Abstract
In the process of orthodontic treatment, root parallelism is related to the relapse of extraction spaces, black triangles, and periodontal health. However, there are few studies on root parallelism in extraction cases with different types of appliances. The objective was to compare the root parallelism in extraction cases treated with clear aligners vs. those treated with fixed appliances by measuring the differences per extraction site and to access the root-movement control capacity of both orthodontic appliances. A retrospective study was conducted on cases in which the first premolars were extracted, treated by clear aligner appliance (“Invisalign” system, 28 patients) or fixed appliance (30 patients). The angulations of the tooth axis (canines, the second premolars, the first molars, and the second molars) were measured to analyze and compare the difference in root parallelism between the two orthodontic appliances. The percentage of root parallelism between the canine and second premolar in both groups had no significant difference. However, judging from the average angle difference value, the fixed appliance might have a greater range in root angulation adjustment than the aligner. In the angulation categories, the aligner mainly showed root apical divergence, while the fixed appliance mainly showed root apical convergence. The dental crown of the molars was mainly non-tipping in both groups, but it could be observed that the dental crown of the maxillary molars had a tendency toward mesial inclination. In conclusion, the same root parallelism and root inclination were obtained in tooth extraction cases whether treated by clear aligners or fixed appliances. This study provides clinicians with more information on the performance of clear aligners and fixed appliances.
1. Introduction
The control and adjustment of the axial inclinations of teeth is a critical step during orthodontic treatment, which may influence the patient’s dental aesthetics and even mental health [1]. Especially in extraction therapy, root axial inclinations are typically evaluated after space closure to ensure that adequate parallelism of roots has been achieved [2]. This is because proper root parallelism is beneficial to obtain a functional, stable, and esthetically pleasing occlusion [2]. In addition, it is also beneficial for long-term periodontal health and is therefore important to ensure a good prognosis for treatment [3,4].
Clear aligner treatment has prominent advantages (e.g., beauty and comfort) and is increasingly favored by both orthodontists and patients [5]. Although previous studies have compared fixed appliances with clear aligners, regarding periodontal biofilm [6], treatment outcomes, and treatment time [7], the performance of both appliances in terms of root parallelism control at the extraction sites is largely unknown. Initially, the clear aligner appliance was mostly used for the correction of non-tooth extraction cases [8,9]. With the innovation of digitization, materials, and systems, it is now gradually being applied in tooth extraction cases or even more complex cases. However, for the efficacy of clear aligner treatment in tooth extraction cases, the previous literature has focused on successful individual cases [10,11,12,13].
To compare the efficacy of the clear aligner appliance and the fixed appliance, most of the literature has reported non-tooth extraction cases [11,14,15,16]. Relatively few comparative studies investigated the effect of the case of tooth extraction. In addition, even fewer studies have reported the adjustment and control of root parallelism in these two orthodontic appliances. For example, Baldwin et al. [17] reported a trend for greater tipping of mandibular teeth into the extraction space and around the second premolar extraction sites during treatment with aligners. Weihong et al. [18] concluded that the objective grading system (OGS) scores were similar between the aligner group and the braces group for root angulation. This indicates that contradictions exist with regard to tooth inclination.
Therefore, a retrospective study was conducted to compare the root parallelism in extraction cases treated with clear aligners vs. those treated with fixed appliances by measuring the differences per extraction site and to assess the root-movement control capacity of both orthodontic appliances. Here, the null hypothesis was that fixed appliances and clear aligners have the same performance on root-movement control.
2. Materials and Methods
The patients were randomly and retrospectively selected from the files of the Department of Orthodontics, West China Hospital of Stomatology, Sichuan University, who completed orthodontic treatment from October 2010 to September 2018; all the treatments were performed by orthodontists of the same seniority. Ethical approvement for this study was acquired from the Ethical Committee of the West China Hospital of Stomatology, Sichuan University (WCHSIRB-D-2022-347).
2.1. Inclusion Criteria
- The subjects were adults with Class I or Class II malocclusion requiring first premolar extraction treatment (not necessarily symmetrical in both arches).
- All extraction spaces were completely closed.
- After treatment, there was a satisfactory dental alignment, occlusal relation, and facial profile.
2.2. Exclusion Criteria
- Periodontal surgery in the extraction area.
- Any refinement adjustment under the guidance of panoramic X-rays or other aspects.
