
Usefulness and Clinical Impact of Whole-Body MRI in Detecting Autoimmune Neuromuscular Disorders

 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
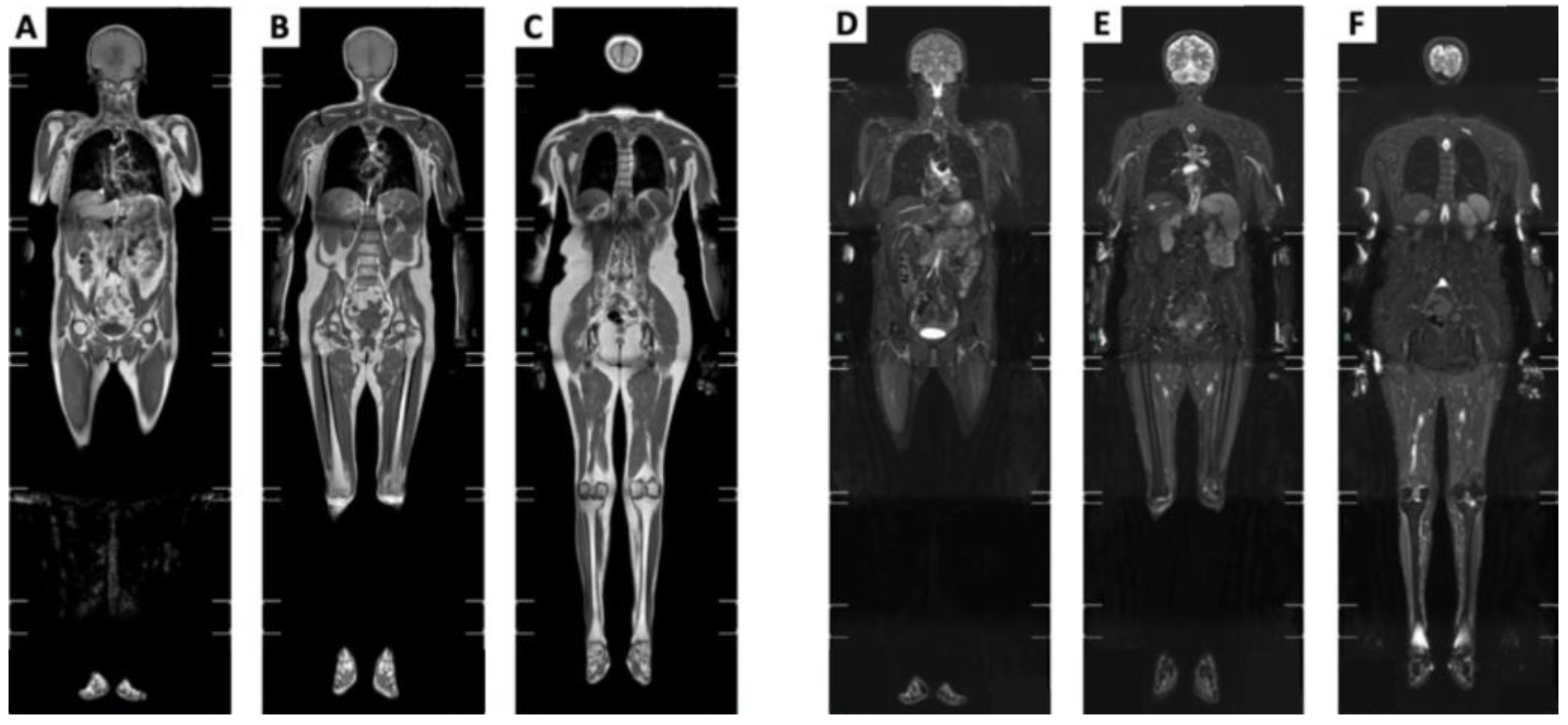
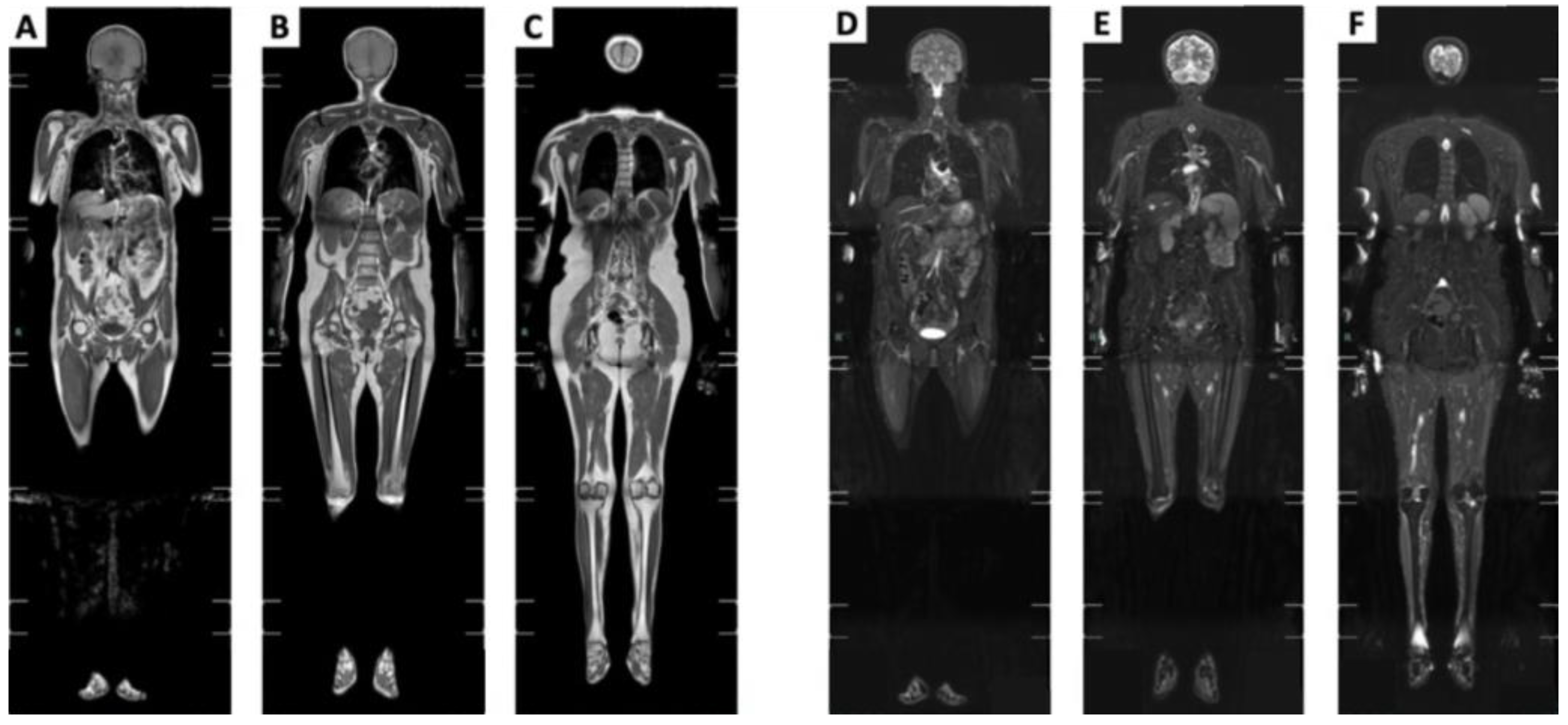
2. MRI Whole-Body Protocols
3. Whole-Body MRI: Qualitative Assessment
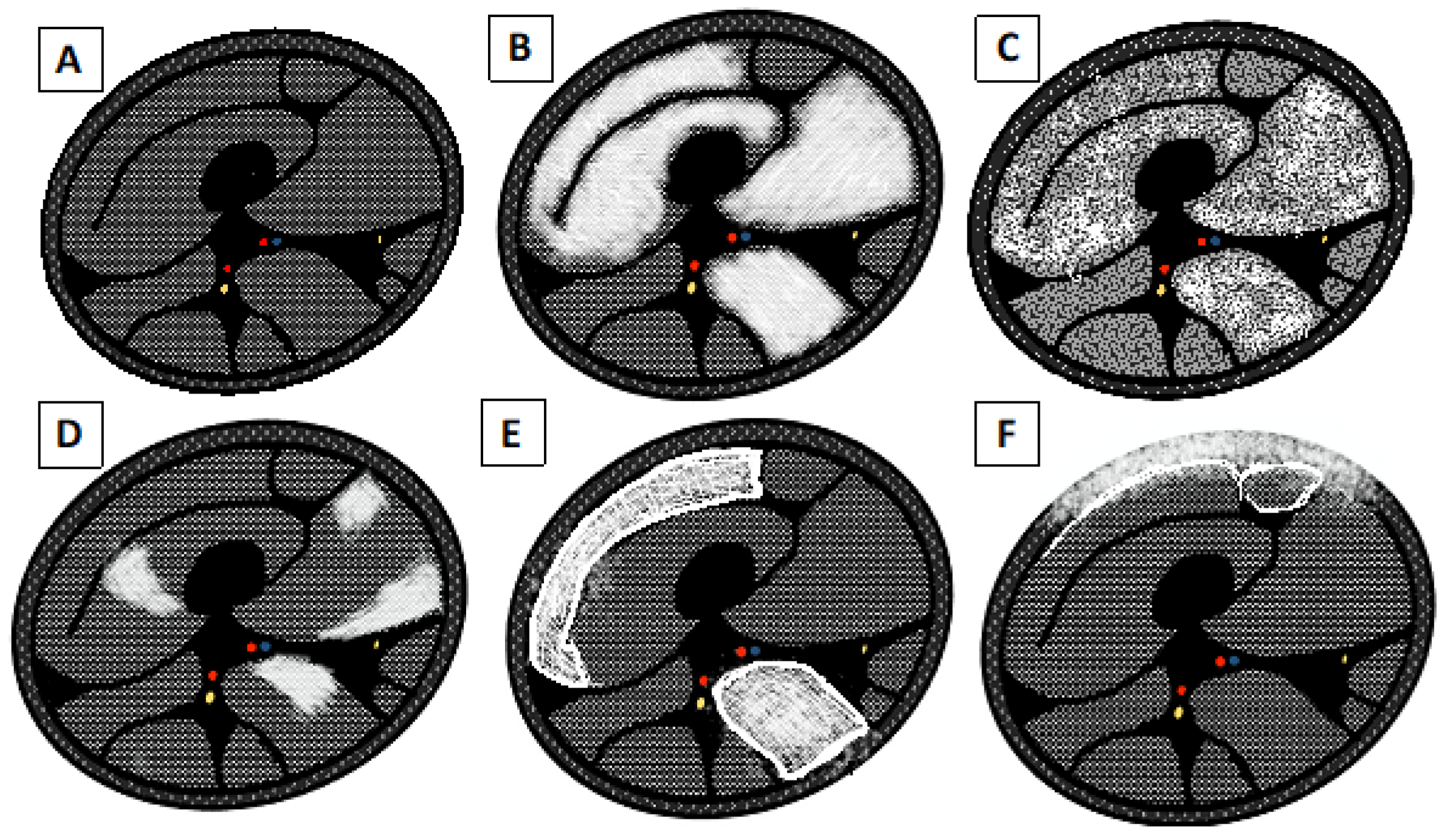
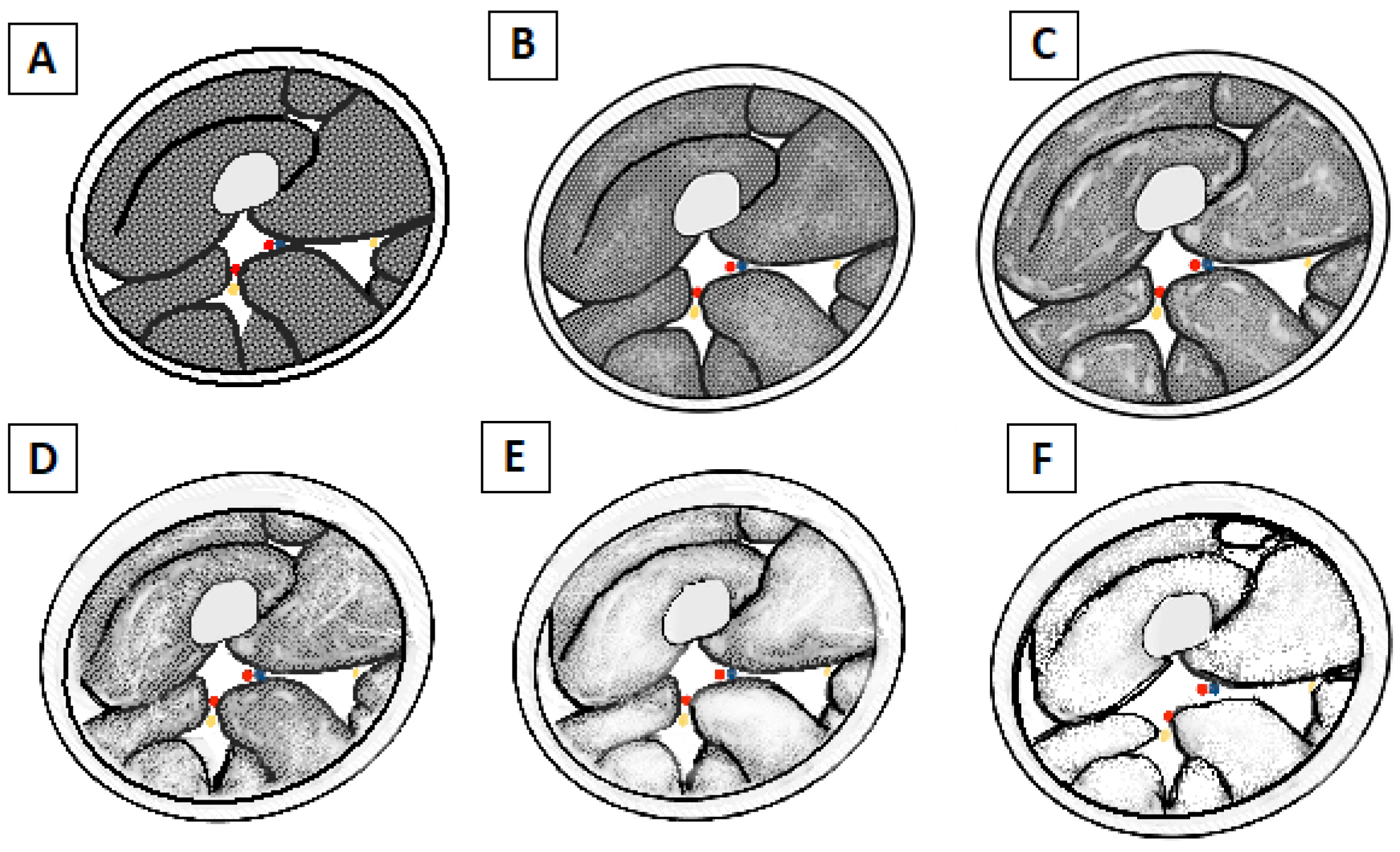
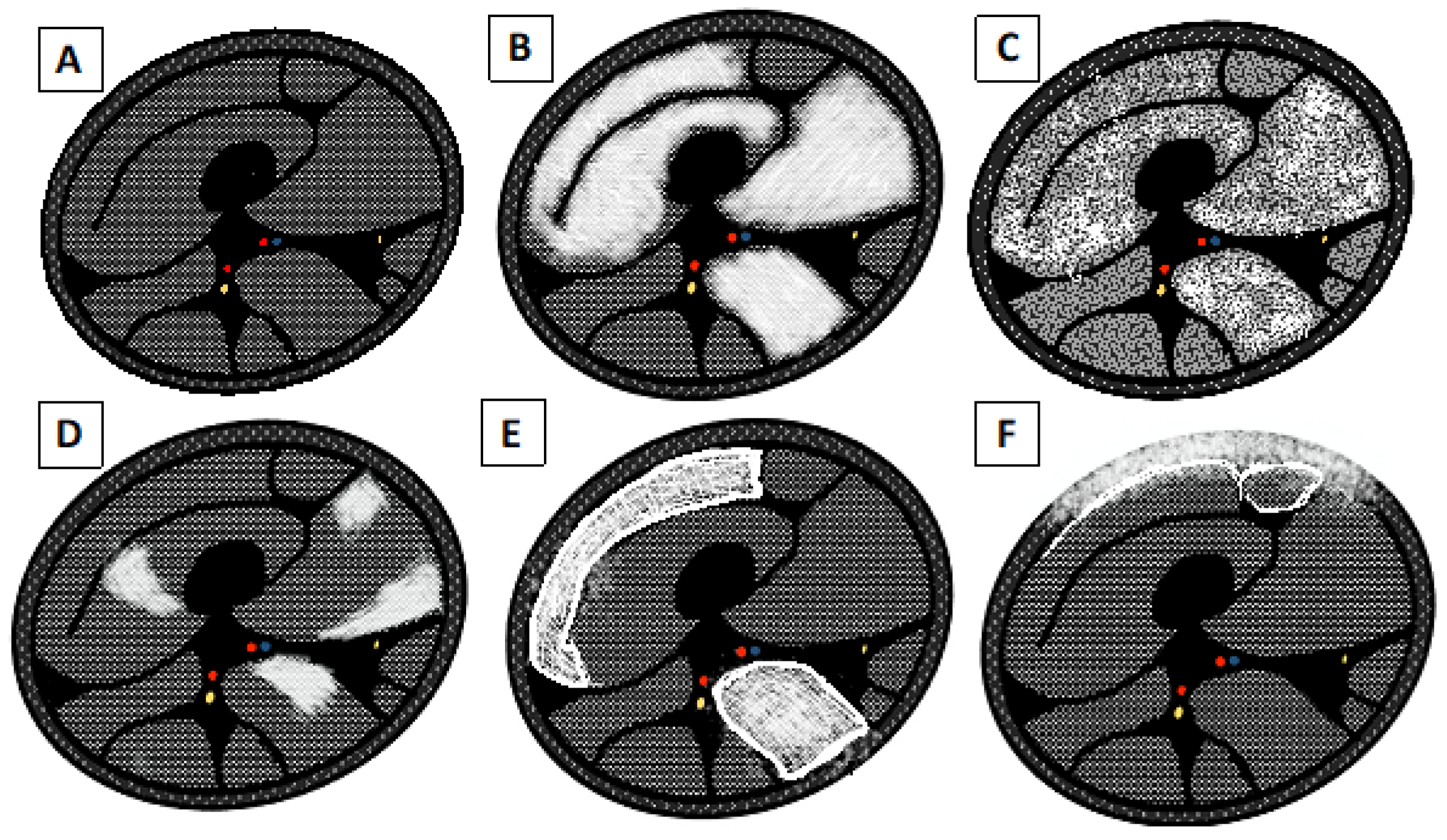
