

Comparative Evaluation of Adequacy of Root Canal Treatment Performed by Interns and Undergraduate Dental Students—A Cross-Sectional, Retrospective Study

 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
- All mature permanent single and multirooted teeth that were treated or retreated with a root canal (RC)
- The cases treated by senior and undergraduate students
- The cases with at least three available X-ray records
- The deciduous teeth
- Permanent immature teeth
- The teeth were treated with no available or unreadable radiographs
- The teeth were treated in the specialty clinics of staff members
- The teeth were already treated outside the outpatient clinics of the Jouf University
3. Results
4. Discussion
5. Conclusions
- The radiographic quality of RCT performed by senior and graduate students was acceptable in 53% of the treated cases.
- The short length of root canal filling was the most recorded error (29%).
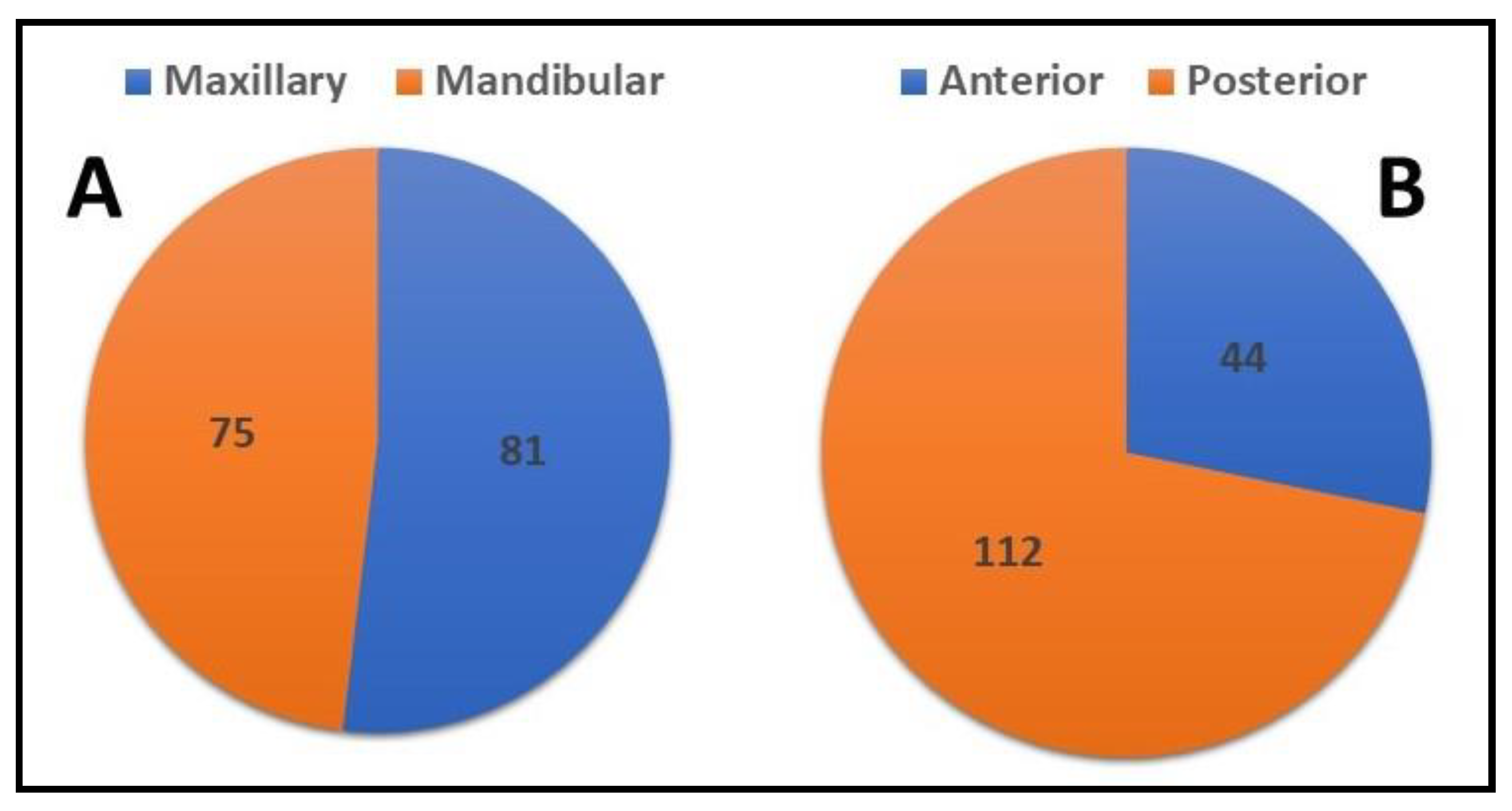
- The posterior teeth were the tooth type most associated with the incidence of the errors.
- There were no significant differences between the quality of RCT performed by different academic grades.
