
A Scoping Review on On-Road Risks Associated with Driving with Dementia: Implications for Driving Technology Advancements


Abstract
1. Overview
2. Background
3. Driving Technology for Individuals with Dementia
4. Problem Statement
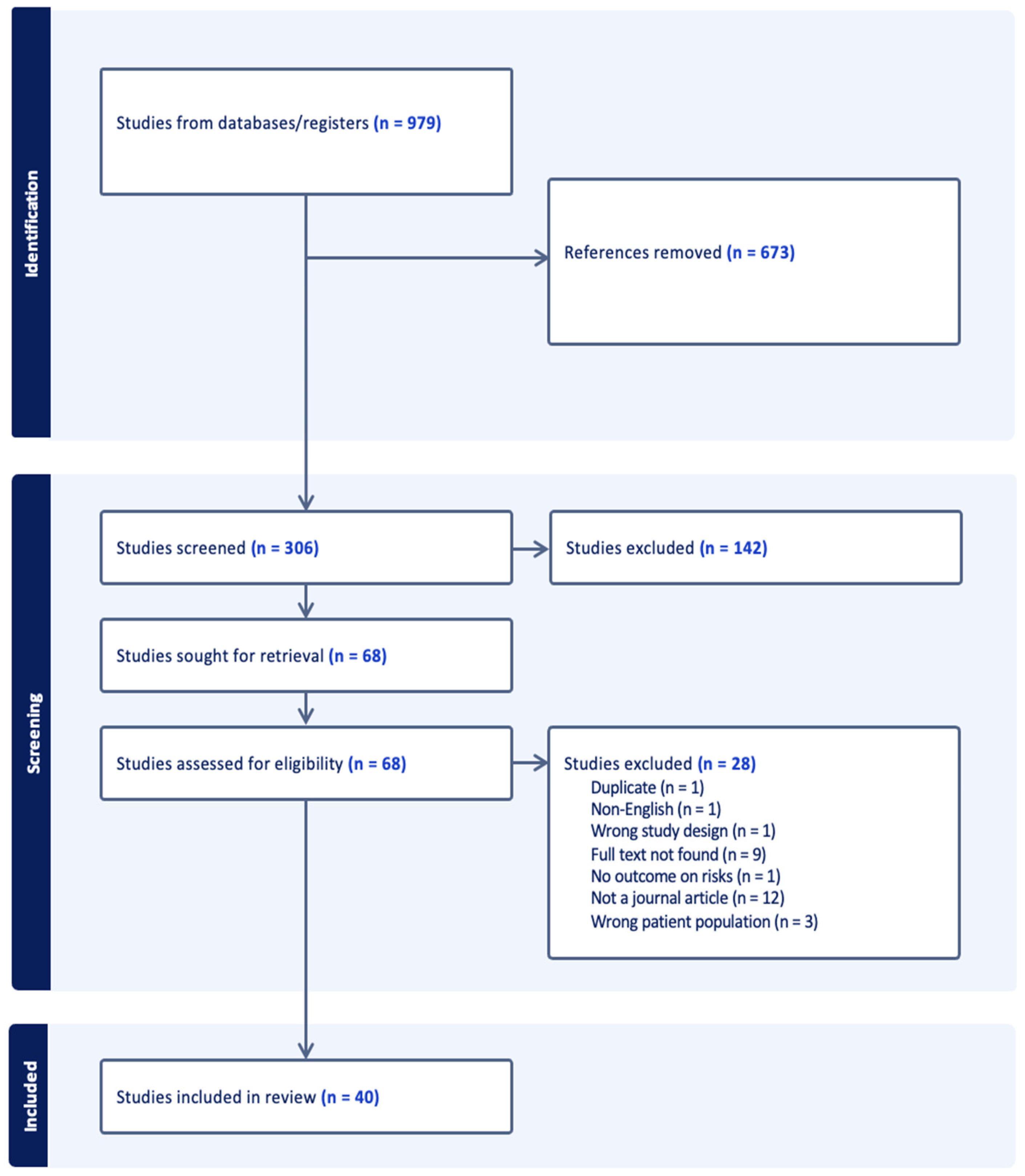
5. Methods
6. Findings
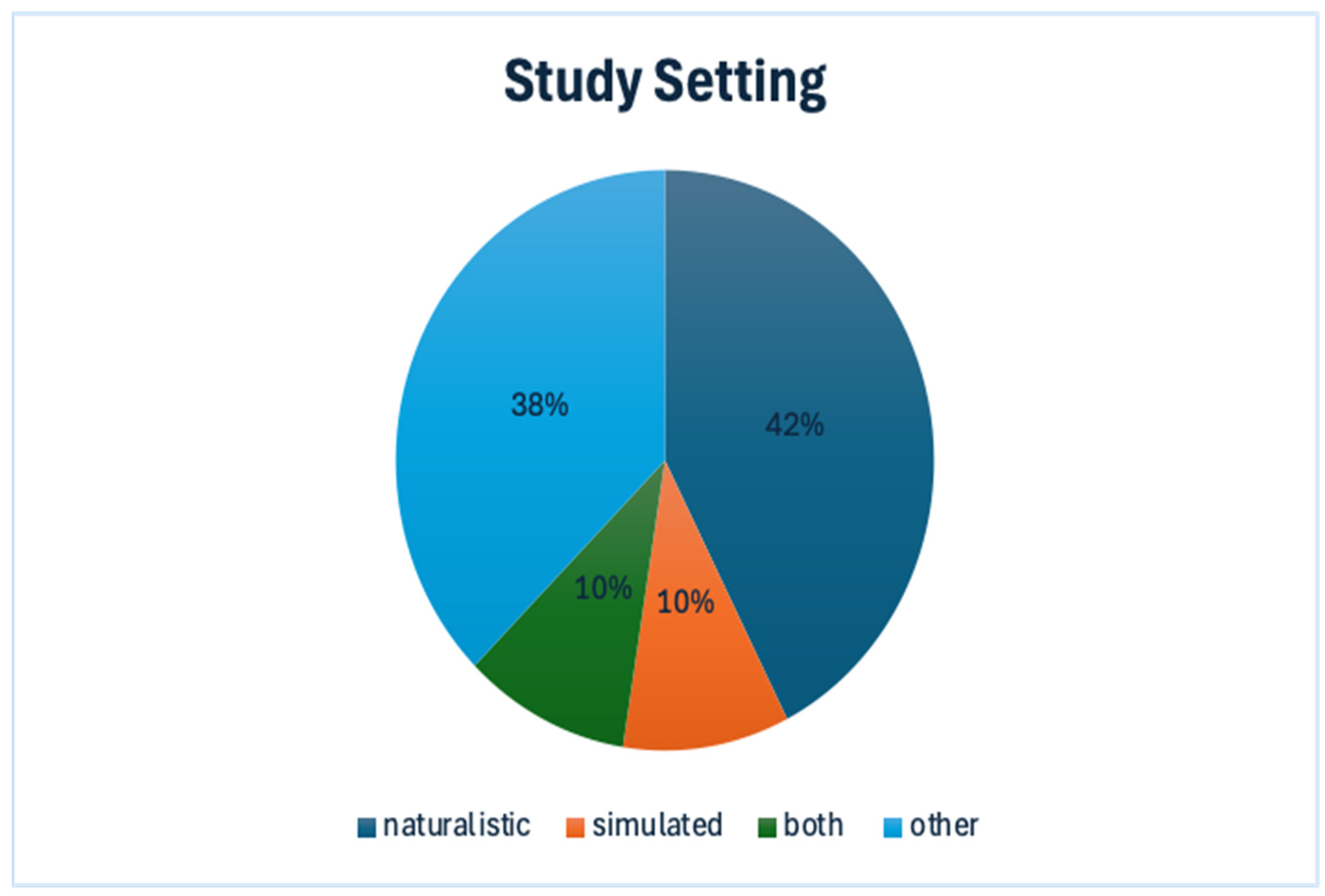
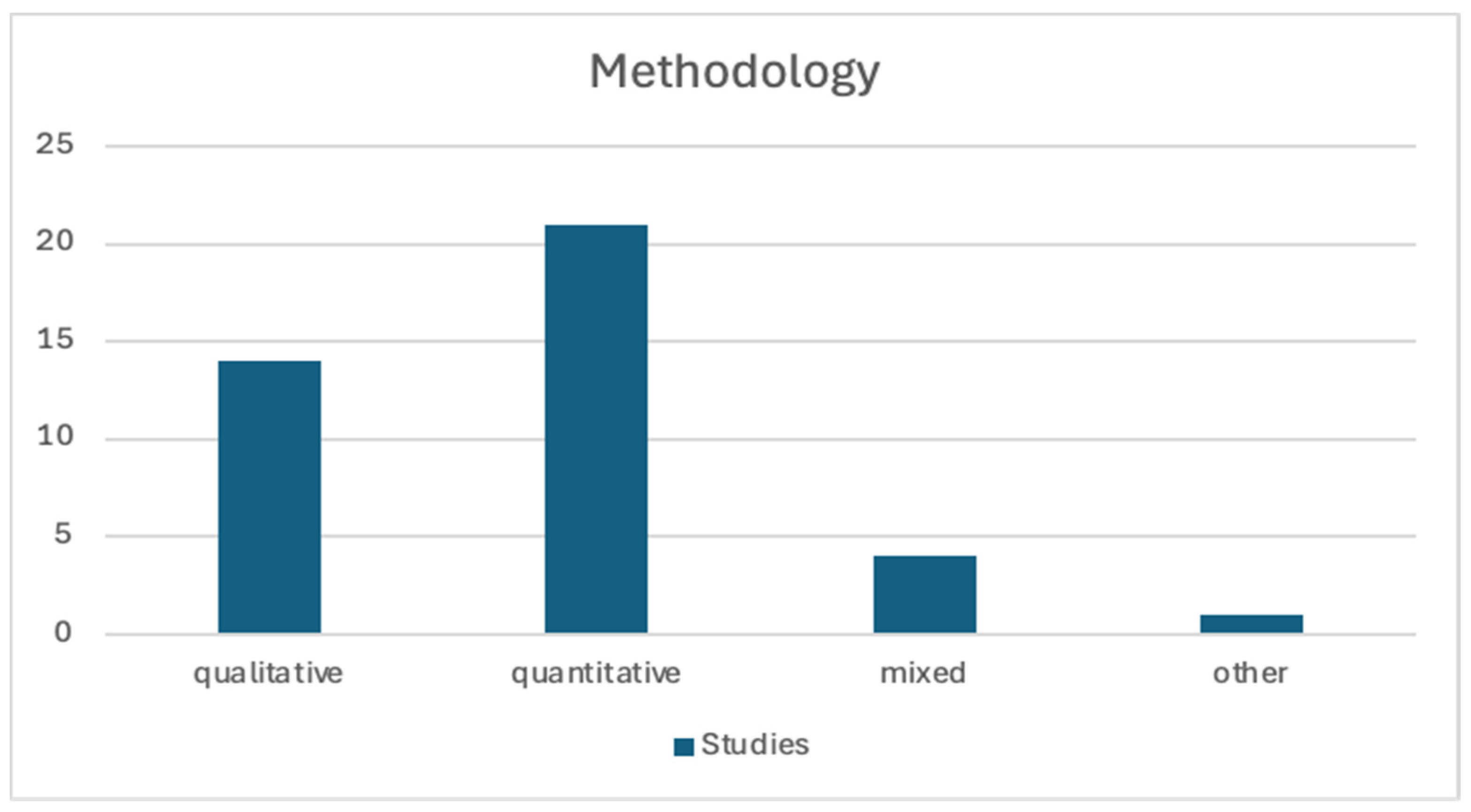
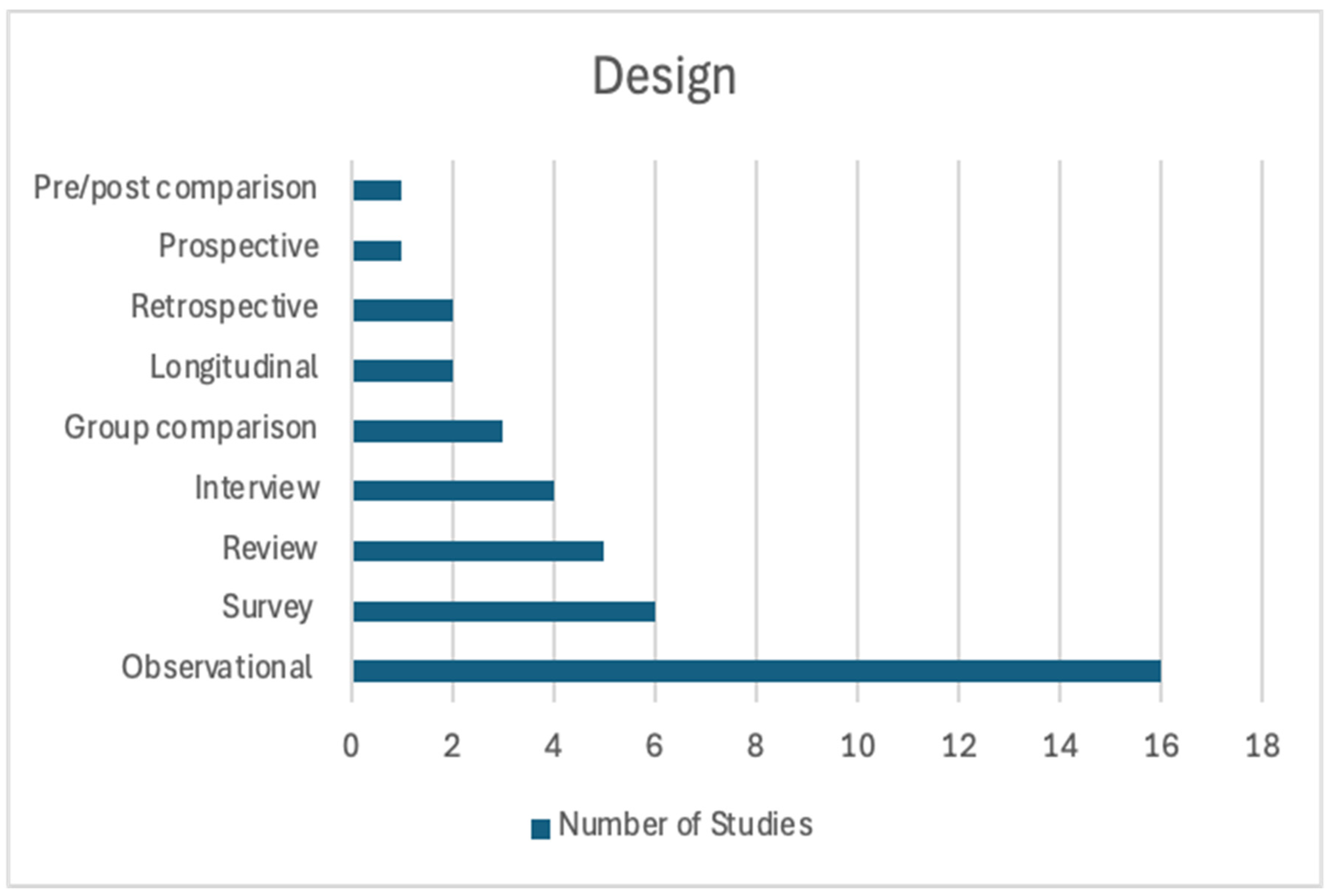
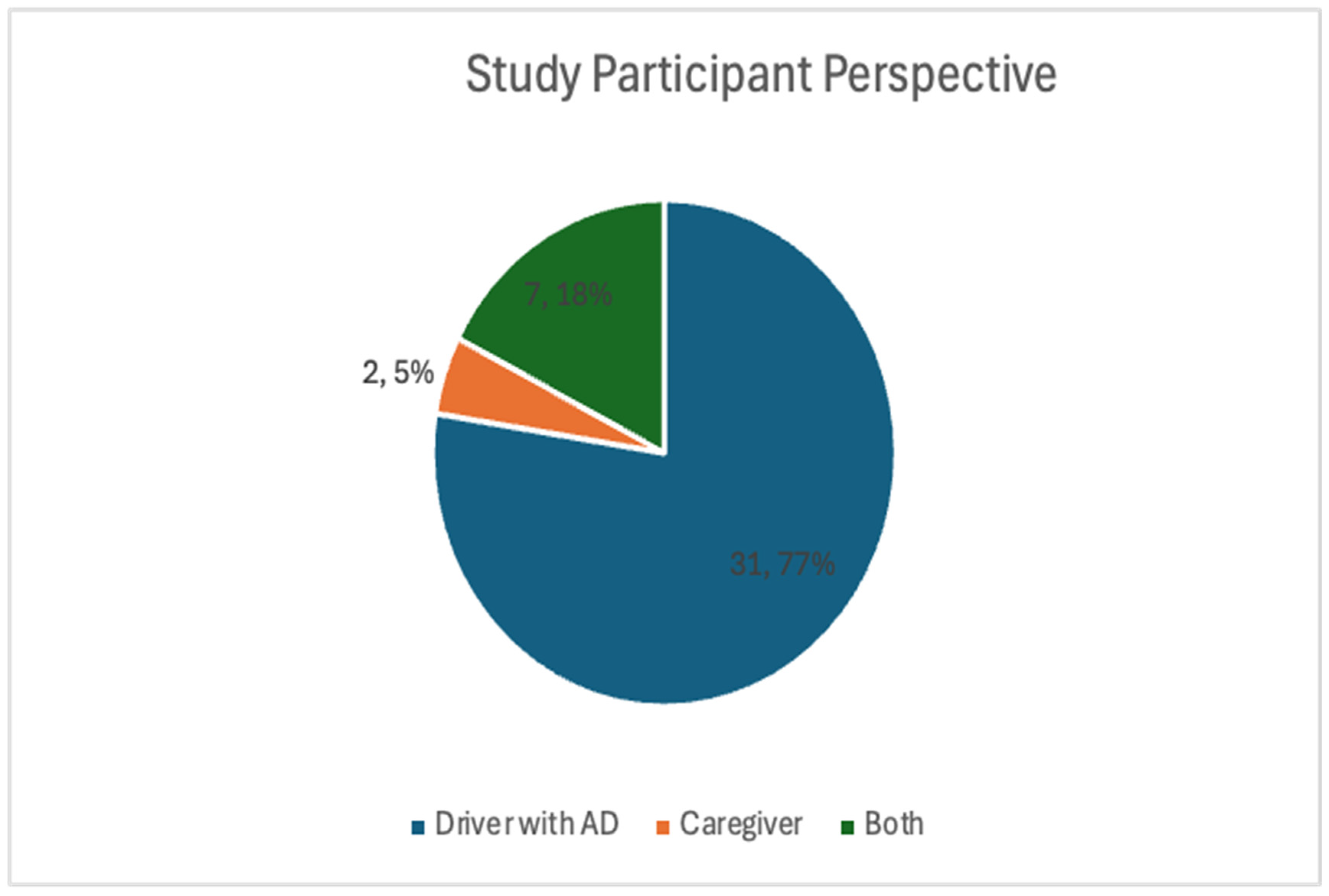
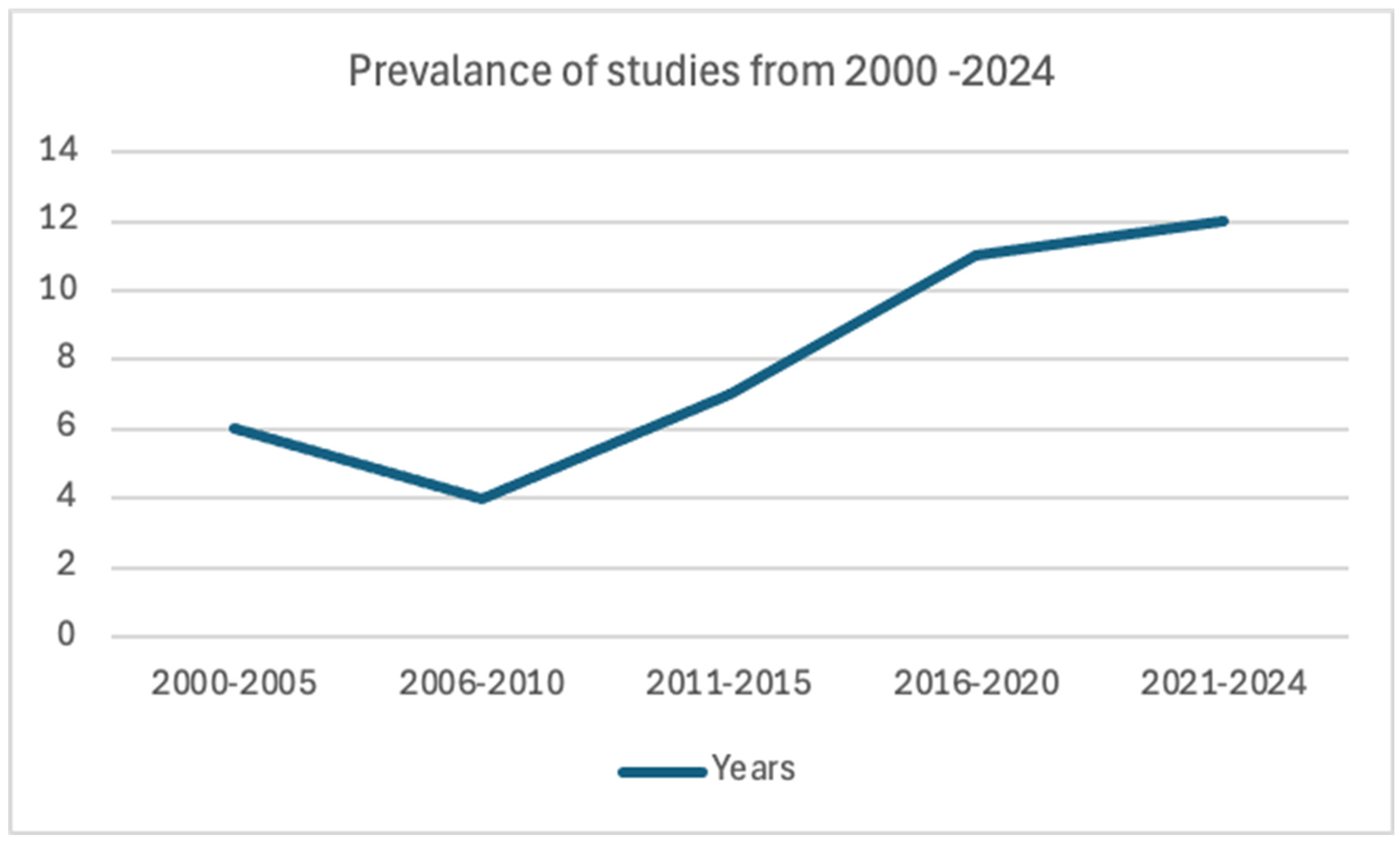
6.1. The Corpus
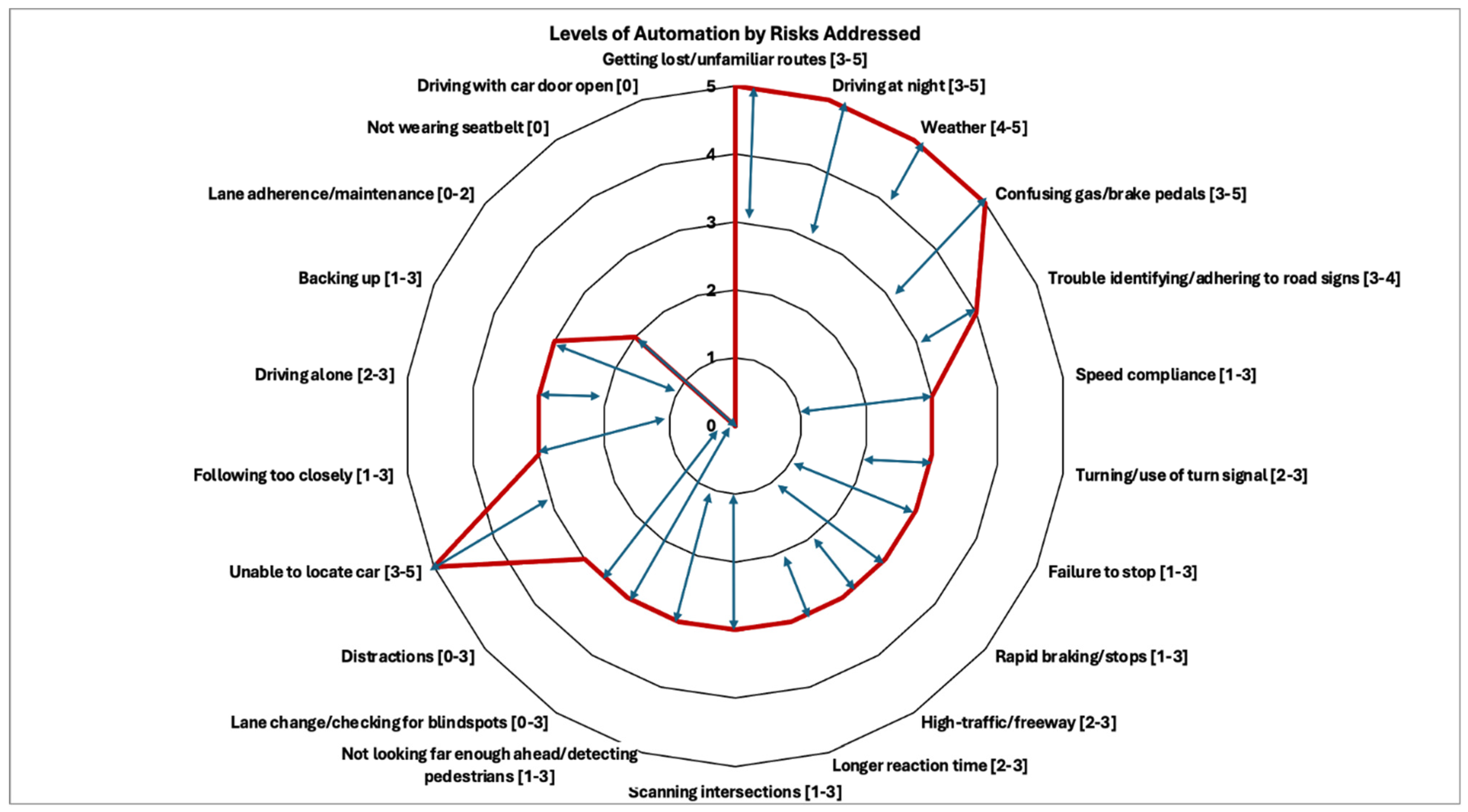
6.2. Risk Factors When Driving with Dementia
7. Discussion
7.1. Implications
7.2. Strengths and Limitations
8. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Aging and Disability Transportation Center. Accessible Transportation for People Living with Dementia. Available online: https://www.nadtc.org/news/blog/accessible-transportation-for-people-living-with-dementia/ (accessed on 29 September 2024).
- Bayne, A.; Siegfried, A.; Beck, L.F.; Freund, K. Barriers and facilitators of older adults’ use of ride share services. J. Transp. Health 2021, 21, 101055. [Google Scholar] [CrossRef] [PubMed]
- Kramarow, E.A. National Health Statistics Reports. Center for Disease Control. Available online: https://www.cdc.gov/nchs/data/nhsr/nhsr203.pdf (accessed on 29 September 2024).
- Alzheimer’s Association. What Is Dementia? Alzheimer’s Disease and Dementia. 2024. Available online: https://www.alz.org/alzheimers-dementia/what-is-dementia (accessed on 16 October 2024).
- Fuermaier, A.B.M.; Piersma, D.; de Waard, D.; Davidse, R.J.; de Groot, J.; Doumen, M.J.A.; Bredewoud, R.A.; Claesen, R.; Lemstra, A.W.; Scheltens, P.; et al. Driving difficulties among patients with alzheimer’s disease and other neurodegenerative disorders. J. Alzheimer’s Dis. 2019, 69, 1019–1030. [Google Scholar] [CrossRef] [PubMed]
- Quintas, J.L.; Trindade, I.O.; Gameiro, K.S.; Pitta, L.S.; Camargos, E.F.; Nóbrega, O.T. Neuropsychological