Abstract
Cone-beam computed tomography (CBCT) remains the diagnostic modality of choice. The involvement of the cortical bone and adjacent teeth can be easily established via CBCT. Magnetic resonance can be helpful in the estimation of any other soft-tissue tumour spread within this anatomical area. The soft, hard-tissue, or mixed aetiology of tumours requires a differential diagnosis and accurate evaluation. If such pathologies arise, an adequate biopsy or incisional biopsy is essential to evaluate the type of tumour histopathologically. The occurrence of some neural tumours in the oral cavity is rare. Schwannomas (SCs), like some neuromas and other types of neural tumours, are rare and atypical. During clinical examination, a smooth, sponge-like, elastic mass could indicate other small salivary gland tumours rather than an oral neural tumour. Such pathologies of neural origins are quite rare and are uncommon findings in the oral cavity; therefore, their appearance may be conflated with other more typical benign or malignant tumours in the oral cavity. Establishing the status of bone via CBCT, the tooth involvement and the composition of the cortical bone may be helpful for establishing the best treatment of choice. The presented case report describes a rare schwannoma localised at the mandibular retromolar trigone.
1. Introduction
The mandibular retromolar triangle (retromolar triangle, fossa, MRT) is an anatomical area at the posterior part of the mandible. It is located distally from the last molar, at the edge of the alveolar rim of the mandibular body, and anteriorly from the ascending ramus of the mandible [1]. Quite commonly in this area, an additional retromolar foramen (RMF) can be found. This anatomical variation connects via a canal to the mandibular canal, and an additional neurovascular bundle can be found [2,3]. The approach to this mandible-associated anatomical area requires careful surgical planning.
Most commonly, the retromolar area of the mandible is associated with impacted molars (wisdom teeth), proximity to the inferior alveolar nerve (IAN), and sometimes even anatomical variations such as a bifid mandibular canal or a retromolar foramen [4]. On the medial side of the MRT, the lingual nerve might also be found. Many odontogenic cysts and mandibular fractures are often observed in this anatomical area, as are some odontogenic tumours, as well as other pathologies that may be present (e.g., pleomorphic adenoma or others) [4,5]. Both odontogenic and nonodontogenic pathologies can be found in this mandibular area. One of the rarest tumours found in the oral cavity is a neural tumour (<0.3–1%); therefore, care should always be taken to differentiate between lesions of odontogenic (cysts, tumours, abscesses, primary bone tumours) and nonodontogenic origins (salivary glands, secondary/metastatic tumours, oral cancers, squamous cell carcinomas), and other benign/malignant processes [4,5,6].
The schwannoma (SC, neurilemmoma, a Schwann cell tumour) is a rare neuroectodermal tumour arising in the oral cavity [4,5,6,7]. The first descriptive cases of the SC came in 1910, and the SC was described later by Stout in 1935. They are common in middle-aged adults (30–50 years of age), without any sex or age predilection. This rare solitary tumour is mostly a slow-growing, nontender rubbery mass that is asymptomatic, covered with the normal oral mucosa, and found accidentally in the oral cavity [7,8]. When present, its benign neurogenic origin is mostly associated with the presence of Schwann cells in the nerve sheath of the oral cavity. Currently, the SC is considered an atypical, benign tumour with well-defined borders and is a slow-growing encapsulated tumour arising from the local nerve trunk. Its malignant transformation is unlikely to occur. It might arise from various nerves; however, its occurrence is uncommon in the oral cavity (<1%), while approximately 20–40% of each SC might be found in the head and neck region. In the oral cavity, SCs are mostly associated with submucosal painless swelling and can be smooth and soft upon examination [9,10]. Oral mucocele, granuloma, lipoma, fibroma, small salivary gland tumours, sarcoma, carcinoma, leiomyoma, rhabdomyoma, haemangioma, lymphangioma, granular cell tumour, and others, such as dermoid cysts in the oral cavity floor, can be misdiagnosed. Atypically, it can be hard on palpation, mimicking a small salivary gland tumour. Because schwannomas arise from nerve sheets, their histopathological features include those of neuromas, neurofibromas, and tumours arising from bone, muscle, and adjacent soft tissues [7,8,9]. Surgical excision is the treatment of choice; however, recurrent SCs require more aggressive excision. The overall prognosis remains good, with a slight chance of recurrence, while malignant transformation remains unclear [10,11,12]. Some authors indicate that the tongue is the most common site of schwannoma, and some rare possible transformations could be related to this occurrence [9,10,11,12]. Other potential sites of schwannoma occurrence in the oral cavity include the tongue, cheek, buccal mucosa, jaw bones, floor of the mouth, posterior intraosseous mandibular areas, mucobuccal vestibular area, and lips [13,14,15,16]. In rare cases, intraosseous mandibular schwannomas might cause pain, nerve compression, local numbness (paraesthesia, Vin-cent sign), cortical expansion, and other atypical symptoms [11,12,13]. In some cases, schwannomas can be associated with a hypoglossal nerve in the floor of the mouth, as reported by Zhong et al. However, as suggested by Lee et al., when present in the tongue or floor of the mouth, schwannomas can cause pain, dysphonia, dysphagia, tongue-limited movements, and sometimes other atypical symptoms [13,14,15,16]. SCs occur as an ONT (oral neural tumour) in the oral cavity in approximately 1% of cases, with the tongue and the floor of the mouth being the most common sites, more common than the mandibular retromolar trigone area. The latter is a very rare site of occurrence. As described in the following text, the studies on this topic are limited, and accurate comparisons are missing in the known literature. Yet, so far, just a few cases of MRT oral SC have been found [14,15,16,17,18].