- A clear plan should be applied to improve the quality of treatment outcomes for undergraduate students by implementing more effective preclinical training courses, increasing the supervision ratio, and using more advanced modalities during treatment.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kishen, A.; Peters, O.A.; Zehnder, M.; Diogenes, A.R.; Nair, M.K. Advances in endodontics: Potential applications in clinical practice. J. Conserv. Dent. 2016, 19, 199. [Google Scholar] [CrossRef] [PubMed]
- Soikkonen, K. Endodontically treated teeth and periapical findings in the elderly. Int. Endod. J. 1995, 28, 200–203. [Google Scholar] [CrossRef] [PubMed]
- Hansrani, V. Assessing root canal fillings on a radiograph—An overview. Br. Dent. J. 2015, 219, 481–483. [Google Scholar] [CrossRef] [PubMed]
- Endodontology ESo. Quality guidelines for endodontic treatment: Consensus report of the European Society of Endodontology. Int. Endod. J. 2006, 39, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Stoll, R.; Betke, K.; Stachniss, V. The influence of different factors on the survival of root canal fillings: A 10-year retrospective study. J. Endod. 2005, 31, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Chandra, A. Discuss the factors that affect the outcome of endodontic treatment. Aust. Endod. J. 2009, 35, 98–107. [Google Scholar] [CrossRef]
- Peters, O.A. Current challenges and concepts in the preparation of root canal systems: A review. J. Endod. 2004, 30, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Kabak, Y.; Abbott, P. Prevalence of apical periodontitis and the quality of endodontic treatment in an adult Belarusian population. Int. Endod. J. 2005, 38, 238–245. [Google Scholar] [CrossRef]
- Chugal, N.M.; Clive, J.M.; Spångberg, L.S. Endodontic infection: Some biologic and treatment factors associated with outcome. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2003, 96, 81–90. [Google Scholar] [CrossRef]
- Naito, T. Better success rate for root canal therapy when treatment includes obturation short of the apex. Evid. Based Dent. 2005, 6, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganji, K.K.; Alam, M.K.; Gudipaneni, R.K.; Algarni, H.; Munisekhar, M.S.; Hamza, M.O.; Mousa, M.A.; Sghaireen, M.G. Do learning style preferences influence the cumulative gross point average and self directed learning hours in dental students: A preliminary study. BMC Med. Educ. 2022, 22, 493. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, K.C.; Shrivastava, D.; Khan, Z.A.; Nagarajappa, A.K.; Mousa, M.A.; Hamza, M.O.; Al-Johani, K.; Alam, M.K. Evaluation of temporomandibular disorders among dental students of Saudi Arabia using Diagnostic Criteria for Temporomandibular Disorders (DC/TMD): A cross-sectional study. BMC Oral Health 2021, 21, 211. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, K.C.; Shrivastava, D.; Nagarajappa, A.K.; Khan, Z.A.; Alzoubi, I.A.; Mousa, M.A.; Hamza, M.; David, A.P.; Al-Johani, K.; Sghaireen, M.G.; et al. Assessing the Prevalence and Association of Pulp Stones with Cardiovascular Diseases and Diabetes Mellitus in the Saudi Arabian Population—A CBCT Based Study. Int. J. Environ. Res. Public Health 2020, 17, 9293. [Google Scholar] [CrossRef]
