
Ex Vivo Fusion Confocal Microscopy of Liver Biopsies: Diagnostic Pattern Identification and Correlation with Conventional Microscopy

 ,
,  , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Sample and Tissue Collection
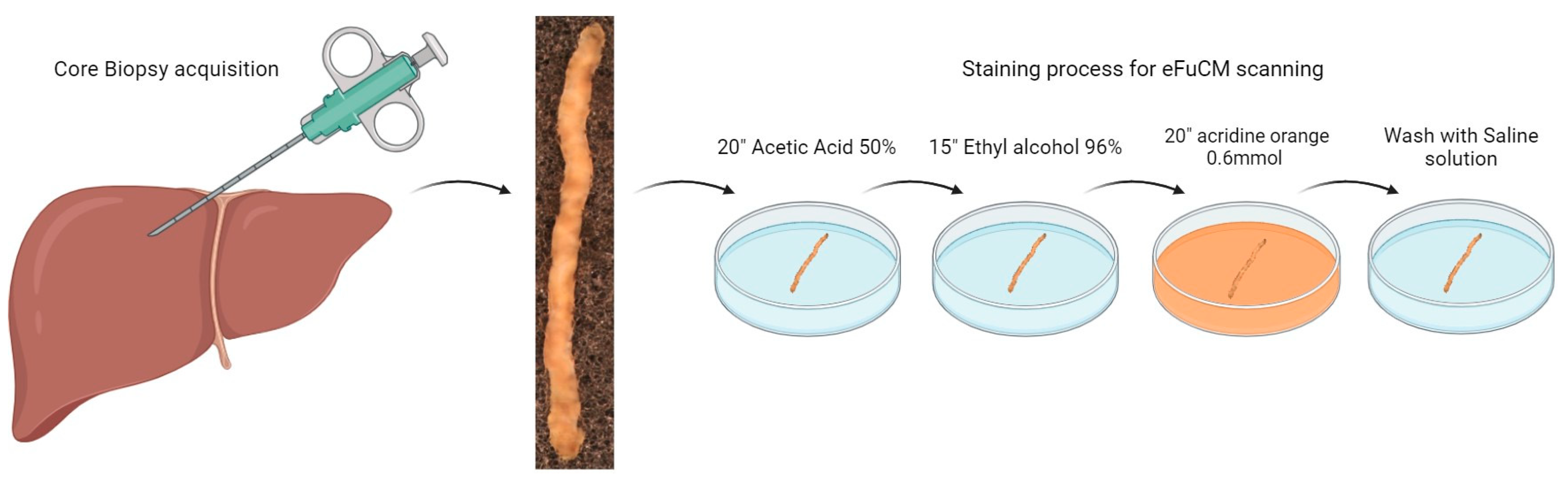
2.2. Ex Vivo Fusion Confocal Microscopy Sample Preparation and Image Acquisition
2.3. Formalin-Fixed Paraffin-Embedded Sample Analysis
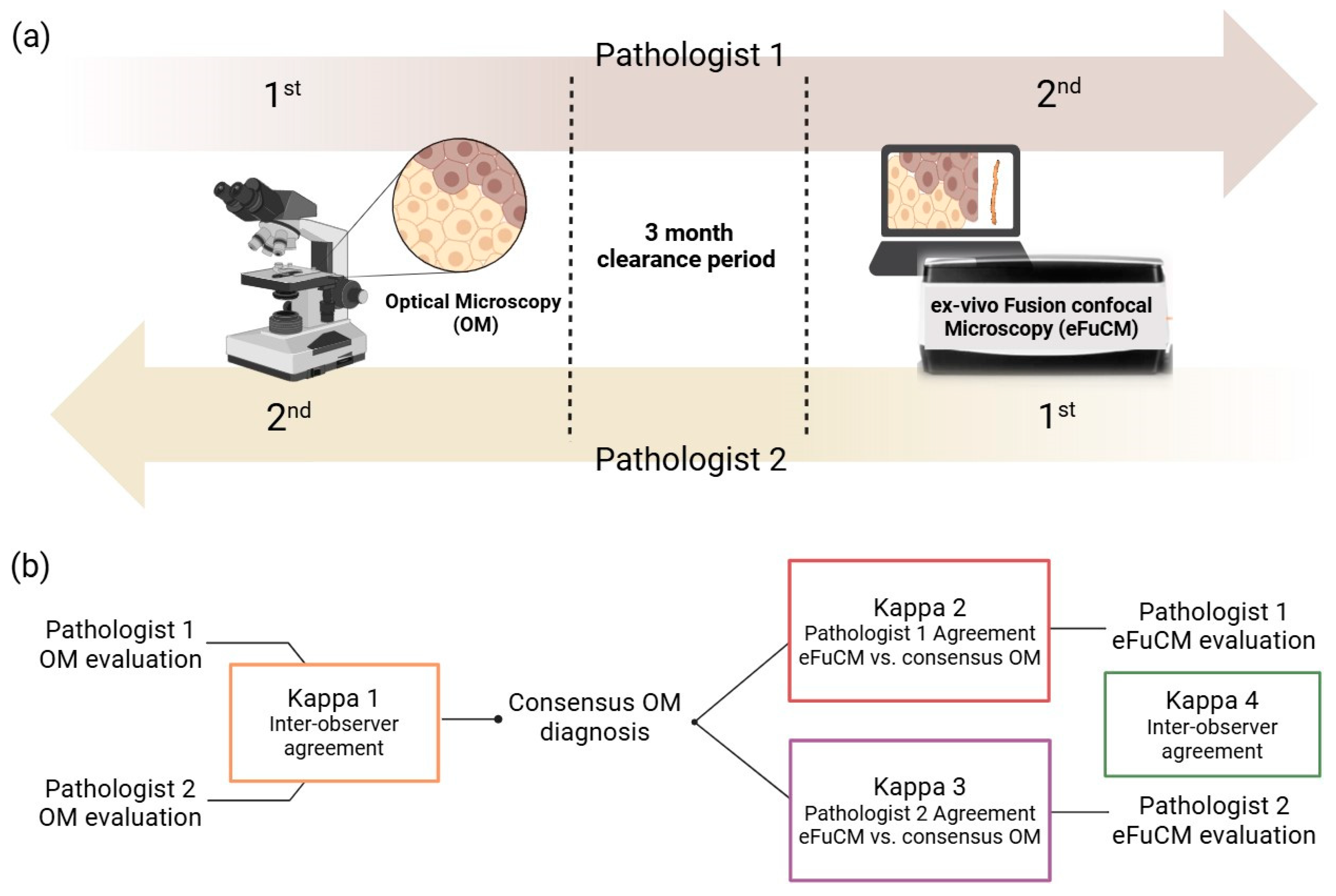