In the present case, we will briefly describe this rare occurrence of an SC and present how the close proximity of any impacted teeth might mimic odontogenic lesions, while a soft and spongy consistency should prompt differentiation from a small salivary gland tumour.
2. Case Description
The following case report is rare and quite unusual because of the occurrence of a neural tumour in the mandibular retromolar area. Because of some atypical features and rare NT locations, a detailed case study will be written according to the CARE guidelines [17].
A 40-year-old patient was referred from a local dental office because of soft swelling in the right mandibular retromolar area. The lesion slowly grew over a long period, was symptomless, and was evaluated in time as a part of the swollen gums or pericoronal tissue enlargement overlying the impacted right mandibular wisdom teeth (Figure 1). Since the tissue had enlarged in time without any pericoronitis, inflammation, or changes in the bone area surrounding the impacted third molar, the patient was scheduled for consultation only because of the following atypical features of the lesion.

Figure 1.
Preoperative panx (panoramic radiograph) showing four fully visible retained wisdom teeth (18, 28, 38, 48) and no osteolytic changes in the right retromolar mandibular trigone. The impacted left mandibular wisdom teeth had a visible follicular-like cyst appearance surrounding the crown; the fully retained right wisdom teeth are fully embedded in the bone in an ankylotic-like manner, without any cysts, in direct proximity to the inferior alveolar nerve.
During the intraoral examination, in the right MRT area, a soft, well-defined mass measuring approximately 15 mm × 10 mm that was painless and had a smooth, fibro-elastic texture was observed. The soft-tumour mass did not bleb upon palpation, was symptomless and partially movable, and was partially well attached to the bone of the MRT. Adjacent teeth remained smooth and healthy, without any visible inflammation, irritation, or tumour infiltration. The tumour was elastic and covered with reddish-like swollen mucosa without any fluctuations; however, it contained some firm and solid structures. The mucosa covering the lesion lacked any abrasions, ulcerations, or any other atypical features (Figure 2).

Figure 2.
Intraoral photograph of the right mandibular retromolar trigone soft-tissue tumour.
The patient was a generally healthy male without any history of surgery, illness, or surgery in the oral cavity region. The occurrence time of this lesion and its growth duration were not established. All of the surrounding anatomical areas and spaces were free of any diseases. Routine panoramic radiography (panx) and cone-beam computed tomography (CBCT) excluded any major changes in the bone near the tumour and excluded any potential odontogenic cause of the MRT swelling. The cortical parts of the bone in the CBCT study were also normal. No bone erosions, infiltrations, tooth resorptions, or bone swelling were detected (Figure 3). Because of the lack of substantial bone involvement, except for the impacted right mandibular wisdom molar with visible signs of bone ankylosis, suspicion of a nonodontogenic tumour was established.
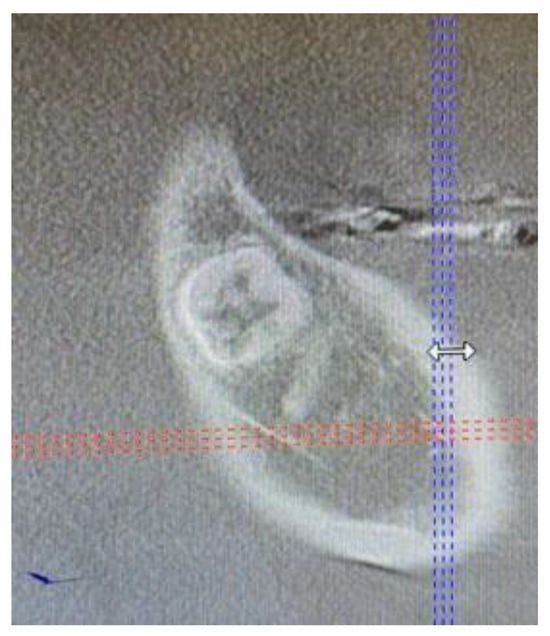
Figure 3.
Cone-beam computed tomography in the sagittal plane before biopsy. The superior part of the cortical bone remained clear and intact without any lesion or perforation.