- Dental anomalies of number (agenesis or supernumerary teeth).
- Systemic diseases.
2.3. Grouping
Group I: The aligner (“Invisalign” system) group included 28 patients (3 male, 25 female) who had at least one first premolar extracted; the attachments on the premolars and molars were followed by the “Invisalign G6” system. In 13 cases, 1–3 first premolars were extracted, and 4 first premolars were extracted in the remaining cases; there were 85 extraction sites in total. The mean age at the beginning of treatment was 25.89 ± 5.93 years (range, 18–35 years).
Group II: The fixed appliance group (0.022 × 0.028-inches, Damon, Ormco, Orange, Calif) included 30 patients (3 male, 27 female) who had 4 first premolars extracted (with 120 extraction sites). The mean age at the beginning of treatment was 23.43 ± 3.80 years (range, 18–31 years). The fixed appliances used the metal self-locking groove system (0.022 × 0.028 in fixed standard edgewise appliances, 3M company), aligning and leveling the dentition followed by 0.016, 0.018, and 0.018 × 0.025 in Nitinol, then 0.019 × 0.025 stainless steel arch wires, which closed the extraction spaces by sliding the wire.
3. Method of Measurement:
Panoramic radiographs of the patients before and after orthodontic treatment (taken by the same machine) were collected and measured blindly in a picture archiving and communication system (PACS system). The measurement of tooth angulation involved the canines, second premolar, first molar, and second molar.
The maxillary reference line was drawn, connecting the lowest points of the orbital rims, and the mandibular reference lines were the tangent lines of the mandibular margin on both sides [17,19,20]. The root axes of these teeth were drawn connecting the midpoint of the mesiodistal diameter of the dental crown along the root canal path or root bifurcation (Figure 1).
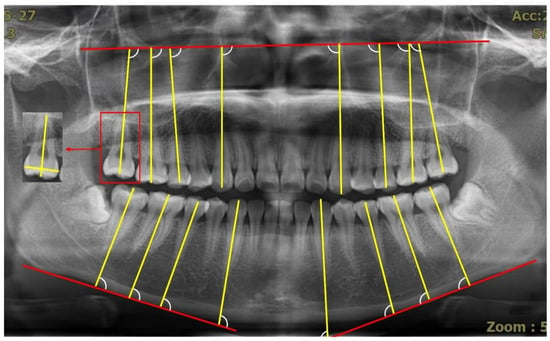
Figure 1.
Measurement of the root axes. The red box shows the determination of the long axis of the posterior tooth); the mesial angle between the long axis of the tooth and the reference line is the angulation of these teeth (canines, second premolars, first molars, and second molars).
The angle of each target tooth was measured and collected, and the mesial angle between the long axis of the tooth and the reference line is shown in Figure 1. t3, t5, t6, and t7 indicated the pretreatment angulation of the canines, second premolars, first molars, and second molars, respectively. In addition, T3, T5, T6, and T7 referred to the post-treatment angulation of the aforementioned teeth, respectively. All the measurements were conducted by the same operator twice after a three-week interval; satisfactory consistency was achieved between this interval, and the average values were calculated as the final results.
The t3–t5 angulation indicated the absolute values of the angulation of the canines minus the angulation of the second premolars in pretreatment, while the T3–T5 angulation indicated the same in post-treatment, and the angle difference value indicated the absolute values of the t3–t5 angulation minus the T3–T5 angulation.
In general, for the difference in T3–T5, the satisfactory parallelism ranges from −6° to +6°; it is called apical convergence if it is less than −7° or apical divergence if more than 7° [21]. If the difference value in t6–T6 and t7–T7 are below −7°, the dental crown of the molars can be considered distal tipping; on the contrary, the dental crown of the molar is mesial tipping, if it is more than 7°, and if it is between −7° and 7°, the tooth axis is assumed to be non-tipping. To ensure the two treatment methods were comparable, the aligner and fixed groups were divided into two subgroups of parallelism (P1) and nonparallelism (NP1), according to the absolute value of the t3–t5 angulation (7°) before treatment. Moreover, they were divided into another two subgroups of parallelism (P2) and nonparallelism (NP2), according to the absolute value of the T3–T5 angulation (7°) after treatment.