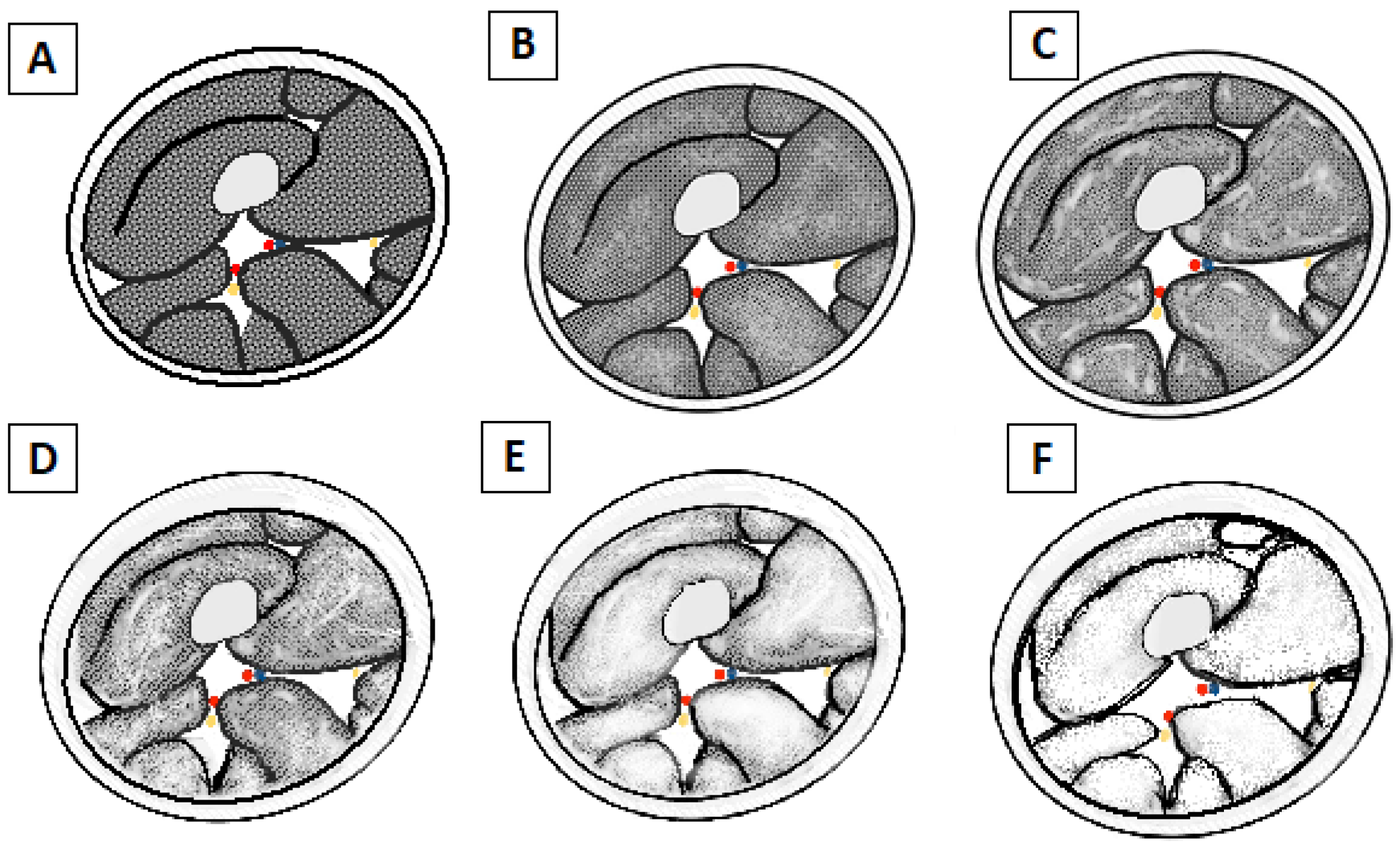
3.1. Distinction between Active and Chronic Disease
3.1.1. Acute Changes
- 0 = Normal muscle intensity;
- 1 = Mild hyperintensity;
- 2 = Definite hyperintensity.
3.1.2. Chronic Changes
- 0 = Normal intensity appearance of the muscle.
- 1 = Early moth-eaten appearance with scattered small areas of high intensity on T1-weighted imaging.
- 2a = Late moth-eaten appearance, with numerous areas of high intensity on T1-weighted imaging, with beginning confluence comprising less than 30%.
- 2b = Late moth-eaten appearance, with numerous areas of high intensity on T1-weighted imaging, with beginning confluence comprising 30–60%.
- 3 = Washed-out, fuzzy appearance due to confluent areas of increased intensity in T1-weighted imaging, with muscle still present at the periphery.
- 4 = End-stage appearance; all muscle replaced by fat with high intensity in T1-weighted.