The tumour was first subjected to an incisional biopsy to ensure a good histopathological specimen for the study, and then the condition of the MRT bone structures was established. Ten centimetres of Lignocain was administered as local anaesthesia with adrenaline (Lignocainum 2% c. noradrenalino Polfa 10 amp × 2 mL, Polfa, Warszawa, Poland). The following was administered: Taromentin (1.2 g–1 g amoksycylin, 200 mg clavulanic acid, Polfa Tarchomin, WarszawaIntravenously, Poland), 100 mg Ketonal (50 mg/mL, 10 amp. 2 m, Sandoz, Warsaw, Poland), and 1 g of paracetamol (Biofarm, Poznań, Poland). The oral cavity and adjacent skin were rinsed with Octanisept mouthwash. Sterile dressings were placed to cover the oral cavity. First, a buccal releasing incision was made via the unilateral sagittal-split of the mandible (USSO) approach at the right bucco-vestibular area of the mandible. The incision was made laterally from the mandibular ascending ramus, just buccally from the tumour, and then lowered to the bucco-alveolar free gingival area close to the teeth 45/46. Blade No. 15c B (Swann Morton, WR Swann, Owlerton Grn, Hillsborough, Sheffield, UK) was used. To safely elevate a mucoperiosteal flap, Obwegeser Periosteal Elevators (Obwegeser 38-630-06-07-38-630-11-07 17.5 cm/6 7/8”, KLS Martin, Tuttlingen, Germany) were used. One lingual spatula was used to protect the medial aspect of the tumour and the entrance to the oral part of the throat (TONGUE DEPRESSOR, DOYEN, 30/33 mm, 16 cm, KLS Martin, Tuttlingen, Germany), and one long Langenbeck hook (Langenbeck retractor, 55 × 11 mm, HR-2604-55x11, Hossa International, Warszawa, Poland) from the buccal side of the incision was used for retraction. After mobilisation of the entire flap, the buccal cortical bone was intact, and adjacent teeth 47 were situated in a stable position in the alveolar bone. After establishing good visibility of the operated field, because of the lack of local bone changes and the small diameter of the tumour, we decided to excise all of the tumour for adequate histopathological evaluation. To gently elevate the tumour, Mosquito clamps were used (Mosquito-Forceps, Crile, Cvd., 14.5 cm, KLS Martin, Tuttlingen, Germany). Later, with a 2 mm surgical margin of soft tissues, the tumour was excised. The cortical bone under the tumour was intact, without any lesions, bone osteolysis, or other visible signs of infiltration. To establish the detailed status of the cortical bone, a large part of the cortical bone was removed for further examination with the use of a bone chisel and bone hammer (Bone Chisel, 4 mm, 17 cm, KLS Martin, Tuttlingen, Germany). Because of the visibility of the atypical impacted mandibular right wisdom molar, with some clinical signs of bone ankylosis, an attempt was made to remove the teeth; however, due to the proximity of the inferior alveolar nerve (IAN)—including related bleeding—and the structure of the impacted teeth embedded with the bone, the procedure was not completed; a second approach after histopathological examination of the excised tumour was possible (Figure 4). The patient was sutured with 4.0 Prolene (Prolene Johnson & Johnson, London, UK), and additional Spongostan-collagen sponges (Spongostan, Ethicon, Ferrosan, London, UK) were applied to the area of the partially removed wisdom teeth. The patient was prescribed 100 mg of intraoral Ketonal 2/day (Sandoz, Warsaw, Poland), 1 g of Augmentin 2/day (Polfa Tar-chomin, Warszawa, Poland), and Multilac (Probiotic+Prebiotic, USP ZDROWIE SP. Z O.O., Warszawa, Poland) along with 0.1% CHX (chlorhexidine gluconate) (Eludril, Pierre-Fabre Oral Care, France) for two weeks postoperatively. An additional 0.32 mg of Neurovit was administered two times per day for fifty days in total (1 tabl. consists of 100 mg wit. B1, 200 mg wit. B6, 0.2 mg wit. B12; 100 tabl.; G.L. Pharma, Gerot-Lannah, Wien, Austria) in the presurgical period for nerve healing stimulation immediately after surgery. The healing period after the biopsy was uneventful. A slight portion of the lower right lip was numb because of IAN nerve involvement, and 48 teeth were not removed. No inflammation, abscess formation, or other bone inflammation occurred after the surgery (Figure 5).
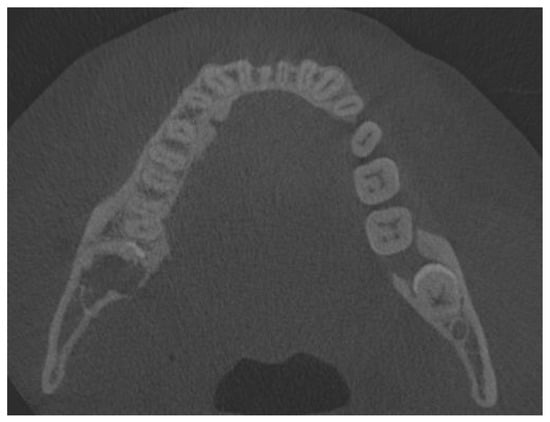
Figure 4.
Cone-beam computed tomography one month after biopsy. Half of the fully retained third molar is visible.

Figure 5.
Intraoral photographs one month after the surgery.
After approximately three weeks, histopathological examination revealed an oral cavity schwannoma (S100+; Ki67 = 5%; p63-) without clear margins after biopsy. The second specimen, which consisted of cortical bone, revealed healthy bone fragments.
Because of the lack of clear margins after the excisional biopsy and the presence of some of the retained wisdom teeth, a decision was made to radicalise the first procedure. The main focus was to maintain good soft tissue margins, and the remaining wisdom teeth were removed, followed by the use of an osteoalveoplasty procedure. Control CBCT and panx evaluation revealed that the bone and tooth status after the first procedure was good and that the patient had healed properly (Figure 4, Figure 5 and Figure 6).

Figure 6.
A routine panoramic (panx) radiograph one year after revision surgery and extended radical removal of the schwannoma. Kinking of the inferior alveolar nerve canal is visible along with the remnants of the impacted third molar crown.
