra, L.; Ylvisaker, M.; Moore Sohlberg, M.; Yorkston, K.; Chiou, H.H.; Kan, P.F. Intervention for executive functions after traumatic brain injury: A systematic review, meta-analysis and clinical recommendations. Neuropsychol. Rehabil. 2008, 18, 257–299. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. Declaration PRISMA 2020: An updated guideline for systematic review publication. Rev. Esp. Cardiol. 2021, 74, 790–799. [Google Scholar] [CrossRef] [PubMed]
- Santos, C.M.D.C.; Pimenta, C.A.D.M.; Nobre, M.R.C. The PICO strategy for the research question construction and evidence search. Rev. Lat. Am. Enferm. 2007, 15, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Fonteille, V.; Cazala, F.; Moulier, V.; Stoléru, S. Pedophilia: Contribution of neurology and neuroimaging techniques. L’encephale 2012, 38, 496–503. [Google Scholar] [CrossRef]
- Poeppl, T.B.; Eickhoff, S.B.; Fox, P.T.; Laird, A.R.; Rupprecht, R.; Langguth, B.; Bzdok, D. Connectivity and functional profiling of abnormal brain structures in pedophilia. Hum. Brain Mapp. 2015, 36, 2374–2386. [Google Scholar] [CrossRef] [PubMed]
- Aguayo-Albasini, J.L.; Flores-Pastor, B.; Soria-Aledo, V. Sistema GRADE: Clasificación de la calidad de la evidencia y graduación de la fuerza de la recomendación. Cirugía Española 2014, 92, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.; Brożek, J.; Guyatt, G.; Oxman, A. GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations. The GRADE Working Group. 2013. Available online: https://gdt.gradepro.org/app/handbook/handbook.html (accessed on 22 December 2024).
- Jordan, K.; Fromberger, P.; Müller, I.; Wernicke, M.; Stolpmann, G.; Müller, J.L. Sexual interest and sexual self-control in men with self-reported sexual interest in children—A first eye tracking study. J. Psychiatr. 2018, 96, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Kärgel, C.; Massau, C.; Weiß, S.; Walter, M.; Kruger, T.H.; Schiffer, B. Diminished functional connectivity on the road to child sexual abuse in pedophilia. J. Sex. Med. 2015, 12, 783–795. [Google Scholar] [CrossRef] [PubMed]
- Kärgel, C.; Massau, C.; Weiß, S.; Walter, M.; Borchardt, V.; Krueger, T.H.; Schiffer, B. Evidence for superior neurobiological and behavioral inhibitory control abilities in non-offending as compared to offending pedophiles. Hum. Brain Mapp. 2017, 38, 1092–1104. [Google Scholar] [CrossRef]
- Rosburg, T.; Deuring, G.; Boillat, C.; Lemoine, P.; Falkenstein, M.; Graf, M.; Mager, R. Inhibition and attentional control in pedophilic child sexual offenders– An event-related potential study. Clin. Neurophysiol. 2018, 129, 1990–1998. [Google Scholar] [CrossRef] [PubMed]
- Rosburg, T.; Pflueger, M.O.; Mokros, A.; Boillat, C.; Deuring, G.; Spielmann, T.; Graf, M. Indirect and neuropsychological indicators of pedophilia. Sex. Abus. 2021, 33, 579–605. [Google Scholar] [CrossRef]
- Schiffer, B.; Vonlaufen, C. Executive dysfunctions in pedophilic and nonpedophilic child molesters. J. Sex. Med. 2011, 8, 1975–1984. [Google Scholar] [CrossRef] [PubMed]
- Schiffer, B.; Amelung, T.; Pohl, A.; Kaergel, C.; Tenbergen, G.; Gerwinn, H.; Mohnke, S.; Massau, C.; Matthias, W.; Weiss, S.; et al. Gray matter anomalies in pedophiles with and without a history of child sexual offending. Transl. Psychiatry 2017, 7, e1129. [Google Scholar] [CrossRef] [PubMed]
- Schuler, M.; Mohnke, S.; Amelung, T.; Beier, K.M.; Walter, M.; Ponseti, J.; Schiffer, B.; Tillmann, H.C.; Walter, H. Neural processing associated with cognitive empathy in pedophilia and child sexual offending. Soc. Cogn. Affect. Neurosci. 2022, 17, 712–722. [Google Scholar] [CrossRef]