- Awooda, E.M.; Siddig, R.I.; Alturki, R.S.; Sanhouri, N.M. Radiographic technical quality of root canal treatment performed by undergraduate dental students at the Academy Dental Teaching Hospital, UMST, Sudan. J. Int. Soc. Prev. Community Dent. 2016, 6, 554. [Google Scholar] [CrossRef]
- Elemam, R.F.; Abdul Majid, Z.S.; Groesbeck, M.; Azevedo, Á.F. Quality of root canals performed by the inaugural class of dental students at Libyan International Medical University. Int. J. Dent. 2015, 2015, 135120. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, R.O.; Abu-bakr, N.H.; Ibrahim, Y.E. Quality of root canal treatment performed by undergraduate dental students at the University of Khartoum, Sudan. Aust. Endod. J. 2011, 37, 56–60. [Google Scholar] [CrossRef]
- Fong, W.; Heidarifar, O.; Killough, S.; Lappin, M.; El Karim, I. An audit on technical quality of root fillings performed by undergraduate students. Int. Endod. J. 2018, 51, e197–e203. [Google Scholar] [CrossRef]
- Vukadinov, T.; Blažić, L.; Kantardžić, I.; Lainović, T. Technical quality of root fillings performed by undergraduate students: A radiographic study. Sci. World J. 2014, 2014, 751274. [Google Scholar] [CrossRef]
- Rapo, H.; Oikarinen-Juusola, K.; Laitala, M.; Pesonen, P.; Anttonen, V. Outcomes of endodontic treatments performed by dental students-a follow-up study. J. Dent. Oral Biol. 2017, 2, 1046. [Google Scholar]
- Polyzos, N.K.; Sarris, K.G.; Pita, A.I.; Mikrogeorgis, G.V.; Lyroudia, K.M. Quality of root canal fillings performed by undergraduate students and the related factors on the treatment outcome: A 2-to 5-year follow-up. Eur. Endod. J. 2018, 3, 179. [Google Scholar] [CrossRef]
- Fritz, A.L.C.; Ribeiro, F.C.; Xavier, J.M.B.; Reis, C.M.; Demuner, C. Evaluation of Quality of Root Canal Fillings Performed by Undergraduate Students of a Brazilian University Avaliação da qualidade da obturação do canal radicular realizada por estudantes de graduação de uma Universidade brasileira. Braz. J. Health Rev. 2021, 4, 18964–18975. [Google Scholar] [CrossRef]
- Ribeiro, D.M.; Henckel, M.D.; Mello, F.W.; Felippe, M.C.S.; Felippe, W.T. Radiographic analysis the obturation’s quality in root canal treatment performed by a South Brazilian sample of undergraduate students. RGO-Rev. Gaúcha De Odontol. 2019, 67, e20190040. [Google Scholar] [CrossRef]
- da Silva, P.Z.; Ribeiro, F.C.; Xavier, J.M.B.; Pratte-Santos, R.; Demuner, C. Radiographic evaluation of root canal treatment performed by undergraduate students, part I; iatrogenic errors. Iran. Endod. J. 2018, 13, 30. [Google Scholar]
- Galhotra, V.; Rai, T.; Kaur, I. Assessment of quality of root canal fillings performed by undergraduate dental students. J. Adv. Med. Dent. Sci. Res. 2017, 5, 153. [Google Scholar]
- Alsulaimani, R.S.; Al-Manei, K.K.; Alsubait, S.A.; AlAqeely, R.S.; Al-Shehri, S.A.; Al-Madi, E.M. Effects of clinical training and case difficulty on the radiographic quality of root canal fillings performed by dental students in Saudi Arabia. Iran. Endod. J. 2015, 10, 268. [Google Scholar] [PubMed]
