
Specific Behavioral Responses Rather Than Autonomic Responses Can Indicate and Quantify Acute Pain among Individuals with Intellectual and Developmental Disabilities

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.2.1. Pressure Algometer
2.2.2. PMD-100 System
2.2.3. Facial Action Coding System (FACS)
2.2.4. Self-Report Rating Scale
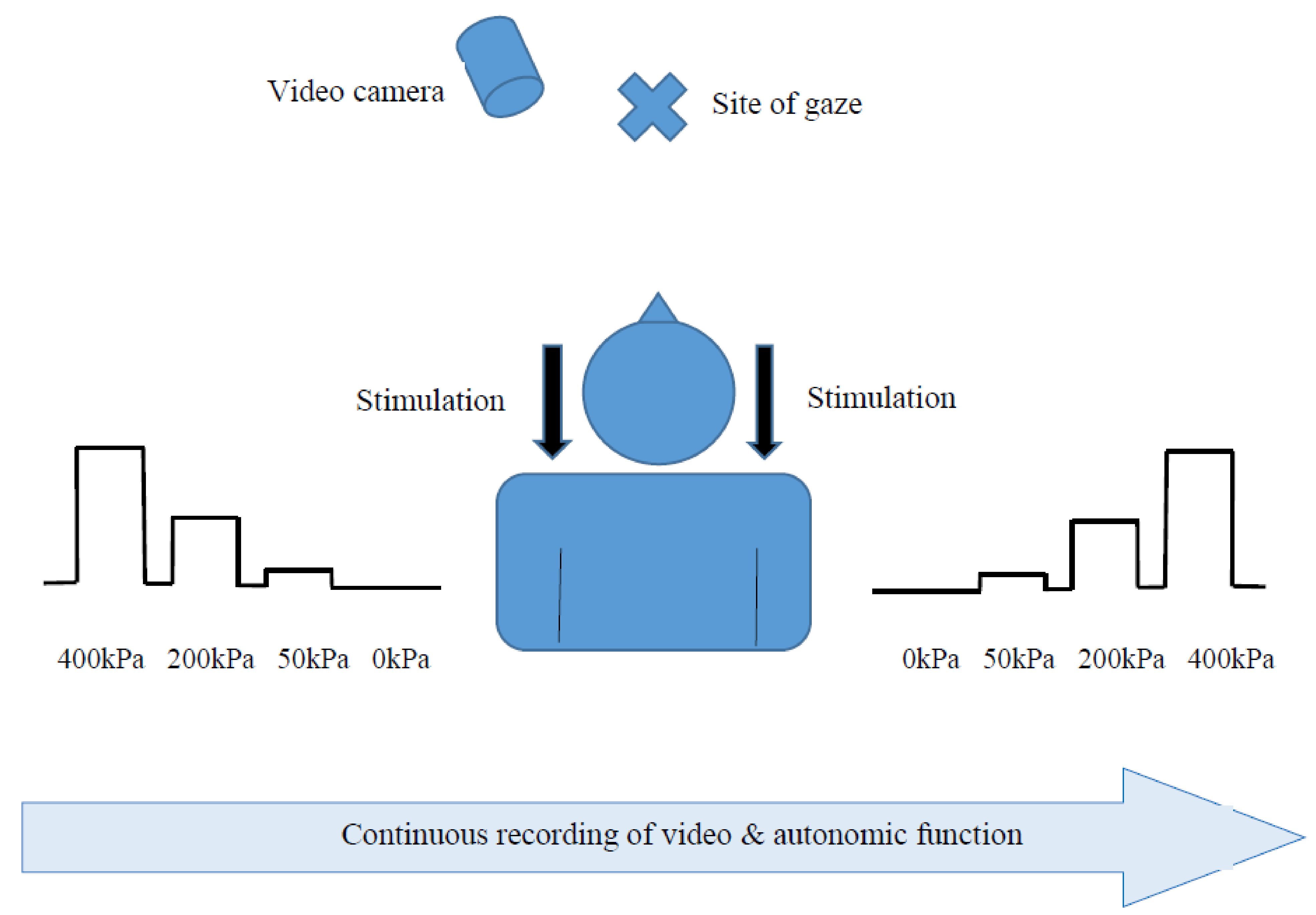
3. Procedures
3.1. Training and Pressure Stimulation
3.2. Recording and Analysis of the Facial and Bodily Responses
3.3. Analyzing the Physiological Signals
4. Data Analysis
5. Results
5.1. The Study Groups
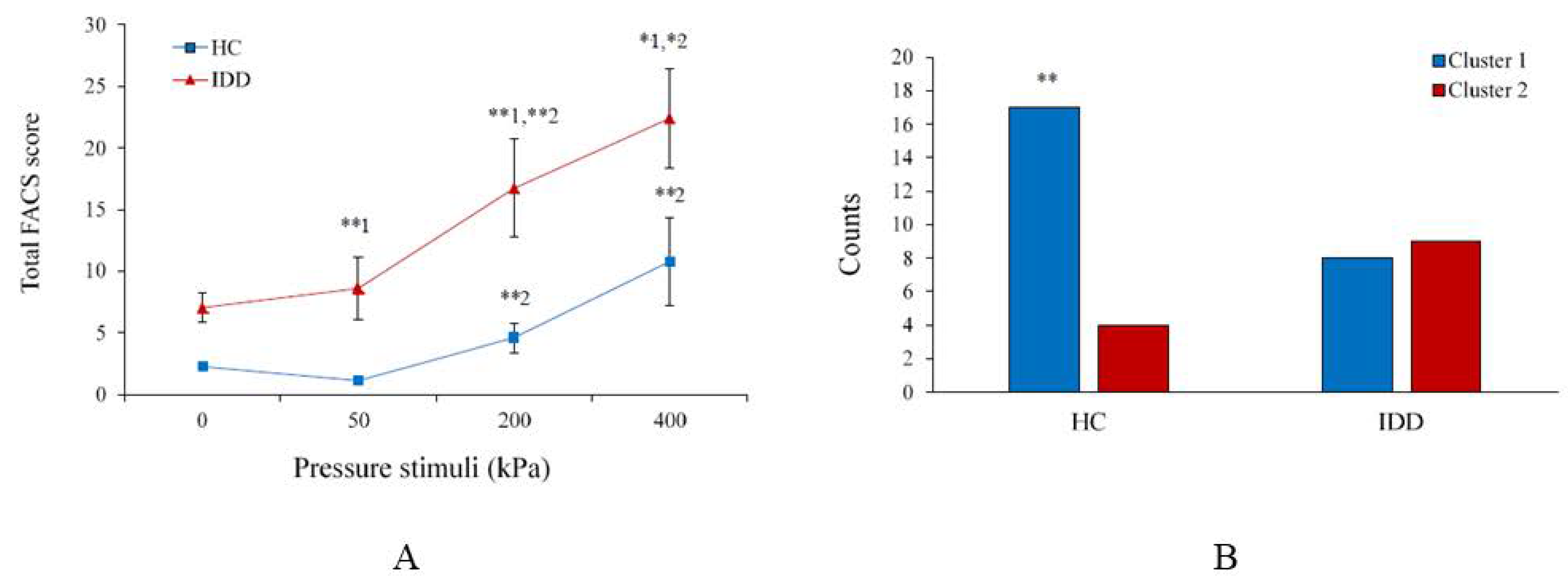
5.2. Facial Expressions (FACS)
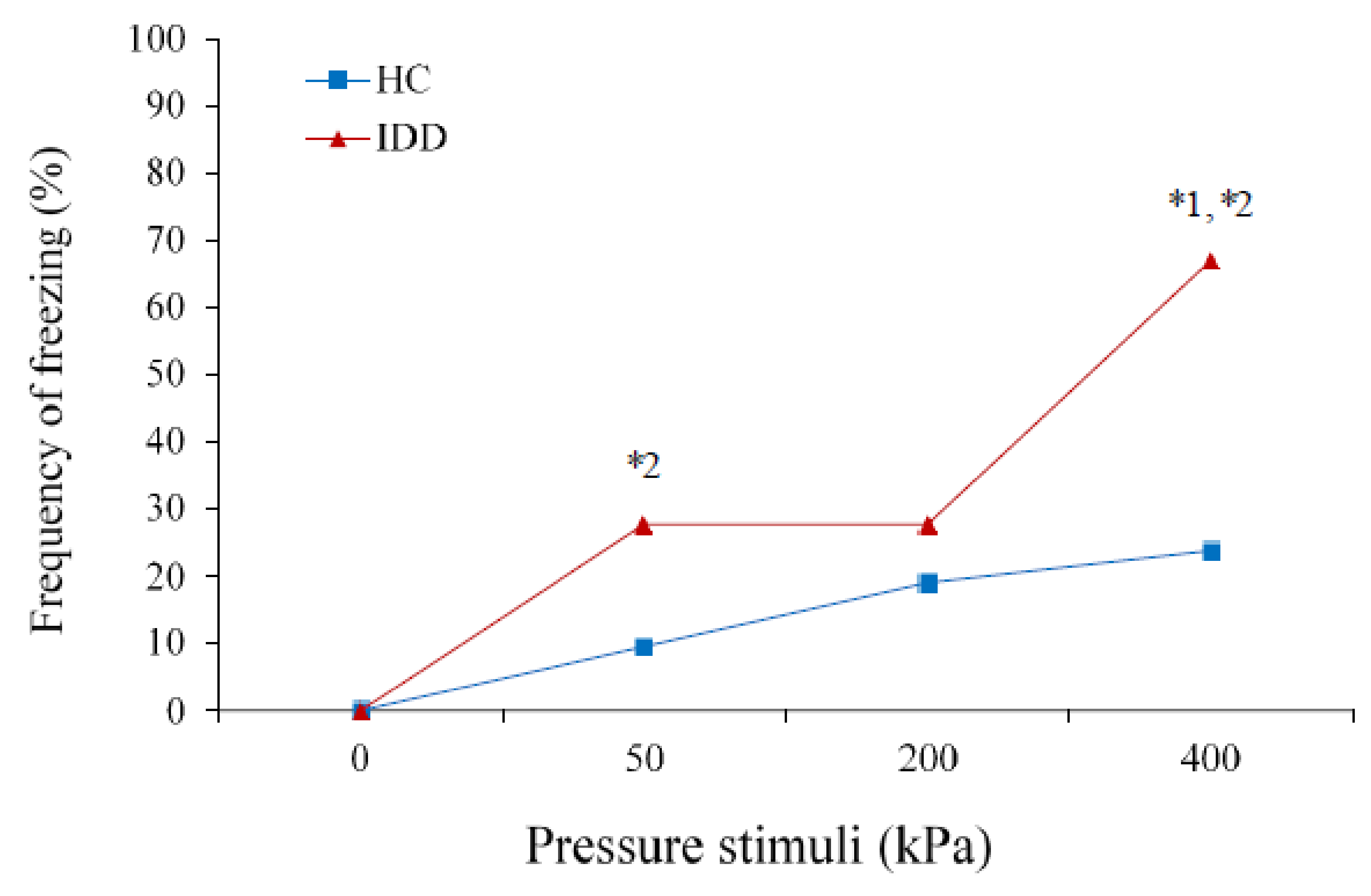
5.3. Body Freezing
5.4. Self-Ratings
5.5. Autonomic Variables
5.6. Correlations between Variables
6. Discussion
6.1. Indices That Differentiate between Painful and Non-Painful States
6.2. Indices That Can Differentiate between the Intensities of Noxious Stimuli
6.3. Comparisons between Individuals with IDD and HC
6.4. Limitations
6.5. Conclusions and Impact
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oberlander, T.F.; Symons, F. The Problem of Pain in Developmental Disability. In Pain in Developmental Disabilities; Oberlander, T.F., Symons, F.J., Eds.; Paul H. Brookes Publishing Co. Inc.: Baltimore, MD, USA, 2006. [Google Scholar]
- Henderson, A.; Lynch, S.A.; Wilkinson, S.; Hunter, M. Adults with Down’s syndrome: The prevalence of complications and health care in the community. Br. J. Gen. Pract. 2007, 57, 50–55. [Google Scholar] [PubMed]
- Abanto, J.; Ciamponi, A.L.; Francischini, E.; Murakami, C.; de Rezende, N.P.M.; Gallottini, M. Medical problems and oral care of patients with Down syndrome: A literature review. Spec. Care Dentist. 2011, 31, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Turk, V.; Khattran, S.; Kerry, S.; Corney, R.; Painter, K. Reporting of health problems and pain by adults with an intellectual disability and by their carers. J. Appl. Res. Intellect. Disabil. 2012, 25, 155–165. [Google Scholar] [CrossRef]
- Kinnear, D.; Morrison, J.; Allan, L.; Henderson, A.; Smiley, E.; Cooper, S.A. Prevalence of physical conditions and multimorbidity in a cohort of adults with intellectual disabilities with and without Down syndrome: Cross-sectional study. BMJ Open 2018, 8, e018292. [Google Scholar] [CrossRef]
- Finlayson, J.; Morrison, J.; Jackson, A.; Mantry, D.; Cooper, S.A. Injuries, falls and accidents among adults with intellectual disabilities: Prospective cohort study. J. Intellect. Disabil. Res. 2010, 54, 966–980. [Google Scholar] [CrossRef] [PubMed]