The final procedure took place under general anaesthesia and nasotracheal intubation. First, 5 mm of tissue surrounding the previous scar tissue was removed via cerclage. Later, a similar USSO approach was used. The bone was visualised. With the use of surgical burrs and Lindeman burrs (Lindemann Burr, Ø 2.1 mm, 7 cm, Storz, KARL STORZ SE & Co. KG—Tuttlingen, Germany), parts of the bone were removed and sent for further examination. Because of the lack of necessity for the removal of tooth 47 and the risk of further damage to the IAN, the most visible and accessible part of the tooth was removed. The remaining bone parts, along with some of the crown in the bony ankylotic mass located near the lingual nerve, were left for clinical and radiological monitoring. After ensuring the safety of both nerves, we performed a local alveolar osteoplasty. The defect was filled with a collagen sponge and sutured with 4.0 sutures (a/s.). The post-surgical period consisted of the same local wound irrigation and intraoral care. The final histopathological result was free of any residual SC.
After one and two weeks, healing was uneventful. Because of the loss of sensation in the lower lip caused by inferior alveolar nerve damage (IAN), an additional course of 0.32 mg Neurovit was administered two times per day for fifty days in total (1 tabl. consisting of 100 mg wit. B1, 200 mg wit. B6, 0.2 mg wit. B12; 100 tabl.; G.L. Pharma, Gerot-Lannah, Wien, Austria). After the second dose of pharmacological treatment, the overall numbness of the lip decreased; however, full lip function was still not restored. After three years, some degree of lip numbness remained; however, there was no recurrence of the SC tumour. Because of the proximity of part of the ankylotic crown of the right wisdom molar, a part of the teeth remained in the bone and was symptomless both clinically and during routine radiological CBCT evaluation (Figure 7, Figure 8 and Figure 9). The scope of paraesthesia decreased slightly over the years, but the scope of missing function was not troublesome for the patient.

Figure 7.
Intraoral photograph after three years. No tumour reoccurrences were present. Some tissue was scarce and contracted in the mandibular retromolar trigone area.
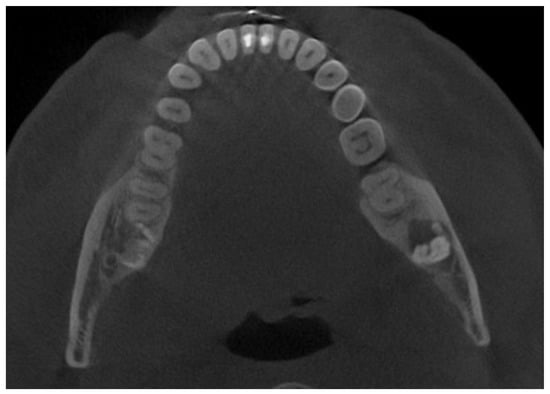
Figure 8.
Cone-beam computed tomography with visible remnants of a fully retained crown of the lower wisdom teeth. No osteolytic, cystic, or inflammatory changes are visible in the bone or adjacent structures. The inferior alveolar nerve is visible in close proximity to the dental crown remnants.
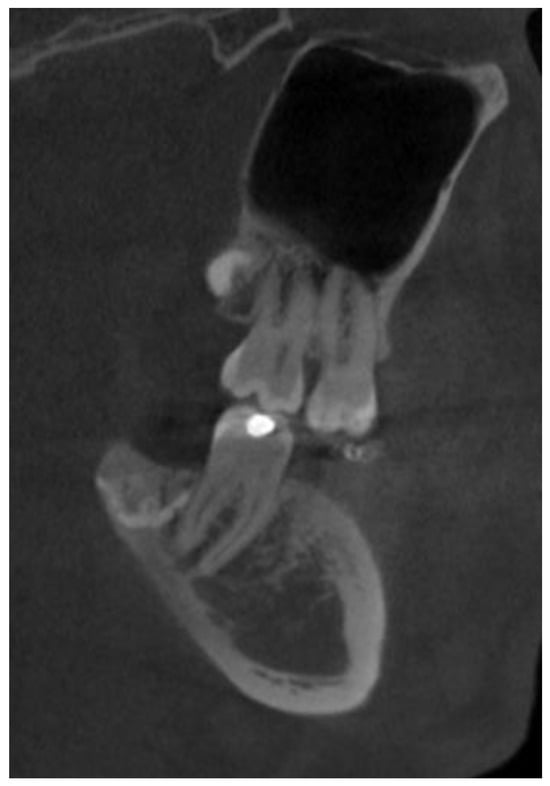
Figure 9.
Cone-beam computed tomography after three years in the sagittal plane showing good healing of the bone superiorly placed from the remnants of the molar crown. Adjacent second molars and adjacent bone without any radiological changes in their structure.
Despite the inability of the IAN to fully recover function, the final outcomes three years after surgery were satisfactory. Further clinical and radiological follow-up every 12 months is scheduled.