- Smadi, L.; Hammad, M.; El-Ma’aita, A. Evaluation of the Quality of Root Canal Treatments Performed by Dental Undergraduates: Is There a Need to Review Preclinical Endodontic Courses? Am. J. Educ. Res. 2015, 3, 1554–1558. [Google Scholar]
- AbuMostafa, A.; Ahmad, I.A.; Alenezy, G.; AlZoman, A. Quality of root canal filling performed by undergraduate students in a Saudi Dental College. J. Dent. Oral Hyg. 2015, 7, 64–70. [Google Scholar]
- AlRahabi, M.K. Evaluation of complications of root canal treatment performed by undergraduate dental students. Libyan J. Med. 2017, 12, 1345582. [Google Scholar] [CrossRef]
- Saatchi, M.; Mohammadi, G.; Sichani, A.V.; Moshkforoush, S. Technical quality of root canal treatment performed by undergraduate clinical students of Isfahan dental school. Iran. Endod. J. 2018, 13, 88. [Google Scholar]
- Yavari, H.; Samiei, M.; Shahi, S.; Borna, Z.; Abdollahi, A.A.; Ghiasvand, N.; Shariati, G. Radiographic evaluation of root canal fillings accomplished by undergraduate dental students. Iran. Endod. J. 2015, 10, 127. [Google Scholar]
- Eskandarloo, A.; Karkehabadi, H.; Hashemi, S.Z.H.; Ahmadi, M.; Hendi, S.S. Radiographic quality of root canal obturation performed by fifth year students of hamadan dental school. Iran. Endod. J. 2017, 12, 236. [Google Scholar] [PubMed]
- Chakravarthy, P.V.K.; Moorthy, J.R.K. Radiographic assessment of quality of root fillings performed by undergraduate students in a Malaysian Dental School. Saudi Endod. J. 2013, 3, 77. [Google Scholar] [CrossRef]
- Moradi, S.; Gharechahi, M. Quality of root canal obturation performed by senior undergraduate dental students. Iran. Endod. J. 2014, 9, 66. [Google Scholar]
- Mukhaimer, R. Radiographic technical quality of root canal fillings performed by dental students in Palestine. Indian J. Oral Sci. 2013, 4, 55. [Google Scholar] [CrossRef]
- Unal, G.C.; Kececi, A.D.; Kaya, B.U.; Tac, A.G. Quality of root canal fillings performed by undergraduate dental students. Eur. J. Dent. 2011, 5, 324–330. [Google Scholar] [CrossRef]
- Habib, A.A.; Doumani, M.D.; Nassani, M.Z.; Shamsy, E.; Jto, B.S.; Arwadi, H.A.; Mohamed, S.A. Radiographic assessment of the quality of root canal fillings performed by senior dental students. Eur. Endod. J. 2018, 3, 101. [Google Scholar] [CrossRef]
- Agwan, M.A.S.; Sheikh, A.; Shaikh, S. Qualitative Analysis of Root Canal Treatments performed by Undergraduate Students: A Retrospective Study. Pesqui. Bras. Em Odontopediatria E Clínica Integr. 2021, 21, e0260. [Google Scholar] [CrossRef]
- Ehsani, M.; Abesi, F.; Ghasemi, T. Technical Quality of Root Fillings Performed by Dental Students in Babol Dental School. J. Dent. Mater. Tech. 2014, 3, 66–70. [Google Scholar]
- Alghamdi, N.S.; Algarni, Y.A.; Ain, T.S.; Alfaifi, H.M.; AlQarni, A.A.; Mashyakhi, J.Q.; Alasmari, S.E.; Alshahrani, M.M. Endodontic mishaps during root canal treatment performed by undergraduate dental students: An observational study. Medicine 2021, 100, e27757. [Google Scholar] [CrossRef]
- Eckerbom, M. Prevalence and technical standard of endodontic treatment in a Swedish population. A longitudinal study. Swed. Dent. J. Suppl. 1993, 93, 1–45. [Google Scholar]