3.2. Biomarker for the Evaluation of the Treatment and Follow-Up (Quantitative Assessment)
4. Whole-Body MRI in Inflammatory Neuromuscular Disease
4.1. Guillan–Barré Syndrome
4.2. Chronic Inflammatory Demyelinating Polyneuropathy
4.3. Myasthenia Gravis
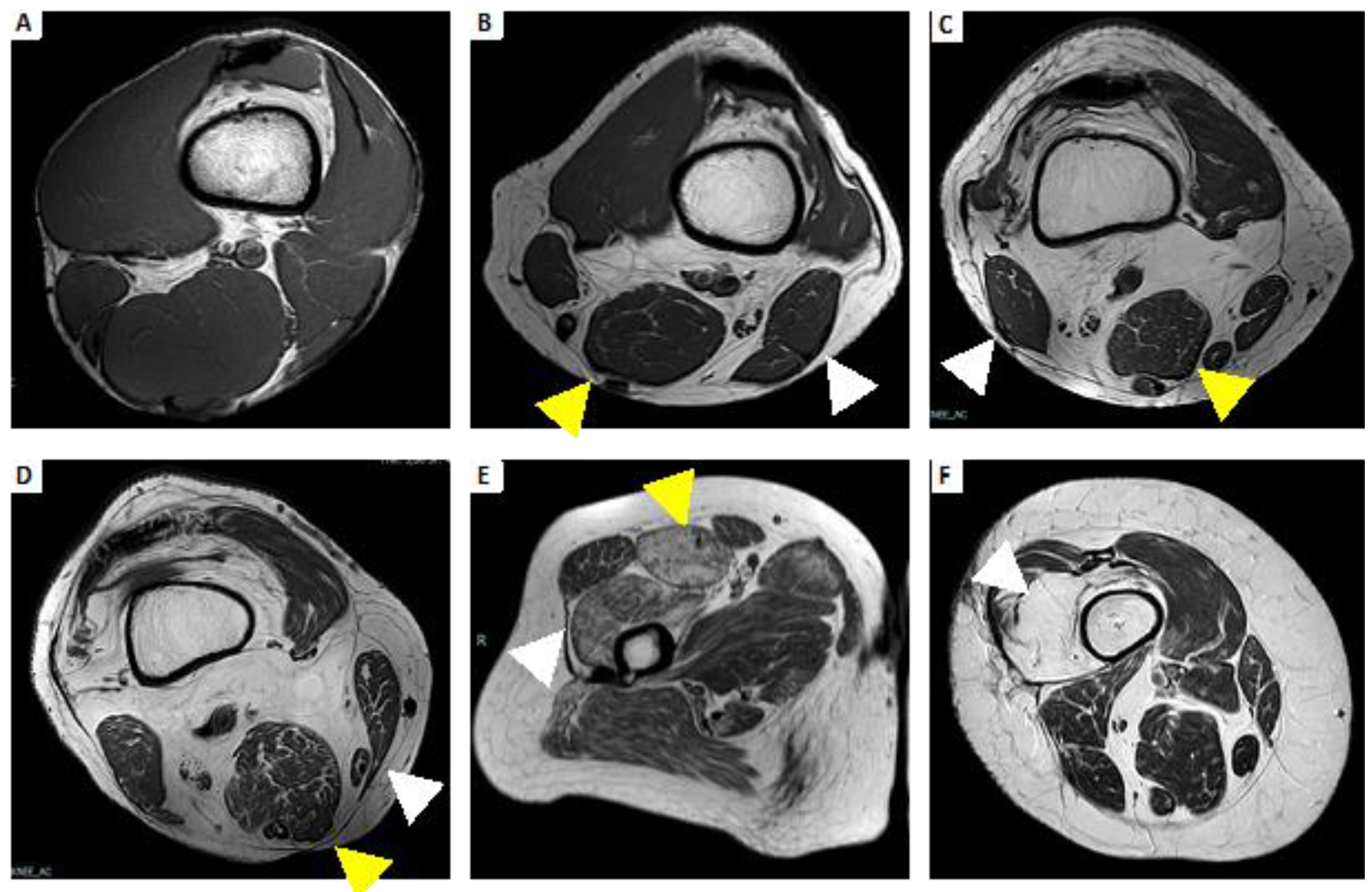
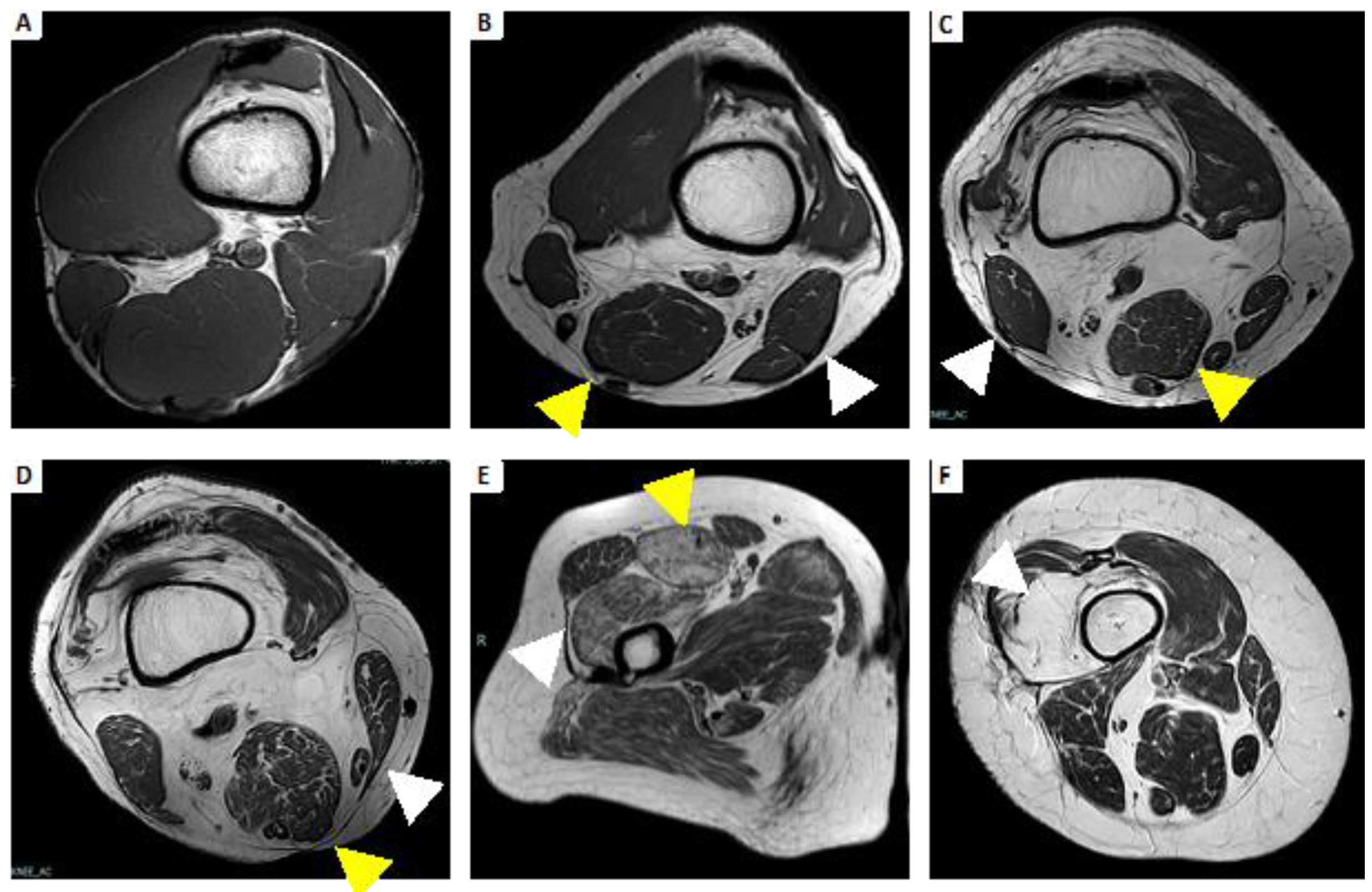
4.4. Idiopathic Inflammatory Myopathies
4.4.1. Dermatomyositis
4.4.2. Polymyositis
4.4.3. Inclusion Body Myositis
4.4.4. Immune-Mediated Necrotizing Myopathy
4.4.5. Focal Myositis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mäurer, M.; Toyka, K.V.; Gold, R. Immune mechanisms in acquired demyelinating neuropathies: Lessons from animal models. Neuromuscul. Disord. 2002, 12, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Punga, A.R.; Maddison, P.; Heckmann, J.M.; Guptill, J.T.; Evoli, A. Epidemiology, diagnostics, and biomarkers of autoimmune neuromuscular junction disorders. Lancet Neurol. 2022, 21, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, I.E.; Fujimoto, M.; Vencovsky, J.; Aggarwal, R.; Holmqvist, M.; Christopher-Stine, L.; Mammen, A.L.; Miller, F.W. Idiopathic inflammatory myopathies. Nat. Rev. Dis. Prim. 2021, 7, 86. [Google Scholar] [CrossRef] [PubMed]
- Chitnis, T.; Khoury, S.J. Immunologic neuromuscular disorders. J. Allergy Clin. Immunol. 2003, 111, S659–S668. [Google Scholar] [CrossRef]
- Wattjes, M.P.; Kley, R.A.; Fischer, D. Neuromuscular imaging in inherited muscle diseases. Eur. Radiol. 2010, 20, 2447–2460. [Google Scholar] [CrossRef]
- Schulze, M.; Kötter, I.; Ernemann, U.; Fenchel, M.; Tzaribatchev, N.; Claussen, C.D.; Horger, M. MRI Findings in Inflammatory Muscle Diseases and Their Noninflammatory Mimics. Am. J. Roentgenol. 2009, 192, 1708–1716. [Google Scholar] [CrossRef]
- Lichtenstein, T.; Sprenger, A.; Weiss, K.; Slebocki, K.; Cervantes, B.; Karampinos, D.; Maintz, D.; Fink, G.R.; Henning, T.D.; Lehmann, H.C. MRI biomarkers of proximal nerve injury in CIDP. Ann. Clin. Transl. Neurol. 2018, 5, 19–28. [Google Scholar] [CrossRef]
- Malartre, S.; Bachasson, D.; Mercy, G.; Sarkis, E.; Anquetil, C.; Benveniste, O.; Allenbach, Y. MRI and muscle imaging for idiopathic inflammatory myopathies. Brain Pathol. 2021, 31, e12954. [Google Scholar] [CrossRef]
- Van De Vlekkert, J.; Maas, M.; Hoogendijk, J.E.; De Visser, M.; Van Schaik, I.N. Combining MRI and muscle biopsy improves diagnostic accuracy in subacute-onset idiopathic inflammatory myopathy. Muscle Nerve 2015, 51, 253–258. [Google Scholar] [CrossRef]
- Fujino, H.; Kobayashi, T.; Goto, I.; Onitsuka, H. Magnetic resonance imaging of the muscles in patients with polymyositis and dermatomyositis. Muscle Nerve 1991, 14, 716–720. [Google Scholar] [CrossRef]
- Quijano-Roy, S.; Avila-Smirnow, D.; Carlier, R.Y. Whole body muscle MRI protocol: Pattern recognition in early onset NM disorders. Neuromuscul. Disord. 2012, 22, S68–S84. [Google Scholar] [CrossRef]
- Shelly, M.J.; Bolster, F.; Foran, P.; Crosbie, I.; Kavanagh, E.C.; Eustace, S.J. Whole-Body Magnetic Resonance Imaging in Skeletal Muscle Disease. Semin. Musculoskelet. Radiol. 2010, 14, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Sookhoo, S.; MacKinnon, I.; Bushby, K.; Chinnery, P.; Birchall, D. MRI for the demonstration of subclinical muscle involvement in muscular dystrophy. Clin. Radiol. 2007, 62, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Carlier, R.Y.; Quijano-Roy, S. Muscle Magnetic Resonance Imaging: A New Diagnostic Tool with Promising Avenues in Therapeutic Trials. Neuropediatrics 2014, 45, 273–274. [Google Scholar] [CrossRef] [PubMed]
- Greer, M.-L.C. Whole-body magnetic resonance imaging: Techniques and non-oncologic indications. Pediatr. Radiol. 2018, 48, 1348–1363. [Google Scholar] [CrossRef] [PubMed]
- Lecouvet, F.E. Whole-Body MR Imaging: Musculoskeletal Applications. Radiology 2016, 279, 345–365. [Google Scholar] [CrossRef]
- Ahlawat, S.; Debs, P.; Amini, B.; Lecouvet, F.E.; Omoumi, P.; Wessell, D.E. Clinical Applications and Controversies of Whole-Body MRI: AJR Expert Panel Narrative Review. Am. J. Roentgenol. 2023, 220, 463–475. [Google Scholar] [CrossRef]
- Chardon, J.W.; Díaz-Manera, J.; Tasca, G.; Bönnemann, C.G.; Gómez-Andrés, D.; Heerschap, A.; Mercuri, E.; Muntoni, F.; Pichiecchio, A.; Ricci, E.; et al. MYO-MRI diagnostic protocols in genetic myopathies. Neuromuscul. Disord. 2019, 29, 827–841. [Google Scholar] [CrossRef]
- Filli, L.; Maurer, B.; Manoliu, A.; Andreisek, G.; Guggenberger, R. Whole-body MRI in adult inflammatory myopathies: Do we need imaging of the trunk? Eur. Radiol. 2015, 25, 3499–3507. [Google Scholar] [CrossRef]
- Pilania, K.; Jankharia, B. Role of MRI in idiopathic inflammatory myopathies: A review article. Acta Radiol. 2022, 63, 200–213. [Google Scholar] [CrossRef]
- Veeger, T.T.J.; van de Velde, N.M.; Keene, K.R.; Niks, E.H.; Hooijmans, M.T.; Webb, A.G.; de Groot, J.H.; Kan, H.E. Baseline fat fraction is a strong predictor of disease progression in Becker muscular dystrophy. NMR Biomed. 2022, 35, e4691. [Google Scholar] [CrossRef] [PubMed]
- Tomas, X.; Milisenda, J.C.; Garcia-Diez, A.I.; Prieto-Gonzalez, S.; Faruch, M.; Pomes, J.; Grau-Junyent, J.M. Whole-body MRI and pathological findings in adult patients with myopathies. Skelet. Radiol. 2019, 48, 653–676. [Google Scholar] [CrossRef] [PubMed]
- Omoumi, P. The Dixon method in musculoskeletal MRI: From fat-sensitive to fat-specific imaging. Skelet. Radiol. 2021, 51, 1365–1369. [Google Scholar] [CrossRef]