3. Discussion
Oral neural tumours (ONT/NOT) are rare in the oral cavity. Most commonly, they are related to the reactive or neoplastic proliferation of nerve sheath cells [18]. During clinical examination, their shape, appearance, and features can mimic any other cyst or tumour within the oral cavity. However, a detailed histopathological examination is the most accurate diagnostic tool to ensure a detailed diagnosis [19]. According to some authors, the most common ONTs are granular cell tumours, neurofibroma, schwannoma, traumatic neuroma, palisaded encapsulated neuroma, and nerve sheath myxoma [18,19,20]. They are found in less than 1% of oral lesions, while their aggressive malignant forms are quite uncommon, occurring in approximately 0.02% of oral lesions [18,19,20]. Nevertheless, their occurrence might lead to many diagnostic dilemmas and challenges. MRI can easily exclude any malignant pathologies, nerves, tissues, or surrounding tissue infiltration or establish if the mass has well-defined borders. In the presented case, the authors first suspected the rare occurrence of a pleomorphic adenoma and, second, an odontogenic-like peripheral ossifying fibroma consisting of mixed fibrous bone with an elastic appearance. MRI with contrast enhancement could improve the diagnosis because of clear visualisation of the margins, borders, and location in the tissues, and some papers confirm this [21]. The adjacency of the tumour to the mandibular body requires CBCT. Very few papers on such MRT locations of SCs are available. One of the studies reported a 70-year-old male with the same anatomical occurrence of this lesion; however, in this case, CBCT was also used because a tumour other than an SC was suspected [22]. On the other hand, when an atypical and rare retromolar tumour in soft tissues is suspected, MRI with contrast enhancement is more precise than any other diagnostic evaluation [23]. The cases by Jadwani and Rathore were some of the first to describe this rare intraoral MRT SC, and, so far, just a few similar cases are known in the world literature [22,23].
A schwannoma in the mandibular retromolar area is a very rare and atypical finding, especially when its position near the retained molar might suggest an odontogenic lesion (follicular cyst, eruption cyst, odontogenic keratocyst-OKC, and others), while the presence of small salivary and mucous glands in the following areas might suggest a salivary gland tumour (MEC-mucoepidermoid carcinoma, tumour mixtus (pleomorphic adenoma), ACC-adenoid cystic carcinoma, or others). CBCT evaluation of the following lesions should establish any intra/extraosseous spread and the status of cortical bone, which is important for differential diagnostic purposes. CBCT/MR can improve the value of any diagnostic imaging technique, while clinical examination remains equally important, especially for solid lesions, cystic lesions, tender lesions, movable lesions, ulcerations, or lesions with other possible features. It is worth noticing that some authors recommend a biopsy, and others an excisional biopsy, while some recommend improved diagnostics with MRI; however, only large ONTs with cortical bone infiltrations or erosions should be scheduled for more radical ostectomies, bone resection, or other procedures [5,6,7,8,9,10,11,12,13,14,15,20,21,22,23,24].
A detailed differential diagnosis should first be established if any lesion, cyst, or tumour in the oral cavity has odontogenic or nonodontogenic origins. CBCT is one of the most important diagnostic steps for evaluating bone and tooth structures in the oral cavity. To establish any odontogenic lesion, cone-beam computed tomography (CBCT) is the diagnostic tool of choice, followed by detailed tooth examination consisting of palpation, cold stimulation, periapical area evaluation, estimation of any tooth resorption, bone osteolysis, crepitation, tooth mobility, and other factors, such as nerve sensation or the Vincent sign. When odontogenic lesions are excluded, detailed diagnostics of any other nonodontogenic cysts and tumours need to be scheduled. First, any primary or secondary bone lesions, small salivary gland-like tumours, metastatic disease, or the occurrence of primary or secondary oral squamous cell carcinoma lesions (OSCCs or SCCs) should be excluded [20]. ONT is quite rare, but, when it is found, its occurrence can mimic any other lesion or tumour. Therefore, the oral cavity should be examined carefully to exclude the occurrence of any other similar lesions. Second, differentiating between SC and neurofibroma is very important since multiple similar tumours in the oral cavity can be used to identify neurofibromas and can indicate rare diseases, such as neurofibromatosis. The most important differential diagnoses related to ONT–salivary gland tumours include pleomorphic adenoma, adenoid cystic carcinoma, and salivary duct carcinoma [12,13,14,15,16,17,18,19,20]. In the present case, the consistency of the lesion, which mimicked a soft, elastic tumour with some hard features inside, mimicked that of a solid tumour, and its good attachment to the bone surface was a diagnostic indicator. In the case of a small lesion, an excisional biopsy is recommended, while larger lesions should be scheduled for a biopsy to determine their histopathological status. On the other hand, the condition of the surrounding bone might require curettage, peripheral ostectomy, or a combination of both, depending on the status of the bone. In the present case, the surgery was quite demanding and challenging because of the fully impacted wisdom teeth with some signs of ankylotic bone formation. If the teeth were not present, only slight bone cortical plate removal would have been scheduled to ensure bone margins.
Since ONT can mimic other possible tumours in the oral cavity, it is quite important to emphasise that ONT can appear in any part of the oral cavity [12,14,15,16]. Bhola et al. described a tongue tumour in a paediatric patient [24]. This finding in the paediatric population should also be differentiated from the ectopic thyroid gland or the Abrikosov tongue lesion [20,21,25]. Additionally, the floor of the mouth or gingiva, which are closely related to the teeth, can be places where SC occurs. When SC or any ONT might appear in the tooth area or tooth-bone-bearing structures, it is important to estimate the condition of the adjacent bone or teeth and the prognosis of the teeth.