- Ho, P.; Bulsara, M.; Downs, J.; Patman, S.; Bulsara, C.; Hill, A.M. Incidence and prevalence of falls in adults with intellectual disability living in the community: A systematic review. JBI Database System Rev. Implement. Rep. 2019, 17, 390–413. [Google Scholar] [CrossRef] [PubMed]
- McGuire, B.E.; Daly, P.; Smyth, F. Chronic pain in people with an intellectual disability: Under-recognised and under-treated? J. Intellect Disabil. Res. 2010, 54, 240–245. [Google Scholar] [CrossRef]
- Amor-Salamanca, A.; Menchon, J.M. Pain underreporting associated with profound intellectual disability in emergency departments. J. Intellect. Disabil. Res. 2017, 61, 341–347. [Google Scholar] [CrossRef] [PubMed]
- de Knegt, N.C.; Lobbezoo, F.; Schuengel, C.; Evenhuis, H.M.; Scherder, E.J.A. Self-Reported Presence and Experience of Pain in Adults with Down Syndrome. Pain Med. 2017, 18, 1247–1263. [Google Scholar] [CrossRef]
- Oviedo, G.R.; Tamulevicius, N.; Guerra-Balic, M. Physical activity and sedentary time in active and non-active adults with intellectual disability: A comparative study. Int. J. Environ. Res. Public Health 2019, 16, 1761. [Google Scholar] [CrossRef] [PubMed]
- McGuire, B.E.; Daly, P.; Smyth, F. Lifestyle and health behaviours of adults with an intellectual disability. J. Intellect Disabil Res. 2007, 51, 497–510. [Google Scholar] [CrossRef]
- Axmon, A.; Sandberg, M.; Ahlström, G.; Midlöv, P. Prescription of potentially inappropriate medications among older people with intellectual disability: A register study. BMC Pharmacol. Toxicol. 2017, 18, 68. [Google Scholar] [CrossRef] [PubMed]
- Segerlantz, M.; Axmon, A.; Gagnemo Persson, R.; Brun, E.; Ahlström, G. Prescription of pain medication among older cancer patients with and without an intellectual disability: A national register study. BMC Cancer 2019, 19, 1040. [Google Scholar] [CrossRef]
- Walsh, M.; Morrison, T.G.; McGuire, B.E. Chronic pain in adults with an intellectual disability: Prevalence, impact, and health service use based on caregiver report. Pain 2011, 152, 1951–1957. [Google Scholar] [CrossRef]
- van der Slot, W.M.A.; Benner, J.L.; Brunton, L.; Engel, J.M.; Gallien, P.; Hilberink, S.R.; Månum, G.; Morgan, P.; Opheim, A.; Riquelme, I.; et al. Pain in adults with cerebral palsy: A systematic review and meta-analysis of individual participant data. Ann. Phys. Rehabil. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Barney, C.C.; Andersen, R.D.; Defrin, R.; Genik, L.M.; McGuire, B.E.; Symons, F.J. Challenges in pain assessment and management among individuals with intellectual and developmental disabilities. Pain Rep. 2020, 5, e821. [Google Scholar] [CrossRef] [PubMed]