- Ödesjö, B.; Helldén, L.; Salonen, L.; Langeland, K. Prevalence of previous endodontic treatment, technical standard and occurrence of periapical lesions in a randomly selected adult, general population. Dent. Traumatol. 1990, 6, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Frisk, F. Incidence, frequency, and prevalence. In Apical Periodontitis in Root-Filled Teeth: Endodontic Retreatment and Alternative Approaches; Springer: Berlin/Heidelberg, Germany, 2018; pp. 7–19. [Google Scholar]
- Endodontology ESo. Consensus report of the European Society of Endodontology on quality guidelines for endodontic treatment. Int. Endod. J. 1994, 27, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y.L.; Mann, V.; Gulabivala, K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: Part 2, tooth survival. Int. Endod. J. 2011, 44, 610–625. [Google Scholar] [CrossRef]
- Grayli, E.; Peyvandi, A.; Mallahi, M.; Naeemi, S.; Afshari, E. Radiographic Evaluation of Iatrogenic Errors of Root Canal Treatments Performed in an Undergraduate Dental Clinic. J. Dent. Mater. Tech. 2021, 10, 16–21. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The Continent | The Study | Location | Type of Study (Type of Course) | Number of Treated Teeth (or Canals) | Adequate (%) | Not Adequate (%) |
|---|---|---|---|---|---|---|
| Africa | Awooda et al., 2016 [14] | Sudan | In-vivo (5th year) | 173 T (324 RC) | 55.5% | 44.5% |
| Elemam et al., 2015 [15] | Libya | In-vivo (4th and 5th year) | 128 T (284 RC) | 53.9% | 46.1% | |
| Elsayed et al., 2011 [16] | Sudan | In-vivo (4th and 5th year) | 166 T (265 RC) | 52.7% | 47.3% | |
| Europe | Fong et al., 2018 [17] | UK | In-vivo (4th and 5th year) | 222 T (381RC) | 66.4% | 33.6% |
| Vukadinov et al., 2014 [18] | Serbia | In-vivo (5th year) | 322 T (565RC) | 74.2% | 25.8% | |
| Rapo et al., 2017 [19] | Finland | In-vivo (Undergrad) | 105 T (167 RC) | 65.7% | 34.3% | |
| Polyzos et al., 2018 [20] | Greece | In-vivo (Undergrad) | 244 T (349 RC) | 40.4% | 59.6% | |
| America | Fritz et al., 2021 [21] | Brazil | In-vivo (4th and 5th year) | 368 T (442 RC) | 93.8% | 6.2% |
| Ribeiro et al., 2019 [22] | Brazil | In-vivo (4th and 5th year) | 274 T (381 RC) | 71.9% | 28.1% | |
| da Silva et al., 2018 [23] | Brazil | In-vivo (4th and 5th year) | 397 T (480 RC) | 92.7% | 7.3% | |
| Asia | Galhotra et al., 2017 [24] | India | In-vivo (5th year and intern) | 135 T (246 RC) | 80.9% | 19.1% |
| Alsulaimani et al., 2017 [25] | KSA | In-vivo (5th and 4th year) | 692 T (1081 RC) | 87.9% | 12.1% | |
| Smadi et al., 2015 [26] | Jordan | In-vivo (4th and 5th year) | 213 T (327 RC) | 29.2% | 70.8% | |
| AbuMostafa et al., 2015 [27] | KSA | In-vivo (5th year) | 241 T (450 RC) | 26.1% | 73.9% | |
| Alrahabi et al., 2017 [28] | KSA | In-vivo (4th and 5th year) | 280 T (533 RC) | 68.9% | 31.1% | |
| Saatchi et al., 2018 [29] | Iran | In-vivo (4th and 5th year) | 784 T (1674 RC) | 54.1% | 55.9% | |
| Yavari et al., 2015 [30] | Iran | In-vivo (4th, 5th, and intern) | 620 T (1183 RC) | 72.1% | 27.9% | |
| Eskandarloo et al., 2017 [31] | Iran | In-vivo (5th year) | 432 T (605 RC) | 70.8% | 29.2% | |
| Chakravarthy et al., 2013 [32] | Malaysia | In-vivo (4th and 5th year) | 153 T (194 RC) | 61.3% | 38.7% | |