In each case of SC/ONT, histopathological diagnosis is the most accurate tool for distinguishing this tumour from any other lesion. Since the occurrence, shape, and localisation in the oral cavity of the tumour and adjacent anatomical areas may be diagnostically challenging, histopathological examination is more sensitive and specific than CBCT or MRI. After the excision of each strange lesion from the oral cavity, ONT can be suspected. Because SC may be more or less elastic in clinical examination and can comprise some forms of fibrous structures and capsules, histopathological evaluation can identify two SC patterns, namely, more structured and more chaotic patterns. It is quite important to note that SCs exhibit some specific histopathological features, such as the expression of the S-100 protein, which is most characteristic of SC, similar to CD34. On the other hand, CD57+ cells are more common in traumatic neuromas. Another feature to be noted is the pattern of eosinophilic areas, whether an Antoni A-type (Verocay bodies) or a B-type (cha-otic pattern), as this helps to identify the type of SC [26,27,28]. The so-called Verocay bodies are named after palisaded nuclei that appear in the microscopic evaluation. This approach might also be helpful in identifying the type of ONT, whether SC or neurofibroma [26,27,28]. Finally, histopathological variants of SC include ancient schwannoma, pseudo glandular schwannoma, plexiform schwannoma, cellular schwannoma, epithelioid schwannoma, and melanotic schwannoma [22,23,24,25,26,27,28,29].
The total removal of each ONT should be included to decrease any potential recurrence. Sometimes this is surgically troublesome, especially if the SC infiltrates key nerves and anatomical structures. Such findings might lead to a conclusion on how extensive the surgical approaches should be. On the other hand, Cohen and Wang reported that tongue SCs are challenging, especially if tongue loss of function and morbidity can be troublesome for patients after surgery [29]. Other methods other than classic surgical excision could be used for small lesions in some vital structures.
The second most troublesome location in the oral cavity is the mouth floor. In the patient, a tumour arising from both the sublingual and submandibular glands was excluded. Proximity to the lingual nerve, tongue muscles, salivary glands, and ducts can be a cause of major challenges [28,29,30]. The occurrence of swelling, the atypical location of each SC, and sometimes some paraesthesia, can raise some diagnostic problems. On the other hand, multiple SCs could be associated with neurofibromatosis [30,31]. Very un-commonly, SC can grow into extremely large tumours, possibly causing serious life-threatening deformations and bleeding. A larger SC can mimic salivary gland tumours. In those cases, MRI imaging should always be performed to avoid any unnecessary treatment complications [29,30,31,32]. In the literature, only one hybrid ONT tumour type, namely, a neurofibroma-schwannoma tumour, was reported by Leite et al. [33]. Surgical removal is the treatment of choice for each patient; however, multiple SCs or even solitary SCs can be associated with some syndromic disorders; therefore, a detailed patient anamnesis is important [25,26,27,28,29,30,31,32,33]. Each site of the oral cavity might be associated with a schwannoma. Size, location, and occurrence are not associated with any pattern. A special type of SC is a rare variant named the ancient schwannoma. This type of SC is rare but is characterised by submucosal swelling with a greater female predilection [34]. On the other hand, a plexiform schwannoma arising from the maxillary alveolar ridge was reported by Bueno et al. In this case, the SC was removed and bone curettage was used for surgical radicalisation followed by local osteoplasty [35]. Currently, oral manifestations of SC at every age are rare and are considered difficult diagnostic challenges [36].
The subsequent case of extraosseous SC in the MRT might be challenging because of the close proximity of the retained wisdom teeth, the atypical occurrence of ONT, the lack of bone erosions, and the consistency of the tumour itself. The following key surgical points were concluded from this case of SC:
- Each time that histopathological evaluation determines the type of tumour, small lesions can be scheduled for an excisional biopsy to gather a helpful amount of material for study; the nature of larger lesions should be identified first, i.e., before planning surgery.
- CBCT can be used to identify any bone lesion and odontogenic-related cysts and tumours, while MRI should be used for identifying solid soft tissue tumours with local malignant potential.
- Surgical excision is the treatment of choice; however, its scope greatly depends on the key anatomical structures in direct proximity to the tumour, such as nerves, arteries, teeth, salivary ducts, tongue, or soft palate.
- When SC involves bone curettage, peripheral ostectomy or bone chiselling is sufficient to ensure clear surgical margins if the SC does not penetrate deep inside the bone area.
- Contrast-enhanced CT/MR should be used for more advanced lesions.
- The location of the lingual, inferior alveolar, and buccal nerves in the MRT should be spared if possible.
The limitations of this study include the small number of patients who were diagnosed with any other SC or ONT tumours in the oral cavity at any of the authors’ daily practices. Because of the limited number of cases of such neural tumours, the authors wanted to highlight the atypical manifestations of SC and the features that mimic those of other oral cavity tumours. Furthermore, other case limitations include the unusual location of the neural oral tumour, the necessity for secondary surgery, the need for such a radical surgical approach, the lack of improved diagnostic methods consisting of MRI/CT with contrast enhancement, the lack of microscopic specimen sample photographs, and the limited number of papers on SC occurrence in the retromolar mandible trigone area for comparison.
4. Conclusions
Neural oral tumours are very rare and can mimic other pathologies. The proximity of teeth might mimic any odontogenic-like features. CBCT is very important for estimating the condition of cortical bone and possible bone erosions, infiltration, or lesions caused by soft tissue tumours. A wide surgical biopsy or excisional biopsy is needed to gather adequate surgical specimens for histopathological evaluation. Adjacent teeth do not always need to be removed. The application of bone ostectomy or curettage in such cases is mostly case-related when bone involvement is present or when bone spread in cortical or medullary bone is visible. CBCT and MRI can easily help in establishing the type of tumour and planning the resection margins. The differential diagnosis should include atypical nonodontogenic tumours, such as pleomorphic adenoma and adenoid cystic carcinoma, as well as odontogenic tumours, such as odontogenic keratocysts and ossifying fibromas.