- Oberlander, T.F.; Gilbert, C.A.; Chambers, C.T.; O’Donnell, M.E.; Craig, K.D. Biobehavioral responses to acute pain in adolescents with a significant neurological impairment. Clin. J. Pain 1999, 15, 201–209. [Google Scholar] [CrossRef] [PubMed]
- La Chapelle, D.L.; Hadijistavropoulos, R.; Craig, K.D. Pain Measurement in Persons with Intellectual Disability. Clin. J. Pain 1999, 15, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Breau, L.M.; McGrath, P.J.; Craig, K.D.; Santor, D.; Cassidy, K.L.; Reid, G.J. Facial expression of children receiving immunizations: A principal components analysis of the child facial coding system. Clin. J. Pain 2001, 17, 178–186. [Google Scholar] [CrossRef]
- Phan, A.; Edwards, C.L.; Robinson, E.L. The assessment of pain and discomfort in individuals with mental retardation. Res. Dev. Disabil. 2005, 26, 433–439. [Google Scholar] [CrossRef]
- Defrin, R.; Lotan, M.; Pick, C.G. The evaluation of acute pain in individuals with cognitive impairment: A differential effect of the level of impairment. Pain 2006, 124, 312–320. [Google Scholar] [CrossRef]
- Valkenburg, A.J.; Boerlage, A.A.; Ista, E. The COMFORT- behavior scale is useful to assess pain and distress in 0- to 3-year-old children with Down syndrome. Pain 2011, 152, 2059–2064. [Google Scholar] [CrossRef] [PubMed]
- Barney, C.C.; Hoch, J.; Byiers, B.; Dimian, A.; Symons, F.J. A Case-controlled Investigation of Pain Experience and Sensory Function in Neuronal Ceroid Lipofuscinosis. Clin. J. Pain 2015, 31, 998–1003. [Google Scholar] [CrossRef][Green Version]
- Rattaz, C.; Dubois, A.; Michelon, C.; Viellard, M.; Poinso, F.; Baghdadli, A. How do children with autism spectrum disorders express pain? A comparison with developmentally delayed and typically developing children. Pain 2013, 154, 2007–2013. [Google Scholar] [CrossRef]
- Aguilar Cordero, M.J.; Mur Villar, N.; GarcíaGarcía, I. Evaluation of pain in healthy newborns and in newborns with developmental problems (down syndrome). Pain Manag. Nurs. 2015, 16, 267–272. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, H.M.; Marschik, P.B.; Khwaja, O.S.; Ho, E.; Barnes, K.V.; Clarkson, T.W.; Bruck, N.M.; Kaufmann, W.E. Detecting autonomic response to pain in Rett syndrome. Dev. Neurorehabil. 2017, 20, 108–114. [Google Scholar] [CrossRef]
- Symons, F.J.; Harper, V.; Shinde, S.K. Evaluating a sham-controlled sensory-testing protocol for nonverbal adults with neurodevelopmental disorders: Self-injury and gender effects. J. Pain 2010, 11, 773–781. [Google Scholar] [CrossRef]