- Chhabra, A.; Madhuranthakam, A.J.; Andreisek, G. Magnetic resonance neurography: Current perspectives and literature review. Eur. Radiol. 2017, 28, 698–707. [Google Scholar] [CrossRef] [PubMed]
- Tasca, G.; Monforte, M.; De Fino, C.; Kley, R.A.; Ricci, E.; Mirabella, M. Magnetic resonance imaging pattern recognition in sporadic inclusion-body myositis. Muscle Nerve 2015, 52, 956–962. [Google Scholar] [CrossRef]
- Ukichi, T.; Yoshida, K.; Matsushima, S.; Kawakami, G.; Noda, K.; Furuya, K.; Kurosaka, D. MRI of skeletal muscles in patients with idiopathic inflammatory myopathies: Characteristic findings and diagnostic performance in dermatomyositis. RMD Open 2019, 5, e000850. [Google Scholar] [CrossRef]
- Lehmann, H.C.; Burke, D.; Kuwabara, S. Chronic inflammatory demyelinating polyneuropathy: Update on diagnosis, immunopathogenesis and treatment. J. Neurol. Neurosurg. Psychiatry 2019, 90, 981–987. [Google Scholar] [CrossRef]
- Schedel, H.; Reimers, C.D.; Vogl, T.; Witt, T.N. Muscle edema in MR imaging of neuromuscular diseases. Acta Radiol. 1995, 36, 228–232. [Google Scholar] [CrossRef]
- Kuo, G.P.; A Carrino, J. Skeletal muscle imaging and inflammatory myopathies. Curr. Opin. Rheumatol. 2007, 19, 530–535. [Google Scholar] [CrossRef]
- Costa, A.F.; Di Primio, G.A.; Schweitzer, M.E. Magnetic resonance imaging of muscle disease: A pattern-based approach. Muscle Nerve 2012, 46, 465–481. [Google Scholar] [CrossRef]
- Elessawy, S.S.; Abdelsalam, E.M.; Razek, E.A.; Tharwat, S. Whole-body MRI for full assessment and characterization of diffuse inflammatory myopathy. Acta Radiol. Open 2016, 5, 205846011666821. [Google Scholar] [CrossRef]
- Morrow, J.M.; Matthews, E.; Rayan, D.L.R.; Fischmann, A.; Sinclair, C.D.; Reilly, M.M.; Thornton, J.S.; Hanna, M.G.; Yousry, T.A. Muscle MRI reveals distinct abnormalities in genetically proven non-dystrophic myotonias. Neuromuscul. Disord. 2013, 23, 637–646. [Google Scholar] [CrossRef]
- Connor, A.; Stebbings, S.; Hung, N.A.; Hammond-Tooke, G.; Meikle, G.; Highton, J. STIR MRI to Direct Muscle Biopsy in Suspected Idiopathic Inflammatory Myopathy. Am. J. Clin. Oncol. 2007, 13, 341–345. [Google Scholar] [CrossRef]
- Simon, N.G.; Noto, Y.-I.; Zaidman, C.M. Skeletal muscle imaging in neuromuscular disease. J. Clin. Neurosci. 2016, 33, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Goutallier, D.; Postel, J.M.; Bernageau, J.; Lavau, L.; Voisin, M.C. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin. Orthop. Relat. Res. 1994, 304, 78–83. [Google Scholar] [CrossRef]
- Mercuri, E.; Pichiecchio, A.; Allsop, J.; Messina, S.; Pane, M.; Muntoni, F. Muscle MRI in inherited neuromuscular disorders: Past, present, and future. J. Magn. Reson. Imaging 2007, 25, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Wynn, T.A. Cellular and molecular mechanisms of fibrosis. J. Pathol. 2008, 214, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Kharraz, Y.; Guerra, J.; Pessina, P.; Serrano, A.L.; Muñoz-Cánoves, P. Understanding the Process of Fibrosis in Duchenne Muscular Dystrophy. BioMed Res. Int. 2014, 2014, 965631. [Google Scholar] [CrossRef]
- Desguerre, I.; Mayer, M.; Leturcq, F.; Barbet, J.-P.; Gherardi, R.K.; Christov, C. Endomysial Fibrosis in Duchenne Muscular Dystrophy: A Marker of Poor Outcome Associated with Macrophage Alternative Activation. J. Neuropathol. Exp. Neurol. 2009, 68, 762–773. [Google Scholar] [CrossRef]
- Siu, A.G.; Ramadeen, A.; Hu, X.; Morikawa, L.; Zhang, L.; Lau, J.Y.C.; Liu, G.; Pop, M.; Connelly, K.A.; Dorian, P.; et al. Characterization of the ultrashort-TE (UTE) MR collagen signal. NMR Biomed. 2015, 28, 1236–1244. [Google Scholar] [CrossRef]
- Carlier, P.G.; Marty, B.; Scheidegger, O.; de Sousa, P.L.; Baudin, P.-Y.; Snezhko, E.; Vlodavets, D. Skeletal Muscle Quantitative Nuclear Magnetic Resonance Imaging and Spectroscopy as an Outcome Measure for Clinical Trials. J. Neuromuscul. Dis. 2016, 3, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Andreassen, C.S.; Jakobsen, J.; Ringgaard, S.; Ejskjaer, N.; Andersen, H. Accelerated atrophy of lower leg and foot muscles—A follow-up study of long-term diabetic polyneuropathy using magnetic resonance imaging (MRI). Diabetologia 2009, 52, 1182–1191. [Google Scholar] [CrossRef]
- Dixon, W.T. Simple proton spectroscopic imaging. Radiology 1984, 153, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Burakiewicz, J.; Sinclair, C.D.J.; Fischer, D.; Walter, G.A.; Kan, H.E.; Hollingsworth, K.G. Quantifying fat replacement of muscle by quantitative MRI in muscular dystrophy. J. Neurol. 2017, 264, 2053–2067. [Google Scholar] [CrossRef] [PubMed]
- Guichoux, F.; Vuillemin, V.; Morvan, G.; Zins, M.; Thevenin, F.; Guerini, H.; Omoumi, P.; Drape, J.L. Fat Suppression with Dixon Techniques in Musculoskeletal Magnetic Resonance Imaging: A Pictorial Review. Semin. Musculoskelet. Radiol. 2015, 19, 335–347. [Google Scholar] [CrossRef]
- Ma, J. Dixon techniques for water and fat imaging. J. Magn. Reson. Imaging 2008, 28, 543–558. [Google Scholar] [CrossRef]
- Baudin, P.-Y.; Marty, B.; Robert, B.; Shukelovitch, A.; Carlier, R.Y.; Azzabou, N.; Carlier, P.G. Qualitative and quantitative evaluation of skeletal muscle fatty degenerative changes using whole-body Dixon nuclear magnetic resonance imaging for an important reduction of the acquisition time. Neuromuscul. Disord. 2015, 25, 758–763. [Google Scholar] [CrossRef]
- Yao, L.; Gai, N. Fat-Corrected T2 Measurement as a Marker of Active Muscle Disease in Inflammatory Myopathy. Am. J. Roentgenol. 2012, 198, W475–W481. [Google Scholar] [CrossRef]