Statistical Analysis
An independent t-test was used to compare the difference in the post-treatment angulation of the canines and the second premolars between the aligner and fixed appliance groups. The chi-square test was used to compare the difference in the root-angulation categories of canines and the second premolars between groups. The independent t-test and chi-square test were also used to compare the difference in the angulation changes of the first and second molars between the aligner and fixed appliance groups.
4. Results
For the subgroup P1, there was no statistically significant difference in the T3–T5 angulation and angle difference value between the aligner and fixed groups (Table 1). In addition, no significant difference was found in the percentage of the root parallelism of the canine and second premolar after treatment (p = 0.191, Table 2). This indicated that the teeth on both sides of the extraction space remained parallel after orthodontic treatment for the cases with parallel roots, independent of whether a clear aligner or fixed appliance was used. For subgroup NP1, no statistically significant difference was found in the T3–T5 angulation and the percentage of root parallelism between the aligner and fixed appliance groups. However, the angle difference value showed a statistically significant difference. This indicated that the same treatment outcome was obtained by both appliances for cases with nonparallel roots, but judging from the average angle difference value (aligner 7.00° ± 5.30°; fixed 10.81° ± 9.16°), the fixed appliance might have a larger range in root angulation adjustment than the aligner (Table 1 and Table 2).

Table 1.
Comparison of the angulation between the canine and second premolar in pretreatment and post-treatment (independent t-test).
Table 2.
Comparison of the root-parallelism percentages between the canine and the second premolar after treatment (chi-square test).
Table 3 showed the root-angulation categories of the canines and second premolars after the treatment between the aligner and fixed appliance groups. With regard to satisfactory parallelism (SP), no difference was found between the two groups. However, there was a significant difference between the two groups with regard to nonparallel angulation. As displayed in Figure 2, the aligner group mainly showed apical divergence (AD), while the fixed group mainly showed apical convergence (AC).
Table 3.
Comparison of the difference in the root-angulation categories of the canines and the second premolars after treatment (chi-square test).
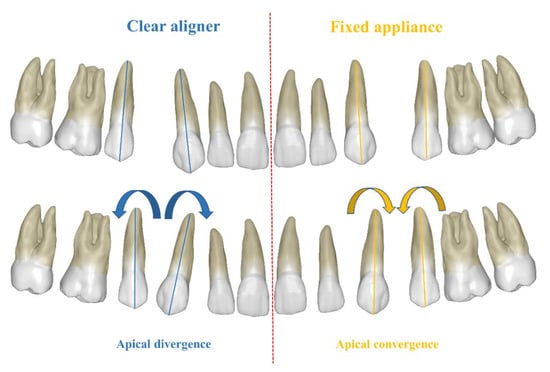
Figure 2.
Root-angulation categories of canines and second premolars after treatment between the aligner and fixed appliance with regard to nonparallel angulation. The aligner mainly showed apical divergence (AD), while the fixed appliance mainly showed apical convergence (AC).
Table 4 and Table 5 showed no significant difference between the aligner and the fixed groups in the angulation changes of the upper first molar, the upper second molar, and the lower first molar. However, a significant difference was found between the aligner and fixed groups in the angulation changes of the lower second molar. For the maxillary first and second molars, regardless of whether clear aligner treatment or fixed appliance treatment were used, non-tipping and mesial tipping accounted for the vast majority, which indicated that the dental crown of the maxillary molars had a tendency toward mesial inclination. In comparison, the mandibular first molars mainly showed non-tipping and distal tipping for both appliances, and the mandibular second molars mainly showed non-tipping in the clear aligner treatment, while they showed non-tipping and distal tipping in the fixed appliance treatment (Table 6).
Table 4.
Comparison of the angulation changes in the upper first and second molars pretreatment and post-treatment (independent t-test).
Table 5.
Comparison of the angulation changes in the lower first and second molars pretreatment and post-treatment (independent t-test).
Table 6.
Comparison of the root-tipping direction of the first molar and the second molar from pretreatment to post-treatment (Chi-square test).
