
Effect of Photobiomodulation Therapy Dosage on Orthodontic Movement, Temporomandibular Dysfunction and Third Molar Surgery Outcomes: A Five-Year Systematic Review

 , , ,
, , , 

Abstract
1. Introduction
- Temporomandibular joint dysfunction syndrome (TMJDS) may encompass a mixed and often complex aetiology, but common symptoms generally arise through muscle pain and spasms together with degrees of trismus; this may be representative of both an acute as well as a chronic inflammatory condition.
- The surgical removal of mandibular third molars, for whatever reason, may involve the incision and raising of a full muco-gingival flap and bone removal to assist in the location and delivery of the tooth. Such surgical intervention will provoke an acute inflammatory reaction, notably through observed post-operative swelling, trismus and pain.
- Orthodontic treatment—embracing appliance-based tooth movement and/or tooth arch expansion—offers an opportunity for otherwise stable and healthy supporting tissue to be reorganised to allow the passage of teeth to a new prescribed location in the dental arch. Inasmuch, there may be induced low-stress inflammation associated with such a therapy, and some levels of pain and discomfort are often experienced. In essence, however, the contribution of PBM therapy is claimed to accentuate the osseous and dental supportive soft tissue cellular activity and to promote reductions in pain episodes and the overall active treatment time.
- Does PBM positively affect and augment the successful outcome of treatment, commensurate with a statistically significant comparison when compared to a control?
- Where inconsistency exists between the three groups, is the outcome of PBM therapy predictability affected according to the underlying status of the treatment area in terms of inflammation or pathology?
- Where inconsistency exists between the groups, is the effectiveness of PBM affected by disparity in light-dose, irradiation spot size or other laser operating parameters?
2. Materials and Methods
2.1. Protocol and Registration
- (i)
- P (Participant): adult patients who received active clinical treatment, associated with one of the three groups of therapy.
- (ii)
- I (Intervention): laser-activated in-office adjunctive PBM therapy.
- (iii)
- C (Control): dental treatment undertaken to address the presenting clinical need, but without adjunctive PBM therapy.
- (iv)
- O (Outcome): clinical assessment of improved outcome and reduction in negative symptoms.
- (v)
- S (Study Type): Randomised clinical trial peer-reviewed published studies.
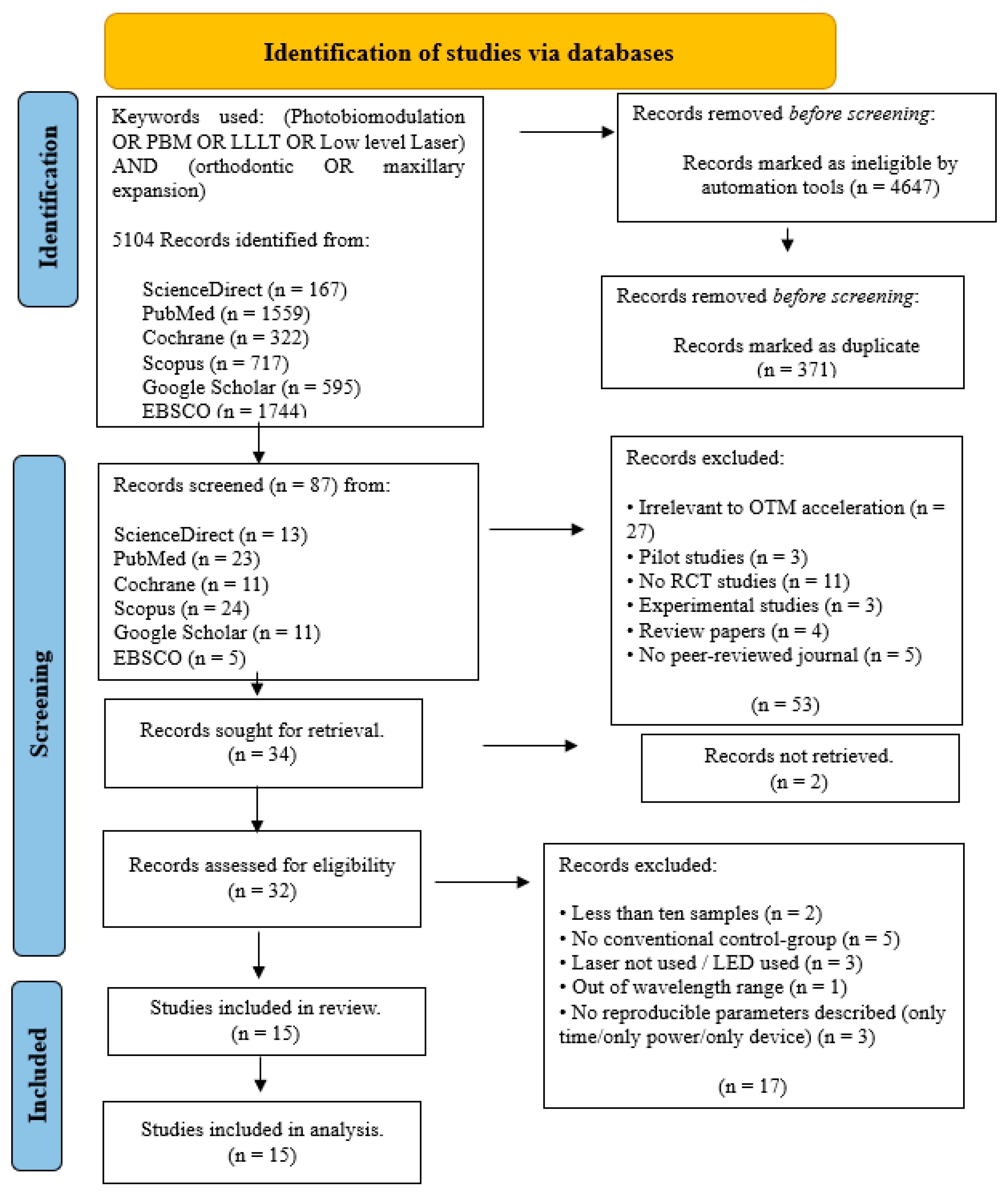
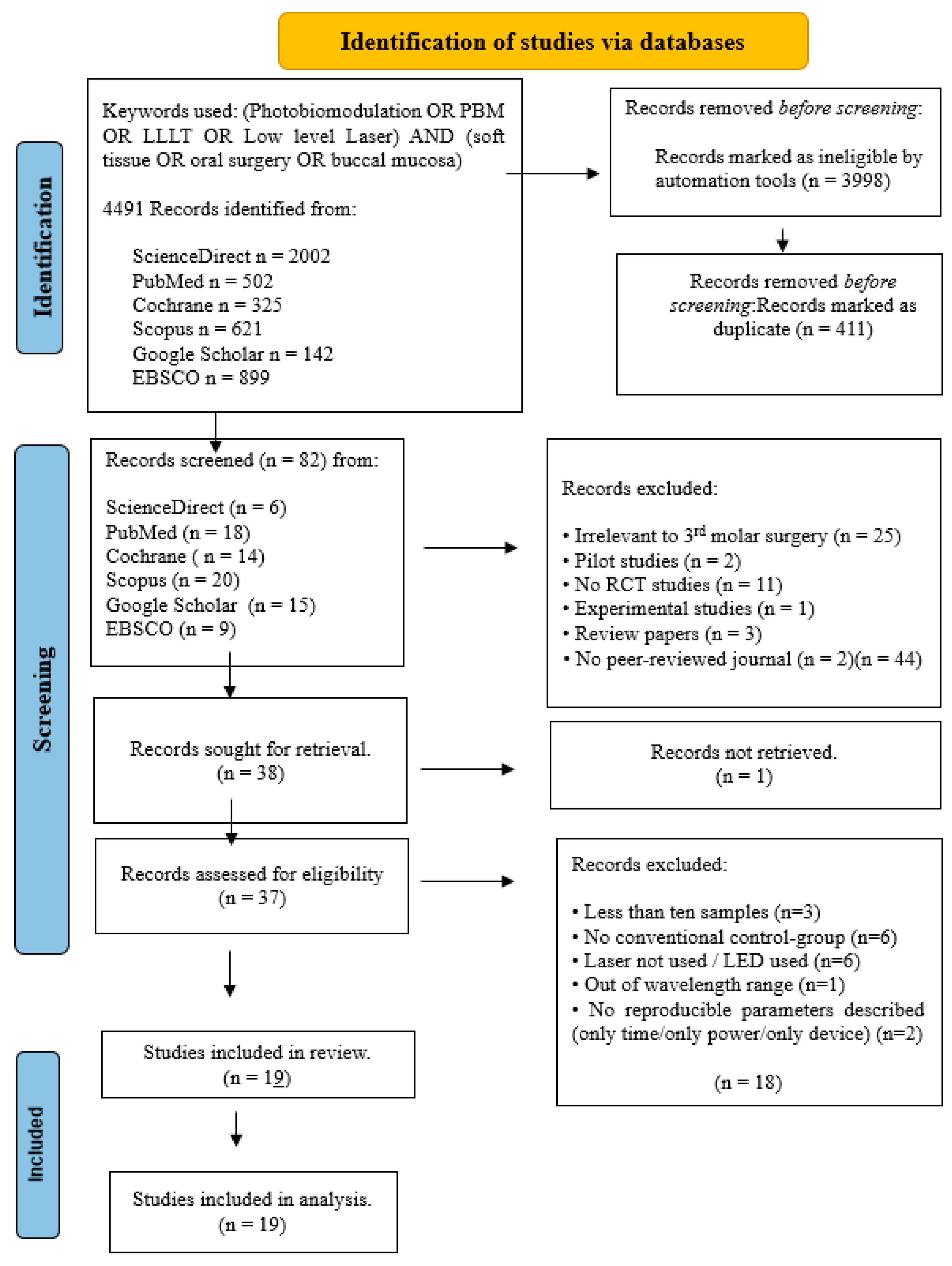
2.2. Search Strategy
- Randomised clinical trials;
- Laser PBM therapy associated with wavelengths in the range of 445–1064 nm;
- Articles were written in the English language;
- Control group and appropriate conventional non-PBM therapy;
- A minimum of 10 patients/samples per group;
- An adequate and appropriate protocol description.
- Laser wavelength outside the range 445–1064 nm;
- Case studies;
- Narrative review papers;
- Languages other than English;
- Pilot studies and/or case series;
- Experimental studies;
- Animal studies;
- Conference presentation papers or book chapters;
- Editorial articles or opinions;
- Short notes or comments in erratum;
- Press articles in the press;
- Non-retrievable studies.
2.3. Data Extraction
- Origin;
- Patient numbers represented in control and test groups;
- Use of randomisation and blinding;
- Laser wavelength applied;
- Laser operation parameters;
- Fluence (as calculated);
- Outcome (statistical significance).
2.4. Quality Assessment
- Randomization employed;
- Existence of sample size calculation and required sample number included;
- Blinding employed;
- Baseline situation similar for all groups;
- Laser operating parameters appropriately described, and any associated calculations correct;
- Optimal fluence applied;
- Power meter used to calibrate the laser used;
- Statistical analysis able to be applied to numerical results;
- Outcome data complete;
- Correct interpretation of data and results.
- High risk: 0–4;
- Moderate risk: 5–7;
- Low risk: 8–10.
3. Results
3.1. Oral Surgery
3.1.1. Primary Outcomes
3.1.2. Data Presentation
3.1.3. Quality Assessment
- Low risk of bias in 6/19 of the articles (31.6%):
- Moderate risk of bias in 13/19 of the articles (68.4%):
- High risk of bias in none of the studies.
3.1.4. Data Analysis
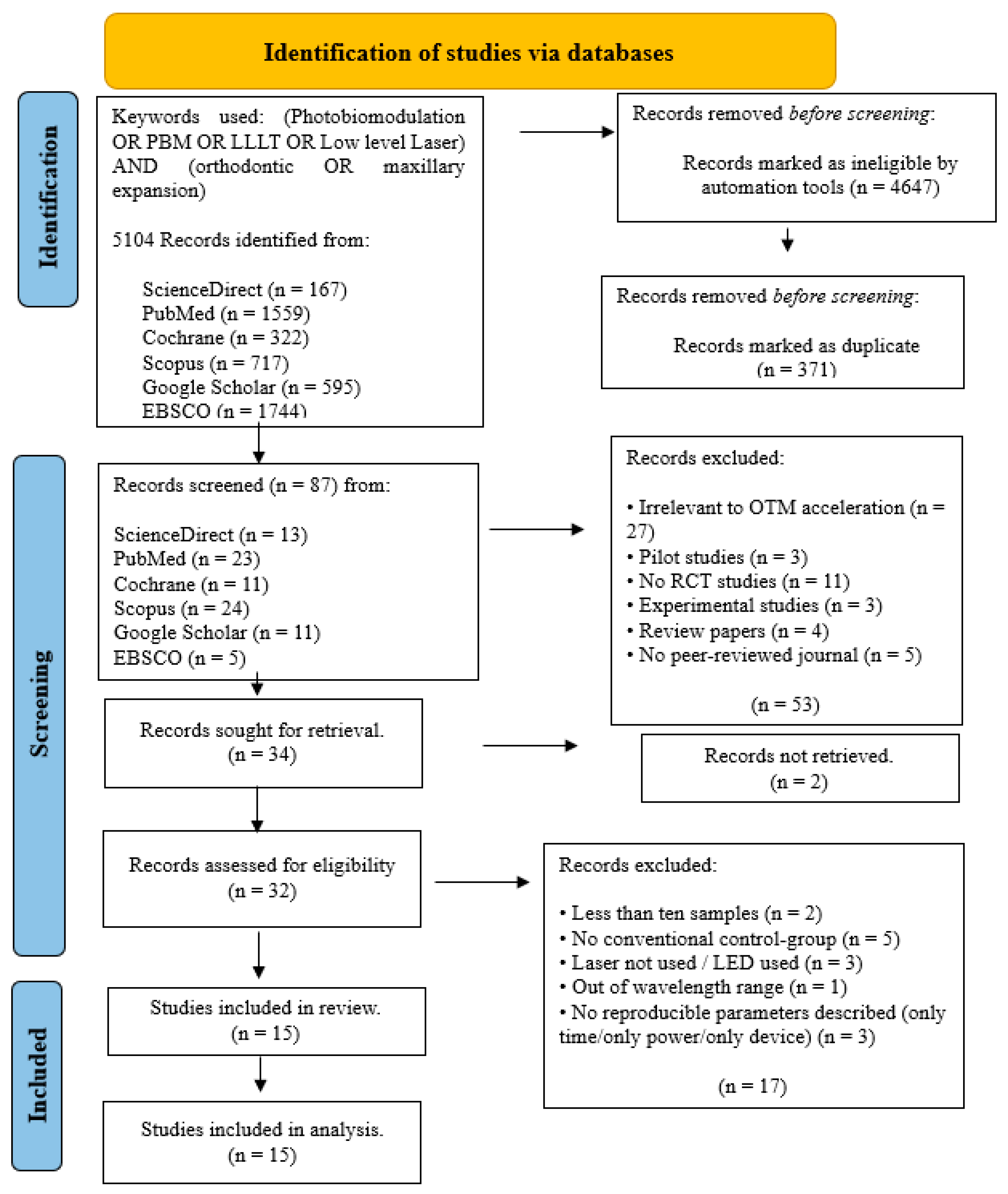
3.2. Orthodontic Movement
3.2.1. Primary Outcomes
3.2.2. Data Presentation
3.2.3. Quality Assessment
- Low risk of bias in 7/15 of the articles (46.7%):
- Moderate risk of bias in 8/15 of the articles (53.3%):
- High risk of bias in none of the studies.