domains and fitness to drive in mild cognitive impairment or Alzheimer’s disease. Accid. Anal. Prev. 2023, 191, 107188. [Google Scholar] [CrossRef] [PubMed]
- Hird, M.A.; Egeto, P.; Fischer, C.E.; Naglie, G.; Schweizer, T.A. A systematic review and meta-analysis of on-road simulator and cognitive driving assessment in Alzheimer’s disease and mild cognitive impairment. J. Alzheimer’s Dis. 2016, 53, 713–729. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.B.; Ott, B.R. Driving and dementia: A review of the literature. J. Geriatr. Psychiatry Neurol. 2004, 17, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Drachman, D.A.; Swearer, J.M. Driving and Alzheimer’s disease: The risk of crashes. Neurology 1993, 43, 2448–2456. [Google Scholar] [CrossRef] [PubMed]
- Braitman, K.A.; Kirley, B.B.; Ferguson, S.; Chaudhary, N.K. Factors leading to older drivers’ intersection crashes. Traffic Inj. Prev. 2007, 8, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Fraade-Blanar, L.A.; Hansen, R.N.; Chan, K.C.; Sears, J.M.; Thompson, H.J.; Crane, P.K.; Ebel, B.E. Diagnosed dementia and the risk of motor vehicle crash among older drivers. Accid. Anal. Prev. 2018, 113, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Almeida, W.M.; Quintas, J.L.; Trindade, I.O.A.; Pitta, L.S.R.; Louzada, L.L.; Nóbrega, O.T.; Camargos, E.F. Diagnosis of Alzheimer’s dementia and vehicle driving restriction: A scoping review. Psychogeriatrics 2024, 24, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Devlin, A.; McGillivray, J.; Charlton, J.; Lowndes, G.; Etienne, V. Investigating driving behaviour of older drivers with mild cognitive impairment using a portable driving simulator. Accid. Anal. Prev. 2012, 49, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Dementia Care Central. Driving & Dementia/Alzheimer’s: State Laws, Coping & Advice for Caregivers. Available online: https://www.dementiacarecentral.com/caregiverinfo/driving-problems (accessed on 10 October 2024).