5. Discussion
The objectives of this study were to compare the root parallelism of the teeth on both sides of the tooth extraction space and the posterior teeth in extraction cases treated with clear aligners vs. fixed appliances by measuring the differences per extraction site and to assess the root-movement control capacity of both orthodontic appliances. The same root parallelism was obtained by both appliances for cases with parallel roots or nonparallel roots. This result was different from the results reported by Baldwin et al. [17] and Womack et al. [11] who reported a trend for increased tipping of the teeth into the extraction space during treatment with aligners, especially in the cases of second premolar extraction. However, the results of the present study matched those reported by Weihong et al. [18] that both the “Invisalign” appliance and fixed appliance achieved good root angulation. This result may be attributed to the innovation in the “Invisalign” system, supported by big data and the improvement in the aligner materials. In addition, judging from the average angle difference (aligner 7.00° ± 5.30°; fixed 10.81° ± 9.16°), the fixed appliance might have a greater range in root angulation adjustment than the aligner, which was basically consistent with the conclusion of a systematic evaluation from Jiafeng et al. [22], who reported the likelihood of achieving “great improvement” in a malocclusion with fixed appliances. Nevertheless, since, the root control performance of clear aligner and fixed appliances remains controversial, we believe that further studies (for example, research on the mechanical properties of materials and 3D printing) are needed to verify the root-movement control capacity of both orthodontic appliances.
The categories of the nonparallel angulation of the root on both sides of the tooth extraction space after treatment with an aligner and a fixed appliance were different: the former mainly showed root apical divergence, while the latter mainly showed root apical convergence. Lack of root parallelism has long been reported as a possible factor for the relapse of extraction spaces [21]. The nonparallel root can lead to an uneven distribution of the bone between the roots. If the distance of the root apical is too large (root apical divergence), the interproximal contacts can move toward the crown, possibly resulting in a black triangle, which is not only unaesthetic but also easily leads to food impaction and thus affects periodontal health [23,24]. Furthermore, if the distance of the root apical was too small (root apical convergence), i.e., a width of bone and tissue < 0.8 mm, it easily causes the risk of periodontitis [25]. Therefore, it is very important to control the root parallelism with an orthodontic system. A clear aligner appliance, which mainly showed root apical convergence, may be prone to relapse, and this inference is consistent with the results of Kuncio et al. [15]. This indicates the necessity to analyze root parallelism near the tooth extraction side before finishing the clear aligner appliance treatment, to guide the axial inclination adjustment of the teeth in refinement.
To avoid the influence of measurement error, we set the angulation change outside this range (between −7° and 7°) to be considered as effective tipping change. The results of this study showed that the dental crown of the maxillary molars had a tendency of mesial tipping after treatment with either appliance. This phenomenon may be caused by the blocking of the maxillary bone structure, the loss of anchorage, and the contraction–deformation of aligner, which is consistent with clinical observations. However, the dental crown of the mandibular first molars had a tendency toward distal tipping after treatment with either appliance. The dental crown of the mandibular second molars showed no obvious tipping change after clear aligner treatment, while it showed a tendency toward distal tipping after fixed appliance treatment. Comparing the mean value of the angulation changes, the difference was statistically significant between the clear aligner and the fixed appliance. In the treatment of class I and class II cases, when close to the tooth extraction spaces, the mandibular molar may need more mesial movement, while the root movement of the mandibular molars was more obvious than the crown due to the pull of the supra-alveolar fibers. This may explain why the mandibular molars likely tended toward distal inclination. Overall, the clear aligner requires both effective attachments and completed aligner coverage to load the orthodontic forces that can be calculated and designed by computer. It is possible that the inclination change in the posterior teeth by the clear aligner will be able to be avoided in the near future.
One of the limitations in our study was that cephalometric analysis data were not added into our research, which may have assisted with the location of the reference line. Another limitation was that we did not take certain factors into consideration, for example, the attachments on the premolars and molars, the biocompatibility of different appliances [26], and the self-perception and cooperation of patients during orthodontic treatment [27,28]. Moreover, future studies on root parallelism control could focus on symmetrical tooth extraction, as well as some special orthodontic patients.
Based on the results of our study, the null hypothesis can be accepted. However, judging from the average angle difference, the fixed appliance might have a greater range in root angulation adjustment than the aligner.
6. Conclusions
- A similar root parallelism of the canine and second premolar was obtained in tooth extraction cases after treatment by either clear aligners or fixed appliances; however, judging from the average angle difference, the fixed appliance might have a greater range in root angulation adjustment than the aligner.
- For the categories of the nonparallel angulation of the root on both sides of the tooth extraction space after treatment, the clear aligner appliance mainly showed root apical divergence, while the fixed appliance mainly showed root apical convergence.
- The dental crown of the molars was mainly non-tipping in both groups; however, the dental crown of maxillary molars had a tendency toward mesial inclination.