3.2.4. Data Analysis
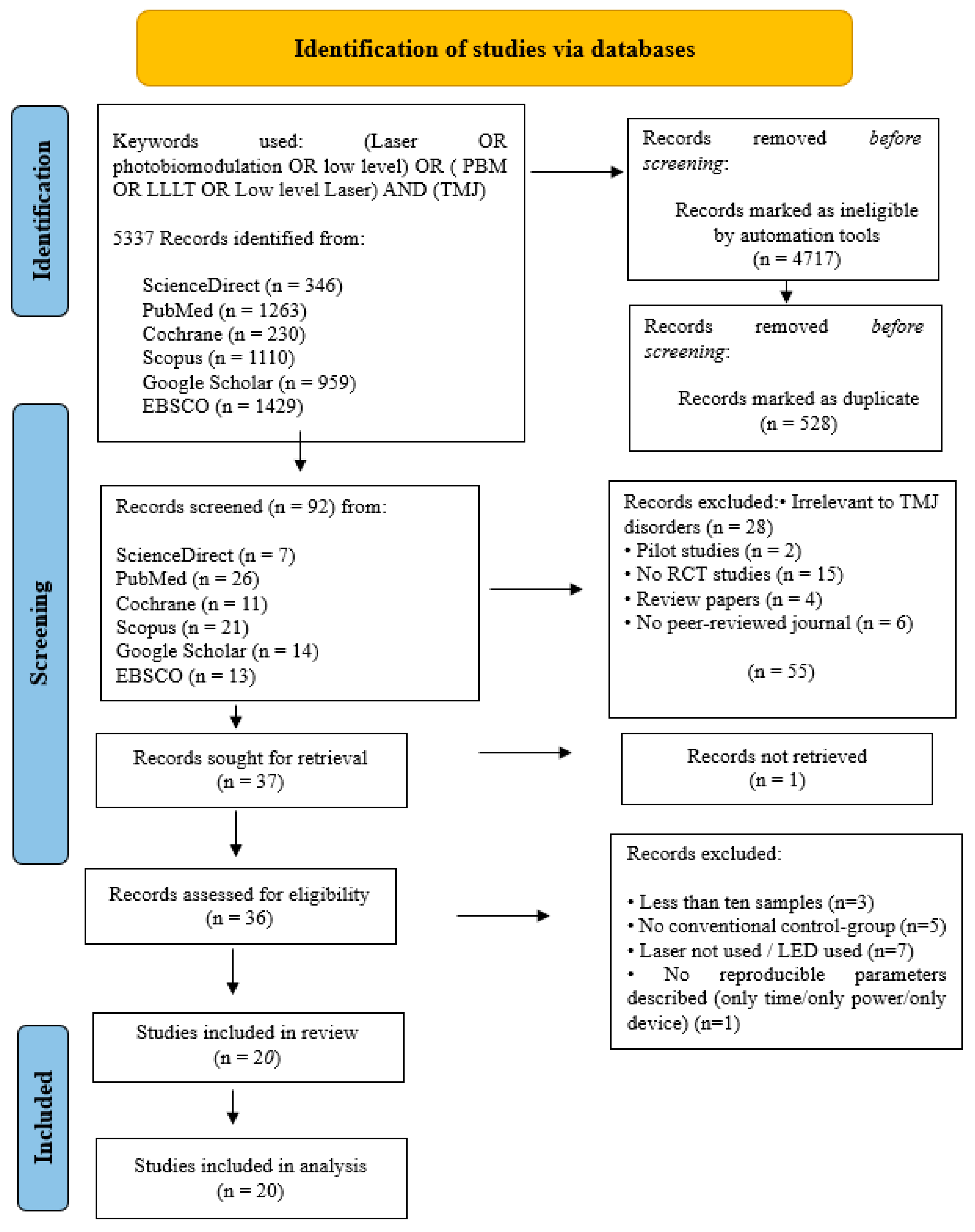
3.3. TMJ Studies
3.3.1. Primary Outcomes
3.3.2. Data Presentation
3.3.3. Quality Assessment
- Low risk of bias in 10/20 of the articles (50%):
- Moderate risk of bias in 10/20 of the articles (50%):
- High risk of bias in none of the studies.
3.3.4. Data Analysis
4. Statistical Analysis
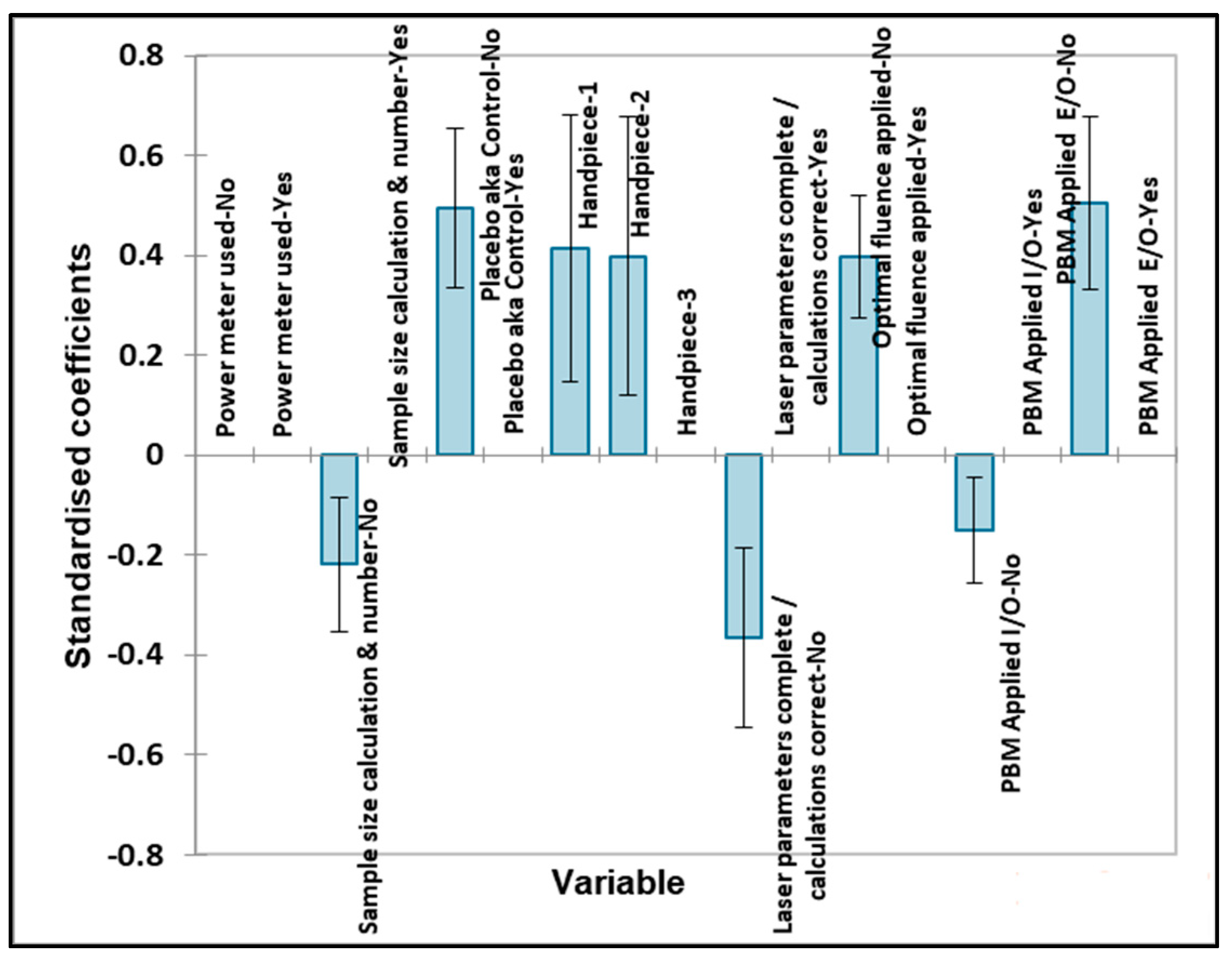
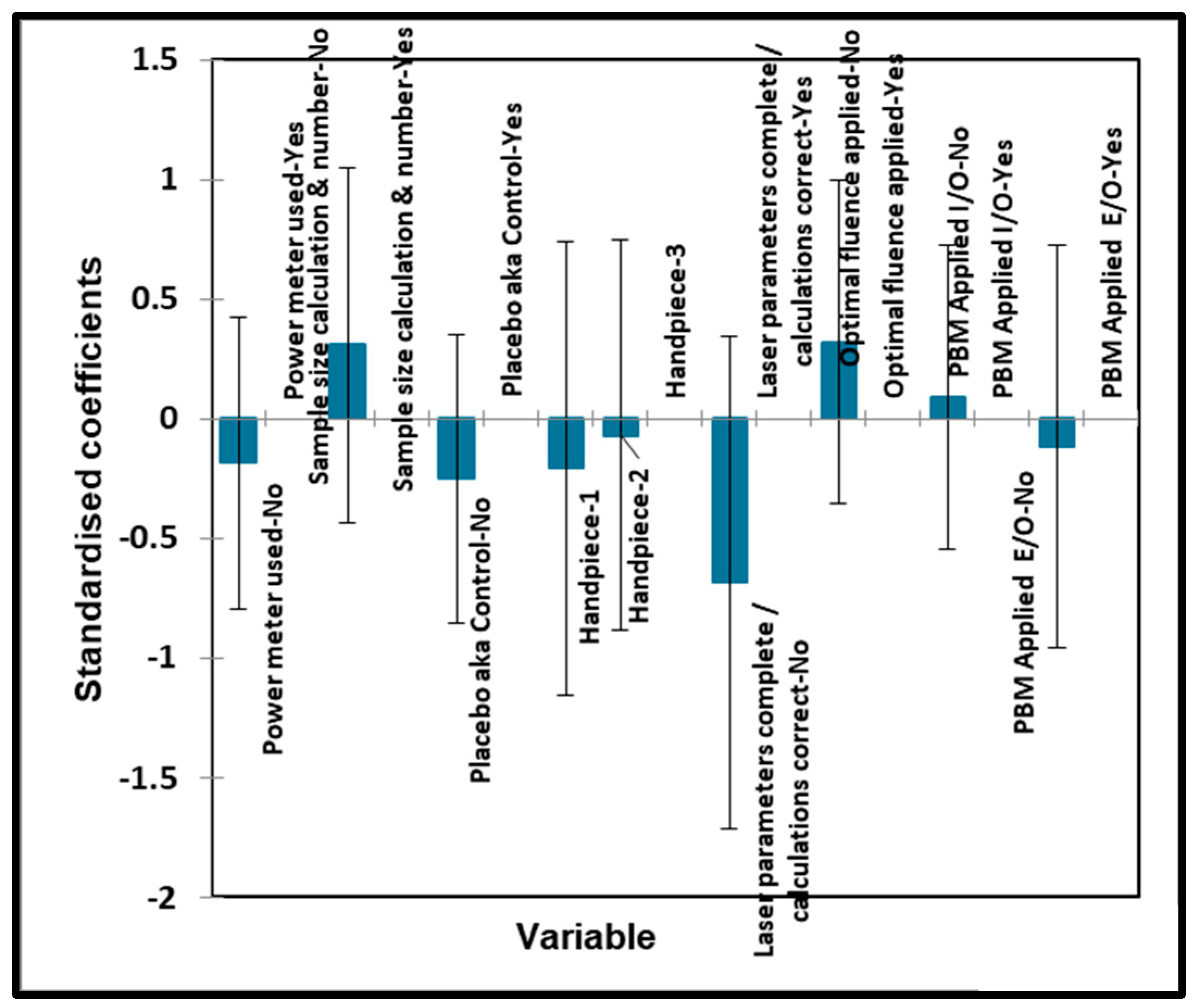
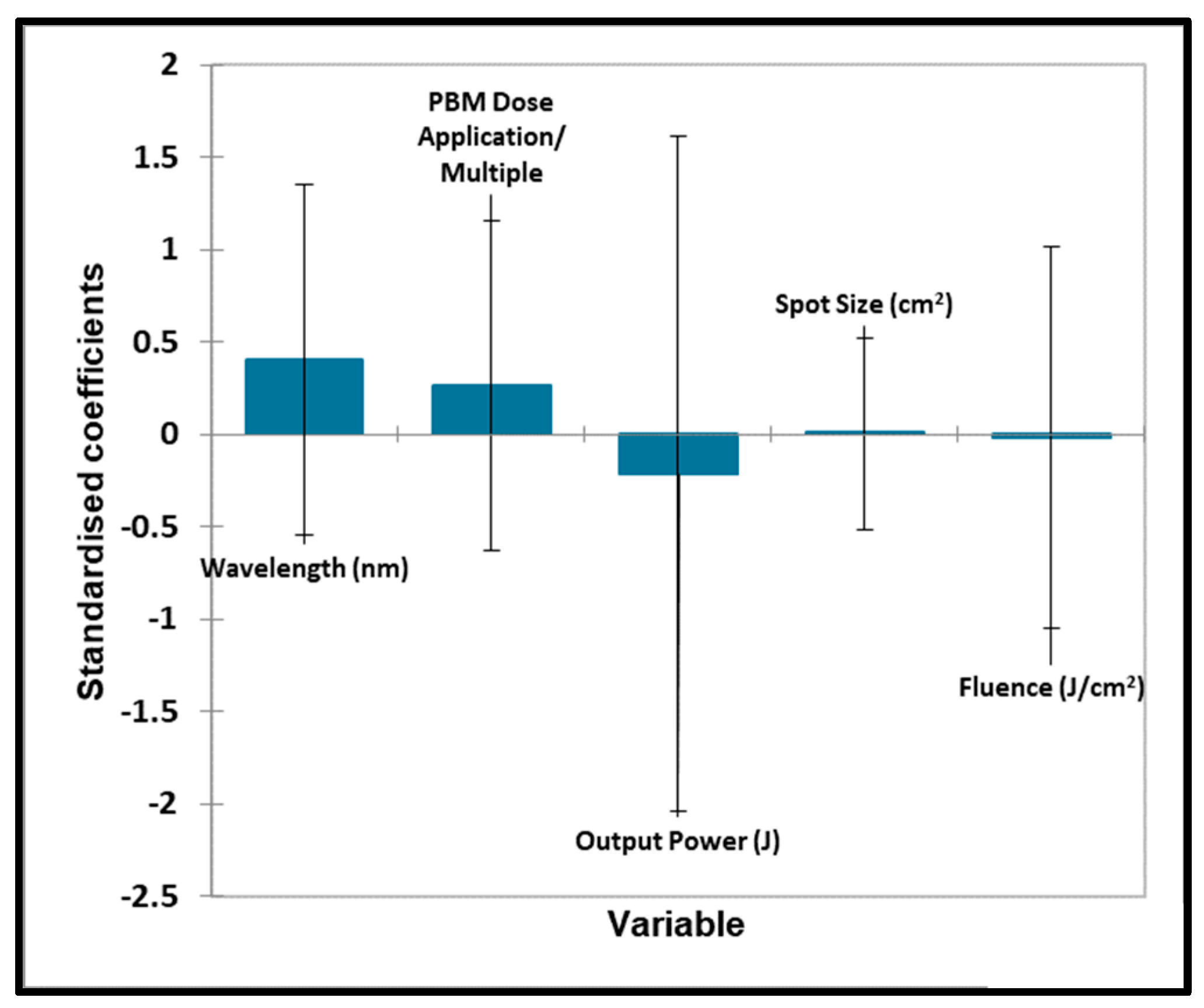
4.1. Oral Surgery
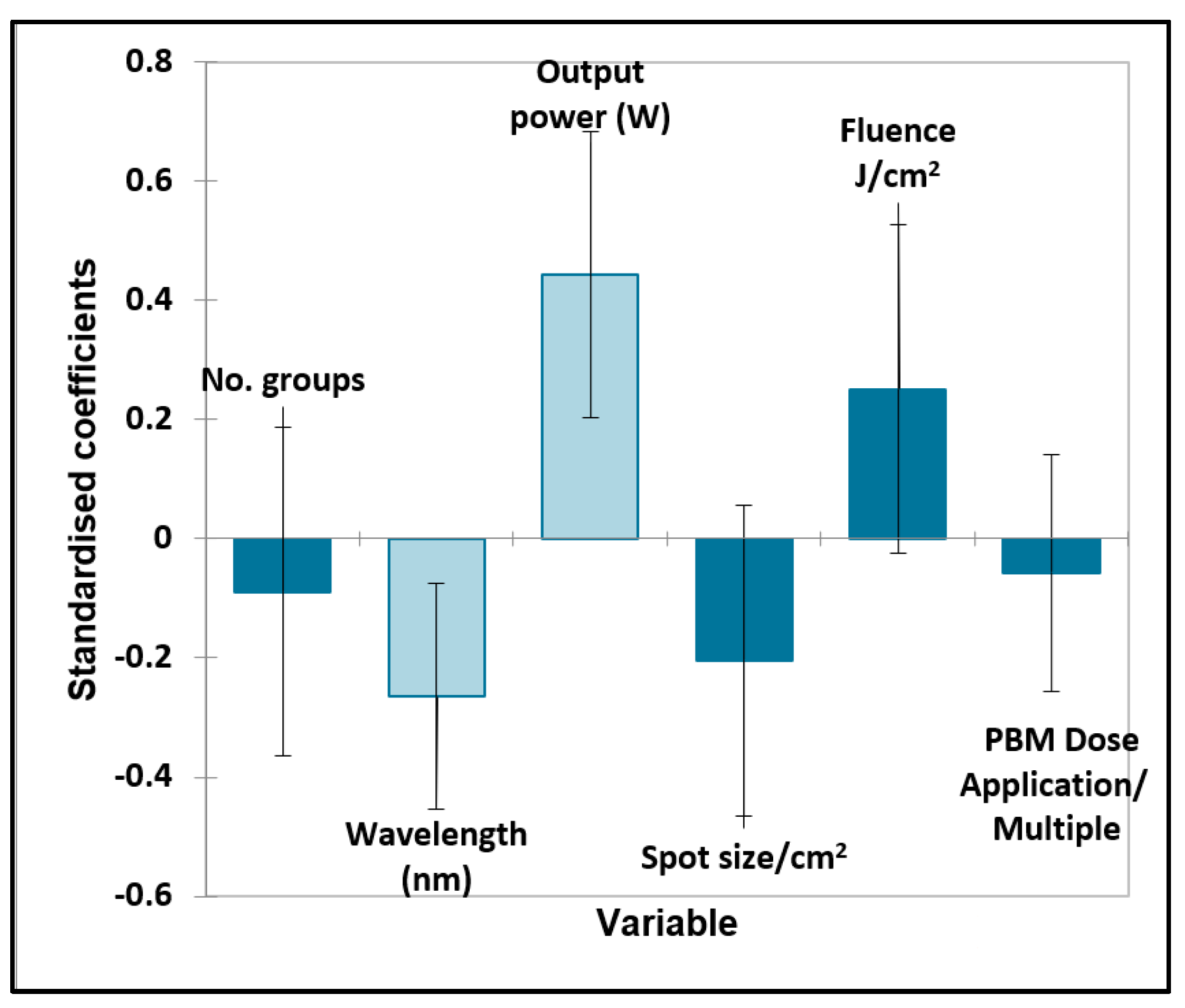
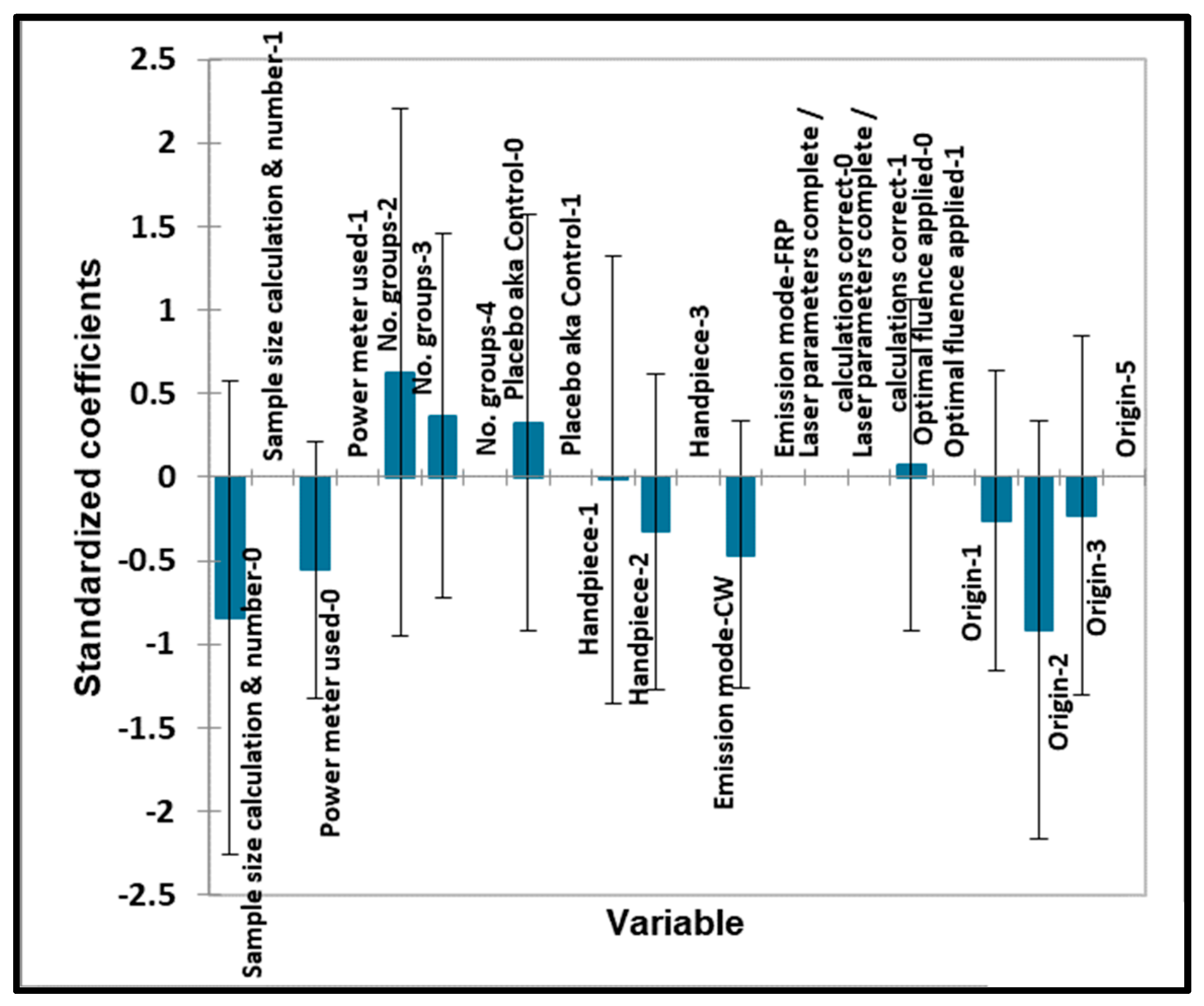
4.2. Orthodontic Tooth Movement
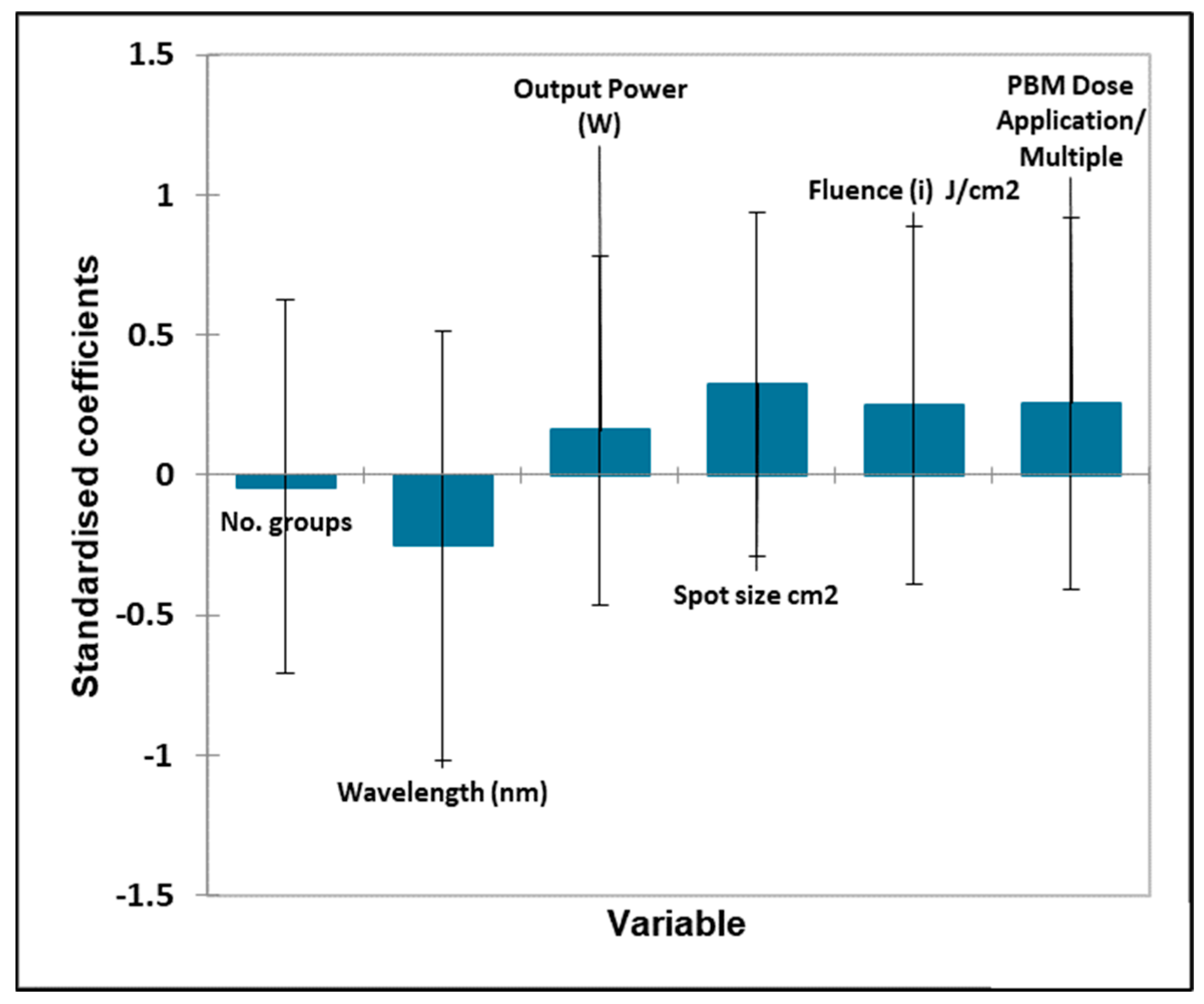
4.3. TMJ
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cronshaw, M.; Mylona, V. Ch. 7. Photobiomodulation Therapy Within Clinical Dentistry: Theoretical and Applied Concepts. In Lasers in Dentistry—Current Concepts, 2nd ed.; Coluzzi, D., Parker, S., Eds.; Springer Nature: Cham, Switzerland, 2024; p. 175. ISBN 978-3-031-43337-5. [Google Scholar]
- Hamblin, M.R.; Hamblin, M.R. Mechanisms and Applications of the Anti-inflammatory Effects of Photobiomodulation. AIMS Biophys. 2017, 4, 337–361. [Google Scholar] [CrossRef] [PubMed]
- Karu, T. Primary and Secondary Mechanisms of Action of Visible to Near-ir Radiation on Cells. J. Photochem. Photobiol. B 1999, 49, 1–17. [Google Scholar] [CrossRef]
- Chung, H.; Dai, T.; Sharma, S.K.; Huang, Y.-Y.; Huang, Y.-Y.; Carroll, J.D.; Hamblin, M.R.; Hamblin, M.R. The Nuts and Bolts of Low-level Laser (light) Therapy. Ann. Biomed. Eng. 2012, 40, 516–533. [Google Scholar] [CrossRef] [PubMed]
- Fekrazad, R.; Fekrazad, R.; Arany, P.R. Photobiomodulation Therapy in Clinical Dentistry. Photobiomodul. Photomed. Laser Surg. 2019, 37, 737–738. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, E.J.; Dhawan, G.; Kapoor, R.; Agathokleous, E.; Calabrese, V. Hormesis: Wound Healing and Fibroblasts. Pharmacol. Res. 2022, 184, 106449. [Google Scholar] [CrossRef] [PubMed]
- Csaba, G. Hormesis and Immunity: A Review. Acta Microbiol. Immunol. Hung. 2018, 66, 155–168. [Google Scholar] [CrossRef] [PubMed]
- Sarian, M.; Zulkefli, N.; Che Zain, M.; Maniam, S.; Fakurazi, S. A review with updated perspectives on in vitro and in vivo wound healing models. Turk. J. Biol. 2023, 47, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; DiPietro, L.A. Factors Affecting Wound Healing. J. Dent. Res. 2010, 89, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.; Cronshaw, M.; Grootveld, M. Photobiomodulation Delivery Parameters in Dentistry: An Evidence-based Approach. Photobiomodul. Photomed. Laser Surg. 2022, 40, 42–50. [Google Scholar] [CrossRef]
- Hamblin, M.; Ferraresi, C.; Huang, Y.; Freitas, L.; Carroll, J. Chapter 1: Photobiomodulation. In Low-Level Light Therapy, 1st ed.; SPIE Press: Bellingham, WA, USA, 2018; p. 1. [Google Scholar]
- Kuffler, D.P. Photobiomodulation in Promoting Wound Healing: A Review. Regen. Med. 2016, 11, 107–122. [Google Scholar] [CrossRef]
- Cronshaw, M.; Parker, S.; Arany, P.R. Feeling the Heat: Evolutionary and Microbial Basis for the Analgesic Mechanisms of Photobiomodulation Therapy. Photobiomodul. Photomed. Laser Surg. 2019, 37, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zhang, Y.-H.P.J. Enzymatic Regeneration and Conservation of ATP: Challenges and Opportunities. Crit. Rev. Biotechnol. 2021, 41, 16–33. [Google Scholar] [CrossRef] [PubMed]
- Pappas, G.; Wilkinson, M.L.; Gow, A.J. Nitric Oxide Regulation of Cellular Metabolism: Adaptive Tuning of Cellular Energy. Nitric Oxide 2022, 131, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.-S.; Calderhead, R.G. Is Light-emitting Diode Phototherapy ((LED-LLLT) Really Effective? Laser Ther. 2011, 20, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Cronshaw, M.; Cronshaw, M.; Parker, S.; Anagnostaki, E.; Mylona, V.; Lynch, E.; Grootveld, M. Photobiomodulation Dose Parameters in Dentistry: A Systematic Review and Meta-analysis. Dent. J. 2020, 8, 114. [Google Scholar] [CrossRef] [PubMed]
- Dompe, C.; Dompe, C.; Moncrieff, L.; Moncrieff, L.; Matys, J.; Grzech-Leśniak, K.; Grzech-Leśniak, K.; Kocherova, I.; Bryja, A.; Bruska, M. Photobiomodulation-underlying Mechanism and Clinical Applications. J. Clin. Med. 2020, 9, 1724. [Google Scholar] [CrossRef] [PubMed]
- Theodoro, L.H.; Marcantonio, R.A.C.; Wainwright, M.; Garcia, V.G. LASER in Periodontal Treatment: Is It an Effective Treatment or Science Fiction? Braz. Oral Res. 2021, 35, e099. [Google Scholar] [CrossRef]
- Kauark-Fontes, E.; Migliorati, C.A.; Epstein, J.B.; Bensadoun, R.-J.; Gueiros, L.A.M.; Carroll, J.; Ramalho, L.M.P.; Santos-Silva, A.R. Twenty-year Analysis of Photobiomodulation Clinical Studies for Oral Mucositis: A Scoping Review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2022, 135, 626–641. [Google Scholar] [CrossRef] [PubMed]
- Fornaini, C.; Fornaini, C.; Arany, P.R.; Rocca, J.-P.; Merigo, E. Photobiomodulation in Pediatric Dentistry: A Current State-of-the-art. Photobiomodul. Photomed. Laser Surg. 2019, 37, 798–813. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Eriksen, M.B.; Frandsen, T.F. The impact of PICO as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A.C. Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019; pp. 205–228. [Google Scholar] [CrossRef]
- De Oliveira, R.; da Silva, C.; de Paula, J.; de Oliveira, K.; de Siqueira, S.; de Freitas, P. Effectiveness of Laser Therapy and Laser Acupuncture on Treating Paraesthesia After Extraction of Lower Third Molars. Photobiomodul. Photomed. Laser Surg. 2021, 39, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Meyfarth, S.; Silva Fraga, R.; Da Costa Fontes, K.B.F.; Guimarães, L.S.; Alves Antunes, L.A.; Antunes, L.S. Do Antimicrobial Photodynamic Therapy and Low-level Laser Therapy Influence Oral Health-related Quality of Life After Molar Extraction? J. Oral Maxillofac. Surg. 2023, 8, 1033–1041. [Google Scholar] [CrossRef]
- Momeni, E.; Barati, H.; Arbabi, M.R.; Jalali, B.; Moosavi, M.-S. Low-level Laser Therapy Using Laser Diode 940 Nm in the Mandibular Impacted Third Molar Surgery: Double-blind Randomized Clinical Trial. BMC Oral Health 2021, 21, 77. [Google Scholar] [CrossRef] [PubMed]