- Shinde, S.K.; Danov, S.; Chen, C.C. Convergent validity evidence for the Pain and Discomfort Scale (Pads) for pain assessment among adults with intellectual disability. Clin. J. Pain 2014, 30, 536–543. [Google Scholar] [CrossRef]
- Barney, C.C.; Tervo, R.; Wilcox, G.L.; Symons, F.J. A Case-Controlled Investigation of Tactile Reactivity in Young Children with and Without Global Developmental Delay. Am. J. Intellect Dev. Disabil. 2017, 122, 409–421. [Google Scholar] [CrossRef]
- Barney, C.C.; Merbler, A.M.; Simone, D.A.; Walk, D.; Symons, F.J. Investigating the Feasibility of a Modified Quantitative Sensory Testing Approach to Profile Sensory Function and Predict Pain Outcomes Following Intrathecal Baclofen Implant Surgery in Cerebral Palsy. Pain Med. 2020, 21, 109–117. [Google Scholar] [CrossRef]
- de Knegt, N.; Defrin, R.; Schuengel, C.; Lobbezoo, F.; Evenhuis, H.; Scherder, E. Quantitative sensory testing of temperature, pain, and touch in adults with Down syndrome. Res. Dev. Disabil 2015, 47, 306–317. [Google Scholar] [CrossRef]
- Benromano, T.; Pick, C.G.; Merick, J.; Defrin, R. Physiological and Behavioral Responses to Calibrated Noxious Stimuli among Individuals with Cerebral Palsy and Intellectual Disability. Pain Med. 2017, 18, 441–453. [Google Scholar] [CrossRef]
- Benromano, T.; Pick, C.G.; Granovsky, Y.; Defrin, R. Increased Evoked Potentials and Behavioral Indices in Response to Pain among Individuals with Intellectual Disability. Pain Med. 2017, 18, 1715–1730. [Google Scholar] [CrossRef]
- Defrin, R.; Pick, C.G.; Peretz, C.; Carmeli, E. A quantitative somatosensory testing of pain threshold in individuals with mental retardation. Pain 2004, 108, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Valkenburg, A.J.; Tibboel, D.; van Dijk, M. Pain sensitivity of children with Down syndrome and their siblings: Quantitative sensory testing versus parental reports. Dev. Med. Child. Neurol. 2015, 57, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Ekman, P.; Friesen, W. Investigators Guide to the Facial Action Coding System; Consulting Psychologist Press: Palo Alto, CA, USA, 1978. [Google Scholar]
- Prkachin, K.M.; Mercer, S.R. Pain expression in patients with shoulder pathology: Validity, properties and relationship to sickness impact. Pain 1989, 39, 257–265. [Google Scholar] [CrossRef]
- Kunz, M.; Meixner, D.; Lautenbacher, S. Facial muscle movements encoding pain-a systematic review. Pain 2019, 160, 535–549. [Google Scholar] [CrossRef]
