Feasibility of Using Foot–Ground Clearance Biofeedback Training in Treadmill Walking for Post-Stroke Gait Rehabilitation




Abstract

1. Introduction
2. Materials and Methods
2.1. Participants
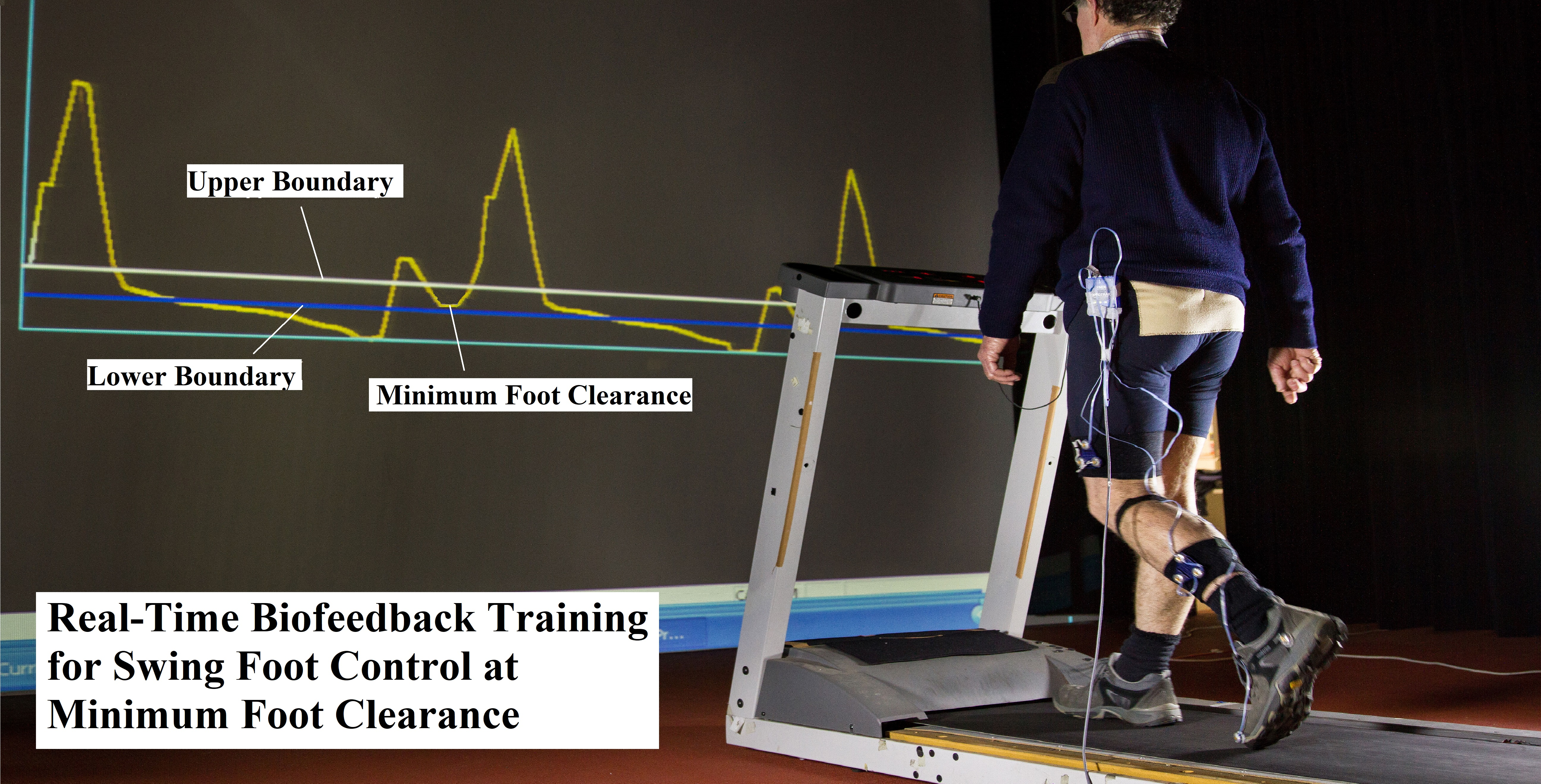
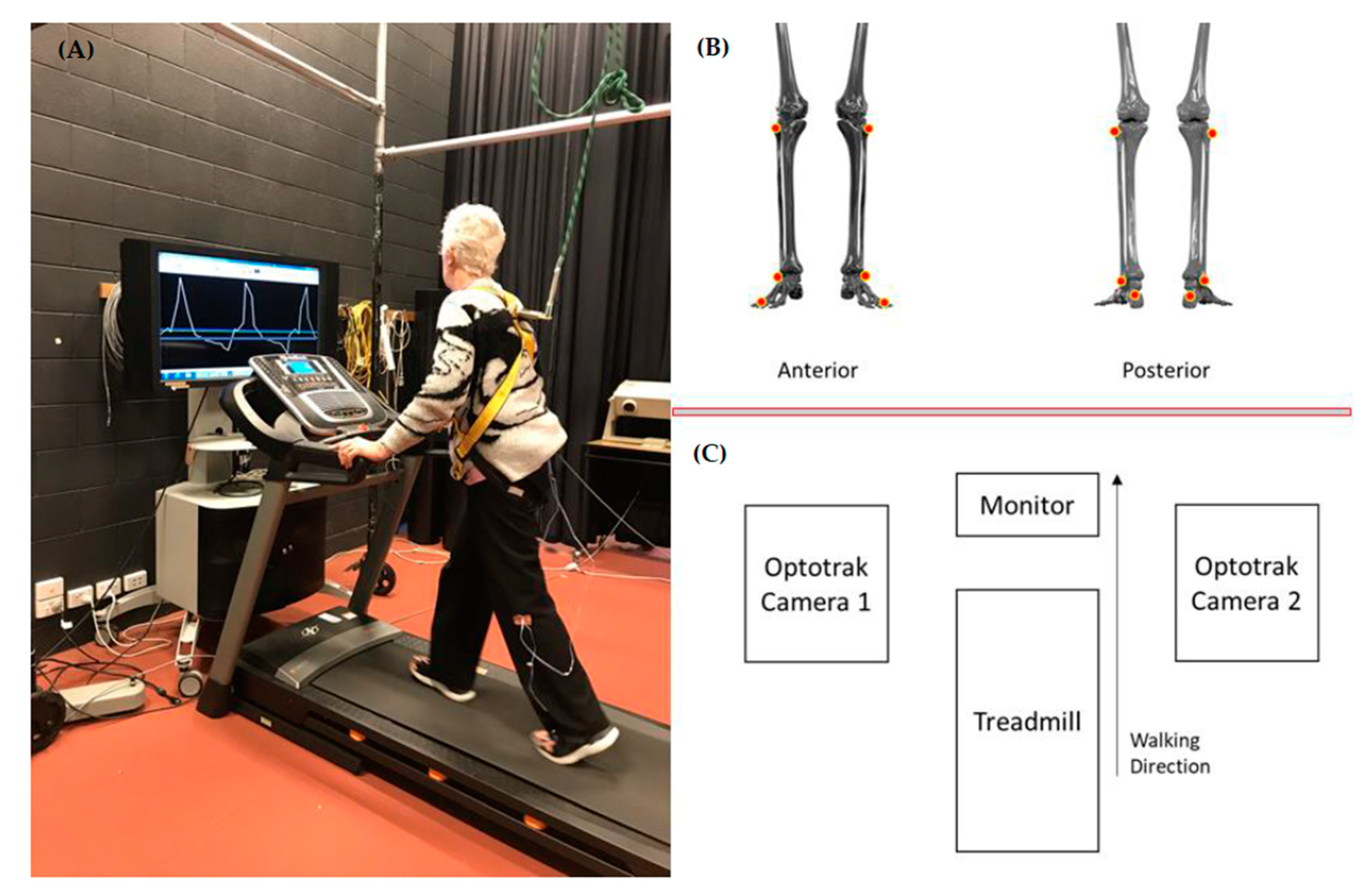
2.2. Testing and Biofeedback Training Protocol
2.3. Marker Setup and Data Analysis