Author Contributions
Conceptualization, H.L. (Hu Long), T.T., and W.L.; methodology, H.L. (Hu Long) and T.T.; formal analysis, T.T., H.L. (Hengyan Liang), X.Y., Q.F., Q.J., F.J., and W.L.; investigation, T.T., H.L. (Hengyan Liang), and W.L.; resources, H.L. (Hengyan Liang); data curation, T.T., H.L. (Hengyan Liang), X.Y., Q.F., Q.J., and F.J.; writing—original draft, T.T.; writing—review and editing, T.T.; supervision, T.T.; project administration, H.L. (Hu Long); funding acquisition, H.L. (Hu Long) and W.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by National Natural Science Foundation of China, grant number (NSFC, No.81400549) And The APC was funded by Orthodontic National Key Clinical Specialty Construction Program of China, West China Hospital of Stomatology, Sichuan University.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chrapla, P.; Paradowska-Stolarz, A.; Skoskiewicz-Malinowska, K. Subjective and Objective Evaluation of the Symmetry of Maxillary Incisors among Residents of Southwest Poland. Symmetry 2022, 14, 1257. [Google Scholar] [CrossRef]
- Shroff, B. Root Correction During Orthodontic Therapy. In Seminars in Orthodontics; WB Saunders Ltd.: Philadelphia, PA, USA, 2001; Volume 7, pp. 50–58. [Google Scholar]
- Edwards, J.G. The prevention of relapse in extraction cases. Am. J. Orthod. 1971, 60, 128–141. [Google Scholar] [CrossRef]
- Jarabak, J.R.; Fizzell, J.A. Technique and Treatment with Light-Wire Edgewise Appliances; Mosby: St. Louis, MO, USA, 1972; pp. 277–379. [Google Scholar]
- Liao, T.H.; Fang, J.C.; Wang, I.K.; Huang, C.S.; Chen, H.L.; Yen, T.H. Characteristics and Dental Indices of Orthodontic Patients Using Aligners or Brackets. Int. J. Environ. Res. Public Health 2022, 19, 6569. [Google Scholar] [CrossRef] [PubMed]
- Carli, E.; Pasini, M.; Lardani, L.; Giuca, G.; Miceli, M. Impact of self-ligating orthodontic brackets on dental biofilm and periodontal pathogens in adolescents. J. Biol. Regul. Homeost. Agents 2021, 35, 107–115. [Google Scholar] [PubMed]
- Borda, A.F.; Garfinkle, J.S.; Covell, D.A.; Wang, M.; Doyle, L.; Sedgley, C.M. Outcome assessment of orthodontic clear aligner vs. fixed appliance treatment in a teenage population with mild malocclusions. Angle Orthod. 2020, 90, 485–490. [Google Scholar] [CrossRef]
- Yassir, Y.A.; Nabbat, S.A.; McIntyre, G.T.; Bearn, D.R. Clinical effectiveness of clear aligner treatment compared to fixed appliance treatment: An overview of systematic reviews. Clin. Oral Investig. 2022, 26, 2353–2370. [Google Scholar] [CrossRef]
- Putrino, A.; Barbato, E.; Galluccio, G. Clear Aligners: Between Evolution and Efficiency-A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 2870. [Google Scholar] [CrossRef]
- Giancotti, A.; Greco, M.; Mampieri, G. Extraction treatment using Invisalign Technique. Prog. Orthod. 2006, 7, 32–43. [Google Scholar]
- Cassetta, M.; Altieri, F.; Pandolfi, S.; Giansanti, M. The combined use of computer-guided, minimally invasive, flapless corticotomy and clear aligners as a novel approach to moderate crowding: A case report. Korean J. Orthod. 2017, 47, 130–141. [Google Scholar] [CrossRef][Green Version]
- Honn, M.; Goz, G. A premolar extraction case using the Invisalign system. J. Orofac. Orthop. 2006, 67, 385–394. [Google Scholar] [CrossRef]
- Meng, M.M.; Chen, S. Four-premolar extraction treatment with clear aligner: A case report. Zhonghua Kou Qiang Yi Xue Za Zhi 2017, 52, 554–556. [Google Scholar] [PubMed]
- Hennessy, J.; Garvey, T.; Al-Awadhi, E.A. A randomized clinical trial comparing mandibular incisor proclination produced by fixed labial appliances and clear aligners. Angle Orthod. 2016, 86, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Caruso, S.; Nota, A.; Ehsani, S.; Maddalone, E.; Ojima, K.; Tecco, S. Impact of molar teeth distalization with clear aligners on occlusal vertical dimension: A retrospective study. BMC Oral Health 2019, 19, 182. [Google Scholar] [CrossRef] [PubMed]