| Moradi et al., 2014 [33] | Iran | In-vivo (4th and 5th year) | 200 T (411 RC) | 45% | 55% | |
| Mukhaimer et al., 2013 [34] | Palestine | In-vivo (4th and 5th year) | 612 T (1013 RC) | 71.7% | 28.3% | |
| Unal et al., 2011 [35] | Turkey | In-vivo (4th and 5th year) | 460 T (833 RC) | 73.7% | 26.3% | |
| Habib et al., 2018 [36] | KSA | In-vivo (senior students) | 246 T (390 RC) | 32.6% | 66.4% | |
| Agwan et al., 2021 [37] | Pakistan | In-vivo (5th year) | 92 T (170 RC) | 52.3% | 47.6% | |
| Ehsani et al., 2014 [38] | Iran | In-vivo (4th and 5th year) | 325 T (727 RC) | 17.5% | 82.5% | |
| Alghamdi et al., 2021 [39] | KSA | In-vivo (4th and 5th year) | 404 T (730 RC) | 86% | 14% | |
| Overall cases | 8288 T (14,205 RC) | 61.4% | 38.6% | |||
| Variable | Definition | Criteria | |
|---|---|---|---|
| 1 | Canal recognition | The canal/s is recognized and filled | Acceptable |
| One or more canals were not recognized | Unacceptable | ||
| 2 | Length of RCF | RCF end 0–2 mm from the radiographic apex | Acceptable |
| RCF end more than 2 mm from the apex | Underextended | ||
| RCF passed the radiographic apex | Overextended | ||
| 3 | Taper of RCF | The taper is consistent from the coronal to the apex of the treated tooth | Acceptable |
| The taper is lacking from the coronal to the apex | Unacceptable | ||
| 4 | Density of RCF | No voids are recognizable within the canal | Acceptable |
| Voids are recognizable within the canal | Unacceptable | ||
| 5 | Coronal seal | The coronal part is adequately sealed by filling, adequate inserted post, or crowning | Acceptable |
| Lack of coronal seal due to deficiency in the restoration | Unacceptable | ||
| 6 | Apical seal | The apex of tooth is apparently sealed with RCF | Acceptable |
| Lack of the seal or voids is recognizable at the apex of the RCF | Acceptable | ||
| 7 | Broken instrument | No broken instrument can be seen within the canals | Acceptable |
| One or more broken instrument is apparent within one or more canals | Unacceptable |
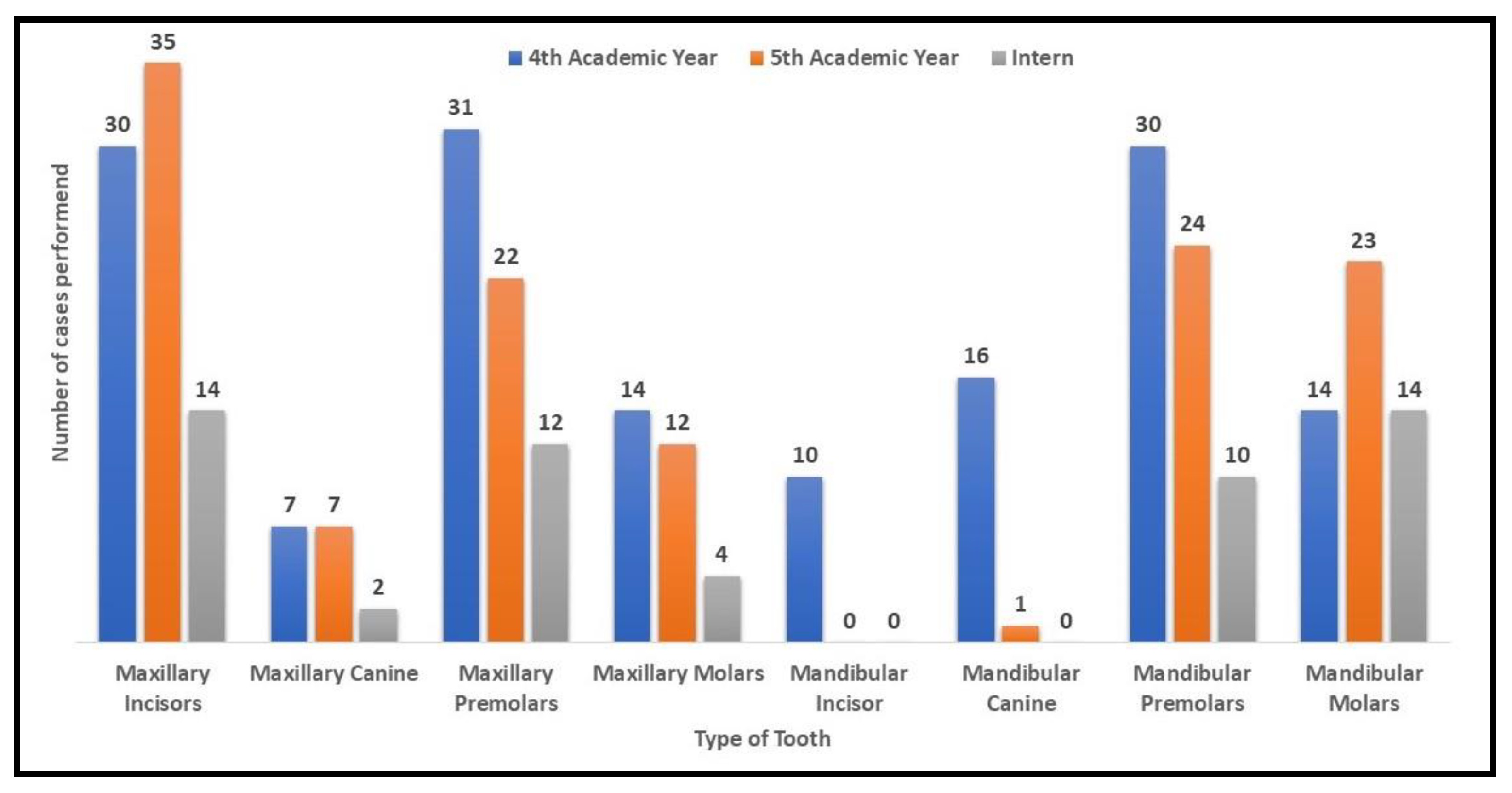
| 4th Year Students [n = 152 (45.8)] | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Nature of Endodontic Error | Tooth Types | p Value | ||||||||
| Max. Incisors (n = 30) | Max. Canine (n = 7) | Max. PM (n = 31) | Max. Molars (n = 14) | Mandi. Incisor (n = 10) | Mandi. Canine (n = 16) | Mandi. PM (n = 30) | Mandi. Molars (n = 14) | n. Errors (%) | ||
| Root perforation | 0 | 0 | 2 (50) | 0 | 0 | 0 | 2 (50) | 0 | 4 (2.9) | 0.525 |
| Short obturation | 6 (18.8) | 2 (6.3) | 10 (31.3) | 2 (6.3) | 0 | 2 (6.3) | 6 (18.8) | 4 (12.5) | 32 (23.4) | 0.444 |
| Over-extended obturation | 4 (25) | 0 | 0 | 6 (37.5) | 0 | 2 (12.5) | 0 | 4 (25) | 16 (11.7) | 0.000 ⁋ |
| Voids | 4 (25) | 0 | 2 (12.5) | 4 (25) | 0 | 2 (12.5) | 4 (25) | 0 | 16 (11.7) | 0.212 |
| Canal Left Unfilled | 2 (14.3) | 2 (14.3) | 4 (28.6) | 0 | 0 | 0 | 4 (28.6) | 2 (14.3) | 14 (10.2) | 0.002 € |
| No Coronal Seal | 2 (12.5) | 0 | 2 (12.5) | 2 (12.5) | 0 | 0 | 4 (25) | 6 (37.5) | 16 (11.7) | 0.004 € |
| No Apical Seal | 2 (8) | 2 (8) | 5 (20) | 6 (24) | 0 | 0 | 6 (24) | 4 (16) | 25 (18.2) | 0.019 * |
| Broken Instrument | 0 | 0 | 8 (57.1) | 0 | 2 (14.3) | 2 (14.3) | 0 | 2 (14.3) | 14 (10.2) | 0.005 € |