- Bergström-Isacsson, M.; Lagerkvist, B.; Holck, U.; Gold, C. How facial expressions in a Rett syndrome population are recognised and interpreted by those around them as conveying emotions. Res. Dev. Disabil. 2013, 34, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Kunz, M.; Scharmann, S.; Hemmeter, U.; Schepelmann, K.; Lautenbacher, S. The facial expression of pain in patients with dementia. Pain 2007, 133, 221–228. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Takeda, K.; Onishi, M.; Deguchi, M.; Higashi, T. Non-verbal communication method based on a biochemical marker for people with severe motor and intellectual disabilities. J. Int. Med. Res. 2006, 34, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Susam, B.T.; Akcakaya, M.; Nezamfar, H.; Diaz, D.; Xu, X.; de Sa, V.R.; Craig, K.D.; Huang, J.S.; Goodwin, M.S. Automated Pain Assessment using Electrodermal Activity Data and Machine Learning. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2018, 2018, 372–375. [Google Scholar] [PubMed]
- Weiner, D.; Peterson, B.; Keefe, F. Chronic pain-associated behaviors in the nursing home: Resident versus caregiver perceptions. Pain 1999, 80, 577–588. [Google Scholar] [CrossRef]
- Rainville, P.; Bao, Q.V.; Chrétien, P. Pain-related emotions modulate experimental pain perception and autonomic responses. Pain 2005, 118, 306–318. [Google Scholar] [CrossRef]
- Jeanne, M.; Logier, R.; De Jonckheere, J.; Tavernier, B. Heart rate variability during total intravenous anesthesia: Effects of nociception and analgesia. Auton. Neurosci. Basic Clin. 2009, 147, 91e96.14. [Google Scholar] [CrossRef] [PubMed]
- Riquelme, I.; Montoya, P. Developmental changes in somatosensory processing in cerebral palsy and healthy individuals. Clin. Neurophysiol. 2010, 121, 1314–1320. [Google Scholar] [CrossRef]
- Riquelme, I.; Cifre, I.; Montoya, P. Are physiotherapists reliable proxies for the recognition of pain in individuals with cerebral palsy? A cross sectional study. Disabil. Health J. 2015, 8, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Priano, L.; Miscio, G.; Grugni, G.; Milano, E.; Baudo, S.; Sellitti, L.; Picconi, R.; Mauro, A. On the origin of sensory impairment and altered pain perception in Prader-Willi syndrome: A neurophysiological study. Eur. J. Pain 2009, 13, 829–835. [Google Scholar] [CrossRef]
- Bembich, S.; Morabito, G.; Simeon, V.; Strajn, T.; Rutigliano, R.; Di Rocco, P.; Cont, G.; Risso, F.M.; Peri, F.; Barbi, E. Venipuncture activates the cerebral cortex in children with intellectual disability. Arch. Dis. Child. 2020, 106, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Vega, J.N.; Hohman, T.J.; Pryweller, J.R.; Dykens, E.M.; Thornton-Wells, T.A. Resting-state functional connectivity in individuals with Down syndrome and Williams syndrome compared with typically developing controls. Brain Connect. 2015, 5, 461–475. [Google Scholar] [CrossRef] [PubMed]