- Maurer, B.; A Walker, U. Role of MRI in Diagnosis and Management of Idiopathic Inflammatory Myopathies. Curr. Rheumatol. Rep. 2015, 17, 67. [Google Scholar] [CrossRef]
- Di Stefano, V.; Barbone, F.; Ferrante, C.; Telese, R.; Vitale, M.; Onofrj, M.; Di Muzio, A. Inflammatory polyradiculoneuropathies: Clinical and immunological aspects, current therapies, and future perspectives. Eur. J. Inflamm. 2020, 18, 205873922094234. [Google Scholar] [CrossRef]
- Winer, J.B. Guillain-Barre syndrome. BMJ 2008, 337, a671. [Google Scholar] [CrossRef] [PubMed]
- Prineas, J.W. Pathology of the Guillain-Barré syndrome. Ann. Neurol. 1981, 9, 6–19. [Google Scholar] [CrossRef]
- Asbury, A.K.; Arnason, B.G.; Adams, R.D. The inflammatory lesion in idiopathic polyneuritis. Medicine 1969, 48, 173. [Google Scholar] [CrossRef]
- Asbury, A.K.; Cornblath, D.R. Assessment of current diagnostic criteria for Guillain-Barr syndrome. Ann. Neurol. 1990, 27, S21–S24. [Google Scholar] [CrossRef] [PubMed]
- Maramattom, B.V. Screening Power of Short Tau Inversion Recovery Muscle Magnetic Resonance Imaging in Critical Illness Myoneuropathy and Guillain–Barre Syndrome in the Intensive Care Unit. Indian J. Crit. Care Med. 2022, 26, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; He, B.; Wang, S.; Zhou, Z.; Gao, F.; Xiao, L.; Luo, X.; Wu, C.; Gong, T.; Chen, W.; et al. Diffusion Tensor Imaging of Tibial and Common Peroneal Nerves in Patients with Guillain–Barre Syndrome: A Feasibility Study. J. Magn. Reson. Imaging 2019, 49, 1356–1364. [Google Scholar] [CrossRef]
- Yikilmaz, A.; Doganay, S.; Gumus, H.; Per, H.; Kumandas, S.; Coskun, A. Magnetic resonance imaging of childhood Guillain–Barre syndrome. Child’s Nerv. Syst. 2010, 26, 1103–1108. [Google Scholar] [CrossRef]
- Rentzos, M.; Anyfanti, C.; Kaponi, A.; Pandis, D.; Ioannou, M.; Vassilopoulos, D. Chronic inflammatory demyelinating polyneuropathy: A 6-year retrospective clinical study of a hospital-based population. J. Clin. Neurosci. 2007, 14, 229–235. [Google Scholar] [CrossRef]
- Dimachkie, M.M.; Barohn, R.J. Chronic Inflammatory Demyelinating Polyneuropathy. Curr. Treat. Options Neurol. 2013, 15, 350–366. [Google Scholar] [CrossRef]
- Thawait, S.; Chaudhry, V.; Thawait, G.; Wang, K.; Belzberg, A.; Carrino, J.; Chhabra, A. High-Resolution MR Neurography of Diffuse Peripheral Nerve Lesions. Am. J. Neuroradiol. 2011, 32, 1365–1372. [Google Scholar] [CrossRef]
- Doneddu, P.E.; Akyil, H.; Manganelli, F.; Briani, C.; Cocito, D.; Benedetti, L.; Mazzeo, A.; Fazio, R.; Filosto, M.; Cosentino, G.; et al. Unclassified clinical presentations of chronic inflammatory demyelinating polyradiculoneuropathy. J. Neurol. Neurosurg. Psychiatry 2023, 94, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Bergh, P.Y.K.V.D.; van Doorn, P.A.; Hadden, R.D.M.; Avau, B.; Vankrunkelsven, P.; Allen, J.A.; Attarian, S.; Blomkwist-Markens, P.H.; Cornblath, D.R.; Eftimov, F.; et al. European Academy of Neurology/Peripheral Nerve Society guideline on diagnosis and treatment of chronic inflammatory demyelinating polyradiculoneuropathy: Report of a joint Task Force—Second revision. J. Peripher. Nerv. Syst. 2021, 26, 3556–3583. [Google Scholar] [CrossRef]
- Abe, Y.; Terashima, H.; Hoshino, H.; Sassa, K.; Sakai, T.; Ohtake, A.; Kubota, M.; Yamanouchi, H. Characteristic MRI features of chronic inflammatory demyelinating polyradiculoneuropathy. Brain Dev. 2015, 37, 894–896. [Google Scholar] [CrossRef] [PubMed]
- Trouth, A.J.; Dabi, A.; Solieman, N.; Kurukumbi, M.; Kalyanam, J. Myasthenia Gravis: A Review. Autoimmune Dis. 2012, 2012, 874680. [Google Scholar] [CrossRef]
- Priola, A.; Priola, S. Imaging of thymus in myasthenia gravis: From thymic hyperplasia to thymic tumor. Clin. Radiol. 2014, 69, e230–e245. [Google Scholar] [CrossRef]
- Amin, S.; Aung, M.; Gandhi, F.R.; Escobar, J.A.P.; Gulraiz, A.; Malik, B.H. Myasthenia Gravis and its Association with Thyroid Diseases. Cureus 2020, 12, 10248. [Google Scholar] [CrossRef]
- Sieb, J.P. Myasthenia gravis: An update for the clinician. Clin. Exp. Immunol. 2014, 175, 408–418. [Google Scholar] [CrossRef]
- Patrick, J.; Lindstrom, J. Autoimmune Response to Acetylcholine Receptor. Science 1973, 180, 871–872. [Google Scholar] [CrossRef]
- McConville, J.; Farrugia, M.E.; Beeson, D.; Kishore, U.; Metcalfe, R.; Newsom-Davis, J.; Vincent, A. Detection and characterization of MuSK antibodies in seronegative myasthenia gravis. Ann. Neurol. 2004, 55, 580–584. [Google Scholar] [CrossRef]
- Higuchi, O.; Hamuro, J.; Motomura, M.; Yamanashi, Y. Autoantibodies to low-density lipoprotein receptor-related protein 4 in myasthenia gravis. Ann. Neurol. 2011, 69, 418–422. [Google Scholar] [CrossRef]
- Gasperi, C.; Melms, A.; Schoser, B.; Zhang, Y.; Meltoranta, J.; Risson, V.; Schaeffer, L.; Schalke, B.; Kröger, S. Anti-agrin autoantibodies in myasthenia gravis. Neurology 2014, 82, 1976–1983. [Google Scholar] [CrossRef] [PubMed]
- Dresser, L.; Wlodarski, R.; Rezania, K.; Soliven, B. Myasthenia Gravis: Epidemiology, Pathophysiology and Clinical Manifestations. J. Clin. Med. 2021, 10, 2235. [Google Scholar] [CrossRef] [PubMed]
- Ciafaloni, E. Myasthenia Gravis and Congenital Myasthenic Syndromes. Contin. Lifelong Learn. Neurol. 2019, 25, 1767–1784. [Google Scholar] [CrossRef] [PubMed]
- Lupica, A.; Di Stefano, V.; Iacono, S.; Pignolo, A.; Quartana, M.; Gagliardo, A.; Fierro, B.; Brighina, F. Impact of COVID-19 in AChR Myasthenia Gravis and the Safety of Vaccines: Data from an Italian Cohort. Neurol. Int. 2022, 14, 406–416. [Google Scholar] [CrossRef]