| Errors% | 137 (90.13) | |||||||||
| 5th Year Students [n = 124 (37.3)] | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Nature of Endodontic Error | Tooth Types | p Value | |||||||
| Max. Incisors (n = 35) | Max. Canine (n = 7) | Max. PM (n = 22) | Max. Molars (n = 12) | Mandi. Canine (n = 1) | Mandi. PM (n = 24) | Mandi. Molars (n = 23) | n. Errors (n = 125) | ||
| Root Perforation | 0 | 1 (16.7) | 2 (33.3) | 0 | 1 (16.7) | 0 | 2 (33.3) | 6 (4.8) | 0.000 ⁋ |
| Short Obturation | 8 (18.6) | 2 (4.7) | 6 (14) | 0 | 0 | 17 (39.5) | 10 (23.3) | 43 (34.4) | 0.000 ⁋ |
| Over-extended obturation | 2 (50) | 0 | 0 | 0 | 0 | 0 | 2 (50) | 4 (3.2) | 0.531 |
| Voids | 0 | 0 | 0 | 0 | 0 | 0 | 3 (100) | 3 (2.4) | 0.036 * |
| Canal Left Unfilled | 3 (21.4) | 0 | 3 (21.4) | 0 | 0 | 4 (28.6) | 4 (28.6) | 14 (11.2) | 0.241 |
| No Coronal Seal | 0 | 5 (50) | 0 | 0 | 0 | 0 | 5 (50) | 10 (8) | 0.01 * |
| No Apical Seal | 8 (20.5) | 2 (5.1) | 7 (17.9) | 1 (2.6) | 0 | 12 (30.8) | 9 (23.1) | 39 (31.2) | 0.167 |
| Broken Instrument | 0 | 0 | 4 (66.7) | 0 | 0 | 0 | 2 (33.3) | 6 (4.8) | 0.039 * |
| Errors | 125 | ||||||||
| Intern [n = 56 (16.9)] | ||||||||
|---|---|---|---|---|---|---|---|---|
| Nature of Endodontic Error | Tooth Types | p Value | ||||||
| Max. Incisors (n = 14) | Max. Canine (n = 2) | Max. PM (n = 12) | Max. Molars (n = 4) | Mandi. PM (n = 10) | Mandi. Molars (n = 14) | Errors (n = 42) | ||
| Root Perforation | 0 | 0 | 0 | 0 | 0 | 0 | 0 (0) | NA |
| Short Obturation | 0 | 0 | 2 (16.7) | 0 | 4 (33.3) | 6 (50) | 12 (28.6) | 0.043 * |
| Over-extended Obturation | 2 (50) | 0 | 0 | 2 (50) | 0 | 0 | 4 (9.5) | 0.010 * |
| Voids | 0 | 0 | 0 | 0 | 0 | 0 | 0 (0) | NA |
| Canal Left Unfilled | 2 (20) | 0 | 0 | 2 (20) | 2 (20.0) | 4 (40) | 10 (23.8) | 0.213 |
| No Coronal Seal | 0 | 0 | 0 | 2 (50) | 0 | 2 (50) | 4 (9.5) | 0.010 * |
| No Apical Seal | 0 | 0 | 2 (16.7) | 2 (16.7) | 4 (33.3) | 4 (33.3) | 12 (28.6) | 0.112 |
| Broken Instrument | 0 | 0 | 0 | 0 | 0 | 0 | 0 (0) | NA |
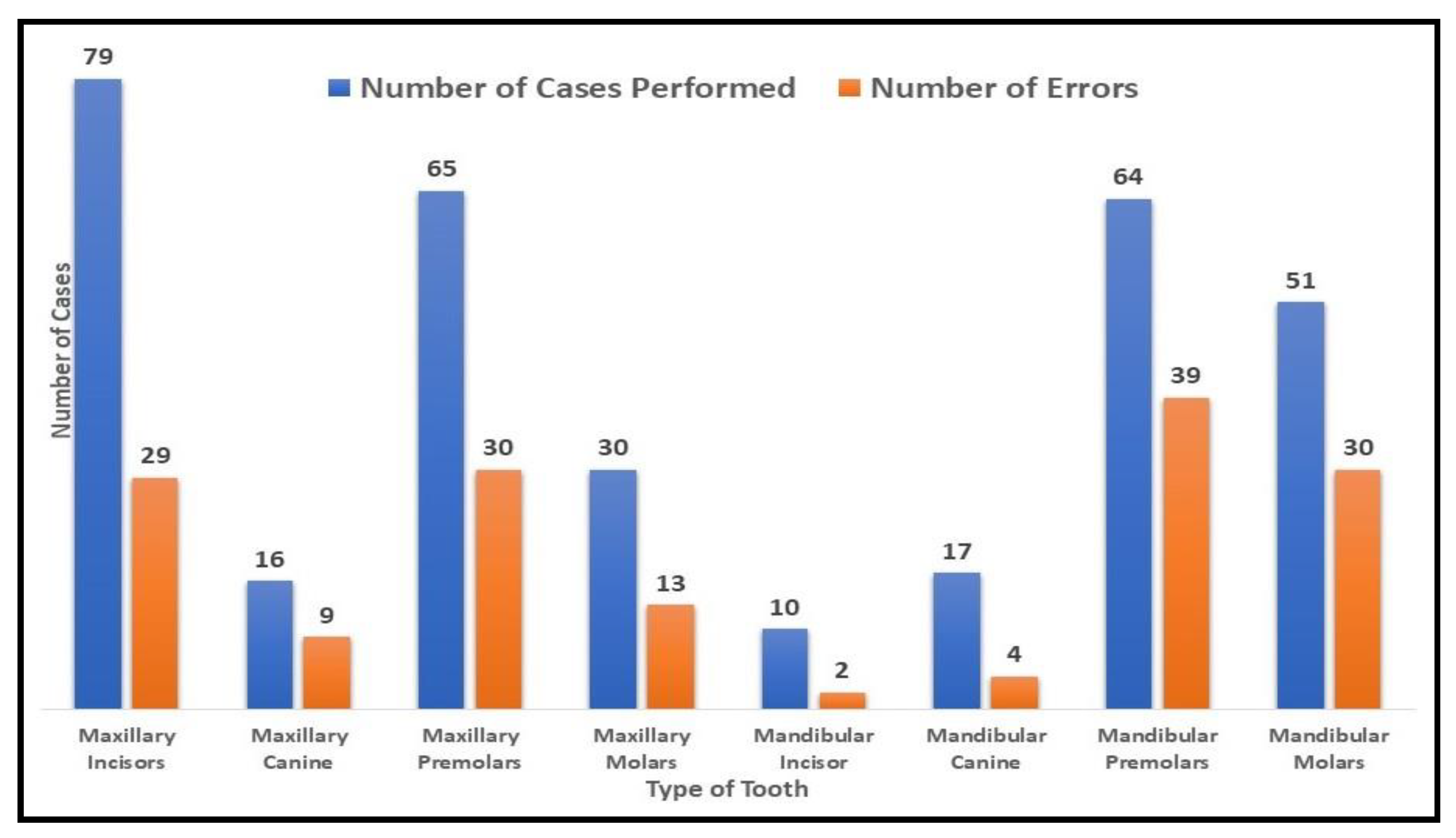
| 4th Yr. + 5th Yr. + Intern = 332 (n) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Nature of Endodontic Error | Tooth Types | |||||||
| Maxillary Incisors (30 + 35 + 14 = 79) | Maxillary Canine (7 + 7 + 2 = 16) | Maxillary Premolars (31 + 22 + 12 = 65) | Maxillary Molars (14 + 12 + 4 = 30) | Mandibular Premolars (30 + 24 + 10 = 64) | Mandibular Molars (14 + 23 + 14 = 51) | Sum of Errors (%) | ||
| Root Perforation | 4th Yr. | 0 | 0 | 2 (6.5) | 0 | 2 (6.7) | 0 | 4 |
| 5th Yr. | 0 | 1 | 2 (9.1) | 0 | 0 | 2 (8.7) | 4 | |
| Intern | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| p value | NA | 0.504 | 0.571 | NA | 0.31 | 0.282 | 8 (2.8) | |
| Short Obturation | 4th Yr. | 6 (20) | 2 (28.6) | 10 (32.3) | 2 (14.3) | 6 (20) | 4 (28.6) | 30 |
| 5th Yr. | 8 (22.9) | 2 (28.6) | 6 (27.3) | 0 | 17 (70.8) | 10 (43.5) | 43 | |
| Intern | 0 | 0 | 2 (16.7) | 0 | 4 (40) | 6 (42.9) | 12 | |
| p value | 0.157 | 0.683 | 0.591 | 0.316 | 0.00 € | 0.632 | 85 (29.6) | |
| Over-extended Obturation | 4th Yr. | 4 (13.3) | 0 | 0 | 6 (42.9) | 0 | 4 (28.6) | 14 |
| 5th Yr. | 2 (5.7) | 0 | 0 | 0 | 0 | 2 (8.7) | 4 | |
