Double-Blinded Randomized Pilot Clinical Trial Comparing Cognitive Side Effects of Standard Ultra-Brief Right Unilateral ECT to 0.5 A Low Amplitude Seizure Therapy (LAP-ST)

 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Assessments
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Treatment Characteristics and Parameters
3.3. Cognitive Assessment
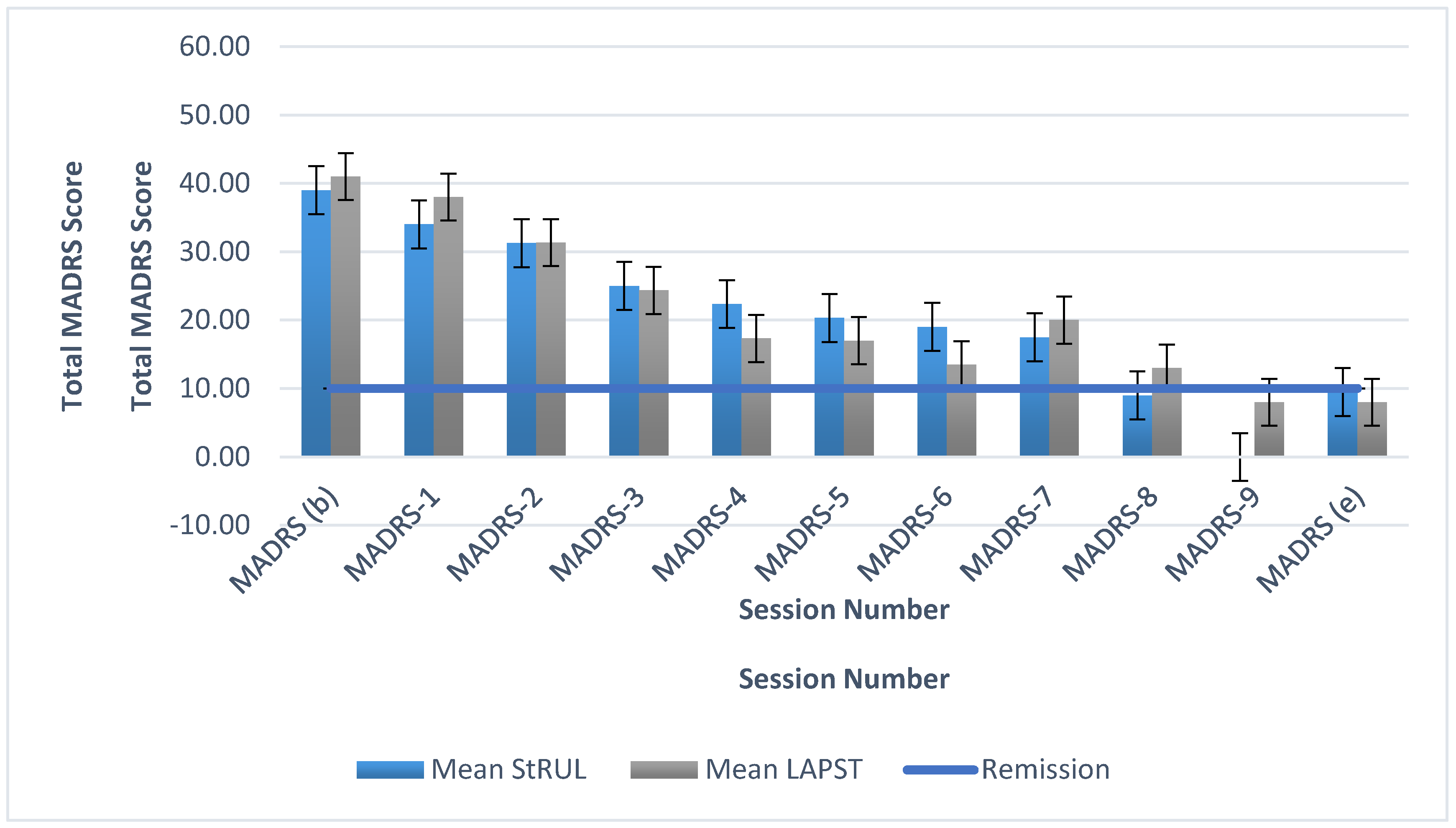
3.4. Efficacy Outcomes
4. Discussion
- (1)
- There is an age difference between the two studies, with no restriction to 50 years and older in our study.