- Szczypiński, J.; Wypych, M.; Krasowska, A.; Wiśniewski, P.; Kopera, M.; Suszek, H.; Wojnar, M. Abnormal behavioral and neural responses in the right dorsolateral prefrontal cortex during emotional interference for cognitive control in pedophilic sex offenders. J. Psychiatr. Res. 2022, 151, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Weidacker, K.; Kärgel, C.; Massau, C.; Krueger, T.H.; Walter, M.; Ponseti, J.; Walter, H.; Schiffer, B. Interference inhibition in offending and non-offending pedophiles: A preliminary event-related fMRI study. Neuropsychologia 2022, 173, 108301. [Google Scholar] [CrossRef] [PubMed]
- Eastvold, A.; Suchy, Y.; Strassberg, D. Executive function profiles of pedophilic and nonpedophilic child molesters. J. Int. Neuropsychol. Soc. 2011, 17, 295–307. [Google Scholar] [CrossRef] [PubMed]
- Suchy, Y.; Whittaker, J.W.; Strassberg, D.S.; Eastvold, A. Neurocognitive differences between pedophilic and nonpedophilic child molesters. J. Int. Neuropsychol. Soc. 2009, 15, 248–257. [Google Scholar] [CrossRef]
- Suchy, Y.; Eastvold, A.D.; Strassberg, D.S.; Franchow, E.I. Understanding processing speed weaknesses among pedophilic child molesters: Response style vs. Neuropathology. J. Abnorm. Psychol. 2014, 123, 273. [Google Scholar] [CrossRef]
- Klöckner, M.S.; Jordan, K.; Kiehl, K.A.; Nyalakanti, P.K.; Harenski, C.L.; Müller, J.L. Widespread and interrelated gray matter reductions in child sexual offenders with and without pedophilia: Evidence from a multivariate structural MRI study. Psychiatry Clin. Neurosci. 2021, 75, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Lett, T.A.; Mohnke, S.; Amelung, T.; Brandl, E.J.; Schiltz, K.; Pohl, A.; Gerwinn, H.; Kärgel, C.; Massau, C.; Tenbergen, G.; et al. Multimodal neuroimaging measures and intelligence influence pedophile child sexual offense behavior. Eur. Neuropsychopharmacol. 2018, 28, 818–827. [Google Scholar] [CrossRef]
- Massau, C.; Tenbergen, G.; Kärgel, C.; Weiß, S.; Gerwinn, H.; Pohl, A.; Amelung, T.; Mohnke, S.; Kneer, J.; Wittfoth, M.; et al. Executive functioning in pedophilia and child sexual offending. J. Int. Neuropsychol. Soc. 2017, 23, 460–470. [Google Scholar] [CrossRef] [PubMed]
- Gómez, P.; Ratcliff, R.; Perea, M. A model of the go/no-go task. J. Exp. Psychol. Gen. 2007, 136, 389. [Google Scholar] [CrossRef]
- De la Iglesia-Vayá, M.; Molina-Mateo, J.; Escarti-Fabra, M.J.; Martí-Bonmatí, L.; Robles, M.; Meneu, T.; Aguilar, E.J.; Sanjuán, J. Técnicas de análisis de posproceso en resonancia magnética para el estudio de la conectividad cerebral. Radiología 2011, 53, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, A.S.; Esterman, M.; Wilson, D.; Serences, J.T.; Yantis, S. Control of spatial and feature-based attention in frontoparietal cortex. J. Neurosci. 2010, 30, 14330–14339. [Google Scholar] [CrossRef] [PubMed]
- Kringelbach, M.L.; Rolls, E.T. The functional neuroanatomy of the human orbitofrontal cortex: Evidence from neuroimaging and neuropsychology. Prog. Neurobiol. 2004, 72, 341–372. [Google Scholar] [CrossRef] [PubMed]
- Buckner, R.L.; Andrews-Hanna, J.R.; Schacter, D.L. The Brain’s Default Network: Anatomy, Function, and Relevance to Disease. Ann. N. Y. Acad. Sci. 2008, 1124, 1–38. [Google Scholar] [CrossRef]
- Popovic, D.; Wertz, M.; Geisler, C.; Kaufmann, J.; Lähteenvuo, M.; Lieslehto, J.; Witzel, J.; Bogerts, B.; Walter, M.; Falkai, P.; et al. Patterns of risk—Using machine learning and structural neuroimaging to identify pedophilic offenders. Front. Psychiatry 2023, 14, 1001085. [Google Scholar] [CrossRef] [PubMed]