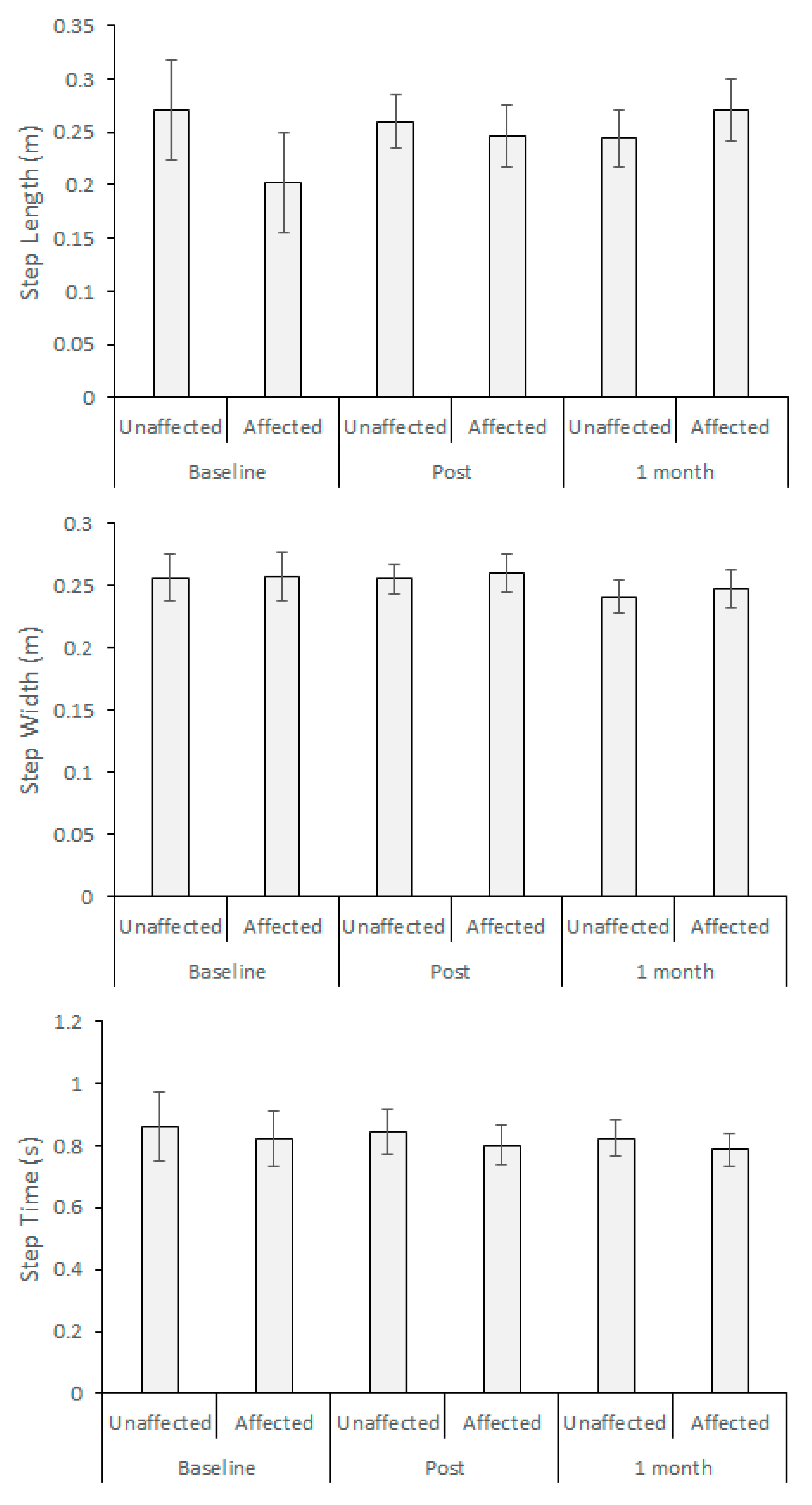
2.4. Spatio-Temporal Step Parameters
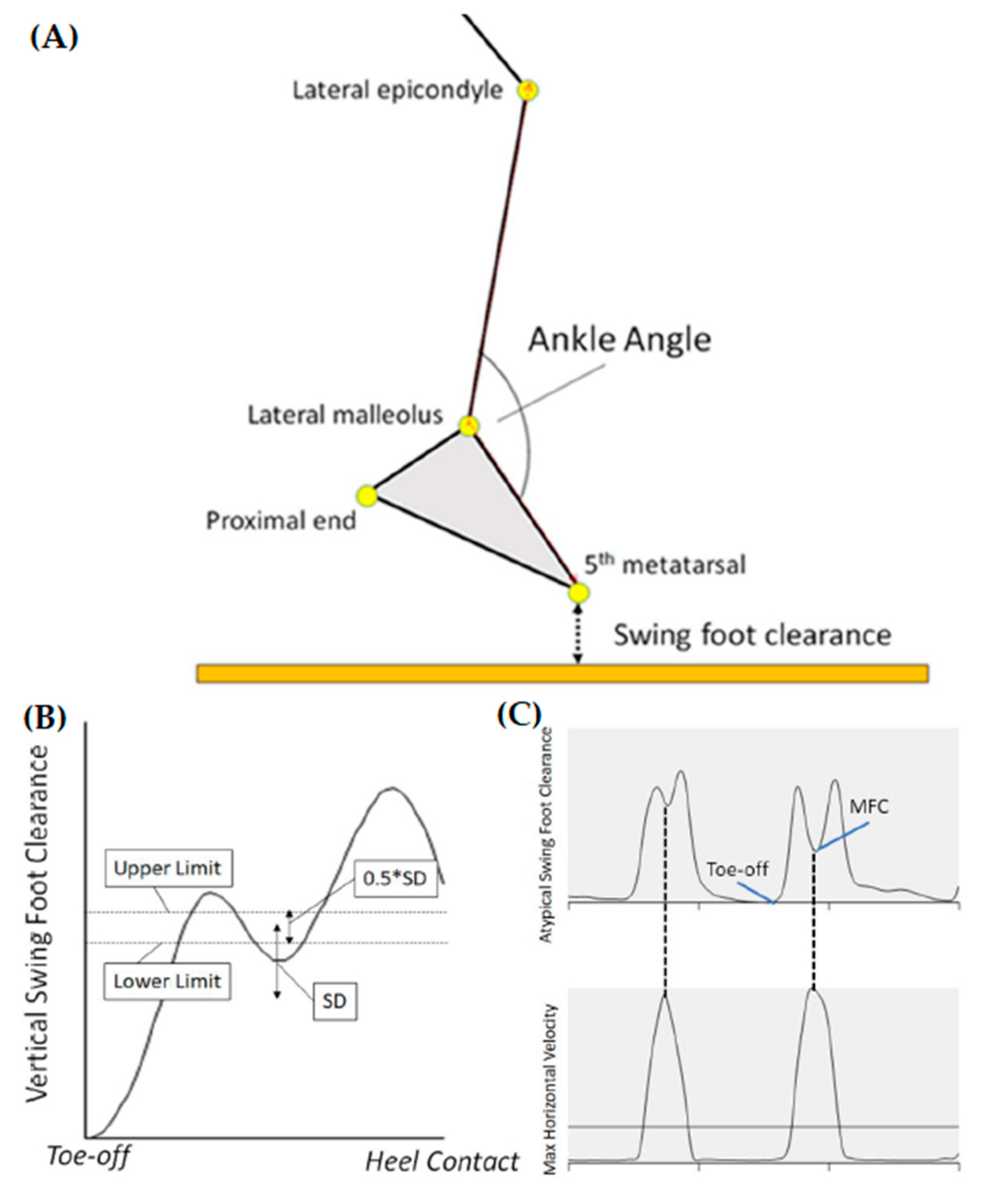
2.5. Minimum Foot Clearance (MFC)
2.6. Ankle Angle
2.7. Design and Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Australian Institute of Health and Welfare, Stroke. Available online: https://www.aihw.gov.au/reports/australias-health/stroke (accessed on 20 August 2020).