- (2)
- (3)
- Another difference is the use of three arms and dividing the stimulation to ultra-brief, and then brief pulse amplitude. This may have reduced the power of the study and the effectiveness of randomization (final of N of 3, 4, and 2 for brief-pulse at the end of the study for the 600, 700, and 800 mA arms respectively). Our study had two arms and had also a small sample size with three participants in one arm and four in the other with ultrabrief pulse. The brief pulse amplitude in the 3 arm study may have also been less efficient that the ultra-brief pulse [33]; as “briefer pulses require less total energy and charge to induce seizures than do longer pulses” [33].
- (4)
- The current study was limited to all participants receiving RUL electrode placement, rather than allowing switching of some participants from RUL to BT within the study protocol.
- (5)
- In this current study, we only followed the titration without allowing for change in parameters based on clinician’s adjustment, in order to decrease variability between the arms of the study as much as possible.
- (6)
- The current study titration schedule allowed variability in frequency and train duration to simultaneously keep total dosage in terms of change similar and homogenous between the titration steps and treatment steps for the two arms of the study.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fava, M. Diagnosis and definition of treatment-resistant depression. Biol. Psychiatry 2003, 53, 649–659. [Google Scholar] [CrossRef]
- Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Warden, D.; Niederehe, G.; Thase, M.E.; Lavori, P.W.; Lebowitz, B.D.; et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: A STAR*D report. Am. J. Psychiatry 2006, 163, 1905–1917. [Google Scholar] [CrossRef] [PubMed]
- Mrazek, D.A.; Hornberger, J.C.; Altar, C.A.; Degtiar, I. A review of the clinical, economic, and societal burden of treatment-resistant depression: 1996–2013. Psychiatr. Serv. 2014, 65, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Szkultecka-Debek, M.; Miernik, K.; Stelmachowski, J.; Jakovljević, M.; Jukić, V.; Aadamsoo, K.; Janno, S.; Bitter, I.; Tolna, J.; Jarema, M.; et al. Schizophrenia causes significant burden to patients’ and caregivers’ lives. Psychiatr. Danub. 2016, 28, 104–110. [Google Scholar]
- Subedi, S.; Aich, T.K.; Sharma, N. Use of ECT in Nepal: A one year study from the country’s largest psychiatric facility. J. Clin. Diagn. Res. 2016, 10, VC01–VC04. [Google Scholar] [CrossRef]
- Murray, C.J.; Lopez, A.D. Alternative projections of mortality and disability by cause 1990–2020: Global burden of disease study. Lancet 1997, 349, 1498–1504. [Google Scholar] [CrossRef]
- UK ECT Review Group. Efficacy and safety of electroconvulsive therapy in depressive disorders: A systematic review and meta-analysis. Lancet 2003, 361, 799–808. [Google Scholar] [CrossRef]
- Prudic, J.; Sackeim, H. Electroconvulsive therapy and suicide risk. J. Clin. Psychiatry 1999, 60, 104–110. [Google Scholar]
- Kellner, C.H.; Husain, M.M.; Knapp, R.G.; McCall, W.V.; Petrides, G.; Rudorfer, M.V.; Young, R.C.; Sampson, S.; McClintock, S.M.; Mueller, M.; et al. Right unilateral ultrabrief pulse ECT in geriatric depression: Phase 1 of the PRIDE study. Am. J. Psychiatry 2016, 173, 1101–1109. [Google Scholar] [CrossRef]
- Youssef, N.A.; McCall, W.V. Relapse prevention after index electroconvulsive therapy in treatment-resistant depression. Ann. Clin. Psychiatry 2014, 26, 288–296. [Google Scholar]