- Cantor, J.; Blanchard, R. White matter volumes in pedophiles, hebephiles, and teleiophiles. Arch. Sex. Behav. 2012, 41, 749–752. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.L.; Liossi, D.; Psych, C. Neuropsychological and neurobehavioral correlates of aggression following traumatic brain injury. J. Neuropsychiatry Clin. Neurosci. 2006, 18, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Lapornik, R.; Lehofer, M.; Moser, M.; Pump, G.; Egner, S.; Posch, C.; Hildebrandt, G.; Zapotoczky, H.G. Long-term imprisonment leads to cognitive impairment. Forensic Sci. Int. 1996, 82, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Stephens, S.; Seto, M.C. Hebephilic sexual offending. In Sexual Offending: Predisposing Antecedents, Assessments and Management; Springer: Berlin/Heidelberg, Germany, 2016; pp. 29–43. [Google Scholar] [CrossRef]
- Schippers, E.E.; Smid, W.J.; Hoogsteder, L.M.; Planting, C.H.; de Vogel, V. Pedophilia is associated with lower sexual interest in adults: Meta-analyses and a systematic review with men who had sexually offended against children. Aggress. Violent Behav. 2023, 69, 101813. [Google Scholar] [CrossRef]
| Authors and Year | Country | Sample Design and Type | Sample | Construct | Instrument | ||
|---|---|---|---|---|---|---|---|
| Size | Groups | Origin | |||||
| [45] | EEUU | Exploratory–comparative Non-probabilistic sampling by convenience | 89 | Middle-aged men 34.50 (ST = 8.3) (PEDs + SOs; n = 30), middle-aged men 31.70 (ST = 7.5) (NPEDs + SOs; n = 30) and middle-aged men 31.00 (ST = 7.2) (NSOs; n = 29). | Residents in intermediate programs between imprisonment and reintegration, and online public forum. | EF: commutation, inhibition, abstraction, working memory, fluency, planning and simple attention. | DEFKS, WAIS-III, WMS-III, SILS. |
| [35] | Germany | Exploratory–comparative Non-probabilistic sampling by convenience | 93 | Middle-aged men 42.09 (ST = 10.92) (PEDs + SOs; n = 22), middle-aged men 39.18 (ST = 8.77) (PEDs + NSOs; n = 11), middle-aged men 26.82 (ST = 9.28) (CG; n = 52 non-sexual offenders/n = 8 ASOs). | Outpatients, inpatients and online public forum. | EF: attentional control and sexual interest. | SMI iView X RED, NRP Picture set. |
| [36] | Germany | Exploratory–comparative Non-probabilistic sampling by convenience | 40 | Middle-aged men 43.67 (ST = 7.08) (PEDs + SOs; n = 12), middle-aged men 28.07 (ST = 5.71) (PEDs + NSOs; n = 14) and middle-aged men 32.86 (ST = 9.89) (CG; n = 14). | Correctional services and online public forum. | RSFC in default mode network (EF). | fMRI. |
| [37] | Germany | Exploratory–comparative Non-probabilistic sampling by convenience | 117 | Middle-aged men 38.25 (ST = 8.54) (PEDs + SOs; n = 40), middle-aged men 37.00 (ST = 8.84) (PEDs + NSOs; n = 37) and middle-aged men 36.65 (ST = 10.13) (CG; n = 40). | Internet platform and penitentiary services. | Neurobiological and behavioral inhibitory control. | MRI, Go/No-Go. |
| [48] | Germany, EEUU | Exploratory–comparative Non-probabilistic sampling by convenience | 63 | Middle-aged men 44.86 (ST = 9.26) (PEDs + SOs; n = 22), middle-aged men 44.24 (ST = 9.90) (NPEDs + SOs; n = 21) and middle-aged men 36.30 (ST = 5.35) (CG; n = 20). | Database of the Kiehl laboratory in the Mind Research Network (MRN), thanks to penitentiary institutions. | Gray matter. | MRI. |
| [49] | Germany, EEUU | Exploratory–comparative Non-probabilistic sampling by convenience | 283 | Middle-aged men 39.80 (ST = 9.00) (PEDs + SOs; n = 73), middle-aged men 34.20 (ST = 9.40) (PEDs + NSOs; n = 77) and middle-aged men 33.60 (10.2) (CG; n = 133). | Clinical centers, penitentiary institutions, online forum, advertisements and mailing lists. | Structural morphology of the encephalon: cortical groove, surface area and white matter FA. | MRI. |