- Lueangaram, S.; Tritanon, O.; Siriyotha, S.; Vanikieti, K.; Padungkiatsagul, T.; Preechawat, P.; Poonyathalang, A.; Dejthevaporn, C.; Pulkes, T.; Tunlayadechanont, S.; et al. Radiological Characteristics of Extraocular Muscles in Myasthenia Gravis Patients with Ocular Manifestations: A Case–Control Study. Clin. Ophthalmol. 2021, 15, 2279–2285. [Google Scholar] [CrossRef]
- Finlayson, S.; Morrow, J.M.; Cruz, P.M.R.; Sinclair, C.D.; Fischmann, A.; Thornton, J.S.; Knight, S.; Norbury, R.; White, M.; Al-Hajjar, M.; et al. Muscle magnetic resonance imaging in congenital myasthenic syndromes. Muscle Nerve 2016, 54, 211–219. [Google Scholar] [CrossRef]
- Somnier, F.E.; Skeie, G.O.; Aarli, J.A.; Trojaborg, W. EMG evidence of myopathy and the occurrence of titin autoantibodies in patients with myasthenia gravis. Eur. J. Neurol. 1999, 6, 555–563. [Google Scholar] [CrossRef]
- Dalakas, M.C. Inflammatory Muscle Diseases. N. Engl. J. Med. 2015, 372, 1734–1747. [Google Scholar] [CrossRef]
- Selva-O’Callaghan, A.; Pinal-Fernandez, I.; Trallero-Araguás, E.; Milisenda, J.C.; Grau-Junyent, J.M.; Mammen, A.L. Classification and management of adult inflammatory myopathies. Lancet Neurol. 2018, 17, 816–828. [Google Scholar] [CrossRef]
- Senécal, J.; Raynauld, J.; Troyanov, Y. Editorial: A New Classification of Adult Autoimmune Myositis. Arthritis Rheumatol. 2017, 69, 878–884. [Google Scholar] [CrossRef]
- Maundrell, A.; Proudman, S.; Limaye, V. Prevalence of other connective tissue diseases in idiopathic inflammatory myopathies. Rheumatol. Int. 2019, 39, 1777–1781. [Google Scholar] [CrossRef] [PubMed]
- Saketkoo, L.A.; Ascherman, D.P.; Cottin, V.; Christopher-Stine, L.; Danoff, S.K.; Oddis, C.V. Interstitial Lung Disease in Idiopathic Inflammatory Myopathy. Curr. Rheumatol. Rev. 2010, 6, 108–119. [Google Scholar] [CrossRef] [PubMed]
- Zanframundo, G.; Tripoli, A.; Cometi, L.; Marcucci, E.; Furini, F.; Cavagna, L.; Barsotti, S. One year in review 2020: Idiopathic inflammatory myopathies. Ann. Rheum. Dis. 2021, 39, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-J.; Wu, C.-Y.; Huang, Y.-L.; Wang, C.-B.; Shen, J.-L.; Chang, Y.-T. Cancer risks of dermatomyositis and polymyositis: A nationwide cohort study in Taiwan. Arthritis Res. Ther. 2010, 12, R70. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Peng, Q.; Yin, L.; Li, S.; Shi, J.; Zhang, Y.; Lu, X.; Shu, X.; Zhang, S.; Wang, G. Identification of multiple cancer-associated myositis-specific autoantibodies in idiopathic inflammatory myopathies: A large longitudinal cohort study. Arthritis Res. Ther. 2017, 19, 259. [Google Scholar] [CrossRef]
- Stockton, D.; Doherty, V.R.; Brewster, D.H. Risk of cancer in patients with dermatomyositis or polymyositis and follow-up implications: A Scottish population-based cohort study. Br. J. Cancer 2001, 85, 41–45. [Google Scholar] [CrossRef]
- Hengstman, G.J.D.; Egberts, W.T.M.V.; Seelig, H.P.; Lundberg, I.E.; Moutsopoulos, H.M.; Doria, A.; Mosca, M.; Vencovsky, J.; van Venrooij, W.J.; van Engelen, B.G.M. Clinical characteristics of patients with myositis and autoantibodies to different fragments of the Mi-2 antigen. Ann. Rheum. Dis. 2006, 65, 242–245. [Google Scholar] [CrossRef]
- Marie, I.; Josse, S.; Decaux, O.; Dominique, S.; Diot, E.; Landron, C.; Roblot, P.; Jouneau, S.; Hatron, P.; Tiev, K.; et al. Comparison of long-term outcome between anti-Jo1- and anti-PL7/PL12 positive patients with antisynthetase syndrome. Autoimmun. Rev. 2012, 11, 739–745. [Google Scholar] [CrossRef]
- Legault, D.; McDermott, J.; Crous-Tsanaclis, A.M.; Boire, G. Cancer-associated myositis in the presence of anti-Jo1 auto-antibodies and the antisynthetase syndrome. J. Rheumatol. 2008, 35, 169–171. [Google Scholar]
- Albayda, J.; Pinal-Fernandez, I.; Huang, W.; Parks, C.; Paik, J.; Casciola-Rosen, L.; Danoff, S.K.; Johnson, C.; Christopher-Stine, L.; Mammen, A.L. Antinuclear Matrix Protein 2 Autoantibodies and Edema, Muscle Disease, and Malignancy Risk in Dermatomyositis Patients. Arthritis Care Res. 2017, 69, 1771–1776. [Google Scholar] [CrossRef]
- DeWane, M.E.; Waldman, R.; Lu, J. Dermatomyositis: Clinical features and pathogenesis. J. Am. Acad. Dermatol. 2020, 82, 267–281. [Google Scholar] [CrossRef] [PubMed]
- Spalkit, S.; Sinha, A.; Prakash, M.; Sandhu, M.S. Dermatomyositis: Patterns of MRI findings in muscles, fascia and skin of pelvis and thigh. Eur. J. Radiol. 2021, 141, 109812. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Liu, L.; Wang, L.; Xiao, J.; Wang, Z.; Lv, H.; Zhang, W.; Yuan, Y. Magnetic resonance imaging changes of thigh muscles in myopathy with antibodies to signal recognition particle. Rheumatology 2015, 54, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- Karino, K.; Kono, M.; Sakamoto, K.; Fujieda, Y.; Kato, M.; Amengual, O.; Oku, K.; Yasuda, S.; Atsumi, T. Myofascia-dominant involvement on whole-body MRI as a risk factor for rapidly progressive interstitial lung disease in dermatomyositis. Rheumatology 2020, 59, 1734–1742. [Google Scholar] [CrossRef]
- Kamiya, M.; Mizoguchi, F.; Takamura, A.; Kimura, N.; Kawahata, K.; Kohsaka, H. A new in vitro model of polymyositis reveals CD8+ T cell invasion into muscle cells and its cytotoxic role. Rheumatology 2020, 59, 224–232. [Google Scholar] [CrossRef]
- Marie, I.; Hatron, P.-Y.; Levesque, H.; Hachulla, E.; Hellot, M.-F.; Michon-Pasturel, U.; Courtois, H.; Devulder, B. Influence of Age on Characteristics of Polymyositis and Dermatomyositis in Adults. Medicine 1999, 78, 139–147. [Google Scholar] [CrossRef]