- Kellner, C.H.; Husain, M.M.; Knapp, R.G.; McCall, W.V.; Petrides, G.; Rudorfer, M.V.; Young, R.C.; Sampson, S.; McClintock, S.M.; Mueller, M.; et al. A novel strategy for continuation ECT in geriatric depression: Phase 2 of the PRIDE study. Am. J. Psychiatry 2016, 173, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, C.; Khan, B.; Youssef, N.A. Need for standardization of measurement of time to reorientation as a predictor of cognitive adverse effects of electroconvulsive therapy. J. ECT 2020. [Google Scholar] [CrossRef]
- Sahlem, G.L.; McCall, W.V.; Short, E.B.; Rosenquist, P.B.; Fox, J.B.; Youssef, N.A.; Manett, A.J.; Kerns, S.E.; Dancy, M.M.; McCloud, L.; et al. A two-site, open-label, non-randomized trial comparing Focal Electrically-Administered Seizure Therapy (FEAST) and right unilateral ultrabrief pulse electroconvulsive therapy (RUL-UBP ECT). Brain Stimul. 2020, 13, 1416–1425. [Google Scholar] [CrossRef] [PubMed]
- Lisanby, S.H.; Luber, B.; Schlaepfer, T.E.; Sackeim, H.A. Safety and feasibility of magnetic seizure therapy (MST) in major depression: Randomized within-subject comparison with electroconvulsive therapy. Neuropsychopharmacology 2003, 28, 1852–1865. [Google Scholar] [CrossRef] [PubMed]
- Cronholm, B.; Ottosson, J.O. Ultrabrief stimulus technique in electroconvulsive therapy. I. Influence on retrograde amnesia of treatments with the Elther ES electroschock apparatus, Siemens Konvulsator III and of lidocaine-modified treatment. J. Nerv. Ment. Dis. 1963, 137, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Cronholm, B.; Ottosson, J.O. Ultrabrief stimulus technique in electroconvulsive therapy. II. Comparative studies of therapeutic effects and memory disturbances in treatment of endogenous depression with the Elther ES electroshock apparatus and Siemens Konvulsator III. J. Nerv. Ment. Dis. 1963, 137, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Weiner, R.D. ECT and seizure threshold: Effects of stimulus wave form and electrode placement. Biol. Psychiatry 1980, 15, 225–241. [Google Scholar]
- Squire, L.R.; Zouzounis, J.A. ECT and memory: Brief pulse versus sine wave. Am. J. Psychiatry 1986, 143, 596–601. [Google Scholar]
- Squire, L.R. ECT and memory loss. Am. J. Psychiatry 1977, 134, 997–1001. [Google Scholar]
- Squire, S.R.; Slater, P.C. Bilateral and unilateral ECT: Effects on verbal and nonverbal memory. Am. J. Psychiatry 1978, 135, 1316–1320. [Google Scholar]
- Sackeim, H.A.; Decina, P.; Kanzler, M.; Kerr, B.; Malitz, S. Effects of electrode placement on the efficacy of titrated, low-dose ECT. Am. J. Psychiatry 1987, 144, 1449–1455. [Google Scholar] [PubMed]
- Sackeim, H.A.; Portnoy, S.; Neeley, P.; Steif, B.L.; Decina, P.; Malitz, S. Cognitive consequences of low-dosage electroconvulsive therapy. Ann. N. Y. Acad. Sci. 1986, 462, 326–340. [Google Scholar] [CrossRef] [PubMed]
- Sackeim, H.A.; Prudic, J.; Devanand, D.P.; Kiersky, J.E.; Fitzsimons, L.; Moody, B.J.; McElhiney, M.C.; Coleman, E.A.; Settembrino, J.M. Effects of stimulus intensity and electrode placement on the efficacy and cognitive effects of electroconvulsive therapy. New Engl. J. Med. 1993, 328, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Sackeim, H.A.; Prudic, J.; Devanand, D.P.; Nobler, M.S.; Lisanby, S.H.; Peyser, S.; Fitzsimons, L.; Moody, B.J.; Clark, J. A prospective, randomized, double-blind comparison of bilateral and right unilateral electroconvulsive therapy at different stimulus intensities. Arch. Gen. Psychiatry 2000, 57, 425–434. [Google Scholar] [CrossRef]
- Sackeim, H.A.; Prudic, J.; Nobler, M.S.; Fitzsimons, L.; Lisanby, S.H.; Payne, N.; Berman, R.M.; Brakemeier, E.V.; Perera, T.; Devanand, D.P. Effects of pulse width and electrode placement on the efficacy and cognitive effects of electroconvulsive therapy. Brain Stimul. 2008, 1, 71–83. [Google Scholar] [CrossRef]