2.4. Image Evaluation
2.5. Statistical Analysis
3. Results
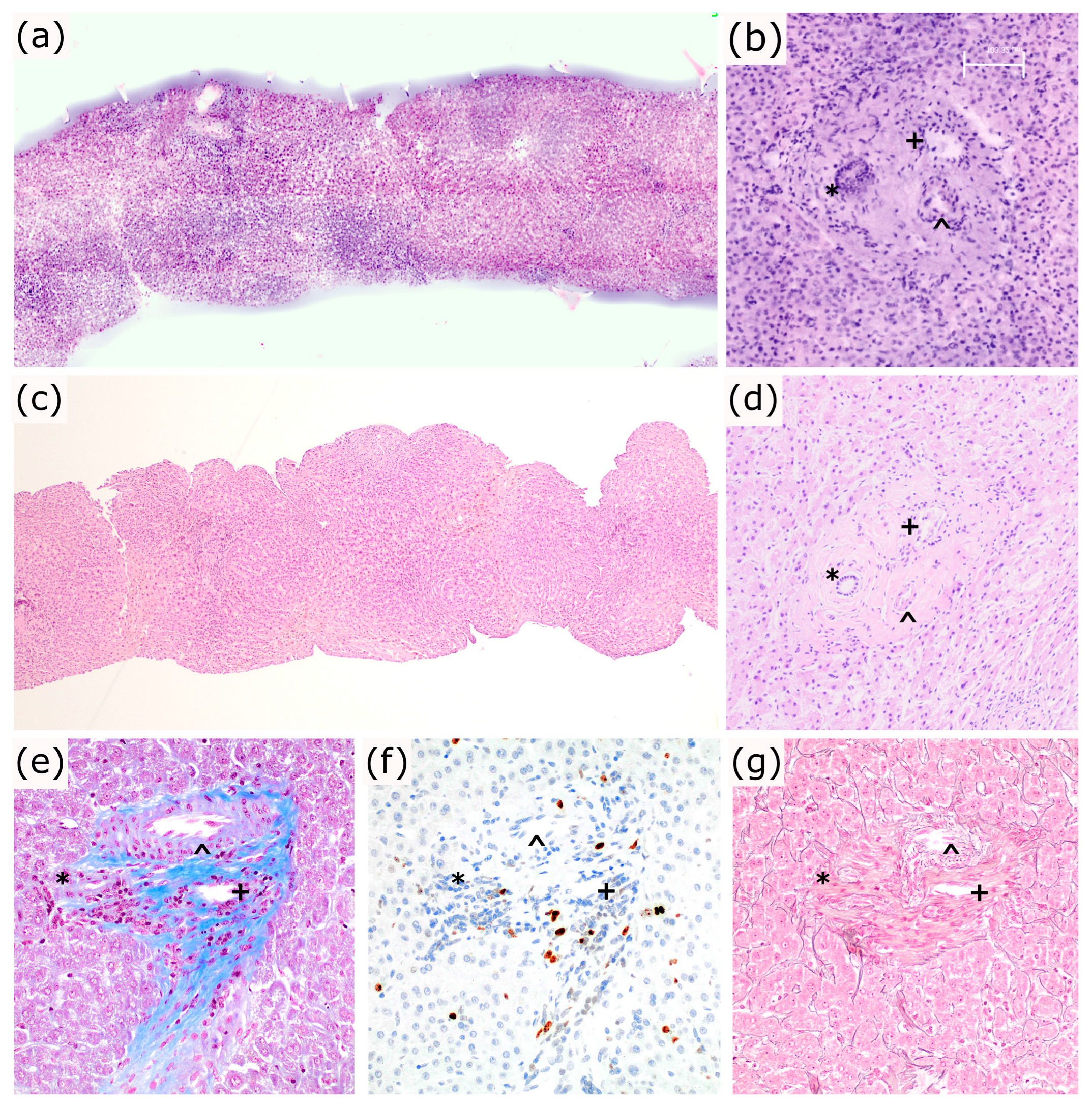
3.1. Characterization of Normal Liver Structures and Liver Tissue Integrity
3.2. Characterization of the Main Liver Pathological Features by Optical Microscopy
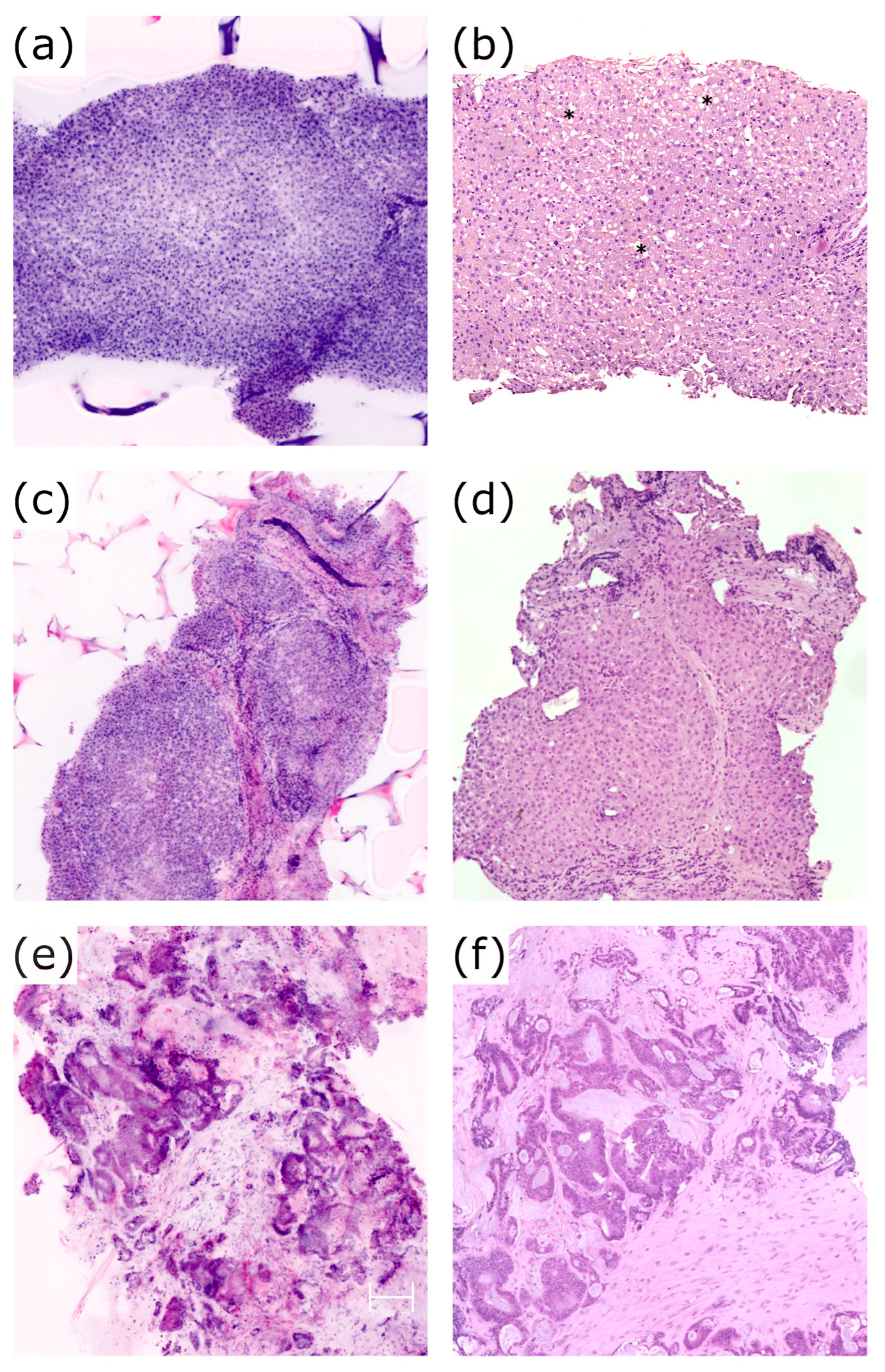
3.3. Reproducibility of Pathological Features and Patterns with eFuCM
3.4. Additional Findings
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Del Pilar, R.; Panqueva, L. Histopathological Evaluation of Liver Donors: An Approach to Intraoperative Consultation During Liver Transplantation. 2015. Available online: https://www.revistagastrocol.com/index.php/rcg/article/view/14/14 (accessed on 25 October 2024).
- Nackenhorst, M.C.; Kasiri, M.; Gollackner, B.; Regele, H. Ex Vivo Fluorescence Confocal Microscopy: Chances and Changes in the Analysis of Breast Tissue. Diagn. Pathol. 2022, 17, 55. [Google Scholar] [CrossRef]
- El-Bahrawy, M.; Ganesan, R. Frozen Section in Gynaecology: Uses and Limitations. Arch. Gynecol. Obstet. 2014, 289, 1165–1170. [Google Scholar] [CrossRef] [PubMed]
- Instant Digital Pathology Confocal Laser Scanning Microscopy ExVivo-with VivaScope® 2500. Available online: https://www.vivascope.com/instant-digital-pathology-ex-vivo/vivascope-2500-ex-vivo/ (accessed on 25 October 2024).