- Isolan, C.P.; de Kinalski, M.A.; de Leão, O.A.A.; Post, L.K.; Isolan, T.M.P.; dos Santos, M.B.F. Photobiomodulation Therapy Reduces Postoperative Pain After Third Molar Extractions: A Randomized Clinical Trial. Med. Oral Patol. Oral Cir. Bucal. 2020, 26, e341–e348. [Google Scholar] [CrossRef] [PubMed]
- Asutay, F.; Ozcan-Kucuk, A.; Alan, H.; Koparal, M. Three-dimensional Evaluation of the Effect of Low-level Laser Therapy on Facial Swelling After Lower Third Molar Surgery: A Randomized, Placebo-controlled Study. Niger. J. Clin. Pract. 2018, 21, 1107–1113. [Google Scholar] [CrossRef] [PubMed]
- de Bianchi Moraes, M.; de Gomes Oliveira, R.; Raldi, F.V.; Nascimento, R.D.; Santamaria, M.P.; Loureiro Sato, F.R. Does the Low-intensity Laser Protocol Affect Tissue Healing After Third Molar Removal? J. Oral Maxillofac. Surg. 2020, 78, 1920.e1–1920.e9. [Google Scholar] [CrossRef] [PubMed]
- Mohajerani, H.; Tabeie, F.; Alirezaei, A.; Keyvani, G.; Bemanali, M. Does Combined Low-level Laser and Light-emitting Diode Light Irradiation Reduce Pain, Swelling, and Trismus After Surgical Extraction of Mandibular Third Molars? A Randomized Double-blinded Crossover Study. J. Oral Maxillofac. Surg. 2021, 79, 1621–1628. [Google Scholar] [CrossRef]
- Nunes, C.; Andrade, K.; Martins, C.; Chaves, F.; Oliveira, D.; Sampieri, M. Effectiveness of low power laser in reducing postoperative signs and symptoms after third molar surgery: A triple-blind clinical trial. Braz. Dent. J. 2023, 34, 158–168. [Google Scholar] [CrossRef]
- Feslihan, E.; Eroglu, C.N. Can Photobiomodulation Therapy Be an Alternative to Methylprednisolone in Reducing Pain, Swelling, and Trismus After Removal of Impacted Third Molars? Photobiomodul. Photomed. Laser Surg. 2019, 37, 700–705. [Google Scholar] [CrossRef]
- Nejat, A.; Eshghpour, M.; Danaeifar, N.; Abrishami, M.; Vahdatinia, F.; Fekrazad, R.; Fekrazad, R. Effect of Photobiomodulation on the Incidence of Alveolar Osteitis and Postoperative Pain Following Mandibular Third Molar Surgery: A Double-blind Randomized Clinical Trial. Photochem. Photobiol. 2021, 97, 1129–1135. [Google Scholar] [CrossRef]
- Badravalli Gururaj, S.; Shankar, S.; Parveen, F.; Kunthur Chidambar, C.; Bhushan, K.S.; Prabhudev, C. Assessment of Healing and Pain Response at Mandibular Third Molar Extraction Sites with and Without Pre- and Postoperative Photobiomodulation at Red and Near-infrared Wavelengths: A Clinical Study. J. Pharm. Bioallied Sci. 2022, 14, S470–S474. [Google Scholar] [CrossRef]
- Ahrari, F.; Eshghpour, M.; Zare, R.; Ebrahimi, S.; Fallahrastegar, A.; Khaki, H. Effectiveness of Low-level Laser Irradiation in Reducing Pain and Accelerating Socket Healing After Undisturbed Tooth Extraction. J. Laser Med. Sci. 2020, 11, 274. [Google Scholar] [CrossRef]
- Tortorici, S.; Messina, P.; Scardina, G.A. Effectiveness of Low-level Laser Therapy on Pain Intensity After Lower Third Molar Extraction. Int. J. Clin. Dent. 2019, 12, 357–367. [Google Scholar]
- Das, A.; Vidya, K.C.; Srikar, M.V.; Pathi, J.; Jaiswal, A. Effectiveness of Low-level Laser Therapy After Surgical Removal of Impacted Mandibular Third Molars: A Randomized Clinical Trial. Natl. J. Maxillofac. Surg. 2022, 13, 60. [Google Scholar] [CrossRef]
- Ali, M.; Al-Adili, S. Low level laser therapy on postoperative trismus and swelling after surgical removal of impacted lower third molar. Indian J. Public Health Res. Dev. 2019, 10, 9. [Google Scholar] [CrossRef]
- Ferreira, G.M.; Prado, L.F.; Santos, K.; Rodrigues, L.; Valladares-Neto, J.; de Torres, É.M.; Silva, M.A. Efficacy of Two Low-level Laser Therapy Protocols Following Lower Third Molar Surgery—A Randomized, Double-blind, Controlled Clinical Trial. Acta Odontol. Latinoam. 2022, 35, 31–38. [Google Scholar] [CrossRef]
- El Saeed, A.; Al-Fakharany, A. Effect of single dose low-level laser therapy on some sequalae after impacted lower third molar surgery. Al-Azhar J. Dent. Sci. 2020, 23, 41–47. [Google Scholar]
- Peimani, A.; Sardari, F.; Sarafi, S.; Sarafi, S.; Aghdam, H.; Chiniforush, N. The evaluation of photobiomodulation by 980 nm diode laser on postoperative complications after third molar surgery. J. Regen. Reconstr. Restor. (Triple R) 2018, 3, x. [Google Scholar]
- Fakour, S.; Hashemzehi, H.; Jahantigh, H.; Arab, K.; Gholami, L. Adjunctive Low-level Laser Therapy Using 980-nm Diode Laser after Impacted Mandibular Third Molar Surgery: A Randomized Clinical Trial. Avicenna J. Clin. Med. 2020, 26, 199–205. [Google Scholar] [CrossRef]
- Jivrajani, S.J.; Bhad, W.A. Effect of Low Intensity Laser Therapy (LILT) on MMP-9 Expression in Gingival Crevicular Fluid and Rate of Orthodontic Tooth Movement in Patients Undergoing Canine Retraction: A Randomized Controlled Trial. Int. Orthod. 2020, 18, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Farhadian, N.; Miresmaeili, A.; Borjali, M.; Salehisaheb, H.; Farhadian, M.; Rezaei-Soufi, L.; Alijani, S.; Soheilifar, S.; Farhadifard, H. The Effect of Intra-oral LED Device and Low-level Laser Therapy on Orthodontic Tooth Movement in Young Adults: A Randomized Controlled Trial. Int. Orthod. 2021, 19, 612–621. [Google Scholar] [CrossRef]
- Lalnunpuii, H.; Batra, P.; Sharma, K.; Srivastava, A.; Raghavan, S. Comparison of Rate of Orthodontic Tooth Movement in Adolescent Patients Undergoing Treatment by First Bicuspid Extraction and En-mass Retraction, Associated with Low Level Laser Therapy in Passive Self-ligating and Conventional Brackets: A Randomized Controlled Trial. Int. Orthod. 2020, 18, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Mistry, D.; Dalci, O.; Papageorgiou, S.N.; Darendeliler, M.A.; Papadopoulou, A.K. The Effects of a Clinically Feasible Application of Low-level Laser Therapy on the Rate of Orthodontic Tooth Movement: A Triple-blind, Split-mouth, Randomized Controlled Trial. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Hasan, A.; Rajeh, N.; Hajeer, M.; Hamadah, O.; Ajaj, M. Evaluation of the acceleration, skeletal and dentoalveolar effects of low-level laser therapy combined with fixed posterior bite blocks in children with skeletal anterior open bite: A three-arm randomised controlled trial. Int. Orthod. 2022, 20, 100597. [Google Scholar] [CrossRef]
- Pérignon, B.; Bandiaky, O.N.; Fromont-Colson, C.; Renaudin, S.; Pere, M.; Badran, Z.; Cuny-Houchmand, M.; Soueidan, A. Effect of 970 Nm Low-level Laser Therapy on Orthodontic Tooth Movement During Class II Intermaxillary Elastics Treatment: A RCT. Sci. Rep. 2021, 11, 23226. [Google Scholar] [CrossRef]
- Lo Giudice, A.; Nucera, R.; Leonardi, R.; Paiusco, A.; Baldoni, M.; Caccianiga, G. A Comparative Assessment of the Efficiency of Orthodontic Treatment with and Without Photobiomodulation During Mandibular Decrowding in Young Subjects: A Single-center, Single-blind Randomized Controlled Trial. Photobiomodul. Photomed. Laser Surg. 2020, 38, 272–279. [Google Scholar] [CrossRef]
- Matos, D.S.; Palma-Dibb, R.G.; de Santos, C.O.; da Saraiva, M.C.P.; Marques, F.V.; Matsumoto, M.A.N.; Romano, F.L. Evaluation of Photobiomodulation Therapy to Accelerate Bone Formation in the Mid Palatal Suture After Rapid Palatal Expansion: A Randomized Clinical Trial. Lasers Med. Sci. 2021, 36, 1039–1046. [Google Scholar] [CrossRef]
- Eid, F.; El-Kenany, W.A.; Mowafy, M.; El-Kalza, A.R.; Guindi, M. A Randomized Controlled Trial Evaluating the Effect of Two Low-level Laser Irradiation Protocols on the Rate of Canine Retraction. Sci. Rep. 2022, 12, 10074. [Google Scholar] [CrossRef]
- Isola, G.; Matarese, M.; Briguglio, F.; Grassia, V.; Picciolo, G.; Fiorillo, L.; Fiorillo, L.; Matarese, G. Effectiveness of Low-level Laser Therapy During Tooth Movement: A Randomized Clinical Trial. Materials 2019, 12, 2187. [Google Scholar] [CrossRef]
- da Costa Pereira, S.C.; Alvarez Avila, F.E.; Pinzan, A.; Lima, L.M.; Storniolo-Souza, J.M.; Janson, G. Low Intensity Laser Influence on Orthodontic Movement: A Randomized Clinical and Radiographic Trial. J. Indian Orthod. Soc. 2020, 54, 127–134. [Google Scholar] [CrossRef]
- Zheng, J.; Yang, K. Clinical Research: Low-level Laser Therapy in Accelerating Orthodontic Tooth Movement. BMC Oral Health 2021, 21, 324. [Google Scholar] [CrossRef]
- Özsoy, B.; Güldüren, K.; Kamiloğlu, B. Effect of Low-level Laser Therapy on Orthodontic Tooth Movement During Miniscrew-supported Maxillary Molar Distalization in Humans: A Single-blind, Randomized Controlled Clinical Trial. Lasers Med. Sci. 2023, 38, 76. [Google Scholar] [CrossRef] [PubMed]
- Abellán, R.; Gómez, C.M.; Palma, J.C. Effects of Photobiomodulation on the Upper First Molar Intrusion Movement Using Mini-screws Anchorage: A Randomized Controlled Trial. Photobiomodul. Photomed. Laser Surg. 2021, 39, 518–527. [Google Scholar] [CrossRef] [PubMed]
- Kamran, M.A. Effect of Photobiomodulation on Orthodontic Tooth Movement and Gingival Crevicular Fluid Cytokines in Adolescent Patients Undergoing Fixed Orthodontic Therapy. Photobiomodul. Photomed. Laser Surg. 2020, 9, 537–544. [Google Scholar] [CrossRef]
- Ekici, Ö.; Dündar, Ü.; Gökay, G.; Büyükbosna, M. Evaluation of the Efficiency of Different Treatment Modalities in Individuals with Painful Temporomandibular Joint Disc Displacement with Reduction: A Randomised Controlled Clinical Trial. Br. J. Oral Maxillofac. Surg. 2022, 60, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Ekici, Ö.; Dündar, Ü.; Büyükbosna, M. Effectiveness of High-intensity Laser Therapy in Patients with Myogenic Temporomandibular Joint Disorder: A Double-blind, Placebo-controlled Study. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e90–e96. [Google Scholar] [CrossRef]
- Chellappa, D.; Thirupathy, M. Comparative Efficacy of Low-level Laser and TENS in the Symptomatic Relief of Temporomandibular Joint Disorders: A Randomized Clinical Trial. Indian J. Dent. Res. 2020, 31, 42–47. [Google Scholar] [CrossRef]
- Shousha, T.M.; Mohamed Alayat, M.S.M.; Moustafa, I.M.; Moustafa, I.M. Effects of Low-level Laser Therapy Versus Soft Occlusive Splints on Mouth Opening and Surface Electromyography in Females with Temporomandibular Dysfunction: A Randomized-controlled Study. PLoS ONE 2021, 16, e0258063. [Google Scholar] [CrossRef]
- Madani, A.; Ahrari, F.; Fallahrastegar, A.; Daghestani, N. A Randomized Clinical Trial Comparing the Efficacy of Low-level Laser Therapy (LLLT) and Laser Acupuncture Therapy (LAT) in Patients with Temporomandibular Disorders. Lasers Med. Sci. 2020, 35, 181–192. [Google Scholar] [CrossRef]
- Brochado, F.T.; de Jesus, L.H.; Carrard, V.C.; Freddo, A.L.; Chaves, K.D.B.; Martins, M.D. Comparative Effectiveness of Photobiomodulation and Manual Therapy Alone or Combined in TMD Patients: A Randomized Clinical Trial. Braz. Oral Res. 2018, 32, e50. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.A.; de Melchior, M.O.; Magri, L.V.; Mazzetto, M.O. Can the Severity of Orofacial Myofunctional Conditions Interfere with the Response of Analgesia Promoted by Active or Placebo Low-level Laser Therapy? Cranio 2020, 38, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Aisaiti, A.; Zhou, Y.; Yue, W.; Zhou, W.; Wang, C.; Zhao, J.; Yu, L.; Zhang, J.; Wang, K.; Wang, K. Effect of Photobiomodulation Therapy on Painful Temporomandibular Disorders. Sci. Rep. 2021, 11, 9049. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, L.; Ferreira, R.; Resende, T.; Pacheco, J.; Salazar, F. Effectiveness of Photobiomodulation in Temporomandibular Disorder-related Pain Using a 635 Nm Diode Laser: A Randomized, Blinded, and Placebo-controlled Clinical Trial. Photobiomodul. Photomed. Laser Surg. 2020, 38, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Magri, L.V.; Carvalho, V.A.; Rodrigues, F.C.C.; Bataglion, C.; Leite-Panissi, C.R.A. Non-specific Effects and Clusters of Women with Painful TMD Responders and Non-responders to LLLT: Double-blind Randomized Clinical Trial. Lasers Med. Sci. 2018, 33, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Gomes da Silva Dias, W.C.F.; Cavalcanti, R.V.A.; Magalhães Junior, H.V.; de Pernambuco, L.A.; dos Santos Alves, G.Â. Effects of Photobiomodulation Combined with Orofacial Myofunctional Therapy on the Quality of Life of Individuals with Temporomandibular Disorder. Codas 2022, 34, e20200313. [Google Scholar] [CrossRef]
- Batra, S.; Srivastava, A.; Shivakumar, G.; Marrapodi, M.; Herford, A.; Cicciu, M.; Minervini, G. Comparative effectiveness of low-level laser therapy and transcutaneous electrical nerve stimulation in symptomatic temporomandibular joint disorders: A Randomized Control Trial. J. Oral Rehabil. 2023, 50, 1185–1193. [Google Scholar] [CrossRef]
- Mengue Maggi Borges, R.; Steffen Cardoso, D.; Chuaste Flores, B.; Dimer da Luz, R.; Roberta Machado, C.; Pessoa Cerveira, G.; Boff Daitx, R.; Baptista Dohnert, M. Effects of Different Photobiomodulation Dosimetries on Temporomandibular Dysfunction: A Randomized, Double-blind, Placebo-controlled Clinical Trial. Lasers Med. Sci. 2018, 33, 1859–1866. [Google Scholar] [CrossRef]
- Maracci, L.M.; Stasiak, G.; de Chami, V.O.; Franciscatto, G.J.; de Milanesi, J.M.; Figueiró, C.; Silva, T.B.; Guimarães, M.B.; Marquezan, M. Treatment of Myofascial Pain with a Rapid Laser Therapy Protocol Compared to Occlusal Splint: A Double-blind, Randomized Clinical Trial. Cranio 2020, 5, 433–439. [Google Scholar] [CrossRef]
- De Oliveira Chami, V.; Maracci, L.M.; Tomazoni, F.; Centeno, A.C.T.; Porporatti, A.L.; Ferrazzo, V.A.; Marquezan, M. Rapid LLLT Protocol for Myofascial Pain and Mouth Opening Limitation Treatment in the Clinical Practice: An RCT. Cranio 2020, 4, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Nadershah, M.; Abdel-Alim, H.M.; Abdel-Alim, H.M.; Bayoumi, A.M.; Bayoumi, A.M.; Jan, A.M.; Elatrouni, A.; Jadu, F.M. Photobiomodulation Therapy for Myofascial Pain in Temporomandibular Joint Dysfunction: A Double-blinded Randomized Clinical Trial. J. Maxillofac. Oral Surg. 2020, 19, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Mansourian, A.; Pourshahidi, S.; Sadrzadeh-Afshar, M.-S.; Ebrahimi, H. A Comparative Study of Low-level Laser Therapy and Transcutaneous Electrical Nerve Stimulation as an Adjunct to Pharmaceutical Therapy for Myofascial Pain Dysfunction Syndrome: A Randomized Clinical Trial. Front. Dent. 2019, 16, 256. [Google Scholar] [CrossRef]
- Desai, A.P.; Roy, S.K.; Semi, R.S.; Balasundaram, T. Efficacy of Low-level Laser Therapy in Management of Temporomandibular Joint Pain: A Double Blind and Placebo Controlled Trial. J. Maxillofac. Oral Surg. 2021, 3, 948–956. [Google Scholar] [CrossRef]
- Bakry, S.; Awad, S.; Kamel, H.M. Comparative Evaluation of Low-level Laser Therapy (lllt) Versus Sodium Hyaluronate with Arthrocentesis in Management Temporomandibular Joint Disorders (tmd): A Clinical Randomized Controlled Study. Egypt. Dent. J. 2021, 67, 1077–1087. [Google Scholar] [CrossRef]
- Baiomy, A.A.; Baiomy, A.; Farhat, M.; Helal, M.A. Efficacy of Occlusal Splints and Low-level Laser Therapy on the Mandibular Range of Motion in Subjects with Temporomandibular Joint Disc Displacement with Reduction. J. Int. Soc. Prev. Community Dent. 2023, 13, 229–236. [Google Scholar] [CrossRef]
- Marques, M.; Diniz, I.; de Cara, S.; Pedroni, A.; Abe, G.; D’Almeida-Couto, R.; Lima, P.; Tedesco, T.; Moreira, M. Photobiomodulation of Dental Derived Mesenchymal Stem Cells: A Systematic Review. Photomed. Laser Surg. 2016, 34, 500–508. [Google Scholar] [CrossRef]
- Rech, C.; Pansani, T.; Cardoso, L.; Ribeiro, I.; Silva-Sousa, Y.; de Souza Costa, C.; Basso, F. Photobiomodulation using LLLT and LED of cells involved in osseointegration and peri-implant soft tissue healing. Lasers Med. Sci. 2022, 37, 573–580. [Google Scholar] [CrossRef]
- Shamshiri, A.; Moslemi, N. Efficacy of photobiomodulation therapy on neurosensory recovery in patients with inferior alveolar nerve injury following oral surgical procedures: A systematic review. Quintessence Int. 2021, 52, 140–153. [Google Scholar]
- Femiano, F.; Femiano, R.; Scotti, N.; Nucci, L.; Lo Giudice, A.; Grassia, V. The Use of Diode Low-Power Laser Therapy before In-Office Bleaching to Prevent Bleaching-Induced Tooth Sensitivity: A Clinical Double-Blind Randomized Study. Dent. J. 2023, 11, 176. [Google Scholar] [CrossRef]
- Femiano, F.; Femiano, L.; Nucci, L.; Grassia, V.; Scotti, N.; Femiano, R. Evaluation of the Effectiveness on Dentin Hypersensitivity of Sodium Fluoride and a New Desensitizing Agent, Used Alone or in Combination with a Diode Laser: A Clinical Study. Appl. Sci. 2022, 12, 6130. [Google Scholar] [CrossRef]
- Cosola, S.; Kim, Y.; Park, Y.; Giammarinaro, E.; Covani, U. Coronectomy of Mandibular Third Molar: Four Years of Follow-Up of 130 Cases. Medicina 2020, 56, 654. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, R.; Rastogi, S.; Rohatgi, R.; Abdulrahman, B.; Dutta, S.; Giri, K. Does pedicle flap design influence the postoperative sequel of lower third molar surgery and quality of life? J. Oral Biol. Craniofac. Res. 2022, 12, 694–701. [Google Scholar] [CrossRef] [PubMed]
- DE Marco, G.; Lanza, A.; Cristache, C.; Capcha, E.; Espinoza, K.; Rullo, R.; Vernal, R.; Cafferata, E.; DI Francesco, F. The influence of flap design on patients’ experiencing pain, swelling, and trismus after mandibular third molar surgery: A scoping systematic review. J. Appl. Oral Sci. 2021, 29, e20200932. [Google Scholar] [CrossRef] [PubMed]
- Bilir, H.; Kurt, H. Influence of Stabilization Splint Thickness on Temporomandibular Disorders. Int. J. Prosthodont. 2022, 35, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Gikić, M.; Vrbanović, E.; Zlendić, M.; Alajbeg, I. Treatment responses in chronic temporomandibular patients depending on the treatment modalities and frequency of parafunctional behaviour. J. Oral Rehabil. 2021, 48, 785–797. [Google Scholar] [CrossRef] [PubMed]
- Supakomonnun, S.; Mitrirattanakul, S.; Chintavalakorn, R.; Saengfai, N. Influence of functional and esthetic expectations on orthodontic pain. J. Orofac. Orthop. 2023, 84, 141–146. [Google Scholar] [CrossRef]
- Verrusio, C.; Iorio-Siciliano, V.; Blasi, A.; Leuci, S.; Adamo, D.; Nicolò, M. The effect of orthodontic treatment on periodontal tissue inflammation: A systematic review. Quintessence Int. 2018, 49, 69–77. [Google Scholar] [CrossRef]
- Parker, S. Laser Photonic Energy Delivery in Clinical Dentistry: Scrutiny of Parameter Variables. Ph.D. Thesis, De Montfort University, Leicester, UK, May 2023. Available online: https://dora.dmu.ac.uk/items/5a60b157-6d26-46ad-ab2a-657aebbef704 (accessed on 16 May 2023).
- Parker, S.; Cronshaw, M.; Grootveld, M.; George, R.; Anagnostaki, E.; Mylona, V.; Chala, M.; Walsh, L.J. The Influence of Delivery Power Losses and Full Operating Parametry on the Effectiveness of Diode Visible–near Infra-red (445–1064 nm) Laser Therapy in Dentistry—A Multi-centre Investigation. Lasers Med. Sci. 2022, 37, 2249–2257. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mediator | Molecules | Action and/or Effects |
|---|---|---|
| Growth factors | GDNF, FGF, β FGF, IGF-1 KGF, PDGF, TGF-β, VEGF | Proliferation, Differentiation, Angiogenesis, Migration, Chemotaxis |
| Anti-inflammatory cytokines | IL-2, IL-4, IL-8, IL-10 | Differentiation, Proliferation, Immune activation, Chemotaxis, Angiogenesis |
| Pro-inflammatory cytokines | IL-1a, IL-1b, IL-6, TNF-α, PGE2, COX2 | Stimulate and accelerate inflammation, Angiogenesis, Promote cell migration, Anti- and pro-apoptosis |
| Heat shock proteins | HSP90, HSP70, HSP25 | Chaperone protein, Enhance cell survival |
| Matrix metalloproteinases | MMP2, MMP9 | Cell survival, Prevention of terminal differentiation, Tissue remodelling |
| Small molecules | ATP, GSH, ROS, Ca2+, NO, H+ | Normalisation of cell function; Migration; Angiogenesis; Proliferation |
| Published Data by Study—PBM-Adjunctive Third Molar Oral Surgery | ||||||
|---|---|---|---|---|---|---|
| Citation—Oral Surgery | Aim of Study | Test Group/ Control/Placebo | Laser λ | Laser Operating Parameters | Application/Repetition | Outcome |
| De Oliveira, R., et al., 2021 [25] | RCT. Post extraction paraesthesia. Laser vs. laser acupuncture | 60 pts (3 groups × 20). No placebo. (i) 20 medication—C (ii) 20 laser—LT (iii) 20 laser acupuncture—LA | 808 nm | 100 mW irradiation CW mode contact, punctual. Spot: 0.028 cm2 acupuncture; 6 sites, same parameters. | 26 points—1 cm apart (40 s per point). Irrad. 3.57 W/cm2. 20 sessions (2 × week × 10 weeks) | T1: Before Tx/T 2:5 weeks T3: 10 weeks/ T1, T2: L = LA = C T3: L > LA > C p T1 > 0.05, T2 > 0.05, T3 0.003 |
| Souza, M., et al., 2023 [26] | RCT. Post-extraction OHRQoL. Laser PBM vs. aPDT vs. PBM + aPDT. | 40 pts (4 groups × 10). No placebo. (i) 10 extractions without any additional treatment—C (ii) 10 extractions + aPDT (iii) 10 extractions + PBM (iv) 10 extractions + PBM + aPDT | aPDT—660 nm PBM—808 nm | aPDT: 100 mW CW, output energy fluence 300 J/cm2, spot of 3 mm2, irradiance of 3.33 W/cm2 for 90 s PBM: 100 mW CW, output energy of 4 J, fluence of 133 J/cm2, spot of 3 mm2, and irradiance of 3.33 W/cm2 for 40 s | PBM therapy appl. to vestibular and lingual gingiva. Contact/CW modes. Single administration | T0: At extraction, T1: 7 days, T2: 30 days. +ve OHIP-14 scores sig. different in T0—T1 and T0—T2 for all (p < 0.001). PBM + aPDT > PBM > other groups. Groups (ii), (iii), (iv) sig. +ve OHRQoL vs. control at T1 (p 0.01–0.043). Best: T1 and T2 with PBM + aPDT. |
| Momeni, E., et al., 2021 [27] | RCT. Impact of laser PBM on post-op pain, trismus | 25 pts. 1 tooth per side. Each pt received (i) PBM to one side and (ii) placebo to contra lateral side. | 940 nm | Application/point time 30 s. Fluence at each point (J/cm2), 10 Power (W), 0.5 CW | Application technique, non-contact. Three application points (three occlusal, buccal, and lingual). Laser applied only on extn day. | VAS pain every day post-op. No sig. diff. between the two groups. Trismus immediately after extn, 2nd and 7th day. No sig. diff. between the two groups (p > 0.05). Mean swelling did not differ significantly (p > 0.05). |
| Isolan, C., et al., 2021 [28] | RCT. Impact of laser PBM on post-op pain. | 44 pts (101 extns) Random. No placebo. (i) Control (n = 50)—surgical removal (ii) Test (n = 51)—extn + laser PBM | 808 nm | Output 50 mW CW. Spot area: 0.4 cm2 Dose per point: 11 J. Total dose of 66 J. | Laser applied only on extn day. T0—extn day + 6 h T1—24 h; T2 48 h. 6 contact points 2-apical + cervical in buccal, lingual and occlusal. | PBMT showed stat. sig. effect (p < 0.001) on VAS pain at T0. Similar VAS pain was observed at T24 (p < 0.001) and T48 (p < 0.001). PBMT. |
| Asutay, F., et al., 2018 [29] | RCT. Impact of laser PBM on post-op outcome | 45 pts. 3 groups: (i) n = 15 Control—ice (ii) n = 15 Test—laser PBM (iii) n = 15 Test—placebo PBM) | 810 nm | Output power: 0.3 W CW, beam area: 3 cm2, energy density: 4 J/cm2, energy delivered: 12 J, irradiation time 40 s | Application Non-contact | VAS pain on days #2 and 7. Swelling on days #2 and 7. No stat. sig. differences between all groups for edema and trismus results (p > 0.05). |
| Bianchi de Moraes, M., 2020 [30] | RCT. Impact of laser PBM on post-op outcome | 57 patients: 3 groups: (i) (low PBM) 19 (ii) (high PBM) 20 (iii) (placebo) 18 | 660 nm | For both laser groups, output: 30 mW CW, beam area: 0.03 cm2, power: 0.03 W, application/point time: (i) 2.25/(ii) 7 s, (i) fluence: 10 J/cm2, (ii) fluence: 30 J/cm2 | Laser application immediate on days #3 and 7. 4 application points: buccal/lingual/cervical/apical. | Post-op pain (VAS) and swelling. Periodontal condition at 6 months, all cf sham. Stat. sig. more effective in group #i—10-J/cm2 laser protocol. (p = 0.017 for the 10-J/cm2 group and p = 0.001 for the 30-J/cm2 group) |
| Mohajerani, H., et al., 2021 [31] | RCT. Impact of laser PBM on post-op outcome | 40 pts. 2 groups: (i) n = 20 extn control (ii) n = 20 extns + PBM (laser and LED) Placebo sham applied to control. | 810 nm LED 632nm | Output: 500 mW CW. Fluence: 5 J/cm2. Fluence: 2 J/cm2 | PBM applied immediately post extraction and 24 h later. Irradiation: 2 intraoral (1 lingual and 1 vestibular side of the wound and with 1 cm the from wound), 1 extraoral (masseter area) | Pain: days #3 and # 7 sig. less in PBM group (p = 0.03 and 0.01, respectively). Trismus: Sig. less in PBM group on day #3 (p = 0.006). On day #7, pain was not significant. Swelling: days #3 and #7 sig. less in PBM group (p < 0.0001). |
| Nunes, C., et al., 2023 [32] | RCT. Impact of laser PBM on post-op outcome | 22 pts (44 teeth). 2 groups: (i) n = 22 extn control (ii) n = 22 extn + laser PBM Placebo applied to control. | 808 nm | Output: 100 mW CW. Beam diameter: 600 µm. 40 s per area. | PBM applied immed post extraction + 24 h later. Placebo, same. 8 applicat spots: E/O 4 and I/O 4. | VAS pain only sig. diff (PBM group) on days #4 and 5 (p < 0.05). Opening: no sig. diff. Edema: no sig. diff. |
| Feslihan, E., et al., 2019 [33] | RCT. Impact of laser PBM vs. steroid on post-op outcome | 30 pts (60) teeth. 2 groups: (i) n = 30 extn control (ii) n = 30 extn + laser PBM No placebo | 810 nm | Output: 300 mW CW Fluence: 6 J/cm2 | Applied extra-orally to insertion point of masseter for 60 s. PBMT repeated on post-operative days 1 and 2. | PBMT was also effective in post-operative pain, edema and trismus at a level similar to that of methylprednisolone. No sig. diff. (p ≤ 0.05) |
| Nejat, A., et al., 2021 [34] | RCT. Impact of laser PBM on post-op osteitis + pain | 80 pts. 2 extns per pt, 1 month apart. 2 groups: (i) Extn + PBM (ii) Extn + placebo | 660 nm 810 nm | Output: 200 mW CW (beam area: ~0.64 cm2, 312.5 mW/cm2, 1 J, Fluence: 1.6 J/cm2). 810 nm, 200 mW CW (400 mW/cm2, 3 J, Fluence: 6 J/cm2). | Applied at ~1 cm to 4 points on socket at tissue surface at 3 points on buccal and lingual gingiva, for 15 s. PBM immediately after extraction and repeated on days #2, 4, 6. | PBM therapy significantly reduced the rate of AO development. In addition, it significantly reduced pain and the need to take analgesics (p ≤ 0.05). |
| Gururaj, S., et al., 2022 [35] | RCT. Impact of laser PBM on post-op outcome | 26 pts. 2 groups: (i) n = 13 pts extn control (ii) n = 13 extn + laser PBM. Random allocation. No placebo | 810 nm 660 nm | 810 nm irradiation at 100 mW CW. 120 s prior and 60 s for both post-extraction irradiations. | 810 nm to the site immed before and after extraction. Also, a transcutaneous irradiation of 660 nm 1-day post-op. Control group—no irradiation | Pain: VAS/Healing Turnbull and Howley’s Index for soft tissue healing on the 7th and 21st days. p: <0.0001. |
| Ahrari, F., et al., 2020 [36] | RCT. Impact of laser PBM on post-op outcome | 40 pts. 4 groups (4 × 10): (i) extn + 660 nm PBM (ii) extn + 810 nm PBM (iii) extn + 660 nm + 810 nm laser (iv) extn + placebo Random allocation. | 660 nm 810 nm | Both 660 nm + 810 nm laser: 200 mW CW output. 30 s radiation to lingual, buccal and occlusal surfaces of the socket, 6 J/area. 660 nm fluence: 4.21 J/cm2. 810 nm fluence: 21.4 J/cm2. | LLLT was performed after 0.5–1 h of extraction and 2 days later. | VAS over 7 days. Healing evaluated on 3rd + 7th days. No sig. diff. in pain scores (p > 0.05). The between-group diffs. in healing scores were small and insignificant (p > 0.05). No greater effect vs. placebo laser for reducing the complications. |
| Tortorici, S., et al., 2019 [37] | RCT. Impact of laser PBM on post-op pain | 41 pts. 2 third molar extns for each pt, 2 months apart. Random allocation | 940 nm | Output 4 W CW Beam size of 2.8 cm2 Energy per point was 1200 J in 10 s | First stage pts rec’d placebo laser (PL) 15 min before extraction and PBM immed. post-op. At 2 months—PBM 15 min pre-extn and PL immediately post op. | VAS at 4, 12, 24, 48, 72 and 168 h. Scores sig. lower in first stage at 4 h and 12 h post-op, VAS similar until 168 h. (p < 0.05). |
| Das, A., et al., 2022 [38] | RCT. Impact of laser PBM on post-op outcome | 30 pts. 2 groups: (i) n = 15 pts extn control (ii) n = 15 extns + laser PBM. Random allocation. No placebo | 660 nm | Output: 0.1-watt CW, Fluence: 6 J/cm2, 60 s | Application immed. post op and on 1st day post op. I/O—B, L, M, D and E/O facial. | Pain: VAS/Healing on day #2 and 7. p < 0.05. PBMT effective in reducing post-op pain, edema and trismus |
| Ali, M., et al., 2019 [39] | RCT. Impact of laser PBM on post-op swelling, trismus | 40 pts. 2 groups: (i) 20—extn + 980 nm PBM (ii) 20—extn + placebo Random allocation. | 980 nm | Output 100 mW CW. 30 s per point. | Application at 6 points—3 E/O, 3 I/O. | 2nd and 4th day sig. diff in swelling (p = 0.05). No sig. diff in trismus. |
| Ferreira, G., et al., 2022 [40] | RCT. Impact of laser PBM on post-op outcome | 21 pts. 42 teeth. (i) 21—extn + PBM (ii) 21—extn + placebo 15-day interval between sides. Random allocation. | 660 nm 789 nm | Output: 660 nm, 20 mW CW. I/O, 5 J/cm2, 10 s, 4 points Output: 789 nm, 60 mW CW. E/O: 30 J/cm2, 20 s, 8 points | PBM immed. post-op (T1), 24 (T2) and 48 (T3) hours | Pain control, swelling and trismus intensity at T1, T2, T3 and 7 days Pain: no sig. diff. (p = 0.909) No differences in swelling (p = 0.958) or trismus (p = 0.837) |
| El Saeed, A., et al., 2020 [41] | RCT. Impact of laser PBM on post-op outcome | 20 pts. 40 teeth. (i) 20—extn + PBM (ii) 20—extn + placebo 3-week interval between sides. Random allocation | 980 nm | Output: 0.5 W CW, 50 J total Beam: 12 cm2 Fluence: 4 J/cm2 | Single application E/O immediately post op. | Swelling, trismus and VAS pain. Sig. diff. between PBM and placebo sides p > 0.001 |
| Peimani, A., et al., 2018 [42] | RCT. Impact of laser PBM on post-op outcome | 30 pts. 2 groups (n = 15): (i) extn + PBM (ii) extn + placebo 3 week-interval between sides. Random allocation | 980 nm | Output: 0.5 W CW. Beam: 7 mm dia. Fluence: 39.06 J/cm2, 15 J total per site | Single application. E/O mandible. I/O B, L, O. 30 s per site. | Pain, trismus, QoL. Pain VAS day #2–7. No sig. diff in any measurable parameters (p ≤ 0.05). |
| Fakour, S., et al., 2020 [43] | RCT. Impact of laser PBM on post-op outcome | 40 pts. 2 groups: (i) n = 20 pts extn control (ii) n = 20 extn + laser PBM. Random allocation. No placebo | 980 nm | Output: 200 mW CW for 60 s per site. Fluence: 12 J/cm2 | Single application. I/O B and L. E/O angle of jaw. | Trismus and facial swelling assessed on day #2 and 7. No significant positive effects on reducing the post-operation complications. |
| Modified Risk of Bias—Oral Surgery (n = 19) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Citation | Randomisation | Sample Size Calc and Number Required | Blinding | Baseline Situation Similar for All Groups | Laser Parameters Complete/Calculations Correct | Optimal Fluence Applied | Power Meter Used | Numerical Results (Statistics) | No Missing Outcome Data | Correct Assessment of Results | Total |
| de Oliveira R et al. [25] | Yes | No | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | 8 |
| Souza M et al. [26] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | 9 |
| Momeni E et al. [27] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 7 |
| Isolan C et al. [28] | Yes | Yes | Yes | No | Yes | No | No | Yes | Yes | Yes | 7 |
| Asutay F et al. [29] | Yes | No | Yes | Yes | No | Yes | No | Yes | Yes | Yes | 7 |
| Bianchi de M et al. [30] | Yes | Yes | Yes | No | Yes | No | No | Yes | Yes | Yes | 7 |
| Mohajerani H et al. [31] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 7 |
| Nunes C et al. [32] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 7 |
| Feslihan E et al. [33] | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Yes | 8 |
| Nejat A et al. [34] | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | 9 |
| Gururaj S et al. [35] | Yes | No | Yes | Yes | No | No | No | Yes | Yes | Yes | 6 |
| Ahrari F et al. [36] | Yes | No | Yes | Yes | No | No | No | Yes | No | Yes | 5 |
| Tortorici S et al. [37] | Yes | No | Yes | Yes | No | No | No | Yes | Yes | Yes | 6 |
| Das A et al. [38] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 7 |
| Ali M et al. [39] | Yes | No | Yes | Yes | No | No | No | Yes | Yes | Yes | 6 |
| Ferreira G et al. [40] | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Yes | 8 |
| El Saeed A et al. [41] | Yes | No | Yes | Yes | No | No | No | Yes | Yes | Yes | 8 |
| Peimani A et al. [42] | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | 9 |
| Fakour S et al. [43] | Yes | No | Yes | Yes | No | No | No | Yes | Yes | Yes | 6 |
| Published Data by Study—PBM-Adjunctive Orthodontic Movement | ||||||
|---|---|---|---|---|---|---|
| Citation—Ortho Movement | Aim of Study | Test Group/ Control/Placebo | Laser λ | Laser Operating Parameters | Application/Repetition | Outcome |
| Sagar, J., et al., 2020 [44] | RCT effect of PBM on ortho movement | 10 pts. 2 groups: (i) 10—PBM (ii) 10—Control Random allocation | 980 nm | Output: 0.3 W CW. Spot: 400 µm dia. | 10 applications (5 B, 5 P) per exposure. Exp. time—15 s B, P. Total energy: 9 J (2 × 15 s × 0.3 W) PBM applied on days #0, 3, 7, 14. After every 15th day | Difference in the rate of displacements stat. sig. (p-value of 0.0026) |
| Farhadian, N., et al., 2021 [45] | RCT effect of PBM on ortho movement | 56 pts. 3 groups: (i) 17—LED (ii) 20—PBM laser (iii) 19—placebo Random allocation | 810 nm | Power: 100 mW CW. Tip was 3.1 mm, and the energy density was 4 J/cm2. | PBM used on days 0, 3, 30 and 60 3 points, buccal, and 3 points, palatal; 3 s each point. | Retraction sig. higher in laser group than control (p = 0.004); indicated a 60.8% increase in the rate of OTM as compared with the latter. |
| Lalnunpuii, H., et al., 2020 [46] | RCT effect of PBM on ortho movement | 65 pts. 3 groups: (i) 20 conventional ligation + PBM (ii) 20 self-ligation + PBM (iii) 25 Control Random allocation | 660 nm | Output—8 mW CW Fluence—2.29 J/cm2 Exposure time/point—10 s | 2 doses—cervical third, 2 doses—apical third, 1 dose—centre of the root. B + L laser regimen was applied on days 0, 3, 7 and 14 Thereafter, irradiations were performed every 15th day | Statistically significant enhancement in the rate of OTM in the 2 experimental groups (p < 0.05) |
| Mistry, D., et al., 2020 [47] | RCT effect of PBM on ortho movement | 20 pts. 2 groups: (i) 10 ortho + PBM (ii) 10 ortho + sham PBM Random allocation | 808 nm | Output: 0.20 W CW Irradiance: 1.97 W/cm2, 1.72 Joules (J) of energy per point, a total of 13.87 J per visit. | 8 points (B, 4 P). 10 s per point. PBM applied at beginning day 0 (T0), day 28 (T1) and day 56 (T2) | LLLT every 4 weeks did not result in differences in the amount of tooth movement, anchorage loss or canine rotation during extraction space closure. (p = 0.27) |
| Hasan, A., et al., 2022 [48] | RCT effect of PBM on ortho movement | 42 patients. 3 groups: (i) 14 fixed posterior bite block + PBM (ii) 14 Bite block (iii) 14 Untreated Random allocation | 808 nm | Output: 250 mW CW Energy at 4 J, and the application time was 16 s/point. | 6 points—3 B, 3 P applied at the first visit; then, days 3, 7 and 14 of the first month. Afterward, it was applied every 15 days until end of Tx | Correction of the AOB required significantly less mean time in the PBM group compared to the FPBB group (x = 7.07, x = 9.42 months, respectively; p = 0.001). |
| Pérignon, B., et al., 2021 [49] | RCT effect of PBM on ortho movement | 42 patients. 2 groups: (i) 21 ortho + PBM (ii) 21 ortho placebo Random allocation | 970 nm | Output 500 mW CW. Spot: 2 mm dia. Fluence: 30 J/cm2. Exposure point received 0.9 J. | 6 points per tooth, 3 B, 3 P. Second laser application session was carried out 1 month after the first | Distance of movement was sig. greater than that on the placebo side (p = 0.009). |
| Lo Giudice, A., et al., 2020 [50] | RCT effect of PBM on ortho movement | 89 patients. 2 groups: (i) 43 ortho + PBM (ii) 46 ortho + control Random allocation | Multi λ 450 to 835 nm | Biostim panel setting. 6 min of irradiation, producing 48 J/cm2 of fluence | PBM every 14 days. 3 sessions, total duration of 18 min and 144 J/cm2 of fluency was administered (i.e., 48 J/cm2 3 stages). | Treatment time was significantly shorter (p < 0.001) for the PBM group |
| Matos, D., et al., 2021 [51] | RCT effect of PBM on max. expansion ortho movement | 34 pts. 2 groups: (i) 18—PBM (ii) 16—placebo Random allocation | 980 nm | Output: 300 mW CW Spot size: 1.26 cm2 Irrad: 238.8 mW/cm2 Exposure: 10 s/point Radiant exp: 238.85 J/cm2 Radiant energy: 3 J/point | 6 spots bilaterally distributed along MPS for 10 s. 12 applications over 10 weeks (1, 5, 10 and 15 days, and once a week for 8 weeks) | PBMT did not accelerate bone regeneration in the MPS (p = 0.2273) |
| Eid, F., et al., 2022 [52] | RCT effect of PBM on ortho movement | 20 pts. 2 groups: (i) 10—PBM (ii) 10—PBM Different frequency of application Random allocation | 980 nm | Output: 100 mW CW Fluence: 8 J/cm2 | days 0, 3, 7, 14 and every 2 weeks thereafter. Group B, PBM applied every 3 weeks on experimental sides, throughout the study period (12 weeks). | PBM can efficiently accelerate the rate of orthodontic tooth movement to approx 1.4 folds, whether applied with a high frequency or with less frequent applications (p < 0.001). |
| Isola, G., et al., 2019 [53] | RCT effect of PBM on ortho movement | 41 pts. 2 groups: (i) 41—PBM (ii) 41—Control Random allocation | 980 nm | Output: 1 W CW Spot size: 600 µm dia. Energy density of 8 J | Buccal/palatal on 3 pts/side (dist, medial and mes.) at baseline and 3, 7, 14 days and every 15 days | Laser group: less mean time required to accomplish space closure compared to the control group (p < 0.001). |
| Pereira, S., et al., 2020 [54] | RCT effect of PBM on ortho movement | 11 pts. 2 groups: (i) 11—PBM (ii) 11—Control Random allocation | 780 nm | Mand: output: 40 mW CW; fluence: 10 J/cm2; exposure: T 10 s. Max B: output: 40 mW; fluence: 10 J/cm2; expos T: 10 s. Max P: power: 70 mW; fluence: 35 J/cm2; expos T: 20 s; spot: 0.04 cm2 | Mand: 10 irradiations were carried out each time, 5 on each buccal and lingual. Max B & P: A total of 5 irradiations carried out each time. Laser therapy ended after 90 days | No difference in movement between the irradiated and nonirradiated sides. (p < 0.05) |
| Zheng, J., et al., 2021 [55] | RCT effect of PBM on ortho movement | 12 pts. 2 groups: (i) 12—PBM (ii) 12—Control Random allocation | 810 nm | Output: 100 mW CW. Fluence: 6.29 J/cm2. | Applied 4 points (M, D, B, P), 40 s on each surface. PBM applied on days #1, 7, 14 and 21 | PBM appeared to increase IL-1β, RANKL and OPG on day #7. |
| Özsoy, B., et al., 2023 [56] | RCT effect of PBM on ortho movement | 20 pts. 2 groups: (i) 10—PBM (ii) 10—Control Random allocation | 980 nm | Output: 20 mW CW Spot: 0.28 cm2 Fluence: 0.71 J/cm2 2 J total energy/molar | PBM pn day #0, 3, 7, 14, 21, 42, 63. Total no. of points, 16. 10 s (per point) | Movement on PBM sig. Higher at all time intervals (1–2) (2–3) (p < 0.001) |
| Abellán, R., et al., 2021 [57] | RCT effect of PBM on ortho movement | 20 pts. 2 groups: (i) 10—Control (ii) 10—PBM Random allocation | 670 nm | Output: 150 mW CW Av fluence: 11.3 J/cm2 Irradiance: 4.78 W/cm2 Spot diameter: 2 mm | Exposure: 3 min/dental surface (total 12 min) Days #0, 1, 2, 3, 4, 7 and in each Tx month. | No significant differences (p > 0.05). |
| Kamran, M. 2020 [58] | RCT effect of PBM on ortho movement | 44 pts. 2 groups: (i) 44—Control (ii) 44—PBM Random allocation | 808 nm | Output: 100 mW G-CW, 50 Hz, 50% duty. Fluence: 25 J/cm2 Area covered: (cm2) 0.04 | Applied for 10 s at 10 points PBM in 4 visits: application days: #0, 3, 7, 14. | PBM group sig. greater in at 1 month (p = 0.04) and 2 months (p < 0.001) |
| Modified Risk of Bias—Orthodontics (n = 15) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Citation | Randomisation | Sample Size Calc & Number Required | Blinding | Baseline Situation Similar for All Groups | Laser Parameters Complete/Calculations Correct | Optimal Fluence Applied | Power Meter Used | Numerical Results (Statistics) | No Missing Outcome Data | Correct Assessment of Results | Total |
| Sagar J et al. [44] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 7 |
| Farhadian N et al. [45] | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | No | Yes | 8 |
| Lalnunpuii H et al. [46] | Yes | Yes | Yes | No | Yes | No | No | Yes | Yes | Yes | 7 |
| Mistry D et al. [47] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 7 |
| Hasan A et al. [48] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 7 |
| Pérignon B et al. [49] | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | 8 |
| Lo Giudice A et al. [50] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 7 |
| Matos D et al. [51] | Yes | Yes | Yes | No | No | No | No | Yes | Yes | Yes | 6 |
| Eid F et al. [52] | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | 9 |
| Isola G et al. [53] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 7 |
| Pereira S et al. [54] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 7 |
| Zheng J et al. [55] | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 7 |
| Özsoy B et al. [56] | Yes | No | Yes | Yes | Yes | No | No | Yes | Yes | Yes | 7 |
| Abellán R et al. [57] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 9 |
| Kamran M et al. [58] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 7 |
| Published Data by Study—PBM-Adjunctive TMJ Therapy | ||||||
|---|---|---|---|---|---|---|
| Citation—TMJ | Aim of Study | Test Group/ Control/Placebo | Laser λ | Laser Operating Parameters | Application/Repetition | Outcome |
| Ekici, Ö., et al., 2022 [59] | RCT. Impact of laser PBM on TMJ therapy | 132 pts. 4 groups: (i) 38—OS (ii) 38—US (iii) 38—PBM (iv) 38—Control Random allocation | 1064 nm | 15–20 Hz Fluence 360 J/cm2 | Five times a week for 4 weeks, 15 min per session. 3 applications: 100 cm2 per 30 s/static masseter and temporal/100 cm2 in 60 s | Significant improvements were observed in terms of pain, function, disability and quality of life at both the 4th and 12th weeks compared to the control group (p < 0.001). QoL scores diff with PBM and US. |
| Ekici, Ö., et al., 2022 [60] | RCT. Impact of laser PBM on TMJ therapy | 76 pts. 2 groups: (i) 38—laser PBM (ii) 38—placebo PBM Random allocation | 1064 nm | 10.5 W Av. FRP. 10–40 Hz, a probe diameter of 0.5 cm, and a spot size of 0.2 cm2 | Applied 1/day × 15 d × period of 3 weeks. 3 applications: 100 cm2 per 30 s/static masseter and temporal/100 cm2 in 60 s | Evaluated for pain, the range of motion of the jaw, disability and quality of life (p ≤ 0.001) |
| Chellappa, D., et al., 2020 [61] | RCT. Impact of laser PBM on TMJ therapy | 60 pts. 2 groups: (i) 30—PBM (ii) 30—TENS Random allocation | 672 nm | Output: 50 mW CW. 3 J/site/4 sites (mass, temp, condyle, i-auricular portion). | Tx on altern days; 2 sessions/week × 3 weeks. Each point: 120 s PBMT, using scanning | VAS scores for pain and movement. Stat. sig. difference between LLLT and TENS groups |
| Shousha, T., et al., 2021 [62] | RCT. Impact of laser PBM on TMJ therapy | 112 pts. 3 groups: (i) 37—PBM (ii) 37—splint OST (iii) 38—control Random allocation | 940 nm | Output: 0.2 W CW 2 J energy. 10 s with an energy density of 2.5 J/cm2. | Sessions were scheduled 3 days a week (every other day) for a total of 10 sessions | TMJ opening index (TOI), visual analogue scale (VAS), surface electromyography (sEMG). Sig. diff. in improving VAS, TOI and sEMG |
| Madani, A., et al., 2020 [63] | RCT. Impact of laser PBM on TMJ therapy | 45 pts. 3 groups: (i) 15—PBM (ii) 15—acupuncture (LAT) PBM (iii) 15—placebo Random allocation | 810 nm | Output: 200 mW CW, Gaussian beam, spot size: 0.28 cm2, fluence: 21 J/cm2 | Pre-Tx (T1), after 5 (T2) and 10 (T3) laser appls, +1 m. (T4). Appl 2 × week, 30s/pt × 5 weeks. In LAT, PBM on acupuncture points (ST6, ST7, LI4) | LLLT and LAT were effective in reducing pain and increasing excursive and protrusive mandibular motion in TMD. p ≤ 0.05. |
| Brochado, F., et al., 2018 [64] | RCT. Impact of laser PBM on TMJ therapy | 51 pts. 3 groups: (i) PBM (n = 18). (ii) Manual MT (n = 16). (iii) Combined CT (n = 17). | 808 nm | Output: 100 mW CW, Spot size: 0.03 cm2, Fluence: 13.3 J/cm2 and 4 J per point | PBM was applied 12 times (3 times a week for 4 consecutive weeks). | All—↓ in pain and ↑ in jaw movements during treatment and at follow-up (<0.001). CT group sig. diff. in improvement (<0.001). |
| Rodrigues, C., et al., 2020 [65] | RCT. Impact of laser PBM on TMJ therapy | 78 pts. 3 groups: (i) 30—PBM (ii) 29—placebo PBM (iii) 19—control Random allocation | 780 nm | Masseter: 30 J/cm2–60 mW/20 s; the lateral pole of the TMJ (75 J/cm2–60 mW/50 s). | 8 Tx sessions. 2× week, Masseter 30 J/cm2–60 mW/20 s. TMJ 75 J/cm2 (60 mW/50 s), performed in 5 pts related to the lateral pole of the mandible head. Placebo HP used. | The active and placebo LLLT showed a reduction in pain during chewing and better recovery levels during the rest of the period (p > 0.05), without differences between OMC groups. |
| Aisaiti, A., et al., 2021 [66] | RCT. Impact of laser PBM on TMJ therapy | 100 pts. 4 groups: (i) 25 TMJ—PBM (ii) 25 Myalgia—PBM (iii) 25 placebo TMJ PBM (iv) 25 placebo myalgia Random allocation | 810 nm | Output power = 100 mW, 10 Hz. Spot dia = 2 cm, tip at 3 cm from tissue. Both sites: fluence: 6 J/cm2 | Masseter muscle: time per site = 20 s, total time = 60 s TMJ: time per point = 6 s, total time = 30 s. | PBMT: greater reduction in pain scores than placebo (p = 0.014). Myalgia: pain intensity decreased over time (p < 0.001); no difference between interventions (p = 0.074). |
| Monteiro, L., et al., 2020 [67] | RCT. Impact of laser PBM on TMJ therapy | 42 pts. 2 groups: (i) 22—PBM (ii) 20 Placebo Random allocation | 635 nm | Output: 200 mW CW. Spot: 0.5 cm2. PD: 400 mW/cm2. Exposure: 20 s. Fluence: 8 J/cm2. Radiant energy: 16 J/pt and 128 J on 4 sessions (av. 8 pts) | Contact mode. No points irradiated: 4 points per side. Area irradiated: 0.5 cm2 per point. Number and frequency of Tx 4 sessions (1 per week) | Pain: sig. reduction in laser group compared with baseline, p < 0.001. Pain during palpation of masticatory muscles was sig. Sig. increase in non-assisted painless mouth opening among laser group (p = 0.007). |
| Magri, L., et al., 2018 [68] | RCT. Impact of laser PBM on TMJ therapy | 64 pts. 3 groups: random (i) PBM laser (n = 20), (ii) placebo (n = 21), (iii) controls (without treatment (n = 23) | 780 nm | Masseter + temporal = 5 J/cm2 (20 mW–0.5 W/cm2), TMJ area = 7.5 J/cm2 (30 mW–0.8 W/cm2) | eight sessions, twice a week. | Laser group showed 80% pain reduction; placebo, 85%; and WT, 43% at 4 weeks. p < 0.05 |
| Dias, W., et al., 2022 [69] | RCT. Impact of laser PBM on TMJ therapy | 34 pts. 2 groups: (i) 17—OF myotherapy + PBM (ii) 17 OF myotherapy + placebo Random allocation | 830 nm | Two settings: (i) sessions #1–5: 6 J/fluence of 51 J/cm2, (ii) session #2: 4 J and fluence of 34 J/cm2, | First phase (#1–#5), to ease painful condition. Second phase (at the sixth session), to biostimulate functional gains | VAS OHQOL No sig. diff. (p ≥ 0.05) |
| Batra, S., et al., 2023 [70] | RCT. Impact of laser PBM on TMJ therapy | 20 pts. 2 groups: (i) 10—TMJDS + PBM (ii) 10—TMJDS + TENS Random allocation | 660 nm | Output: 100 mW CW. 6 J/ point | 60 s/pt, 2 sessions/week × 4 weeks On mass., temporalis, condylar, i-auricular regions | Pain VAS: diff. not statistically significant. Excursive movement: sig. diff. (p ≤ 0.05) |
| Borges, R., et al., 2018 [71] | RCT. Impact of laser PBM on TMJ therapy | 44 pts. 4 groups: (i) 11—8 J/cm2 (ii) 11—60 J/cm2 (iii) 11—105 J/cm2 (iv) 11—control placebo Random allocation | 830 nm | Output: 30 mW CW. Spot size: 0.116 cm2. Irradiation: 2.59 W/cm2. Fluence: J/cm2 (i–iii) 64 480 840. | Frequency of irradiation 3× week/10 sessions. 8 points (4 per side). | Study did not show effect of PBM over TMJ mobility. Results demonstrated sig. reductions in TMD pain and symptoms in all the PBM protocols used, including the placebo group. |
| Maracci, L., et al., 2022 [72] | RCT. Impact of laser PBM on TMJ therapy | 30 pts. 3 groups: (i) 11—splint (ii) 10—PBM (iii) 9—placebo Random allocation | 808 nm | Power: 100 mW, fluence of 80 J/cm2, 22 s per application, distance of 1 cm between each site. | T0: start of Tx. T1: 1 month after occlusal splint (G1) or 1 month after PBMT (G2) or placebo PBMT (G3). | VAS pain: G1 improvement (p = 0.014). G2 and G3, no sig. diff. OHRQoL, G1 + G2 sig. improvement (p = 0.005) cf. G3. |
| De Oliveira Chami, V., et al., 2022 [73] | RCT. Impact of laser PBM on TMJ therapy | 20 pts. 2 groups: (i) 10—laser group (LG) (ii) 10—placebo group (PG) Random allocation | 808 nm | Output: 100 mW, fluence: 80 J/cm2, 22 s per application, distance of 1 cm between each site. | T1: pre-PBM Tx; T2: after 1st PBM Tx; T3: before 2nd PBM Tx 48 h post 1st; T4: post 2nd Tx; T5: 7d post T2; T6: 30d post T1. | OHRQoL assessed at T1 and T6. Significant increase in mouth opening (p = 0.04) and improvement in QoL (p = 0.003) observed in the LG after 30 days. |
| Nadershah, M., et al., 2020 [74] | RCT. Impact of laser PBM on TMJ therapy | 202 pts. 2 groups: (i) 108—PBM group (ii) 94—placebo group Random allocation | 940 nm | Power: 7 W/2.8 cm2 Fluence: 300 J/cm2 Irradiance: 7 W/2.8 cm2 | E/O application, 2 min (24 s/appl. pt), 2 cm from skin, 5 points Every 48 h for 10 days | Sig. diff. pain—VAS (p = 0.01). |
| Mansourian, A., et al., 2019 [75] | RCT. Impact of laser PBM on TMJ therapy | 107 pts. 3 groups: (i) 35—PBM group (ii) 33—TENS (iii) 32—control group Random allocation | 810 nm | Power: 0.2 W Fluence: 2 J/cm2 | 10 s time and every week × 2 months. | Pain VAS: sig. diff. (p = 0.003). At 2 months, no sig. diff. found between the groups. (p = 0.38) |
| Desai, A., et al., 2022 [76] | RCT. Impact of laser PBM on TMJ therapy | 60 pts. 2 groups: (i) 30—placebo group (ii) 30—PBM group Random allocation | 633 nm | Power: 30 mW continuous wave. | 20 sessions of LLLT applied both in closed mouth and the maximum opened-mouth position, administered over a period of 08 weeks. | Pain VAS, mouth opening, lateral movement: better treatment outcome in PBM laser group but no sig. diffs. (p > 0.8). |
| Bakry, S., et al., 2021 [77] | RCT. Impact of laser PBM on TMJ therapy | 40 pts. 2 groups: (i) 20—PBM group (ii) 20—placebo group Random allocation | 635 nm | Power: 200 mW CW. Fluence: 5 Jcm2. | Applied at the height of the joint capsule with a mouth closed/opened position. 10 doses per joint. The total cycle dose was 100, and the cycle repeated for 10 days (every 2nd day). | One moth—VAS pain/opening—no sig. diff. Three months—sig. diff. from pre-operative state until post-operative state at three months (p ≤ 0.0001). |
| Emam, A., et al., 2023 [78] | RCT. Impact of laser PBM on TMJ therapy | 100 pts. 4 groups: (i) 25—behavioural therapy (BT). (ii) PBMT (LT) (iii) max. ant. Repos. splint (MARS). (iv) stabilisation splint (SS). | 808 nm | 70 mW and doses of 105 J/cm | 2/week for 4 weeks (total of 8 sessions). Admin. at 5 specific points on the TMJ, as well as the external acoustic canal. | MRM was evaluated for each patient before treatment and after 6 months (p < 0.05). There were significant improvements for SS and MARS on the different movements of MRM, more than those for LLLT and BT (p ≤ 0.05). |
| Modified Risk of Bias—TMJ (n = 20) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Citation | Randomisation | Sample Size Calc & Number Required | Blinding | Baseline Situation Similar for All Groups | Laser Parameters Complete/Calculations Correct | Optimal Fluence Applied | Power Meter Used | Numerical Results (Statistics) | No Missing Outcome Data | Correct Assessment of Results | Total |
| Ömer E et al. [59] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 7 |
| Ömer E et al. [60] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 7 |
| Chellappa D et al. [61] | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Yes | 8 |
| Shousha T et al. [62] | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | 7 |
| Madani A et al. [63] | Yes | No | Yes | Yes | Yes | No | No | Yes | Yes | Yes | 9 |
| Brochado F et al. [64] | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | 9 |
| Rodrigues C et al. [65] | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | 7 |
| Aisaiti A et al. [66] | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | 8 |
| Monteiro L et al. [67] | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | 9 |
| Magri L et al. [68] | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | 9 |
| Dias W et al. [69] | Yes | No | Yes | Yes | No | No | No | Yes | Yes | Yes | 6 |
| Batra S et al. [70] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 7 |
| Borges R et al. [71] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | 9 |
| Maracci L et al. [72] | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | 8 |
| De O Chami V et al. [73] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | 9 |
| Nadershah M et al. [74] | Yes | Yes | Yes | No | No | Yes | No | Yes | Yes | Yes | 7 |
| Mansourian A et al. [75] | Yes | No | Yes | No | No | No | No | Yes | Yes | Yes | 5 |
| Desai A et al. [76] | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Yes | 7 |
| Bakry S et al. [77] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 7 |
| Emam A et al. [78] | Yes | No | Yes | Yes | No | No | No | Yes | Yes | Yes | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parker, S.; Cronshaw, M.; Anagnostaki, E.; Mylona, V.; Lynch, E.; Grootveld, M. Effect of Photobiomodulation Therapy Dosage on Orthodontic Movement, Temporomandibular Dysfunction and Third Molar Surgery Outcomes: A Five-Year Systematic Review. Appl. Sci. 2024, 14, 3049. https://doi.org/10.3390/app14073049
Parker S, Cronshaw M, Anagnostaki E, Mylona V, Lynch E, Grootveld M. Effect of Photobiomodulation Therapy Dosage on Orthodontic Movement, Temporomandibular Dysfunction and Third Molar Surgery Outcomes: A Five-Year Systematic Review. Applied Sciences. 2024; 14(7):3049. https://doi.org/10.3390/app14073049
Chicago/Turabian StyleParker, Steven, Mark Cronshaw, Eugenia Anagnostaki, Valina Mylona, Edward Lynch, and Martin Grootveld. 2024. "Effect of Photobiomodulation Therapy Dosage on Orthodontic Movement, Temporomandibular Dysfunction and Third Molar Surgery Outcomes: A Five-Year Systematic Review" Applied Sciences 14, no. 7: 3049. https://doi.org/10.3390/app14073049
APA StyleParker, S., Cronshaw, M., Anagnostaki, E., Mylona, V., Lynch, E., & Grootveld, M. (2024). Effect of Photobiomodulation Therapy Dosage on Orthodontic Movement, Temporomandibular Dysfunction and Third Molar Surgery Outcomes: A Five-Year Systematic Review. Applied Sciences, 14(7), 3049. https://doi.org/10.3390/app14073049