- Wilson, L.R.; Vatansever, D.; Annus, T.; Williams, G.B.; Hong, Y.T.; Fryer, T.D.; Nestor, P.J.; Holland, A.J.; Zaman, S.H. Differential effects of Down’s syndrome and Alzheimer’s neuropathology on default mode connectivity. Hum. Brain Mapp. 2019, 40, 4551–4563. [Google Scholar] [CrossRef] [PubMed]
- Shiohama, T.; Levman, J.; Baumer, N.; Takahashi, E. Structural Magnetic Resonance Imaging-Based Brain Morphology Study in Infants and Toddlers with Down Syndrome: The Effect of Comorbidities. Pediatr. Neurol. 2019, 100, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Kucyi, A.; Davis, K.D. The Neural Code for Pain: From Single-Cell Electrophysiology to the Dynamic Pain Connectome. Neuroscientist 2017, 23, 397–414. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Gadotti, V.M.; Chen, L.; Souza, I.A.; Huang, S.; Wang, D.; Ramakrishnan, C.; Deisseroth, K.; Zhang, Z.; Zamponi, G.W. A neuronal circuit for activating descending modulation of neuropathic pain. Nat. Neurosci. 2019, 22, 1659–1668. [Google Scholar] [CrossRef]
- Bromley, J.; Emerson, E.; Caine, A. The development of a self-report measure to assess the location and intensity of pain in people with intellectual disabilities. J. Intellect Disabil. Res. 1998, 42, 72–80. [Google Scholar] [CrossRef]
- de Knegt, N.C.; Evenhuis, H.M.; Lobbezoo, F.; Schuengel, C.; Scherder, E.J. Does format matter for comprehension of a facial affective scale and a numeric scale for pain by adults with down syndrome? Res. Dev. Disabil. 2013, 34, 3442–3448. [Google Scholar] [CrossRef]
- Wingert, J.R.; Sinclair, R.J.; Dixit, S.; Damiano, D.L.; Burton, H. Somatosensory-evoked cortical activity in spastic diplegic cerebral palsy. Hum. Brain Mapp. 2010, 31, 1772–1785. [Google Scholar] [CrossRef] [PubMed]
- Chibnall, J.T.; Tait, R.C. Pain assessment in cognitively impaired and unimpaired older adults: A comparison of four scales. Pain 2001, 92, 173–186. [Google Scholar] [CrossRef]
- Hadden, K.L.; LeFort, S.; O’Brien, M.; Coyte, P.C.; Guerriere, D.N. A comparison of observers’ and selfreport pain ratings for children with cerebral palsy. J. Dev. Behav. Pediatr. 2015, 36, 14–23. [Google Scholar] [CrossRef]
- Hadjistavropoulos, T.; Craig, K.D. A theoretical framework for understanding self-report and observational measures of pain: A communications model. Behav. Res. Ther. 2002, 40, 551–570. [Google Scholar] [CrossRef]