- Grunheid, T.; Loh, C.; Larson, B.E. How accurate is Invisalign in nonextraction cases? Are predicted tooth positions achieved? Angle Orthod. 2017, 87, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, K.D.; King, G.; Ramsay, D.S.; Huang, G.; Bollen, A.M. Activation time and material stiffness of sequential removable orthodontic appliances. Part 3: Premolar extraction patients. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 837–845. [Google Scholar] [CrossRef]
- Li, W.; Wang, S.; Zhang, Y. The effectiveness of the Invisalign appliance in extraction cases using the the ABO model grading system a multicenter randomized controlled trial. Int. J. Clin. Exp. Med. 2015, 8, 8276–8282. [Google Scholar]
- Rocha, A.C.; Almeida, R.R.; Henriques, J.F.; Flores-Mir, C.; Almeida, M.R. Evaluation of long-term stability of mesiodistal axial inclinations of maxillary molars through panoramic radiographs in subjects treated with Pendulum appliance. Dent. Press J. Orthod. 2016, 21, 67–74. [Google Scholar] [CrossRef][Green Version]
- Puricelli, E. Panorametry: Suggestion of a method for mandibular measurements on panoramic radiographs. Head Face Med. 2009, 5, 19. [Google Scholar] [CrossRef]
- Chiqueto, K.; Janson, G.; de Almeida, C.T.; Storniolo, J.M.; Barros, S.E.; Henriques, J.F. Influence of root parallelism on the stability of extraction-site closures. Am. J. Orthod. Dentofac. Orthop. 2011, 139, e505–e510. [Google Scholar] [CrossRef]
- Gu, J.; Tang, J.S.; Skulski, B.; Fields, H.W., Jr.; Beck, F.M.; Firestone, A.R.; Kim, D.G.; Deguchi, T. Evaluation of Invisalign treatment effectiveness and efficiency compared with conventional fixed appliances using the Peer Assessment Rating index. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 259–266. [Google Scholar] [CrossRef]
- Ficho, A.C.; de Souza Faloni, A.P.; Pennisi, P.R.C.; Borges, L.G.F.; de Macedo Bernadino, I.; Paranhos, L.R.; Queiroz, T.P.; Santos, P.L. Is interdental papilla filling using hyaluronic acid a stable approach to treat black triangles? A systematic review. J. Esthet. Restor. Dent. 2021, 33, 458–465. [Google Scholar] [CrossRef]
- Rashid, Z.J.; Gul, S.S.; Shaikh, M.S.; Abdulkareem, A.A.; Zafar, M.S. Incidence of Gingival Black Triangles following Treatment with Fixed Orthodontic Appliance: A Systematic Review. Healthcare 2022, 10, 1373. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Miyamoto, T.; Nunn, M.E.; Garcia, R.I.; Dietrich, T. Root proximity as a risk factor for progression of alveolar bone loss: The Veterans Affairs Dental Longitudinal Study. J. Periodontol. 2008, 79, 654–659. [Google Scholar] [CrossRef] [PubMed]
- Pagano, S.; Lombardo, G.; Costanzi, E.; Balloni, S.; Bruscoli, S.; Flamini, S.; Coniglio, M.; Valenti, C.; Cianetti, S.; Marinucci, L. Morpho-functional effects of different universal dental adhesives on human gingival fibroblasts: An in vitro study. Odontology 2021, 109, 524–539. [Google Scholar] [CrossRef] [PubMed]
- Sarul, M.; Lewandowska, B.; Kawala, B.; Kozanecka, A.; Antoszewska-Smith, J. Objectively measured patient cooperation during early orthodontic treatment: Does psychology have an impact? Adv. Clin. Exp. Med. 2017, 26, 1245–1251. [Google Scholar] [CrossRef]
- Sarul, M.; Antoszewska-Smith, J.; Park, H.S. Self-perception of smile attractiveness as a reliable predictor of increased patient compliance with an orthodontist. Adv. Clin. Exp. Med. 2019, 28, 1633–1638. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).