- Sienaert, P. Based on a true story? The portrayal of ECT in international movies and television programs. Brain Stimul. 2016, 9, 882–891. [Google Scholar] [CrossRef]
- Matthews, A.M.; Rosenquist, P.B.; McCall, W.V. Representations of ECT in English-language film and television in the new millennium. J. ECT 2016, 32, 187–191. [Google Scholar] [CrossRef]
- Patel, R.S.; Sreeram, V.; Thakur, T.; Bachu, R.; Youssef, N.A. A national study for regional variation of inpatient ECT utilization from 4,411 hospitals across the United States. Ann. Clin. Psychiatry 2019, 31, 200–208. [Google Scholar] [CrossRef]
- McCall, W.V.; Lisanby, S.H.; Rosenquist, P.B.; Dooley, M.; Husaind, M.M.; Knapp, R.G.; Petridese, G.; Rudorfer, M.V.; Young, R.C.; McClintock, S.M.; et al. Effects of continuation electroconvulsive therapy on quality of life in elderly depressed patients: A randomized clinical trial. J. Psychiatr. Res. 2018, 97, 65–69. [Google Scholar] [CrossRef]
- McCall, W.V.; Reboussin, D.; Prudic, J.; Haskette, R.F.; Isenberg, K.; Olfson, M.; Rosenquist, P.B.; Sackeim, H.A. Poor health-related quality of life prior to ECT in depressed patients normalizes with sustained remission after ECT. J. Affect. Disord. 2013, 147, 107–111. [Google Scholar] [CrossRef]
- McCall, W.V.; Rosenquist, P.B.; Kimball, J.; Haskett, R.; Isenberg, K.; Prudic, J.; Lasater, B.; Sackeim, H.A. Health-related quality of life in a clinical trial of ECT followed by continuation pharmacotherapy: Effects immediately after ECT and at 24 weeks. J. ECT 2011, 27, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Youssef, N.A.; Sidhom, E. Feasibility, safety, and preliminary efficacy of Low Amplitude Seizure Therapy (LAP-ST): A proof of concept clinical trial in man. J. Affect. Disord. 2017, 222, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Peterchev, A.V.; Rosa, M.A.; Deng, Z.D.; Prudic, J.; Lisanby, S.H. Electroconvulsive therapy stimulus parameters: Rethinking dosage. J. ECT 2010, 26, 159–174. [Google Scholar] [CrossRef]
- Deng, Z.D.; Lisanby, S.H.; Peterchev, A.V. Effect of anatomical variability on electric field characteristics of electroconvulsive therapy and magnetic seizure therapy: A parametric modeling study. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 22–31. [Google Scholar] [CrossRef]
- Peterchev, A.V.; Krystal, A.D.; Rosa, M.A.; Lisanby, S.H. Individualized low-amplitude seizure therapy: Minimizing current for electroconvulsive therapy and magnetic seizure therapy. Neuropsychopharmacology 2015, 40, 2076–2084. [Google Scholar] [CrossRef] [PubMed]
- Noda, Y.; Silverstein, W.K.; Barr, M.S.; Vila-Rodriguez, F.; Downar, J.; Rajji, T.K.; Fitzgerald, P.B.; Mulsant, B.H.; Vigod, S.N.; Daskalakis, Z.J.; et al. Neurobiological mechanisms of repetitive transcranial magnetic stimulation of the dorsolateral prefrontal cortex in depression: A systematic review. Psychol. Med. 2015, 45, 3411–3432. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, S.A.; Asberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Youssef, N.A.; Ravilla, D.; Patel, C.; Yassa, M.; Sadek, R.; Zhang, L.F.; McCloud, L.; McCall, W.V.; Rosenquist, P.B. Magnitude of reduction and speed of remission of suicidality for low amplitude seizure therapy (LAP-ST) compared to standard right unilateral electroconvulsive therapy: A pilot double-blinded randomized clinical trial. Brain Sci. 2019, 9, 99. [Google Scholar] [CrossRef]
- Sobin, C.; Sackeim, H.A.; Prudic, J.; Devanand, D.P.; Moody, B.J.; McElhiney, M.C. Predictors of retrograde amnesia following ECT. Am. J. Psychiatry 1995, 152, 995–1001. [Google Scholar]