- Cantwell, C.; Ryan, M.; O’Connell, M.; Cunningham, P.; Brennan, D.; Costigan, D.; Lynch, T.; Eustace, S. A comparison of inflammatory myopathies at whole-body turbo STIR MRI. Clin. Radiol. 2005, 60, 261–267. [Google Scholar] [CrossRef]
- Del Grande, F.; Carrino, J.A.; Del Grande, M.; Mammen, A.L.; Stine, L.C. Magnetic Resonance Imaging of Inflammatory Myopathies. Top. Magn. Reson. Imaging 2011, 22, 39–43. [Google Scholar] [CrossRef]
- Dion, E.; Cherin, P.; Payan, C.; Fournet, J.-C.; Papo, T.; Maisonobe, T.; Auberton, E.; Chosidow, O.; Godeau, P.; Piette, J.-C.; et al. Magnetic resonance imaging criteria for distinguishing between inclusion body myositis and polymyositis. J. Rheumatol. 2002, 29, 1897–1906. [Google Scholar]
- Cox, F.M.; Reijnierse, M.; van Rijswijk, C.S.P.; Wintzen, A.R.; Verschuuren, J.J.; Badrising, U.A. Magnetic resonance imaging of skeletal muscles in sporadic inclusion body myositis. Rheumatology 2011, 50, 1153–1161. [Google Scholar] [CrossRef]
- Reimers, C.D.; Schedel, H.; Fleckenstein, J.L.; Witt, T.N.; Pongratz, D.E.; Vogl, T.J.; Nägele, M. Magnetic resonance imaging of skeletal muscles in idiopathic inflammatory myopathies of adults. J. Neurol. 1994, 241, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Ansari, B.; Salort-Campana, E.; Ogier, A.; Le Troter, A.; Marie, B.D.S.; Guye, M.; Delmont, E.; Grapperon, A.; Verschueren, A.; Bendahan, D.; et al. Quantitative muscle MRI study of patients with sporadic inclusion body myositis. Muscle Nerve 2020, 61, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Pinal-Fernandez, I.; Casal-Dominguez, M.; Mammen, A.L. Immune-Mediated Necrotizing Myopathy. Curr. Rheumatol. Rep. 2018, 20, 21. [Google Scholar] [CrossRef] [PubMed]
- Pinal-Fernandez, I.; Parks, C.; Werner, J.L.; Albayda, J.; Paik, J.J.; Danoff, S.K.; Casciola-Rosen, L.; Christopher-Stine, L.; Mammen, A.L. Longitudinal Course of Disease in a Large Cohort of Myositis Patients with Autoantibodies Recognizing the Signal Recognition Particle. Arthritis Care Res. 2017, 69, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Fionda, L.; Lauletta, A.; Leonardi, L.; Perez, J.A.; Morino, S.; Merlonghi, G.; Alfieri, G.; Costanzo, R.; Tufano, L.; Vanoli, F.; et al. Muscle MRI in immune-mediated necrotizing myopathy (IMNM): Implications for clinical management and treatment strategies. J. Neurol. 2023, 270, 960–974. [Google Scholar] [CrossRef]
- Devic, P.; Gallay, L.; Streichenberger, N.; Petiot, P. Focal myositis: A review. Neuromuscul. Disord. 2016, 26, 725–733. [Google Scholar] [CrossRef]
- Lunde, H.M.B.; Skeie, G.O.; Bertelsen, A.K.; Karlsen, B.; Miletic, H.; Lindal, S.; Brautaset, N.J.; Bindoff, L.A. Focal myositis—A neurogenic phenomenon? Neuromuscul. Disord. 2012, 22, 350–354. [Google Scholar] [CrossRef]
- Sekiguchi, K.; Kanda, F.; Oishi, K.; Hamaguchi, H.; Nakazawa, K.; Maeda, N.; Ishihara, H.; Chihara, K. HLA typing in focal myositis. J. Neurol. Sci. 2004, 227, 21–25. [Google Scholar] [CrossRef]
- Gaeta, M.; Mazziotti, S.; Minutoli, F.; Genitori, A.; Toscano, A.; Rodolico, C.; Blandino, A. MR imaging findings of focal myositis: A pseudotumour that may mimic muscle neoplasm. Skelet. Radiol. 2009, 38, 571–578. [Google Scholar] [CrossRef]
- Scott, I.U.; Siatkowski, R.M. Idiopathic orbital myositis. Curr. Opin. Rheumatol. 1997, 9, 504–512. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| POLYMYOSITIS | DERMATOMYOSITIS | IBM | |
|---|---|---|---|
| SIDE INVOLVEMENT | Symmetric | Symmetric | Asymmetric |
| MUSCLE GRADIENT | Proximal predominance | Proximal predominance | Distal predominance |
| PATTERN OF EDEMA | Diffuse homogeneous | Peripheral distribution, patchy or honeycomb pattern | Less frequent than fat degeneration |
| PATTERN OF MUSCLE FAT INFILTRATION | Less frequent than edema | Less frequent than edema | Predominant fatty infiltration |
| FASCIAL INVOLVEMENT | Not always, less than dermatomyositis | Present | Absent |
| SUBCUTANEOUS INVOLVEMENT | Absent | Significant subcutaneous edema | Absent |
| MUSCLE MORE INVOLVED | Thigh with global or posterior compartment involvement | Thigh with anterior compartment involvement (quadriceps) | medial head of gastrocnemius, flexor digitorum profundus, anterior compartment of the thigh |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pace, M.; Cannella, R.; Di Stefano, V.; Lupica, A.; Alonge, P.; Morici, G.; Brighina, F.; Brancato, F.; Midiri, F.; Galia, M. Usefulness and Clinical Impact of Whole-Body MRI in Detecting Autoimmune Neuromuscular Disorders. Brain Sci. 2023, 13, 1500. https://doi.org/10.3390/brainsci13101500
Pace M, Cannella R, Di Stefano V, Lupica A, Alonge P, Morici G, Brighina F, Brancato F, Midiri F, Galia M. Usefulness and Clinical Impact of Whole-Body MRI in Detecting Autoimmune Neuromuscular Disorders. Brain Sciences. 2023; 13(10):1500. https://doi.org/10.3390/brainsci13101500
Chicago/Turabian StylePace, Mario, Roberto Cannella, Vincenzo Di Stefano, Antonino Lupica, Paolo Alonge, Giulio Morici, Filippo Brighina, Federica Brancato, Federico Midiri, and Massimo Galia. 2023. "Usefulness and Clinical Impact of Whole-Body MRI in Detecting Autoimmune Neuromuscular Disorders" Brain Sciences 13, no. 10: 1500. https://doi.org/10.3390/brainsci13101500
APA StylePace, M., Cannella, R., Di Stefano, V., Lupica, A., Alonge, P., Morici, G., Brighina, F., Brancato, F., Midiri, F., & Galia, M. (2023). Usefulness and Clinical Impact of Whole-Body MRI in Detecting Autoimmune Neuromuscular Disorders. Brain Sciences, 13(10), 1500. https://doi.org/10.3390/brainsci13101500