| Intern | 2 (14.3) | 0 | 0 | 2 (50) | 0 | 0 | 4 | |
| p value | 0.513 | NA | NA | 0.025 * | NA | 0.053 | 22 (7.7) | |
| Voids | 4th Yr. | 4 (13.3) | 0 | 2 (6.5) | 4 | 4 (13.3) | 0 | 16 |
| 5th Yr. | 0 | 0 | 0 | 0 | 0 | 3 (13) | 3 | |
| Intern | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| p value | 0.03 * | NA | 0.323 | 0.072 | 0.089 | 0.144 | 19 (6.6) | |
| Canal left unfilled | 4th Yr. | 2 (6.7) | 2 (28.6) | 4 (13) | 0 | 4 (13.3) | 2 (14.3) | 14 |
| 5th Yr. | 3 (8.6) | 0 | 3 (13.6) | 0 | 4 (16.7) | 4 (17.4) | 14 | |
| Intern | 2 (14.2) | 0 | 0 | 2 (50) | 2 (20) | 4 (28.6) | 10 | |
| p value | 0.78 | 0.01 | 0.13 | 0.00 € | 0.867 | 0.595 | 38 (13.2) | |
| No Coronal Seal | 4th Yr. | 2 (6.7) | 0 | 2 (6.5) | 2 (14.3) | 4 (13.3) | 6 (42.9) | 16 |
| 5th Yr. | 0 | 2 (28.6) | 0 | 0 | 0 | 5 (21.7) | 7 | |
| Intern | 0 | 0 | 0 | 2 (50) | 0 | 2 (14.3) | 4 | |
| p value | 0.191 | 0.23 | 0.323 | 0.039 * | 0.089 | 0.19 | 27 (9.4) | |
| No Apical Seal | 4th Yr. | 2 (6.7) | 2 (28.6) | 5 (16.7) | 6 (42.9) | 6 (20) | 4 (28.6) | 25 |
| 5th Yr. | 8 (22.9) | 2 (28.6) | 7 (31.8) | 1 (8.3) | 12 (50) | 9 (39.1) | 35 | |
| Intern | 0 | 0 | 2 (16.7) | 2 (50) | 4 (40) | 4 (28.6) | 12 | |
| p value | 0.045 * | 0.683 | 0.379 | 0.103 | 0.064 | 0.728 | 72 (25.1) | |
| Broken Instrument | 4th Yr. | 0 | 0 | 8 (25.8) | 0 | 0 | 2 (14.3) | 10 |
| 5th Yr. | 0 | 0 | 4 (18.2) | 0 | 0 | 2 (8.7) | 6 | |
| Intern | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| p value | NA | NA | 0.147 | NA | NA | 0.364 | 16 (5.6) | |
| Sum of errors | 287 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mousa, M.A.; Alshammari, A.M.; Alshammari, A.Z.; Alsharari, M.M.; Baig, M.N.; Srivastava, K.C.; Shrivastava, D.; Alam, M.K.; Alonazi, M.A.; Algarni, H.A. Comparative Evaluation of Adequacy of Root Canal Treatment Performed by Interns and Undergraduate Dental Students—A Cross-Sectional, Retrospective Study. Appl. Sci. 2022, 12, 9079. https://doi.org/10.3390/app12189079
Mousa MA, Alshammari AM, Alshammari AZ, Alsharari MM, Baig MN, Srivastava KC, Shrivastava D, Alam MK, Alonazi MA, Algarni HA. Comparative Evaluation of Adequacy of Root Canal Treatment Performed by Interns and Undergraduate Dental Students—A Cross-Sectional, Retrospective Study. Applied Sciences. 2022; 12(18):9079. https://doi.org/10.3390/app12189079
Chicago/Turabian StyleMousa, Mohammed Assayed, Akram Mojidea Alshammari, Abdulelah Zaid Alshammari, Meshari M. Alsharari, Muhammad Nadeem Baig, Kumar Chandan Srivastava, Deepti Shrivastava, Mohammad Khursheed Alam, Meshal Aber Alonazi, and Hmoud Ali Algarni. 2022. "Comparative Evaluation of Adequacy of Root Canal Treatment Performed by Interns and Undergraduate Dental Students—A Cross-Sectional, Retrospective Study" Applied Sciences 12, no. 18: 9079. https://doi.org/10.3390/app12189079
APA StyleMousa, M. A., Alshammari, A. M., Alshammari, A. Z., Alsharari, M. M., Baig, M. N., Srivastava, K. C., Shrivastava, D., Alam, M. K., Alonazi, M. A., & Algarni, H. A. (2022). Comparative Evaluation of Adequacy of Root Canal Treatment Performed by Interns and Undergraduate Dental Students—A Cross-Sectional, Retrospective Study. Applied Sciences, 12(18), 9079. https://doi.org/10.3390/app12189079