- Martin, D.M.; Galvez, V.; Loo, C.K. Predicting retrograde autobiographical memory changes following electroconvulsive therapy: Relationships between individual, treatment, and early clinical factors. Int. J. Neuropsychopharmacol. 2015, 18. [Google Scholar] [CrossRef]
- Kellner, C.H.; Knapp, R.; Husain, M.M.; Rasmussen, K.; Sampson, S.; Cullum, M.; McClintock, S.M.; Tobias, K.G.; Martino, C.; Mueller, M.; et al. Bifrontal, bitemporal and right unilateral electrode placement in ECT: Randomised trial. Br. J. Psychiatry 2010, 196, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Loo, C.K.; Katalinic, N.; Smith, D.J.; Ingram, A.; Dowling, N.; Martin, D.; Addison, K.; Hadzi-Pavlovic, D.; Simpson, B.; Schweitz, I. A randomized controlled trial of brief and ultrabrief pulse right unilateral electroconvulsive therapy. Int. J. Neuropsychopharmacol. 2014, 18. [Google Scholar] [CrossRef] [PubMed]
- Abbott, C.C.; Quinn, D.; Miller, J.; Ye, E.; Iqbal, S.; Lloyd, M.; Jones, T.R.; Upston, J.; de Deng, Z.; Erhardt, E.; et al. Electroconvulsive therapy pulse amplitude and clinical outcomes. Am. J. Geriatr. Psychiatry 2020. [Google Scholar] [CrossRef] [PubMed]
- Lisanby, S.H.; McClintock, S.M.; Alexopoulos, G.; Bailine, S.H.; Bernhardt, E.; Briggs, M.C.; Cullum, C.M.; Deng, Z.; Dooley, M.; Geduldig, E.T.; et al. Neurocognitive effects of Combined Electroconvulsive Therapy (ECT) and venlafaxine in geriatric depression: Phase 1 of the PRIDE study. Am. J. Geriatr. Psychiatry 2020, 28, 304–316. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patient ID | Age | Gender | Race | Highest Education | Group | Included in the ITT Descriptive Analysis |
|---|---|---|---|---|---|---|
| 1 | 55 | Male | White | High School graduate | LAP-ST | Yes |
| 2 | 56 | Female | White | Some College | RUL | No |
| 3 | 44 | Male | Hispanic | High School graduate | RUL | No |
| 4 | 31 | Female | White | College | RUL | No |
| 5 | 51 | Female | White | College | RUL | Yes |
| 6 | 29 | Female | African American | College | RUL | No |
| 7 | 27 | Female | White | Some College | RUL | Yes |
| 8 | 47 | Male | African American | College | LAP-ST | Yes |
| 9 | 59 | Female | White | Master’s Degree | RUL | Yes |
| 10 | 24 | Male | White | Some College | LAP-ST | Yes |
| 11 | 24 | Male | White | Some College | RUL | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Youssef, N.A.; McCall, W.V.; Ravilla, D.; McCloud, L.; Rosenquist, P.B. Double-Blinded Randomized Pilot Clinical Trial Comparing Cognitive Side Effects of Standard Ultra-Brief Right Unilateral ECT to 0.5 A Low Amplitude Seizure Therapy (LAP-ST). Brain Sci. 2020, 10, 979. https://doi.org/10.3390/brainsci10120979
Youssef NA, McCall WV, Ravilla D, McCloud L, Rosenquist PB. Double-Blinded Randomized Pilot Clinical Trial Comparing Cognitive Side Effects of Standard Ultra-Brief Right Unilateral ECT to 0.5 A Low Amplitude Seizure Therapy (LAP-ST). Brain Sciences. 2020; 10(12):979. https://doi.org/10.3390/brainsci10120979
Chicago/Turabian StyleYoussef, Nagy A., William V. McCall, Dheeraj Ravilla, Laryssa McCloud, and Peter B. Rosenquist. 2020. "Double-Blinded Randomized Pilot Clinical Trial Comparing Cognitive Side Effects of Standard Ultra-Brief Right Unilateral ECT to 0.5 A Low Amplitude Seizure Therapy (LAP-ST)" Brain Sciences 10, no. 12: 979. https://doi.org/10.3390/brainsci10120979
APA StyleYoussef, N. A., McCall, W. V., Ravilla, D., McCloud, L., & Rosenquist, P. B. (2020). Double-Blinded Randomized Pilot Clinical Trial Comparing Cognitive Side Effects of Standard Ultra-Brief Right Unilateral ECT to 0.5 A Low Amplitude Seizure Therapy (LAP-ST). Brain Sciences, 10(12), 979. https://doi.org/10.3390/brainsci10120979