| [50] | Germany, EEUU | Exploratory–comparative Non-probabilistic sampling by convenience | 158 | Middle-aged men 38.04 (ST = 8.62) (PEDs + SOs; n = 45), middle-aged men 36.51 (ST = 9.46) (PEDs + NSOs; n = 45), middle-aged men 40.26 (ST = 12.71) (NPEDs + SOs; n = 19) and middle-aged men 36.43 (ST = 6.70) (CG; n = 49). | Penitentiary institutions, German prevention project “Dunkelfield” and Internet platforms. | EF: impulsivity, planning and working memory. | CANTAB, IED, SOC, SWM. |
| [38] | Swiss, Germany | Exploratory–comparative Non-probabilistic sampling by convenience | 61 | Middle-aged men 35.30 (ST = 10.9) (PEDs + SOs; n = 21), middle-aged men 37.80 (ST = 9.7) (PEDs + NSOs; n = 19) and middle-aged men 30.80 (ST = 10.2) (CG; n = 21). | Penitentiary institutions and public newspapers. | Response inhibition and attentional control. | EEG, ERPs, Go/No-Go. |
| [39] | Swiss, Germany | Exploratory–comparative Non-probabilistic sampling by convenience | 62 | Middle-aged men 35.50 (ST = 10.64) (PEDs + SOs; n = 21), middle-aged men 37.19 (ST = 9.79) (PEDs + NSOs but convicted by sexual material; n = 20) and middle-aged men 30.76 (ST = 10.15) (CG; n = 21). | Penitentiary institutions, psychiatric hospitals and public newspapers. | IQF, IQC, alertness, orientation, risk-taking, resistance to interference, and episodic and working memory. | LPS, MWT-B, ANT, CGT, Stroop, CVLT, IAT, SMP, CRT task. |
| [40] | Germany | Exploratory–comparative Non-probabilistic sampling by convenience | 63 | Middle-aged men 38.70 (ST = 8.9) (PEDs + SOs; n = 15), middle-aged men 44.20 (ST = 7.9) (NPEDs + SOs; n = 15), middle-aged men 37.40 (ST = 9.1) (FC = 16) and middle-aged men 37.70 (ST = 10.2) (CG; n = 17). | Five penitentiary institutions and public newspapers. | EF: attentional control, cognitive flexibility, working memory, behavioral response change and inhibition and fluency. | WSCT, TMT-A, TMT-B, WMS-R, CBT, Go/No-Go, Tower of London. |
| [41] | Germany | Exploratory–comparative Non-probabilistic sampling by convenience | 219 | Middle-aged men 40.10 (ST = 9.1) (PEDs + SOs; n = 58), middle-aged men 34.40 (ST = 9.2) (PEDs + NSOs = 60) and middle-aged men 33.80 (ST = 10.5) (CG; n = 101). | Correctional institutions, clinical institutions, online advertisements, forum posts and email lists. | GI, impulsivity, empathy, inhibition and laterality. | WAIS-IV, BIS-11, IRI, SIS/SES, EHI. |
| [42] | Germany | Exploratory–comparative Non-probabilistic sampling by convenience | 54 | Middle-aged men 41.00 (ST = 9.00) (PEDs + SOs; n = 15), middle-aged men 38.80 (ST = 10.5) (PEDs + NSOs = 15) and middle-aged men 36.80 (ST = 12.9) (CG; n = 24). | Five penitentiary and clinical institutions, online advertisements, forum posts and email lists. | Intelligence (matrix reasoning, block design), laterality and cognitive empathy. | WAIS-IV, PD, IRI, fMRI. |
| [46] | EEUU | Exploratory–comparative Non-probabilistic sampling by convenience | 60 | Middle-aged men 34.30 (ST = 7.04) (PEDs + SOs; n = 20), middle-aged men 30.85 (ST = 6.32) (NPEDs + SOs; n = 20) and middle-aged men 36.70 (ST = 8.88) (CG; n = 20). | Three penitentiary institutions. | EF: intelligence, behavioral dyscontrol, resistance to interference, visual and auditory memory, and processing and motor speed. | WAIS-III, PIAT, SCWT, RV, RFFT, BDS, WMS-III. |
| [47] | EEUU | Exploratory–comparative Non-probabilistic sampling by convenience | 60 | Middle-aged men 34.15 (ST = 7.60) (PEDs + SOs; n = 20), middle-aged men 31.90 (7.79) (NPEDs + SOs = 20) and middle-aged men 29.70 (ST = 6.0) (CG; n = 20). | Residents in intermediary programs between prison and reintegration. | EF: working memory, processing speed and intelligence. | WAIS-III, SILS, WMS-III, FT, SS, DSC, ITT. |