- Braunschweig, T.; Knüchel-Clarke, R. Editorial for: Bertoni et al. Ex Vivo Fluorescence Confocal Microscopy: Prostatic and Periprostatic Tissues Atlas and Evaluation of the Learning Curve. Virchows Archiv. 2020, 476, 487–488. [Google Scholar] [CrossRef]
- Pérez-Anker, J.; Ribero, S.; Yélamos, O.; García-Herrera, A.; Alos, L.; Alejo, B.; Combalia, M.; Moreno-Ramírez, D.; Malvehy, J.; Puig, S. Basal Cell Carcinoma Characterization Using Fusion Ex Vivo Confocal Microscopy: A Promising Change in Conventional Skin Histopathology. Br. J. Dermatol. 2020, 182, 468–476. [Google Scholar] [CrossRef]
- Pérez-Anker, J.; Puig, S.; Malvehy, J. A Fast and Effective Option for Tissue Flattening: Optimizing Time and Efficacy in Ex Vivo Confocal Microscopy. J. Am. Acad. Dermatol. 2020, 82, e157–e158. [Google Scholar] [CrossRef]
- Mathur, S.C.; Fitzmaurice, M.; Reder, N.P.; Krishnamurthy, S.; Kennedy, M.; Tearney, G.J.; Shevchuk-Chaban, M.M. Development of Functional Requirements for Ex Vivo Pathology Applications of In Vivo Microscopy Systems. Arch. Pathol. Lab. Med. 2019, 143, 1052–1057. [Google Scholar] [CrossRef]
- Malvehy, J.; Pérez-Anker, J.; Toll, A.; Pigem, R.; Garcia, A.; Alos, L.L.; Puig, S. Ex Vivo Confocal Microscopy: Revolution in Fast Pathology in Dermatology. Br. J. Dermatol. 2020, 183, 1011–1025. [Google Scholar] [CrossRef] [PubMed]
- Puliatti, S.; Bertoni, L.; Pirola, G.M.; Azzoni, P.; Bevilacqua, L.; Eissa, A.; Elsherbiny, A.; Sighinolfi, M.C.; Chester, J.; Kaleci, S.; et al. Ex Vivo Fluorescence Confocal Microscopy: The First Application for Real-Time Pathological Examination of Prostatic Tissue. BJU Int. 2019, 124, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Shavlokhova, V.; Flechtenmacher, C.; Sandhu, S.; Vollmer, M.; Vollmer, A.; Saravi, B.; Engel, M.; Ristow, O.; Hoffmann, J.; Freudlsperger, C. Ex Vivo Fluorescent Confocal Microscopy Images of Oral Mucosa: Tissue Atlas and Evaluation of the Learning Curve. J. Biophotonics 2022, 15, e202100225. [Google Scholar] [CrossRef]
- Dobbs, J.; Krishnamurthy, S.; Kyrish, M.; Benveniste, A.P.; Yang, W.; Richards-Kortum, R. Confocal Fluorescence Microscopy for Rapid Evaluation of Invasive Tumor Cellularity of Inflammatory Breast Carcinoma Core Needle Biopsies. Breast Cancer Res. Treat. 2015, 149, 303–310. [Google Scholar] [CrossRef]
- Villarreal, J.Z.; Pérez-Anker, J.; Puig, S.; Pellacani, G.; Solé, M.; Malvehy, J.; Quintana, L.F.; García-Herrera, A. Ex Vivo Confocal Microscopy Performs Real-Time Assessment of Renal Biopsy in Non-Neoplastic Diseases. J. Nephrol. 2020, 34, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Bertoni, L.; Azzoni, P.; Reggiani, C.; Pisciotta, A.; Carnevale, G.; Chester, J.; Kaleci, S.; Reggiani Bonetti, L.; Cesinaro, A.M.; Longo, C.; et al. Ex Vivo Fluorescence Confocal Microscopy for Intraoperative, Real-Time Diagnosis of Cutaneous Inflammatory Diseases: A Preliminary Study. Exp. Dermatol. 2018, 27, 1152–1159. [Google Scholar] [CrossRef]
- Shavlokhova, V.; Flechtenmacher, C.; Sandhu, S.; Vollmer, M.; Hoffmann, J.; Engel, M.; Ristow, O.; Freudlsperger, C. Features of Oral Squamous Cell Carcinoma in Ex Vivo Fluorescence Confocal Microscopy. Int. J. Dermatol. 2021, 60, 236–240. [Google Scholar] [CrossRef]