Author Contributions
Conceptualisation—K.N., M.J., K.Ż. and G.G.; methodology—K.N., S.B. and I.M.; software—M.J.; validation—K.N., E.P. and M.J.; formal analysis—K.N., M.J., S.B. and I.M.; investigation—K.N.; resources—M.J. and K.Ż.; data curation—M.J. and M.D.; writing and original draft preparation—K.N., E.P. and M.D.; writing and review/editing—E.P., S.B., G.G. and J.N.; visualisation—K.N.; supervision—M.J.; project administration—M.J., M.D. and E.P.; funding acquisition—M.J., M.D., G.G. and J.N. All authors have read and agreed to the published version of the manuscript.
Funding
This work was financed by a subsidy from Wroclaw Medical University, number SUBZ.B180.24.058.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Bioethics Committee (No. 4-BNR-2022).
Informed Consent Statement
Patient written consent for publication was obtained.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- Shah, S.P.; Mehta, D. Mandibular Retromolar Foramen and Canal—A Systematic Review and Meta-Analysis. Ann. Maxillofac. Surg. 2020, 10, 444–449. [Google Scholar] [CrossRef]
- Park, M.K.; Jung, W.; Bae, J.H.; Kwak, H.H. Anatomical and radiographic study of the mandibular retromolar canal. J. Dent. Sci. 2016, 11, 370–376. [Google Scholar] [CrossRef]
- Truong, M.K.; He, P.; Adeeb, N.; Oskouian, R.J.; Tubbs, R.S.; Iwanaga, J. Clinical Anatomy and Significance of the Retromolar Foramina and Their Canals: A Literature Review. Cureus 2017, 9, 1781. [Google Scholar] [CrossRef]
- Orchard, A.; Adatia, A.; Moore, R.; Prabhu, S. Management of inferior alveolar nerve and lingual nerve injuries in the UK—A cross-sectional study. Br. J. Oral Maxillofac. Surg. 2022, 60, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Panesar, K.; Susarla, S.M. Mandibular Fractures: Diagnosis and Management. Semin. Plast. Surg. 2021, 35, 238–249. [Google Scholar] [CrossRef]
- Ranganath, M.K.; Matmari, V.; Narayanaswamy, U.D.; Bavle, R.M. Mucoepidermoid carcinoma presenting as a retromolar mucocele. Ann. Maxillofac. Surg. 2011, 1, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Parhar, S.; Singh, H.P.; Nayyar, A.; Manchanda, A.S. Intra-oral schwannoma—A case report. J. Clin. Diagn. Res. 2014, 8, 264–265. [Google Scholar] [PubMed]
- Chrysomali, E.; Papanicolaou, S.I.; Dekker, N.P.; Regezi, J.A. Benign neural tumors of the oral cavity. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1997, 84, 381–390. [Google Scholar] [CrossRef]
- Lambade, P.N.; Palve, D.; Lambade, D. Schwannoma of the cheek: Clinical case and literature review. J. Maxillofac. Oral Surg. 2015, 14, 327–331. [Google Scholar] [CrossRef][Green Version]
- Llewelyn, J.; Sugar, A.W. Neurilemmoma of the mandible: Report of a case. Br. J. Oral Maxillofac. Surg. 1989, 127, 512–516. [Google Scholar] [CrossRef]
- Kumaravelu, R.; Sathyanarayanan, R.; Jude, N.J. An Uncommon and Rare Soft Tissue Tumor of the Cheek (Schwannoma): A Case Report. J. Sci. Dent. 2020, 10, 38–40. [Google Scholar]
- Sardinha, S.D.C.S.; Paza, A.O.; Vargas, P.A.; Moreira, R.W.F.; Moraes, M. Schwannoma of the oral cavity. Histological and immunohistochemical features. Braz. J. Oral Sci. 2015, 4, 806–809. [Google Scholar]
- Zhong, J.; Zhou, Z.; Hu, Y.; Zhao, T.; Yao, Y.; Zhong, L.; Zhu, D. Diagnosis and management of hypoglossal nerve-derived schwannoma in the floor of mouth: A case series. BMC Oral Health 2022, 22, 265. [Google Scholar] [CrossRef] [PubMed]
- Koopaie, M. Schwannoma of the Hard Palate in a Child: Case Report. J. Arch. Mil. Med. 2019, 7, 98076. [Google Scholar] [CrossRef]
- Lee, E.Y.; Kim, J.J.; Seok, H. Schwannoma of the tongue: A case report with review of literature. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 17. [Google Scholar] [CrossRef] [PubMed]
- Martins, M.D.; de Jesus Anunciato, L.; Fernandes, K.P.; Bussadori, S.K.; Taghloubi, S.A.; Martins, M.T. Intra-oral schwannoma: Case report and literature review. Indian J. Dent. Res. 2009, 20, 121–125. [Google Scholar] [CrossRef] [PubMed]
- The CARE Guidelines (for CAse REports) Were Developed. Available online: https://www.care-statement.org/checklist (accessed on 16 March 2023).
- Tamiolakis, P.; Chrysomali, E.; Sklavounou-Andrikopoulou, A.; Nikitakis, N.G. Oral neural tumors: Clinicopathologic analysis of 157 cases and review of the literature. J. Clin. Exp. Dent. 2019, 11, 721–731. [Google Scholar] [CrossRef] [PubMed]
- Mohindra, M.; Verma, S.; Kang, M.S.; Goel, B.; Kumar, A.P.; Manchanda, G.V. Analysis of Clinical, Radiographic, and Treatment Profile of 10 Cases of Neurogenic Tumors and Tumor-Like Lesions of the Oral and Maxillofacial Region: An Observational Study. J. Pharm. Bioallied Sci. 2021, 13, 68–71. [Google Scholar] [CrossRef] [PubMed]
- Demir, U.L.; Öztürk, Y.H. Treatment Outcomes for Primary Retromolar Trigone Carcinoma: A Single Institution Experience. Turk. Arch. Otorhinolaryngol. 2020, 58, 87–92. [Google Scholar] [CrossRef]
- Swain, S.K.; Agrawala, R. Opis przypadku Intraoral schwannoma in a seven-year-old boy—A case report. Pediatr. Pol. 2020, 95, 52–55. [Google Scholar] [CrossRef]
- Rathore, A.S.; Srivastava, D.; Narwal, N.; Shetty, D.C. Neurilemmoma of Retromolar Region in the Oral Cavity. Case Rep. Dent. 2015, 2015, 320830. [Google Scholar] [CrossRef] [PubMed]
- Jadwani, S.; Bansod, S.; Mishra, B. Intraoral schwannoma in retromolar region. J. Maxillofac. Oral Surg. 2012, 11, 491–494. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bhola, N.; Jadhav, A.; Borle, R.; Khemka, G.; Bhutekar, U.; Kumar, S. Schwannoma of the tongue in a paediatric patient: A case report and 20-year review. Case Rep. Dent. 2014, 2014, 780762. [Google Scholar] [CrossRef] [PubMed]
- Bajpai, M.; Pardhe, N.; Kumar, M. Ancient Schwannoma of oral cavity in a pediatric patient. J. Pak. Assoc. Dermatol. Internet 2018, 27, 290–292. [Google Scholar]
- Bajpai, M.; Pardhe, N. Ancient schwannoma of gingiva—A rare case report. J. Indian Soc. Periodontol. 2017, 21, 234–236. [Google Scholar] [CrossRef]
- Fanburg-Smith, J.C.; Majidi, M.; Miettinen, M. Keratin expression in schwannoma; a study of 115 retroperitoneal and 22 peripheral schwannomas. Mod. Pathol. 2006, 19, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Thompson, L.D.R.; Koh, S.S.; Lau, S.K. Tongue Schwannoma: A Clinicopathologic Study of 19 Cases. Head Neck Pathol. 2020, 14, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.; Wang, M.B. Schwannoma of the tongue: Two case reports and review of the literature. Eur. Arch. Otorhinolaryngol. 2009, 266, 1823–1829. [Google Scholar] [CrossRef]
- Farooqui, A.; Khalekar, Y.; Farooqui, J.; Kasat, V. Schwannoma of floor of mouth: A case report. J. Indian Acad. Oral Med. Radiol. 2017, 29, 135–137. [Google Scholar]
- Santos, P.P.; Freitas, V.S.; Pinto, L.P.; Freitas, R.A.; de Souza, L.B. Clinicopathologic analysis of 7 cases of oral schwannoma and review of the literature. Ann. Diagn. Pathol. 2010, 14, 235–239. [Google Scholar] [CrossRef]
- Nassehi, Y.; Rashid, A.; Pitiyage, G.; Jayaram, R. Floor of mouth schwannoma mimicking a salivary gland neoplasm: A report of the case and review of the literature. BMJ Case Rep. 2021, 14, 239452. [Google Scholar] [CrossRef]
- Leite, A.A.; Mariz, B.A.L.A.; Oliveira, L.A.; Assunção, J.N.R., Jr.; de Almeida, O.P.; Vargas, P.A. Hybrid Neurofibroma/Schwannoma of the Oral Cavity: A Rare Case Report and Literature Review. Int. J. Surg. Pathol. 2022, 31, 695–701. [Google Scholar] [CrossRef]
- Piyush, P.; Mohanty, S.; Ghosh, S.; Gupta, S. A Rare Report of Two Cases: Ancient Schwannoma of Infratemporal Fossa and Verocay Schwannoma of Buccal Mucosa. Ann. Maxillofac. Surg. 2017, 7, 140–142. [Google Scholar] [CrossRef]
- Bueno, M.V.; Coelho Duarte, A.C.; Sinhorini, P.A.; Inácio de Carvalho, T.M.; Machado, G.G.; Ceccheti, M.M.; Zambon, C.E. Plexiform schwannoma in the maxillary alveolar ridge: A case report. J. Oral Diag. 2021, 06, 20210010. [Google Scholar] [CrossRef]
- Ahmed, S.; Al Dayel, O.; Tabassum, N.; Al Qanabr, M.H.; Ali, H.A.; Mathekor, N.; Albannawi, G.A.; Al Taqi, F.Z.; Al Shehri, A.H.; Shaker, S.M. Lingual schwannoma in an adolescent girl—A diagnostic challenge. J. Fam. Med. Prim. Care 2020, 9, 1775–1777. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).