| [43] | Poland | Exploratory–comparative Non-probabilistic sampling by convenience | 42 | Middle-aged men 43.80 (ST = 8.46) (PEDs + SOs; n = 11), middle-aged men 36.56 (ST = 8.8) (PEDs + NSOs = 14) and middle-aged men 32.24 (ST = 7.85) (CG; n = 17). | Department of Sexology at Nowowiejski Hospital (Warsaw) and social networks. | Emotional interference in cognitive control. | Go/No-Go, fMRI. |
| [44] | United Kingdom, Germany | Exploratory–comparative Non-probabilistic sampling by convenience | 29 | Middle-aged men 43.55 (ST = 11.58) (PEDs + SOs; n = 11), middle-aged men 33.25 (ST = 10.79) (PEDs + NSOs n = 8) and middle-aged men 37.70 (ST = 13.12) (CG; n = 10). | Penitentiary institutions, web page of the study, online forum, flyers and advertisements in public institutions. | Inhibition of interference. | Stroop interference NSIBP, error processing, post error slowing, fMRI |
| Authors and Year | Sample | Results | Limitations |
|---|---|---|---|
| [45] | n = 89 Residents in reintegration and control programs | Higher abstract reasoning is observed in PEDs + SOs and NPEDs + SOs than in NSOs. Lower inhibition is observed in PEDs + SOs and NPEDs + SOs. PEDs + SOs show higher planning and development. PEDs + SOs show two-thirds below average interference, while NPEDs show one-third. | All offenders come from residential treatment programs with an interest in reintegrating into society. There is an insufficient sample size for more sophisticated statistical procedures (structural equations to examine contributing factors). There are poorly paired groups to present different characteristics. There is a lack of sensitivity in tests of executive functions (may detect inadequately). |
| [35] | n = 93 Clinical and control patients | PEDs + SOs show lower attentional control and therefore little interference control (inhibitory functions). PEDs + NSOs show a higher ability of self-control and self-regulation. Sexual interest in minors is the same in the two samples with pedophilic inclination. | A limitation may be the intelligence of ambulatory pedophile individuals as opposed to that of forensic pedophile individuals, with a higher score in ambulatory individuals. This study did not observe significant differences, but influence is not ruled out. The control groups are heterogeneous. |
| [36] | n = 40 Residents in prison and control | In PEDs + SOs, the lowest decrease in RSFC appears in the left medial OFC, followed by PEDs + NSOs and controls. In PEDs + SOs, there is also a decrease in RSFC in the DMPFC and in the rostral and caudal NAc. In addition, decreased connectivity appears in amygdala–OFC interaction. There is also a decreased connectivity of the ITC with the left amygdala. | The differences between PEDs + SOs and NSOs may be due to the age differences between the groups (PEDs + SOs exceeded 15 years in mean age), and, therefore, there may be bias in the comparative samples and lack of control for variables associated with experience It may influence the source of participant recruitment (the impact of age, gender preferences and incarceration). |
| [37] | n = 117 Residents in prison and control | PEDs + SOs show less activation of the medial parietal cortex (left caudal PCC) and the left SFC, and decreased FPCN activity. PEDs + NSOs have a neural mechanism with a compensatory function. Higher inhibitory control is observed in PEDs + NSOs. No differences between groups in the prefrontal area are observed. | Imprisonment may limit executive functions in the sample. |
| [48] | n = 63 Residents in prison and control | In PEDs + SOs, without significant differences with NSOs, a reduction in gray matter appears in the bilateral frontal lobe (premotor area, OFC, frontal pole, inferior frontal junction, DM/DLPFC), the parietal lobe (postcentral gyrus, precuneus medial, inferior and superior parietal lobe), the temporal lobe (inferior temporal, fusiform and parahippocampal gyrus) and the occipital lobe, and also in the bilateral basal ganglia (ventromedial and dorsolateral putamen, ventral caudate, nucleus accumbens, globus pallidus, left dorsal caudate), in the bilateral cerebellum, in the bilateral medial cingulate and in the hippocampus. Less gray matter is observed in the right hemisphere. There is more evidence in SOs than in pedophilia. | Age can be a risk factor (PEDs + SOs greater than PEDs + NSOs). PEDs + NSOs may not be considered SOs due to having been incarcerated before committing the act. There is a limited sample size. The assignment of subjects to each group according to criminological basis and the erroneous assignment of pedophiles (according to the DSM-IV) to the NPED group are limitations. This study does not include PEDs + NSOs. |
| [49] | n = 283 Residents in clinic and in prison and control | PEDs + SOs show reductions in cortical SA, white matter FA and CT. A lower SA is observed in the left CPF and right superior frontal cortex. Lower inhibitory control is observed in PEDs + SOs. The left DLPFC is uncoupled in a frontoparietal network in PEDs + SOs, which may indicate disinhibition. | Cortical mediation is a secondary statistical model; it may not be reliable. The sample differs in age and is strongly related to structural neuroimaging phenotypes. There is a reduced sample in neuroimaging studies. No “dose effect” is observed where the PED + NSO group is intermediary between PEDs + SOs and the CG. Cognitive function is not analyzed, so the components cannot be specified. |
| [50] | n = 158 Residents in prison and control | Less impulse control is observed in PEDs + SOs and NPEDs + SOs. PEDs + SOs show higher cognitive flexibility and change of scene. NPEDs + SOs show a lower capacity for the strategic use of working memory. Increasing age is associated with reduced response inhibition abilities (but no differences from the CG). | Imprisonment can be a limitation in the analysis of cognitive and executive functioning. There are possible confounding effects between psychiatric comorbidities and educational level. There is a lack of use of instruments for the diagnosis of sexual preference. The cross-sectional design does not allow us to clarify the impact of age on impulsivity and the onset of criminal behavior. |
| [38] | n = 61 Residents in prison and control | PEDs + SOs have less response inhibition. There are no differences between PEDs + SOs and PEDs + NSOs in behavioral self-control. Error-related positivity (PE) is greatly reduced in PEDs + SOs. | It is unclear whether criminal history and cognitive functioning co-vary. The sample is small and homogeneous (they do not differ in different pedophile behaviors). |
| [39] | n = 62 Residents in clinic and in prison and control | Deficits in errors in working memory are observed in PEDs + SOs. There is an observed correlation between pedophilia and low IQ. PEDs + NSOs exhibit less cognitive distortion, take less risks and are less prone to interference than PEDs + SOs. | The sample size is reduced. The absence of neuropsychological differences between SOs and the CG may be due to the influence of psychological factor such as low levels of antisociality (also associated with reduced levels of spatial intelligence. This study does not include PEDs + NSOs. |
| [40] | n = 63 Residents in prison and control | A dysfunction in response inhibition is observed in PEDs + SOs and NPEDs + SOs (OFC). NPEDs + SOs show little impulsivity and more time in taking tests. PEDs + SOs show higher perseverance and reactive cognitive flexibility. There are no significant differences between the groups in spontaneous cognitive flexibility. NPEDs + SOs show deficits in verbal memory performance. | Non-significant results comparing two groups may be biased by a lack of rigor in the post-hoc analysis (Bonferroni). The sample size is reduced. |
| [41] | n = 219 Residents in clinic and in prison and control | PEDs + SOs show a decrease in gray matter volume in the right temporal lobe compared to NPEDs + SOs. PEDs + SOs show a lower gray matter volume in the dorsomedial PFC and ACC. There are no gray matter differences between the groups in the right amygdala. | The cross-sectional design does not allow us to see causal explanations or predictions in the groups. There is a potential for social desirability bias in the PED + NSO sample (although there are clear differences, indicating that bias is low). |
| [42] | n = 54 Residents in clinic and in prison and control | Altered cognitive empathy neural processing is observed in PEDs + NSOs. Higher activation in the left NAc is observed. Higher activation in the STG is observed in PEDs + NSOs than in PEDs + SOs. | There are no correlations between behavior and brain activation between groups. It may be important to target the scanner’s task in activation rather than sensitivity. There is a possibility of social desirability bias in PEDs + NSOs (denying their status as SOs). There is no association between Pcu deactivation and PD level. A total of 2.7% of the correlations are above 0.50. The sample size is reduced. The cross-sectional design avoids future inferences. |
| [46] | n = 60 Residents in prison and control | Both PEDs and NPEDs show deficits in learning difficulties. PEDs + SOs show lower performance in information processing speed. NPEDs + SOs show lower performance in semantic knowledge and greater impulsivity. | There are errors in the analysis of the profiles in various neurocognitive domains, in the analysis of the reliability of the measures and in the differences between PEDs and NPEDs. Significant differences are not guaranteed by standard scores. There is a small sample size and a lack of rigorous definition of the groups. The results on FEs may be biased by the presence of general delinquent behavior and a low schooling level. |
| [47] | n = 60 Resident in reintegration and control programs | PEDs + SOs exhibit slower visual perception and visuomotor integration (lower processing speed) due to abnormalities in the white matter of the fronto-occipital fascicle [21]. | The findings do not include cognitive elements in conjunction with neuroimaging. Biomarkers cannot be isolated from pedophilia alone. The sample size is reduced. There are differences between the groups, but no further information on this is provided. There is a ceiling and floor effect on some tasks (scores contrary to expectations). This study only examines visuo-perceptual processing speed. |
| [43] | n = 42 Clinical patients and control | PEDs + SOs show behavioral and neural abnormality during emotional interference in cognitive control (higher interference). PEDs + SOs show a decrease in the activity of the right DLPFC, with higher activity in PEDs + NSOs and the CG. There are no differences in cognitive control between SOs and the CG. | The sample size is reduced. Effects may be caused by a lower reactivity to emotional stimuli. There is subjective image evaluation. |
| [44] | n = 29 Residents in prison and control | PEDs + SOs show higher Stroop interference and a greater response time than NSOs and the CG (lower processing speed) due to the activation of the angular gyrus, left angular gyrus and cerebellum. PEDs + SOs have less inhibitory control of interference than NSOs (hyperactivation in the left SPL and precentral gyrus/SMG). PEDs + NSOs show higher activity in the left IFG, posterior cingulate, precuneus and medial temporal gyrus than PEDs + SOs. PEDs differ from the CG in their lack of error awareness. | The sample size is reduced. There is difficulty in differentiating criminal and non-criminal pedophiles. The effects of fMRI analysis with a uncorrected height threshold <0.001 may give false positives. |
| Executive Functions | Pedophile | Non-Pedophile | ||
|---|---|---|---|---|
| SO | NSO | SO | NSO (CG) | |
| Abstract Reasoning | High | Regular | High | Regular |
| Inhibition of Response (Control) | Low | High | Low | Regular |
| Attentional Control | Low | Regular | Low | Regular |
| Processing Speed | Low | Regular | Regular | Regular |
| Semantic Performance | Regular | Regular | Low | Regular |
| Self-Control/Self-Regulation | Low | High | Low | Regular |
| Social and Emotional Cognition | Low | High | Low | Regular |
| Cognitive Flexibility, Perseverance and Set-Shifting | High | Regular | Low | Regular |
| Working Memory | Low | Regular | Low | Regular |
| Cognitive Distortion | High | Low | Regular | Regular |
| Awareness of Error (Risk Assumption) | Low | High | Low | Regular |
| Neuroanatomical Structures | Pedophilic | Non-Pedophilic | ||
|---|---|---|---|---|
| SO | NSO | SO | NSO (CG) | |
| Left lower amygdala of temporal cortex, dorsal–medial prefrontal cortex, left upper frontal cortex, left caudal posterior cingulate cortex and frontoparietal control network | Low activity | Regular | Low activity | Regular |
| Superior parietal lobe and supramarginal gyrus | High activity | Low activity | Regular | Regular |
| Connectivity in amygdala–orbitofrontal cortex interaction | Low connectivity | Regular | Low connectivity | Regular |
| Temporal gyrus | Regular | Low activity | Regular | Regular |
| Angular gyrus and cerebellum | ||||
| Nucleus accumbens | Low activity | High activity | Low activity | Regular |
| Gray matter (*) | Reduction | Regular | Regular | Regular |
| White matter (**) | Reduction | Regular | Regular | Regular |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ara-García, Y.; Martí-Vilar, M.; Badenes-Ribera, L.; González-Sala, F. Neuroanatomical and Neurocognitive Differences Between the Executive Functions in Child Sexual Offenders: A Systematic Review. Brain Sci. 2025, 15, 38. https://doi.org/10.3390/brainsci15010038
Ara-García Y, Martí-Vilar M, Badenes-Ribera L, González-Sala F. Neuroanatomical and Neurocognitive Differences Between the Executive Functions in Child Sexual Offenders: A Systematic Review. Brain Sciences. 2025; 15(1):38. https://doi.org/10.3390/brainsci15010038
Chicago/Turabian StyleAra-García, Yaiza, Manuel Martí-Vilar, Laura Badenes-Ribera, and Francisco González-Sala. 2025. "Neuroanatomical and Neurocognitive Differences Between the Executive Functions in Child Sexual Offenders: A Systematic Review" Brain Sciences 15, no. 1: 38. https://doi.org/10.3390/brainsci15010038
APA StyleAra-García, Y., Martí-Vilar, M., Badenes-Ribera, L., & González-Sala, F. (2025). Neuroanatomical and Neurocognitive Differences Between the Executive Functions in Child Sexual Offenders: A Systematic Review. Brain Sciences, 15(1), 38. https://doi.org/10.3390/brainsci15010038