- United States Environmental Protection Agency. Self-Driving Vehicles. Available online: https://www.epa.gov/greenvehicles/self-driving-vehicles (accessed on 10 October 2024).
- Scoblete, G. The Emerging Risks of Level 3 Autonomous Vehicles. Verisk. Available online: https://core.verisk.com/Insights/Emerging-Issues/Articles/2024/September/Week-4/The-Emerging-Risks-of-Level-3-Autonomous-Vehicles (accessed on 31 September 2024).
- Haghzare, S.; Stasiulis, E.; Delfi, G.; Mohamud, H.; Rapoport, M.J.; Naglie, G.; Mihailidis, A.; Campos, J.L. Automated vehicles for people with dementia: A “tremendous potential” that “has ways to go”—Reports of a qualitative study. Gerontol. 2022, 63, 140–154. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.; Owens, M. Self-regulation of driving behaviors in persons with early-stage Alzheimer’s disease. J. Gerontol. Nurs. 2021, 47, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Duchek, J.M.; Carr, D.B.; Hunt, L.; Roe, C.M.; Xiong, C.; Shah, K.; Morris, J.C. Longitudinal driving performance in early-stage dementia of the Alzheimer type. J. Am. Geriatr. Soc. 2003, 51, 1342–1347. [Google Scholar] [CrossRef] [PubMed]
- Hemmy, L.; Rottunda, S.; Adler, G. The Older Driver with Cognitive Impairment: Perceptions of Driving Ability and Results of a Behind the Wheel Test. Geriatrics 2016, 1, 6. [Google Scholar] [CrossRef] [PubMed]
- Detjen, H.; Schneegass, S.; Geisler, S.; Kun, A.; Sundar, V. An emergent design framework for accessible and inclusive future mobility. In Proceedings of the 14th International Conference on Automotive User Interfaces and Interactive Vehicular Applications, Seoul, Republic of Korea, 17–20 September 2022; pp. 1–12. [Google Scholar] [CrossRef]
- Society of Automobile Engineers. Taxonomy and Definitions for Terms Related to Driving Automation Systems for On-Road Vehicles. 2021. Available online: https://www.sae.org/standards/content/j3016_202104/ (accessed on 2 December 2024).
- Miller, L.; Koniakowsky, I.M.; Kraus, J.; Baumann, M. The impact of expectations about automated and manual vehicles on drivers’ behavior: Insights from a mixed traffic driving simulator study. In Proceedings of the 14th International Conference on Automotive User Interfaces and Interactive Vehicular Applications, Seoul, Republic of Korea, 17–20 September 2022; pp. 150–161. [Google Scholar] [CrossRef]
- Davis, J.D.; Babulal, G.M.; Papandonatos, G.D.; Burke, E.M.; Rosnick, C.B.; Ott, B.R.; Roe, C.M. Evaluation of naturalistic driving behavior using in-vehicle monitoring technology in preclinical and early Alzheimer’s disease. Front. Psychol. 2020, 11, 596257. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Area | Boolean Operators | Inclusion | Exclusion | |
|---|---|---|---|---|
| P* | -Older adults -Alzheimer’s disease -Dementia -Mild Cognitive Impairment -Cognition -Aging | dementia* OR alzheimer* OR mild cognitive impairment OR cognitive disorder AND Older adults | -Individuals with dementia, Alzheimer’s, mild cognitive impairment, and preclinical Alzheimer markers -Caregiver perspective -Mini-Mental State Examination (MMSE) score below 23 | -Healthy older adults -Individuals with comorbidities -No defined population -Expert opinion -Focus on attitudes and quality of life |
| C | -Driving cessation -Driving technology -Driving simulator -Driving rehabilitation | driving OR [driving technology] OR driving cessation OR driving behaviors OR driving simulator | -Naturalistic -Simulated driving scenarios -Training/intervention programs | -Legislation focus -Law enforcement focus |
| C | -Accidents -Safety -Risks -Decision making | safety OR acciden* OR injur* OR risk factors OR decision making OR limitations | -Describes cause of accident | -No outcome for on-road related risks -Disconnect between body functions and driving outcomes -Results described risks of general aging not specific to AD/MCI/dementia |
| Title | PMID |
|---|---|
| Predictors of accidents in people with mild cognitive impairment, mild dementia due to Alzheimer’s disease and healthy controls in simulated driving | 32249449 |
| Occupational Therapy Interventions to Improve Driving Performance in older people with mild cognitive impairment or early-stage dementia: A systematic review | 34780644 |
| Driving cessation and self-reported car crashes in older drivers: The impact of cognitive impairment and dementia in a population-based study | 18503033 |
| Impact of cognitive impairment on driving behaviour and route choices of older drivers: A real-world driving study | 38898026 |
| Computer-Based Driving in Dementia Decision Tool With Mail Support: Cluster Randomized Controlled Trial | 29802093 |
| Development of a decision-making tool for reporting drivers with mild dementia and mild cognitive impairment to transportation administrators | 28325164 |
| Driving Ability Evaluation and Rehabilitation for People With Alzheimer’s Disease and Related Dementias | 35984740 |
| Line 1 | dementia* OR alzheimer* OR mild cognitive impairment OR cognitive disorder |