- Iovieno, A.; Longo, C.; De Luca, M.; Piana, S.; Fontana, L.; Ragazzi, M. Fluorescence Confocal Microscopy for Ex Vivo Diagnosis of Conjunctival Tumors: A Pilot Study. Am. J. Ophthalmol. 2016, 168, 207–216. [Google Scholar] [CrossRef]
- Forest, F.; Cinotti, E.; Yvorel, V.; Habougit, C.; Vassal, F.; Nuti, C.; Perrot, J.L.; Labeille, B.; Péoc’h, M. Ex Vivo Confocal Microscopy Imaging to Identify Tumor Tissue on Freshly Removed Brain Sample. J. Neurooncol 2015, 124, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthy, S.; Sabir, S.; Ban, K.; Wu, Y.; Sheth, R.; Tam, A.; Meric-Bernstam, F.; Shaw, K.; Mills, G.; Bassett, R.; et al. Comparison of Real-Time Fluorescence Confocal Digital Microscopy With Hematoxylin-Eosin–Stained Sections of Core-Needle Biopsy Specimens. JAMA Netw. Open 2020, 3, e200476. [Google Scholar] [CrossRef] [PubMed]
- Kinzler, M.N.; Schulze, F.; Reitz, A.; Gretser, S.; Ziegler, P.; Shmorhun, O.; Friedrich-Rust, M.; Bojunga, J.; Zeuzem, S.; Schnitzbauer, A.A.; et al. Fluorescence Confocal Microscopy on Liver Specimens for Full Digitization of Transplant Pathology. Liver Transplant. 2023, 29, 940–951. [Google Scholar] [CrossRef]
- Krishnamurthy, S.; Cortes, A.; Lopez, M.; Wallace, M.; Sabir, S.; Shaw, K.; Mills, G. Ex Vivo Confocal Fluorescence Microscopy for Rapid Evaluation of Tissues in Surgical Pathology Practice. Arch. Pathol. Lab. Med. 2018, 142, 396–401. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.-C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and Validation of a Histological Scoring System for Nonalcoholic Fatty Liver Disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Villarreal, J.Z.; Pérez-Anker, J.; Puig, S.; Xipell, M.; Espinosa, G.; Barnadas, E.; Larque, A.B.; Malvehy, J.; Cervera, R.; Pereira, A.; et al. Ex Vivo Confocal Microscopy Detects Basic Patterns of Acute and Chronic Lesions Using Fresh Kidney Samples. Clin. Kidney J. 2023, 16, 1005–1013. [Google Scholar] [CrossRef] [PubMed]
- Titze, U.; Sievert, K.D.; Titze, B.; Schulz, B.; Schlieker, H.; Madarasz, Z.; Weise, C.; Hansen, T. Ex Vivo Fluorescence Confocal Microscopy in Specimens of the Liver: A Proof-of-Concept Study. Cancers 2022, 14, 590. [Google Scholar] [CrossRef] [PubMed]
- Marenco, J.; Calatrava, A.; Casanova, J.; Claps, F.; Mascaros, J.; Wong, A.; Barrios, M.; Martin, I.; Rubio, J. Evaluation of Fluorescent Confocal Microscopy for Intraoperative Analysis of Prostate Biopsy Cores. Eur. Urol. Focus 2021, 7, 1254–1259. [Google Scholar] [CrossRef]
- Sievert, K.D.; Hansen, T.; Titze, B.; Schulz, B.; Omran, A.; Brockkötter, L.; Gunnemann, A.; Titze, U. Ex Vivo Fluorescence Confocal Microscopy (FCM) of Prostate Biopsies Rethought: Opportunities of Intraoperative Examinations of MRI-Guided Targeted Biopsies in Routine Diagnostics. Diagnostics 2022, 12, 1146. [Google Scholar] [CrossRef]
- Guerrero, J.A.; Pérez-Anker, J.; Fernández-Esparrach, G.; Archilla, I.; Diaz, A.; Lopez-Prades, S.; Rodrigo-Calvo, M.; Lahoz, S.; Camps, J.; Puig, S.; et al. Ex Vivo Fusion Confocal Microscopy of Colorectal Polyps: A Fast Turnaround Time of Pathological Diagnosis. Pathobiology 2021, 88, 392–399. [Google Scholar] [CrossRef]
- Bishop, K.W.; Maitland, K.C.; Rajadhyaksha, M.; Liu, J.T.C. In Vivo Microscopy as an Adjunctive Tool to Guide Detection, Diagnosis, and Treatment. J. Biomed. Opt. 2022, 27, 040601. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Number | Surgical Specimen Type | Indication | Final Diagnosis |