- Breau, L.M.; Burkitt, C. Assessing pain in children with intellectual disabilities. Pain Res. Manag. 2009, 14, 116–120. [Google Scholar] [CrossRef]
- Genik, L.M.; McMurtry, C.M.; Breau, L.M. Caring for children with intellectual disabilities part 2: Detailed analyses of factors involved in respite workers’ reported assessment and care decisions. Res. Dev. Disabil. 2017, 63, 1–10. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Sex | Etiology | Age | ID Level | Medications |
|---|---|---|---|---|---|
| 1 | F | DS | 37 | Mild-moderate | Antihypothyroidism |
| 2 | F | DS | 34 | Mild | None |
| 3 | F | DS | 31 | Moderate | Muscle relaxants, steroids |
| 4 | F | DS | 31 | Moderate | Antipsychotic, muscle relaxants, steroids |
| 5 | M | DS | 32 | Moderate | Antihypothyroidism, antipsychotic |
| 5 | M | DS | 36 | Mild | Antihypothyroidism, antihypertention |
| 7 | F | DS | 33 | Mild-moderate | Muscle relaxants, antihypertention |
| 8 | F | DS | 37 | Mild-moderate | Antihypothyroidism, antihypertention |
| 9 | F | DS | 34 | Mild-moderate | Antihypothyroidism |
| 10 | M | UID | 49 | Mild | Antipsychotic, muscle relaxants |
| 11 | M | 40 | UID | Mild | None |
| 12 | M | 52 | UID | Mild-moderate | Antihyperthyroidism |
| 13 | M | UID | 38 | Mild-moderate | None |
| 14 | F | UID | 26 | Mild-moderate | Antipsychotic |
| 15 | M | UID | 40 | Mild | Antidepressant |
| 16 | M | UID | 27 | Mild | Antidepressant |
| 17 | F | UID | 50 | Moderate | Antihypertention |
| 18 | F | UID | 29 | Mild | Antiepileptic, antihypertension Antihypothyroidism, muscle relaxants |
| 50 kPa | 200 kPa | 400 kPa | |||||
|---|---|---|---|---|---|---|---|
| IDD | HC | IDD | HC | IDD | HC | Partial Eta2 | |
| Brow lowerer (AU4) | 0.83 (1.5) * | 0.0 (0) | 1.11 (1.7) | 0.57 (1.3)# | 1.29 (1.9) | 1.14 (1.9) | 0.002 |
| Cheek raiser (AU6) | 0.61 (1.4) # * | 0.0 (0) | 1.56 (2.2) # ** | 0.05 (0.2) | 2.06 (2.3) | 0.86 (1.5) | 0.096 * |
| Lid tightened (AU7) | 0.89 (1.7) # * | 0.0 (0) | 2.11 (2.2) # ** | 0.43 (1.0) # | 2.88 (2.4) * | 1.24 (2.0) | 0.131 * |
| Nose wrinkle (AU9) | 0.28 (0.9) # | 0.0 (0) | 1.22 (2.1) * | 0.0 (0) | 1.24 (2.0) | 0.52 (1.4) | 0.046 |
| Upper lip raiser (AU10) | 0.39 (1.2) # | 0.0 (0) | 1.33 (2.0) ** | 0.05(0.2) # | 1.88 (2.2) | 0.90 (1.8) | 0.062 |
| Lip corner puller (AU12) | 0.44 (1.3) # | 0.0 (0) | 1.50 (2.1) # ** | 0.0(0) # | 2.12 (2.4) | 1.14 (2.1) | 0.049 |
| Lip stretcher (AU20) | 0.44 (1.3) | 0.0 (0) | 1.00 (1.5) ** | 0.05 (0.2) # | 0.94 (1.6) | 1.14 (1.9) | 0.0030 |
| Lip pressor (AU24) | 0.44 (1.4) | 0.05 (0.2) | 0.56 (1.3) | 0.10 (0.3) | 0.59 (1.3) | 0.71 (1.6) | 0.002 |