| Line 2 | driving OR [driving technology] OR driving cessation OR driving behaviors OR driving simulator |
| Line 3 | safety OR acciden* OR injur* OR risk factors OR decision making OR limitations |
| Line 4 | AND Older adults |
| Risks | Cognitive Skills | Inclusive Mobility Application Categories | Specific Features of Driving Automation | Additional After-Market Technology (*) |
|---|---|---|---|---|
| Speed compliance * (n = 24) | Attentional capacity, visual perception | -Safety | -Adaptive cruise control -Road speed limit indicator -Automated speed control | -Head-up digital (HUD) display GPS speedometer |
| Getting lost/unfamiliar routes * (n = 17) | Orientation, memory, executive functioning | -Orientation | -Automated navigation | -GPS navigation -GPS trackers |
| Turning/Use of turn signal (n = 17) | Visual–spatial, judgment, praxis, attention, reaction time | -Safety | -Automated navigation | |
| Lane adherence/maintenance (n = 15) | Visual–spatial, attention | -Safety | -Lane departure warning -Lane-keeping assistance | |
| Failure to stop (n = 13) | Reaction time, processing speed, attention | -Safety | -Traffic sign recognition and speed control | |
| Trouble identifying/adhering to road signs (n = 13) | Visual discrimination, visual memory, attention | -Safety -Orientation | -Traffic sign recognition and speed control | |
| Rapid braking/stops (n = 12) | Processing speed, visual–spatial, judgment | -Safety -Convenience | -Adaptive cruise control | -GPS trackers |
| Driving at night * (n = 11) | Judgment, visual–spatial, reaction time | -Safety -Orientation | -Automated navigation | -Anti-glare lenses -Thermal Infrared Night Vision Camera |
| High-traffic area/freeway (n = 10) | Attention, processing speed, judgment, visual–spatial | -Safety | -Lane centering -Adaptive cruise control -Automated lane change | |
| Longer reaction time (n = 9) | Processing speed, judgment, attention | -Safety -Convenience | -Automated braking | |
| Scanning intersections (n = 9) | Visual perception, attention, executive function | -Safety | -Traffic sign recognition and speed control -Alert driver of potential hazards | |
| Not looking far enough ahead/detecting pedestrians (n = 9) | Visual–spatial, attention, visual perception | -Safety | - Pedestrians alert -Automated braking -Automated navigation | |
| Lane change/ checking blindspots * (n = 9) | Attention, visual–spatial, decision making, impulse control | -Safety | -Blindspot warning -Automated lane change | -Blindspot mirrors |
| Weather (n = 7) | Judgment, problem-solving, executive function, visual–spatial | -Ride Configuration -Convenience -Safety | -Automated navigation -Adverse weather alerting | |
| Confusing gas/brake pedals (n = 4) | Processing speed, motor planning, executive function, procedural memory | -Safety | -Automated navigation -Automated parking | |
| Distractions * (n = 4) | Attention | -Safety | -Visual/audible alerting when distracted | |
| Not wearing seatbelt * (n = 3) | Executive function, memory | -Safety | -Seatbelt warning | -GPS trackers |
| Unable to locate car * (n = 3) | Spatial memory, orientation | -Convenience -Orientation | -Key fob panic button -Summon | -App called “My Car Finder” |
| Following too closely (n = 2) | Visual–spatial, judgment, attention, visual perception, decision making | -Safety | -Forward collision warning -Adaptive cruise control | |
| Driving alone * (n = 2) | Attention, memory, executive function | -Orientation -Ride Configuration | -Lane centering -Adaptive cruise control -Automated navigation | -GPS tracker -GPS navigation |
| Backing up * (n = 1) | Visual–spatial and perception, attention | -Safety | -Rear cross-traffic alert -Back up camera -Automated braking | -Backup camera |
| Driving with car door open (n = 1) | Attention, praxis, memory | -Safety -Convenience | -Door alert (visual and audible) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walker, C.M.; Herron, M.J.; Mirnig, A.G.; Kun, A.; Arthanat, S. A Scoping Review on On-Road Risks Associated with Driving with Dementia: Implications for Driving Technology Advancements. Appl. Sci. 2025, 15, 4832. https://doi.org/10.3390/app15094832
Walker CM, Herron MJ, Mirnig AG, Kun A, Arthanat S. A Scoping Review on On-Road Risks Associated with Driving with Dementia: Implications for Driving Technology Advancements. Applied Sciences. 2025; 15(9):4832. https://doi.org/10.3390/app15094832
Chicago/Turabian StyleWalker, Carly May, Makenzy Joy Herron, Alexander G. Mirnig, Andrew Kun, and Sajay Arthanat. 2025. "A Scoping Review on On-Road Risks Associated with Driving with Dementia: Implications for Driving Technology Advancements" Applied Sciences 15, no. 9: 4832. https://doi.org/10.3390/app15094832
APA StyleWalker, C. M., Herron, M. J., Mirnig, A. G., Kun, A., & Arthanat, S. (2025). A Scoping Review on On-Road Risks Associated with Driving with Dementia: Implications for Driving Technology Advancements. Applied Sciences, 15(9), 4832. https://doi.org/10.3390/app15094832