|---|---|---|---|
| 1 | Total hepatectomy | ALD-related cirrhosis (transplantation) | Cirrhosis with grade 1 steatosis and bilirrubinostasis |
| 2 | Total hepatectomy | DILI (Anakinra)-related acute liver failure (transplantation) | Acute hepatitis, necroinflammatory + cholestatic pattern, with submassive hepatic necrosis |
| 3 | Total hepatectomy | Discarded donor liver | Moderate sinusoidal dilatation |
| 4 | Total hepatectomy | MASLD-related cirrhosis with HCC (transplantation) | 1.6 cm HCC Cirrhosis with grade 1 steatosis |
| 5 | Partial hepatectomy | ICC on HCV-related cirrhosis | 4.8 cm ICC. Advanced fibrosis (F3) without necroinflammatory activity |
| 6 | Total hepatectomy | AIH-related cirrhosis (transplantation) | Cirrhosis with moderate necroinflammatory activity, plasma cells and bilirrubinostasis |
| 7 | Partial hepatectomy | ICC in a MASLD-related cirrhosis | 2.7 cm ICC Cirrhosis with grade 1 steatosis |
| 8 | Total hepatectomy | ALD-related cirrhosis (transplantation) | Inactive cirrhosis |
| 9 | Partial hepatectomy | ICC on a steatotic liver | 6.9 cm ICC. Grade 1 steatosis |
| 10 | Total hepatectomy | DILI vs. AIH related acute liver failure (transplantation) | Acute hepatitis, necroinflammatory pattern with bridging confluent necrosis |
| 11 | Partial hepatectomy | ICC on HCV-related cirrhosis | 1.8 cm ICC. Inactive cirrhosis |
| 12 | Partial hepatectomy | HCC on HCV-related cirrhosis. | 1.7 cm HCC Inactive cirrhosis |
| 13 | Total hepatectomy | HBV-related cirrhosis with HCC (transplantation) | 3 and 1.3 cm HCC. Cirrhosis with slight necroinflammatory activity |
| 14 | Partial hepatectomy | Complex liver mass | 5.2 cm mature cystic teratoma Grade 1 steatosis |
| 15 | Partial hepatectomy | Left lobe mass in a MASLD-related cirrhosis | 1.6 cm ICC Cirrhosis with grade 3 steatosis |
| 16 | Partial hepatectomy | HCC on a HBV and enol related cirrhosis | 4.6 cm HCC. Advanced fibrosis (F3), without necroinflammatory activity |
| 17 † | Partial hepatectomy | Right lobe mass on HCV chronic hepatitis | 5 cm HCC. Advanced fibrosis (F3), without necroinflammatory activity |
| 18 † | Partial hepatectomy | Right lobe mass on HCV chronic hepatitis | 5 cm HCC. Advanced fibrosis (F3), without necroinflammatory activity |
| 19 | Total hepatectomy | MetALD-related cirrhosis with HCC (transplantation) | Multifocal HCC Inactive cirrhosis |
| 20 | Partial hepatectomy | CRC metastasis | 3.6 cm CRC metastasis. Grade 1 steatosis |
| 21 | Total hepatectomy | ALD-related cirrhosis with ablated HCC (transplantation) | 3.5 and 2.2 necrotic lesions (treated HCC). Cirrhosis with slight necroinflammatory activity |
| 22 | Total hepatectomy | Hepatorenal polycystic disease (transplantation) | Polycystic liver |
| 23 | Total hepatectomy | AIH-related acute liver failure (transplantation) | Acute hepatitis, necroinflammatory pattern, with submassive hepatic necrosis |
| Part I | |||||||
| Pathologist 1, n | Observed Agreement | Kappa 1 | Agreement | ||||
| Pathologist 2, n | Yes | No | |||||
| Fibrotic septa | 91.3% | 0.777 | Substantial | ||||
| Yes | 16 | 0 | |||||
| No | 2 | 5 | |||||
| Cirrhosis | 100.0% | 1.000 | Perfect | ||||
| Yes | 11 | 0 | |||||
| No | 0 | 12 | |||||