- Faralli, A.; Bigoni, M.; Mauro, A.; Rossi, F.; Carulli, D. Noninvasive strategies to promote functional recovery after stroke. Hindawi Neural Plast. 2013, 2013, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Blennerhassett, J.M.; Dite, W.; Ramage, E.R.; Richmond, M.E. Changes in balance and walking from stroke rehabilitation to the community: A follow-up observational study. Arch. Phys. Med. Rehabil. 2012, 93, 1782–1787. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, F.A.; Mackintosh, S.M.; Said, C.M.; Hill, K.D. Falls after stroke. Int. J. Stroke 2012, 7, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Mackintosh, S.; Hill, K.; Dodd, K.; Goldie, P.; Culham, E. Falls and injury prevention should be part of every stroke rehabilitation plan. Clin. Rehabil. 2005, 19, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Martin, K.D.; Polanski, W.; Schackert, G.; Sobottka, S.B. New therapeutic option for drop foot with the ActiGait peroneal nerve stimulator—A technical note. World Neurosurg. 2015, 84, 2037–2042. [Google Scholar] [CrossRef] [PubMed]
- Sulzer, J.S.; Gordon, K.E.; Dhaher, Y.Y.; Peshkin, M.A.; Patton, J.L. Preswing knee flexion assistance is coupled with hip abduction in people with stiff-knee gait after stroke. Stroke 2010, 41, 1709–1714. [Google Scholar] [CrossRef] [PubMed]
- Blake, A.J.; Morgan, K.; Bendall, M.J.; Dallosso, H.; Ebrahim, S.B.J.; Arie, T.H.D.; Fentem, P.H.; Bassey, E.J. Falls by elderly people at home prevalence and associated factors. Age Ageing 1988, 17, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Berg, W.R.; Alessio, H.M.; Mills, E.M.; Tong, C. Circumstances and consequences of falls in independent community dwelling older adults. Age Ageing 1997, 26, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Smeesters, C.; Hayes, W.C.; McMahon, T.A. Disturbance type and gait speed affect fall direction and impact location. J. Biomech. 2001, 34, 309–317. [Google Scholar] [CrossRef]
- Begg, R.; Best, R.; Dell’Oro, L.; Taylor, S. Minimum foot clearance during walking: Strategies for the minimisation of trip-related falls. Gait Posture 2007, 25, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.A. The Biomechanics and Motor Control of Human Gait: Normal, Elderly and Pathological, 2nd ed.; Waterloo Biomechanics: Waterloo, ON, Canada, 1991. [Google Scholar]
- Sadeghi, H.; Allard, P.; Prince, F.; Labelle, H. Symmetry and limb dominance in able-bodied gait: A review. Gait Posture 2000, 12, 34–45. [Google Scholar] [CrossRef]
- Tirosh, O.; Cambell, A.; Begg, R.K.; Sparrow, W.A. Biofeedback training effects on minimum toe clearance variability during treadmill walking. Ann. Biomed. Eng. 2012, 41, 1661–1669. [Google Scholar] [CrossRef] [PubMed]