| Lips part (AU25) | 1.00 (1.5) # * | 0.0 (0) | 1.44 (1.8) # ** | 0.0 (0) | 1.88 (1.9) * | 0.71 (1.9) | 0.095 * |
| Jaw dropper (AU26) | 0.72 (1.0 ** | 0.0 (0) | 0.89 (1.4) ** | 0.0 (0) | 1.35 (1.9) | 0.57 (1.5) | 0.053 |
| Mouth stretch (AU27) | 0.29 (0.6) * | 0.0 (0) | 0.72 (1.5) * | 0.0 (0) | 0.94 (1.7) | 0.29 (1.1) | 0.0540 |
| Eyelid drop (AU41) | 0.72 (1.2) * | 0.05 (0.2) # | 0.89 (1.4) | 1.05 (1.8) # | 1.06 (1.8) | 1.86 (2.3) | 0.037 |
| Eyes closed (AU43) | 0.33 (1.2) # | 0.05 (0.2) | 1.39 (2.1) | 0.38 (1.1) # | 1.82 (2.1) | 1.52 (2.2) | 0.005 |
| Blink (AU45) | 1.22 (1.3) | 1.00 (0.9) # | 1.00 (1.6) | 1.95 (1.6) | 0.35 (0.8) *** | 2.43 (1.8) | 0.346 *** |
| FACS | Pyramid Scale | NRS | HR | HRV | PPGA | GSR | ||
|---|---|---|---|---|---|---|---|---|
| Simulation intensity | ID | 0.41 ** | 0.57 *** | 0.38 ** | −0.05 | −0.24 | 0.11 | 0.23 |
| HC | 0.41 ** | 0.89 *** | 0.82 *** | −0.85 | 0.13 | −0.76 | 0.19 | |
| FACS | ID | 0.37 ** | 0.06 | 0.26 | 0.05 | 0.14 | 0.31 * | |
| HC | 0.44 ** | 0.49 *** | −0.09 | 0.05 | −0.09 | −0.05 | ||
| Pyramid scale | ID | 0.68 *** | −0.31 * | −0.15 | −0.37 ** | −0.04 | ||
| HC | 0.94 *** | −0.13 | 0.05 | −0.04 | 0.21 | |||
| NRS | ID | −0.18 | 0.02 | −0.16 | −0.05 | |||
| HC | −0.02 | −0.01 | 0.07 | 0.16 | ||||
| HR | ID | −0.27 * | 0.07 | 0.33 * | ||||
| HC | −0.35 ** | 0.34 ** | 0.27 * | |||||
| HRV | ID | −0.18 | −0.17 | |||||
| HC | −0.37 ** | −0.05 | ||||||
| PPGA | ID | 0.39 ** | ||||||
| HC | −0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Defrin, R.; Benromano, T.; Pick, C.G. Specific Behavioral Responses Rather Than Autonomic Responses Can Indicate and Quantify Acute Pain among Individuals with Intellectual and Developmental Disabilities. Brain Sci. 2021, 11, 253. https://doi.org/10.3390/brainsci11020253
Defrin R, Benromano T, Pick CG. Specific Behavioral Responses Rather Than Autonomic Responses Can Indicate and Quantify Acute Pain among Individuals with Intellectual and Developmental Disabilities. Brain Sciences. 2021; 11(2):253. https://doi.org/10.3390/brainsci11020253
Chicago/Turabian StyleDefrin, Ruth, Tali Benromano, and Chaim G. Pick. 2021. "Specific Behavioral Responses Rather Than Autonomic Responses Can Indicate and Quantify Acute Pain among Individuals with Intellectual and Developmental Disabilities" Brain Sciences 11, no. 2: 253. https://doi.org/10.3390/brainsci11020253
APA StyleDefrin, R., Benromano, T., & Pick, C. G. (2021). Specific Behavioral Responses Rather Than Autonomic Responses Can Indicate and Quantify Acute Pain among Individuals with Intellectual and Developmental Disabilities. Brain Sciences, 11(2), 253. https://doi.org/10.3390/brainsci11020253