| Septal inflammation | 95.7% | 0.893 | Almost perfect | ||||
| Yes | 16 | 1 | |||||
| No | 0 | 6 | |||||
| Lobular inflammation | 82.6% | 0.553 | Moderate | ||||
| Yes | 4 | 3 | |||||
| No | 1 | 15 | |||||
| Steatosis | 95.7% | 0.881 | Almost perfect | ||||
| Yes | 5 | 0 | |||||
| No | 1 | 17 | |||||
| Tumor | 100.0% | 1.000 | Perfect | ||||
| Yes | 2 | 0 | |||||
| No | 0 | 21 | |||||
| Part II | |||||||
| Pathologist 2, n | Pathologist 1, n | Observed Agreement | Kappa 1 | Agreement | |||
| Grade of portal inflammation | No | Mild | Moderate | Severe | 84.5% | 0.669 | Substantial |
| No | 4 | 1 | 0 | 0 | |||
| Mild | 2 | 14 | 0 | 0 | |||
| Moderate | 0 | 2 | 0 | 0 | |||
| Severe | 0 | 0 | 0 | 0 | |||
| Grade of lobular inflammation | No | Mild | Moderate | Severe | 73.9% | 0.378 | Fair |
| No | 15 | 1 | 0 | 0 | |||
| Mild | 3 | 1 | 0 | 0 | |||
| Moderate | 0 | 1 | 0 | 0 | |||
| Severe | 0 | 1 | 0 | 1 | |||
| Grade of steatosis | No | Mild | Moderate | Severe | 95.7% | 0.881 | Almost perfect |
| No | 17 | 1 | 0 | 0 | |||
| Mild | 0 | 5 | 0 | 0 | |||
| Moderate | 0 | 0 | 0 | 0 | |||
| Severe | 0 | 0 | 0 | 0 | |||
| Histopathological Features | Pathologist 1 with No eFuCM Experience (Kappa 2) | Pathologist 2 with eFuCM Experience (Kappa 3) |
|---|---|---|
| Fibrotic septa | 0.597 | 0.838 |
| Cirrhosis | 0.667 | 0.840 |
| Portal inflammation | 0.597 | 0.565 |
| Grade of portal inflammation | 0.233 | 0.497 |
| Lobular inflammation | 0.247 | 0.802 |
| Grade of lobular inflammation | 0.158 | 0.492 |
| Steatosis | 0.519 | 0.750 |
| Grade of steatosis | 0.519 | 0.603 |
| Tumor | 0.779 | 0.834 |
| Histopathological Patterns | Pathologist 1 with No eFuCM Experience (Kappa 2) | Pathologist 2 with eFuCM Experience (Kappa 3) |
|---|---|---|
| Normal or minimal changes | 0.467 | 1 |
| Steatosis | 0.679 | 1 |
| Acute hepatitis | 0.834 | 0.603 |
| Chronic hepatitis | 0.834 | 1 |
| Tumor | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopez-Prades, S.; Fuster-Anglada, C.; Millán, R.; Ferrer-Fàbrega, J.; Bassegoda, O.; Boix, L.; Cuatrecasas, M.; Díaz, A. Ex Vivo Fusion Confocal Microscopy of Liver Biopsies: Diagnostic Pattern Identification and Correlation with Conventional Microscopy. Appl. Sci. 2024, 14, 11121. https://doi.org/10.3390/app142311121
Lopez-Prades S, Fuster-Anglada C, Millán R, Ferrer-Fàbrega J, Bassegoda O, Boix L, Cuatrecasas M, Díaz A. Ex Vivo Fusion Confocal Microscopy of Liver Biopsies: Diagnostic Pattern Identification and Correlation with Conventional Microscopy. Applied Sciences. 2024; 14(23):11121. https://doi.org/10.3390/app142311121
Chicago/Turabian StyleLopez-Prades, Sandra, Carla Fuster-Anglada, Rosana Millán, Joana Ferrer-Fàbrega, Octavi Bassegoda, Loreto Boix, Miriam Cuatrecasas, and Alba Díaz. 2024. "Ex Vivo Fusion Confocal Microscopy of Liver Biopsies: Diagnostic Pattern Identification and Correlation with Conventional Microscopy" Applied Sciences 14, no. 23: 11121. https://doi.org/10.3390/app142311121
APA StyleLopez-Prades, S., Fuster-Anglada, C., Millán, R., Ferrer-Fàbrega, J., Bassegoda, O., Boix, L., Cuatrecasas, M., & Díaz, A. (2024). Ex Vivo Fusion Confocal Microscopy of Liver Biopsies: Diagnostic Pattern Identification and Correlation with Conventional Microscopy. Applied Sciences, 14(23), 11121. https://doi.org/10.3390/app142311121