- Begg, R.K.; Tirosh, O.; Said, C.M.; Sparrow, W.A.; Steinberg, N.; Levinger, P.; Galea, M.P. Gait training with real-time augmented toe-ground clearance information decreases tripping risk in older adults and a person with chronic stroke. Front. Hum. Neurosci. 2014, 8, 243. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Kim, H.B.; Wold, S.L.; Kesarl, T.M. Comparison of the immediate effects of audio, visual, or audiovisual gait biofeedback on propulsive force generation in able-bodies and post-stroke individuals. Appl. Psychophysiol. Biofeedback 2020, 45, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Nagano, H.; Begg, R.; Sparrow, W.; Taylor, S. A comparison of treadmill and overground walking effects on step cycle variability and asymmetry in young and older individuals. J. Appl. Biomech. 2012, 29, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Nagano, H.; Begg, R.; Sparrow, W.; Taylor, S. Ageing and limb dominance effects on foot-ground clearance during treadmill and overground walking. Clin. Biomech. 2011, 26, 962–968. [Google Scholar] [CrossRef] [PubMed]
- Wass, E.; Taylor, N.; Matsas, A. Familiarisation to treadmill walking in unimpaired older people. Gait Posture 2005, 21, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Alcock, L.; Galna, B.; Perkins, R.; Lord, S.; Rochester, L. Step length determines minimum toe clearance in older adults and people with Parkinson’s disease. J. Biomech. 2018, 11, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Moosabhoy, M.A.; Gard, S.A. Methodology for determining the sensitivity of swing leg toe clearance and leg length to swing leg joint angles during gait. Gait Posture 2006, 24, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, C.K.; Neptune, R.R.; Kautz, S.A. Variability in spatiotemporal step characteristics and its relationship to walking performance post-stroke. Gait Posture 2009, 29, 408–414. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Age (years) | Gait Speed (km/h) | Body Height (m) | Body Mass (kg) | Affected Limb | Time from Stroke (years) | Lesion Area | STREAM (20-Point Scale) |
|---|---|---|---|---|---|---|---|---|
| 1 | 70 | 1.0 | 1.56 | 66.3 | Right | 21.0 | SAH | 13 |
| 2 | 80 | 1.1 | 1.70 | 78.8 | Right | 0.8 | PICA | 18 |
| 3 | 76 | 0.4 | 1.61 | 80.0 | Left | 1.4 | MCA | 14 |
| 4 | 67 | 1.5 | 1.80 | 115.1 | Right | 0.8 | MCA | 20 |
| 5 | 78 | 1.8 | 1.71 | 85.3 | Left | 0.7 | ACA | 16 |
| 6 | 37 | 1.3 | 1.77 | 59.7 | Left | 1.1 | MCA | 15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagano, H.; Said, C.M.; James, L.; Begg, R.K. Feasibility of Using Foot–Ground Clearance Biofeedback Training in Treadmill Walking for Post-Stroke Gait Rehabilitation. Brain Sci. 2020, 10, 978. https://doi.org/10.3390/brainsci10120978
Nagano H, Said CM, James L, Begg RK. Feasibility of Using Foot–Ground Clearance Biofeedback Training in Treadmill Walking for Post-Stroke Gait Rehabilitation. Brain Sciences. 2020; 10(12):978. https://doi.org/10.3390/brainsci10120978
Chicago/Turabian StyleNagano, Hanatsu, Catherine M. Said, Lisa James, and Rezaul K. Begg. 2020. "Feasibility of Using Foot–Ground Clearance Biofeedback Training in Treadmill Walking for Post-Stroke Gait Rehabilitation" Brain Sciences 10, no. 12: 978. https://doi.org/10.3390/brainsci10120978
APA StyleNagano, H., Said, C. M., James, L., & Begg, R. K. (2020). Feasibility of Using Foot–Ground Clearance Biofeedback Training in Treadmill Walking for Post-Stroke Gait Rehabilitation. Brain Sciences, 10(12), 978. https://doi.org/10.3390/brainsci10120978