
The Use of Social Robots in the Diagnosis of Autism in Preschool Children

 , , , , , and
, , , , , and
Abstract
:1. Introduction
- Q1:
- Are there significant differences between turn-taking behaviors in neurotypical children compared with children with autism when interacting with a social robot?
- Q2:
- Can human–robot social interactions differentiate patterns of interest and motoric behaviors in children with a diagnosis of autism?
2. Study Design
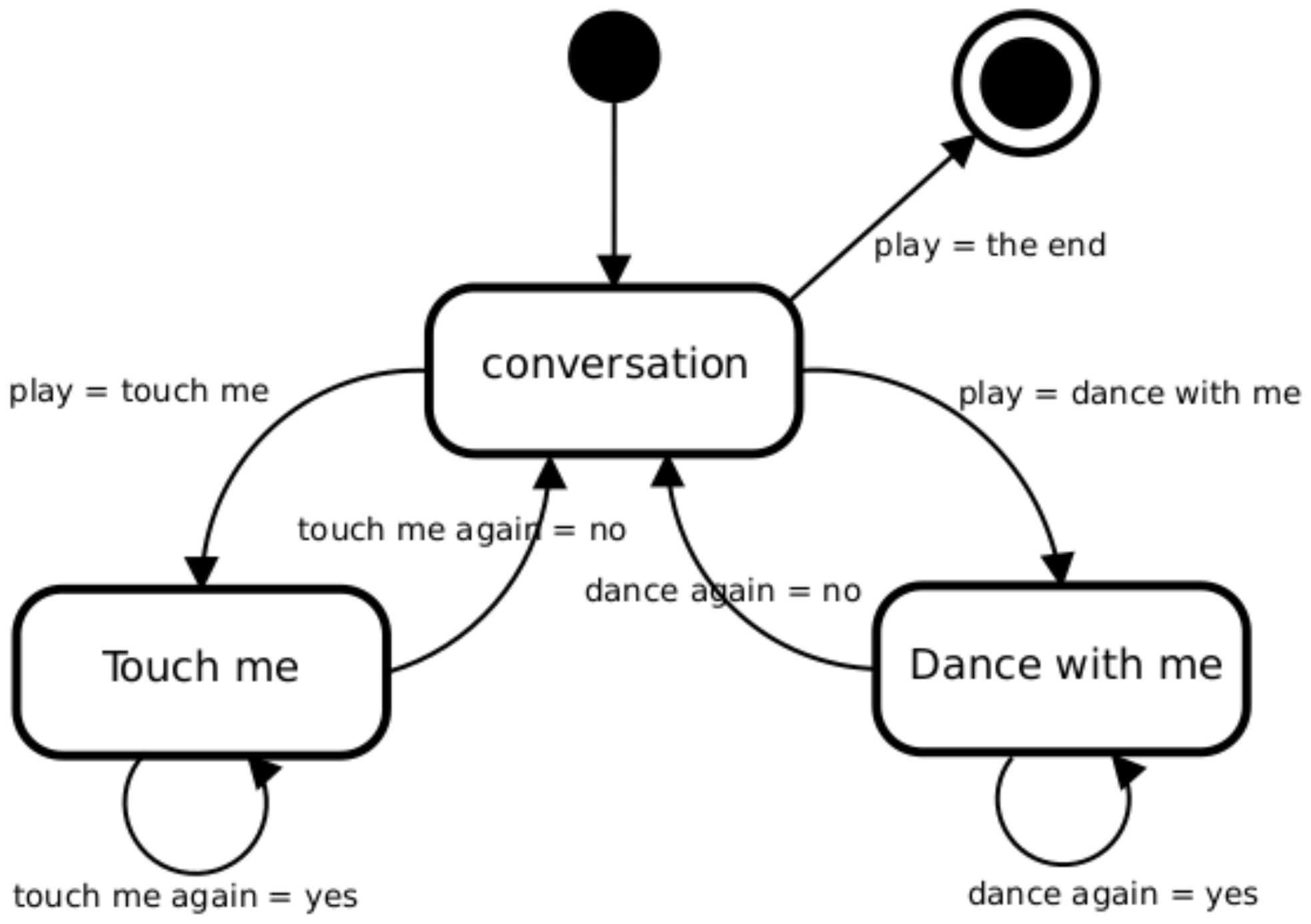
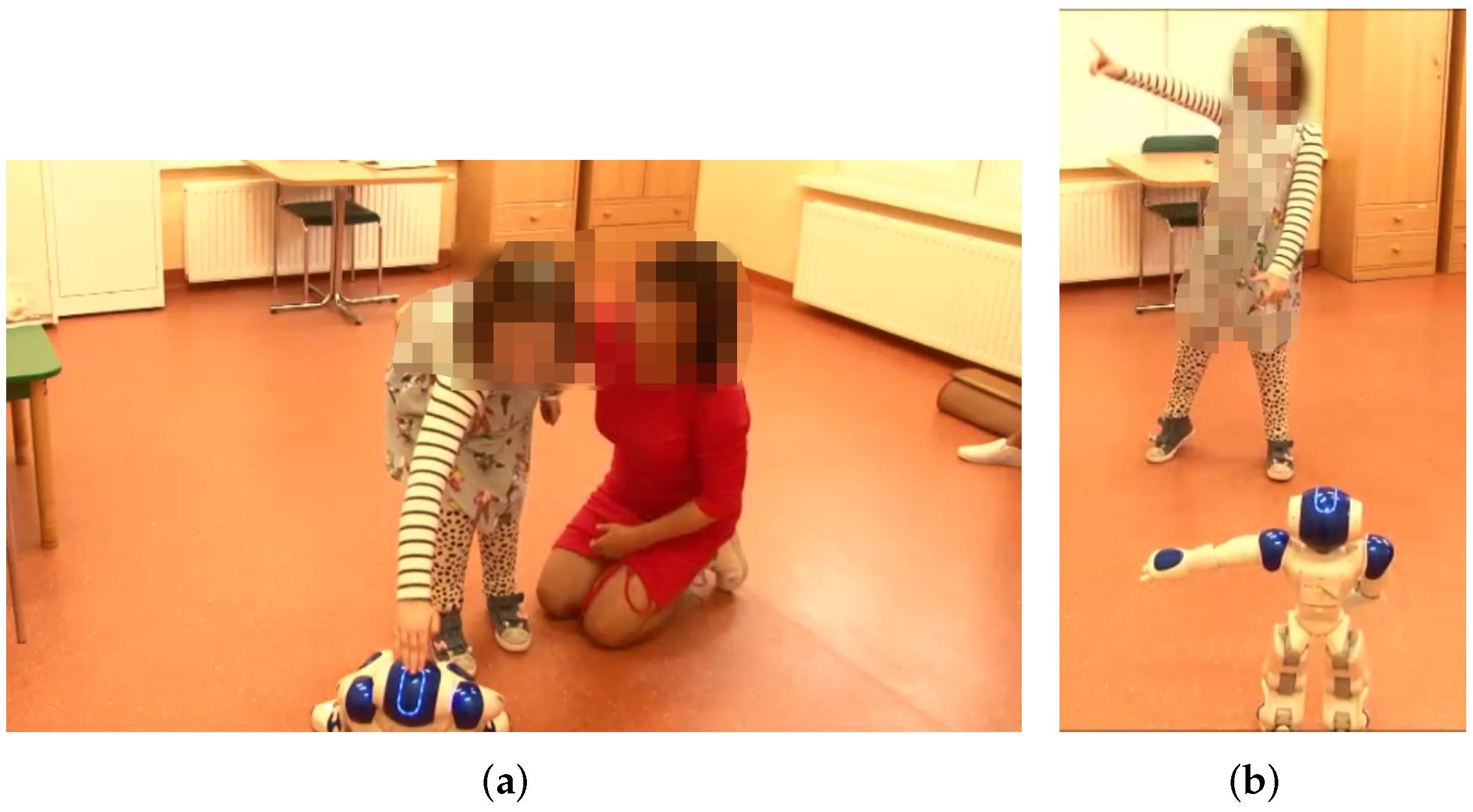
2.1. The NAO Robot and the Interactive Games Designed for the Study
2.2. Participants
2.3. Procedure and Materials
2.4. Psychological Assessment of Children’s Behavior from Video Material: The Procedure Used by the Competent Raters
3. Results
3.1. Non-Parametric Analysis of Turn-Taking in the Touch Me and Dance-with-Me Games
3.2. Observational Measures of ASD Symptoms, i.e., Children’s Interest in the Robot and Additional Movements
- Interest in the robot subscale. The Mann–Whitney test for non-parametric analysis of the collected ratings showed that interest in the robot for autistic children () was higher than presented by typically developing children (). The distributions in the two groups differed significantly (Mann–Whitney , (5 children times 6 competent raters), ).
- Additional movements subscale. Further analysis of the presence of ASD symptoms based on the same test indicated that autistic children expressed more additional movements () than typically developing children () during interaction with NAO. The distributions in the two groups differed significantly (Mann–Whitney , , ).
4. Discussion
5. Limitations and Further Directions of Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| The Child’s ID | Competent Rater’s ID | ||||||
|---|---|---|---|---|---|---|---|
| Instruction: In the part The interaction with the robot Please focus on the child’s activity while playing with the robot. Please provide “a precise number of all observed movement activities of the child”: (i) imitating the gestures and movements of the robot; (ii) touching the robot on command. The quality of the imitation or the quality of the instructions performed does not matter. Reactions of a child when supported by a teacher should also be approved if the child initiated them. In the Interest in the robot and Additional Movements sections, the child’s different reactions while playing with the robot should be assessed globally and the intensity/frequency of these reactions should be indicated on a scale. | |||||||
| I Interaction with the robot | |||||||
| 1 | Movement activity of the child during the Touch me game | ||||||
| Count each movement activity initiated by a child at the robot’s command and ending with a touch of the robot. | |||||||
| Give the number of all movement activities initiated by the child at the robot’s command, ending with a touching the robot. | |||||||
| 2 | Imitation reactions | ||||||
| Count each child’s response that imitates the robot’s movements during its dance | |||||||
| Give the total number of the child’s responses that imitate the robot’s movements during the dance. | |||||||
| II Interest in the robot | |||||||
| (0-none, 1-sporadic, 2-average, 3-frequent, 4-very intense, 5-constant) | |||||||
| 3 | Visual contact | 0 | 1 | 2 | 3 | 4 | 5 |
| The child looks towards the robot or into the eyes of the robot | |||||||
| 4 | Motor activity | 0 | 1 | 2 | 3 | 4 | 5 |
| The child shows movement activity in the presence of the robot: e.g., approaches the robot, reduces the distance to the robot, approaches the robot with the teacher. | |||||||
| 5 | Expression of gestures | 0 | 1 | 2 | 3 | 4 | 5 |
| The child uses gestures to express emotions while playing with the robot: e.g., points to the robot, picks up the robot. | |||||||
| 6 | Spontaneous expression | 0 | 1 | 2 | 3 | 4 | 5 |
| The child speaks to the robot (e.g., ‘Hello, robot.’). The child speaks about the robot (e.g., ‘It looks at me.’) | |||||||
| 7 | Emotional reactions | 0 | 1 | 2 | 3 | 4 | 5 |
| The child smiles at the robot, can laugh spontaneously in the presence of the robot. | |||||||
| III Additional movements | |||||||
| (0-none, 1-sporadic, 2-average, 3-frequent, 4-very intense, 5-constant) | |||||||
| 8 | Stereotypical movements | 0 | 1 | 2 | 3 | 4 | 5 |
| The child jumps and/or spins in circles. | |||||||
| 9 | Compulsions | 0 | 1 | 2 | 3 | 4 | 5 |
| The child grabs his clothes and twists them around. The child grabs his or her hair and twists it. | |||||||
| 10 | Movement mannerisms | 0 | 1 | 2 | 3 | 4 | 5 |
| The child waves or flaps his arms; clapping. | |||||||
Appendix B
| Interaction with the Robot | Interest in the Robot | Additional Movements | ||
|---|---|---|---|---|
| N | 30 | 30 | 30 | 30 |
| Mean | 1.0883 | 0.3231 | 7.63 | 0.3667 |
| SD | 0.2526 | 0.2447 | 3.792 | 1.0662 |
| Interaction with the Robot | Interest in the Robot | