
A Retrospective Analysis of Temporal Lobe Gliosis after Middle Fossa Resection of Small Vestibular Schwannomas

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Data
2.2. Surgery
2.3. Imaging
2.4. Predictors
2.5. Statistics
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Monfared, A.; Mudry, A.; Jackler, R. The history of middle cranial fossa approach to the cerebellopontine angle. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2010, 31, 691–696. [Google Scholar] [CrossRef]
- House, W.F. Surgical exposure of the internal auditory canal and its contents through the middle, cranial fossa. Laryngoscope 1961, 71, 1363–1385. [Google Scholar] [CrossRef]
- Fisch, U. Transtemporal extralabyrinthine surgery of the internal auditory canal. Arch. Klin. Exp. Ohren Nasen Kehlkopfheilkd. 1969, 194, 232–243. [Google Scholar] [CrossRef]
- Brackmann, D.E.; House, J.R., 3rd; Hitselberger, W.E. Technical modifications to the middle fossa craniotomy approach in removal of acoustic neuromas. Am. J. Otol. 1994, 15, 614–619. [Google Scholar]
- Ren, Y.; Merna, C.M.; Tawfik, K.O.; Schwartz, M.S.; Friedman, R.A. Auditory Brain Stem Response Predictors of Hearing Outcomes after Middle Fossa Resection of Vestibular Schwannomas. J. Neurol. Surg. B Skull Base 2022, 83, 496–504. [Google Scholar] [CrossRef]
- Budohoski, K.P.; Rennert, R.C.; Gordon, S.A.; Raheja, A.; Brandon, C.; Henson, J.C.; Azab, M.A.; Patel, N.S.; Karsy, M.; Gurgel, R.K.; et al. Factors associated with hearing outcomes after a middle fossa approach in 131 consecutive patients with vestibular schwannomas. J. Neurosurg. 2022, 139, 432–441. [Google Scholar] [CrossRef]
- Ginzkey, C.; Scheich, M.; Harnisch, W.; Bonn, V.; Ehrmann-Müller, D.; Shehata-Dieler, W.; Mlynski, R.; Hagen, R. Outcome on hearing and facial nerve function in microsurgical treatment of small vestibular schwannoma via the middle cranial fossa approach. Eur. Arch. Otorhinolaryngol. 2013, 270, 1209–1216. [Google Scholar] [CrossRef]
- Scheich, M.; Ginzkey, C.; Ehrmann-Müller, D.; Shehata Dieler, W.; Hagen, R. Complications of the Middle Cranial Fossa Approach for Acoustic Neuroma Removal. J. Int. Adv. Otol. 2017, 13, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Koos, W.T.; Day, J.D.; Matula, C.; Levy, D.I. Neurotopographic considerations in the microsurgical treatment of small acoustic neurinomas. J. Neurosurg. 1998, 88, 506–512. [Google Scholar] [CrossRef] [PubMed]
- Concheri, S.; Deretti, A.; Tealdo, G.; Zanoletti, E. Prognostic Factors for Hearing Preservation Surgery in Small Vestibular Schwannoma. Audiol. Res. 2023, 13, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Schick, B.; Greess, H.; Gill, S.; Pauli, E.; Iro, H. Magnetic resonance imaging and neuropsychological testing after middle fossa vestibular schwannoma surgery. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2008, 29, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Brors, D.; Schäfers, M.; Bodmer, D.; Draf, W.; Kahle, G.; Schick, B. Postoperative magnetic resonance imaging findings after transtemporal and translabyrinthine vestibular schwannoma resection. Laryngoscope 2003, 113, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Minovi, A.; Mangold, R.; Kollert, M.; Hofmann, E.; Draf, W.; Bockmühl, U. Functional results, cognitive and effective quality of life disturbances after trans-temporal resection of acoustic neuroma. Laryngo-Rhino-Otol. 2005, 84, 915–920. [Google Scholar] [CrossRef]
- Burda, J.E.; Sofroniew, M.V. Reactive gliosis and the multicellular response to CNS damage and disease. Neuron 2014, 81, 229–248. [Google Scholar] [CrossRef] [PubMed]
- Pekny, M.; Pekna, M. Reactive gliosis in the pathogenesis of CNS diseases. Biochim. Biophys. Acta 2016, 1862, 483–491. [Google Scholar] [CrossRef]
- Scheich, M.; Hagen, R. The middle cranial fossa approach. In Surgery of the Lateral Skull Base: A 50-Year Endeavour; Zanoletti, E., Mazzoni, A., Martini, A., Eds.; ACTA Otorhinolaryngologica Italica: Brescia, Italy, 2019; Volume 39, Supply S1; pp. S11–S14. [Google Scholar]
- Kashani, R.G.; Kocharyan, A.; Claussen, A.D.; Gantz, B.J.; Hansen, M.R. Middle Cranial Fossa Approach for Sporadic Vestibular Schwannoma: Patient Selection, Technical Pearls, and Hearing Results. Otolaryngol. Clin. N. Am. 2023, 56, 495–507. [Google Scholar] [CrossRef]
- Silk, P.S.; Lane, J.I.; Driscoll, C.L. Surgical approaches to vestibular schwannomas: What the radiologist needs to know. Radiographics 2009, 29, 1955–1970. [Google Scholar] [CrossRef]
- Yang, J.X.; Aygun, N.; Nadgir, R.N. Imaging of the Postoperative Skull Base and Cerebellopontine Angle. Neuroimaging Clin. N. Am. 2022, 32, 159–174. [Google Scholar] [CrossRef]
- Ginat, D.T.; Martuza, R.L. Postoperative imaging of vestibular schwannomas. Neurosurg. Focus 2012, 33, E18. [Google Scholar] [CrossRef]
- Bennett, M.L.; Jackson, C.G.; Kaufmann, R.; Warren, F. Postoperative imaging of vestibular schwannomas. Otolaryngol. Head. Neck Surg. 2008, 138, 667–671. [Google Scholar] [CrossRef]
- Mueller, D.P.; Gantz, B.J.; Dolan, K.D. Gadolinium-enhanced MR of the postoperative internal auditory canal following acoustic neuroma resection via the middle fossa approach. AJNR Am. J. Neuroradiol. 1992, 13, 197–200. [Google Scholar]
- Stripf, T.; Bruehl, K.; Mann, W.J.; Amedee, R.G. Clinical and radiologic sequelae of the middle fossa approach to the internal auditory canal. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2004, 25, 787–790. [Google Scholar] [CrossRef] [PubMed]
- Gjuric, M.; Wigand, M.E.; Wolf, S.R. Enlarged middle fossa vestibular schwannoma surgery: Experience with 735 cases. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2001, 22, 223–230; discussion 230–221. [Google Scholar] [CrossRef]
- Wigand, M.E.; Haid, T.; Berg, M.; Schuster, B.; Goertzen, W. Extended middle cranial fossa approach for acoustic neuroma surgery. Skull Base Surg. 1991, 1, 183–187. [Google Scholar] [CrossRef]
- Zwirner, J.; Scholze, M.; Waddell, J.N.; Ondruschka, B.; Hammer, N. Mechanical Properties of Human Dura Mater in Tension—An Analysis at an Age Range of 2 to 94 Years. Sci. Rep. 2019, 9, 16655. [Google Scholar] [CrossRef] [PubMed]
- Karibe, H.; Hayashi, T.; Narisawa, A.; Kameyama, M.; Nakagawa, A.; Tominaga, T. Clinical Characteristics and Outcome in Elderly Patients with Traumatic Brain Injury: For Establishment of Management Strategy. Neurol. Med. Chir. 2017, 57, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Saliba, J.; Mohammadzadeh, A.; Tawfik, K.O.; Carriere, J.S.; Schwartz, M.S.; Nguyen, Q.T.; Friedman, R.A. The Direct Costs of Microsurgical Resection of Vestibular Schwannomas. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2020, 41, 397–402. [Google Scholar] [CrossRef]
- Raghavan, A.M.; Lipschitz, N.; Kohlberg, G.D.; Samy, R.N.; Zuccarello, M.; Pensak, M.L.; Breen, J.T. Is Longer Surgery More Dangerous? Operative Duration Not Associated With Complications After Vestibular Schwannoma Resection. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2020, 41, e268–e272. [Google Scholar] [CrossRef]
- Sameshima, T.; Fukushima, T.; McElveen, J.T., Jr.; Friedman, A.H. Critical assessment of operative approaches for hearing preservation in small acoustic neuroma surgery: Retrosigmoid vs middle fossa approach. Neurosurgery 2010, 67, 640–644; discussion 644–645. [Google Scholar] [CrossRef]
- Scheich, M.; Ginzkey, C.; Harnisch, W.; Ehrmann, D.; Shehata-Dieler, W.; Hagen, R. Use of flexible CO2 laser fiber in microsurgery for vestibular schwannoma via the middle cranial fossa approach. Eur. Arch. Otorhinolaryngol. 2012, 269, 1417–1423. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| none (0) | |
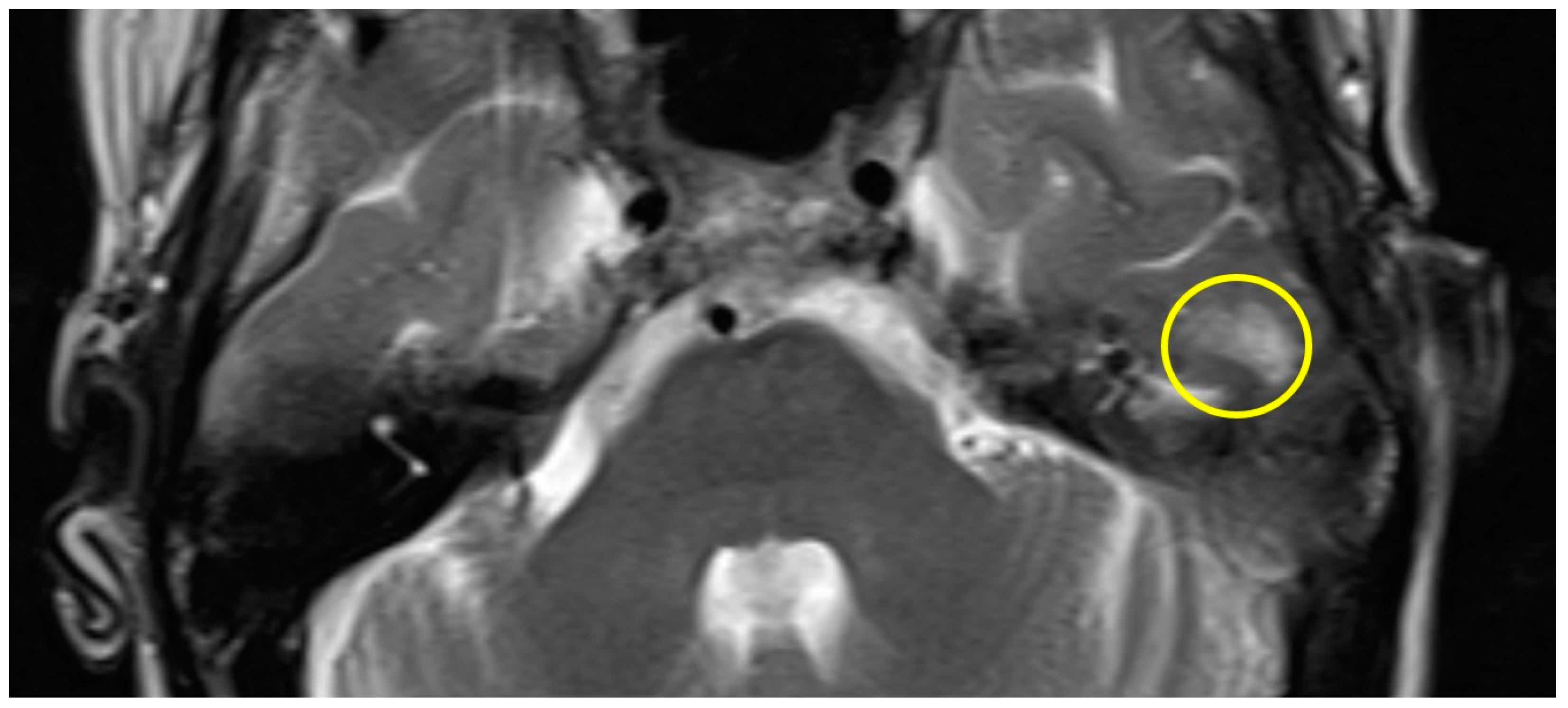
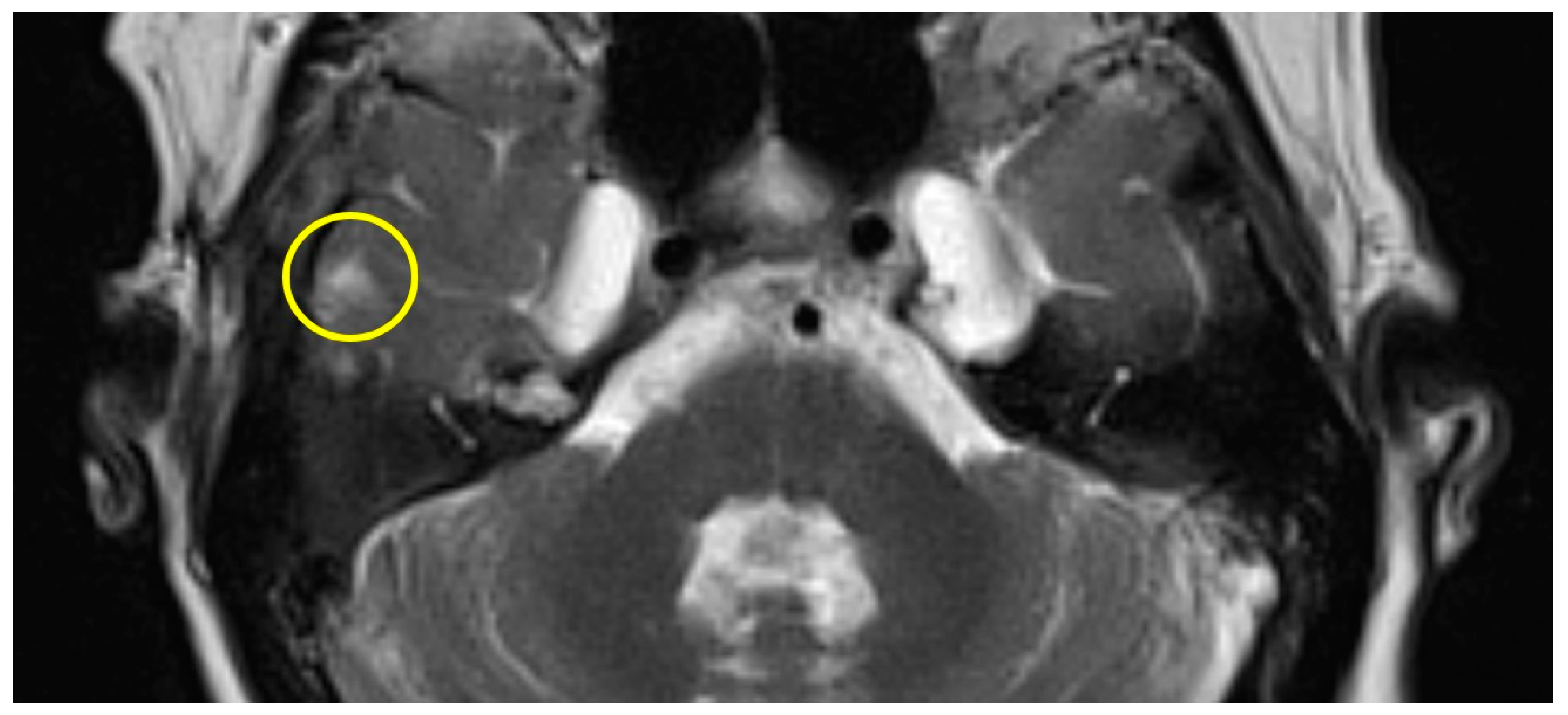
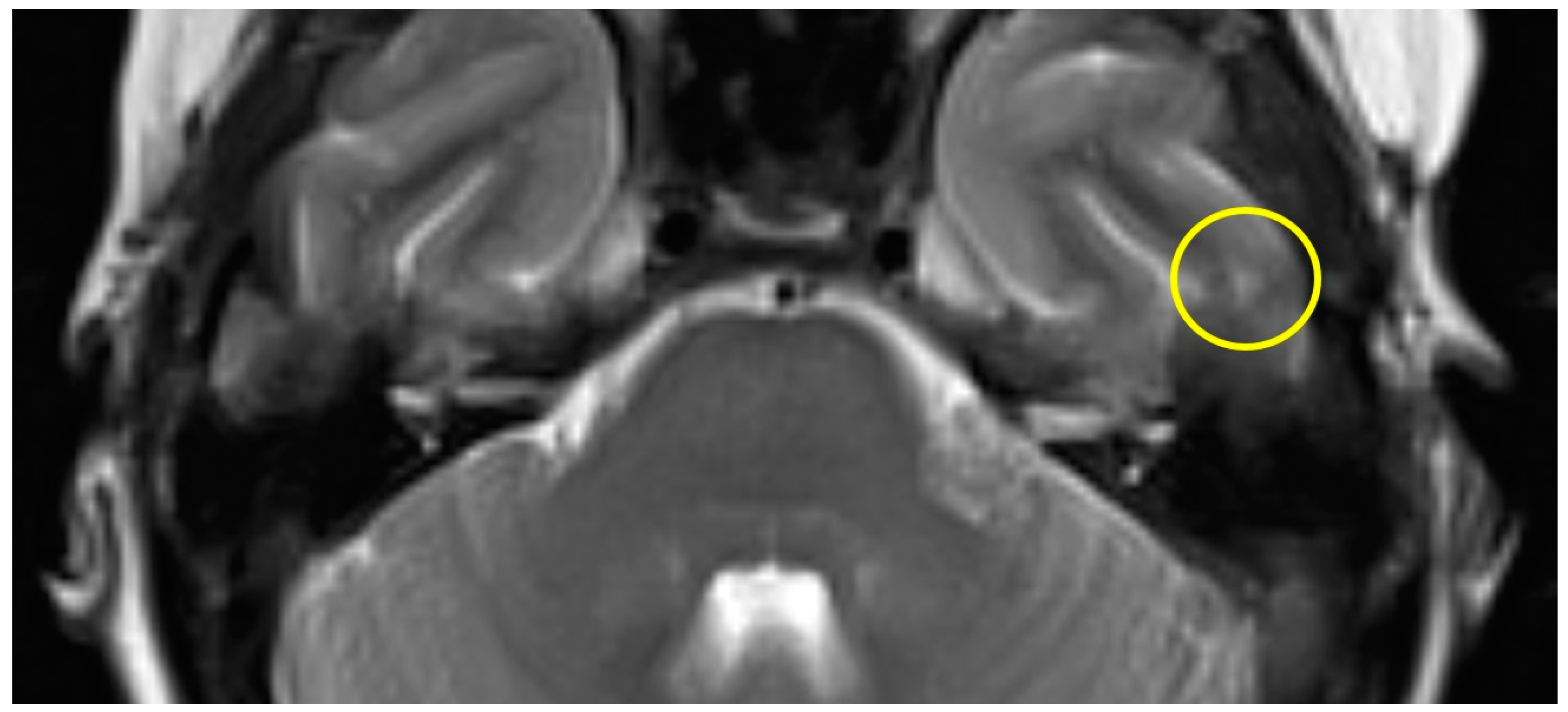
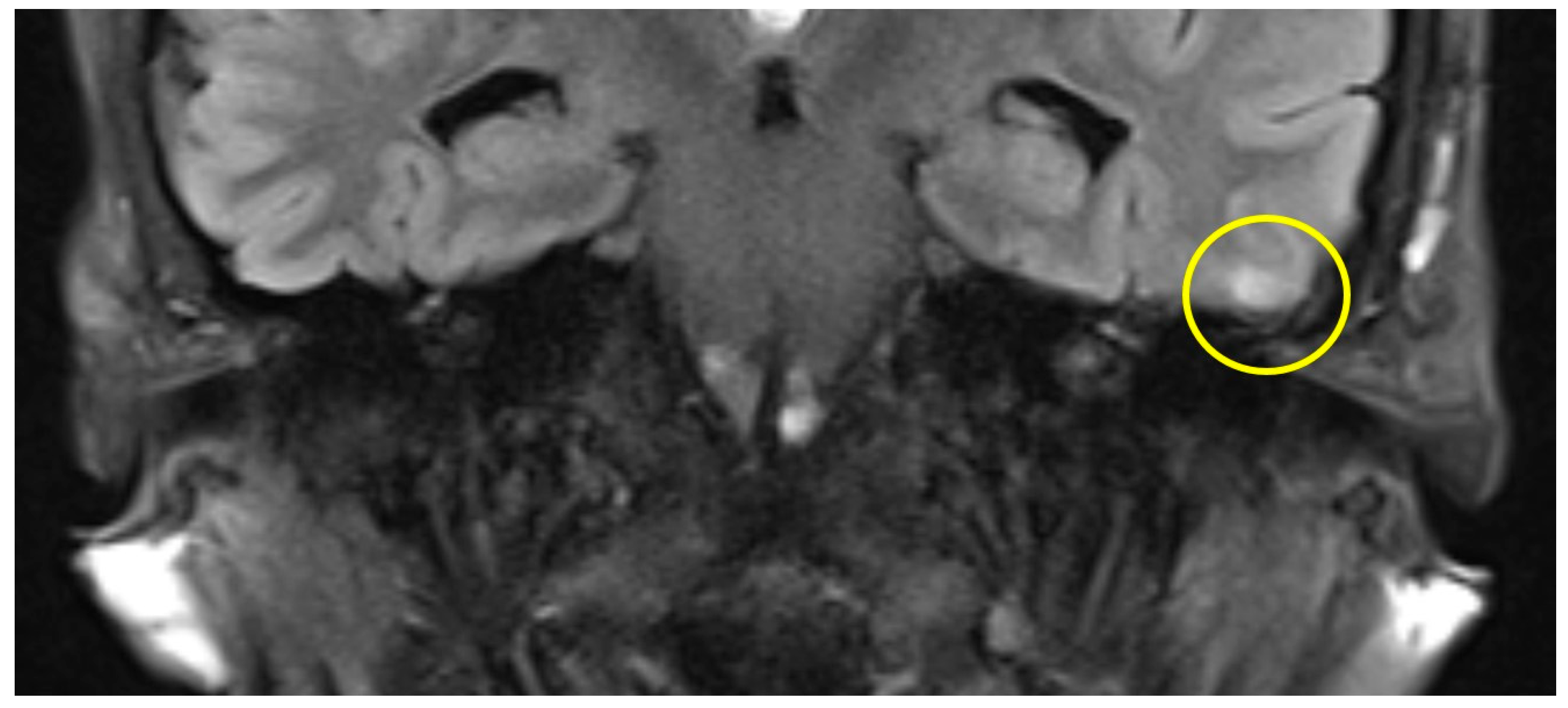
| slight (1) | parts of the inferior temporal gyrus, less than half of the thickness (cranial-caudal) |
| moderate (2) | further parts of the inferior temporal gyrus |
| severe (3) | more than one gyrus |
| Tumor Stage | Sex | Age | Laterality | Time Interval between Surgery and MRI | Incision-to-Closure Time | Extent of Gliosis | |
|---|---|---|---|---|---|---|---|
| Patient #1 | T2 | f | 58 | left | 12 months | 175 min | slight |
| Patient #2 | T2 | f | 62 | right | 16 months | 159 min | slight |
| Patient #3 | T2 | f | 57 | left | 11 months | 131 min | slight |
| Patient #4 | T1 | f | 49 | left | 12 months | 159 min | slight |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scheich, M.; Bürklein, M.; Stöth, M.; Bison, B.; Hagen, R.; Hackenberg, S.; Vogt, M.L. A Retrospective Analysis of Temporal Lobe Gliosis after Middle Fossa Resection of Small Vestibular Schwannomas. Brain Sci. 2024, 14, 295. https://doi.org/10.3390/brainsci14030295
Scheich M, Bürklein M, Stöth M, Bison B, Hagen R, Hackenberg S, Vogt ML. A Retrospective Analysis of Temporal Lobe Gliosis after Middle Fossa Resection of Small Vestibular Schwannomas. Brain Sciences. 2024; 14(3):295. https://doi.org/10.3390/brainsci14030295
Chicago/Turabian StyleScheich, Matthias, Miriam Bürklein, Manuel Stöth, Brigitte Bison, Rudolf Hagen, Stephan Hackenberg, and Marius L. Vogt. 2024. "A Retrospective Analysis of Temporal Lobe Gliosis after Middle Fossa Resection of Small Vestibular Schwannomas" Brain Sciences 14, no. 3: 295. https://doi.org/10.3390/brainsci14030295
APA StyleScheich, M., Bürklein, M., Stöth, M., Bison, B., Hagen, R., Hackenberg, S., & Vogt, M. L. (2024). A Retrospective Analysis of Temporal Lobe Gliosis after Middle Fossa Resection of Small Vestibular Schwannomas. Brain Sciences, 14(3), 295. https://doi.org/10.3390/brainsci14030295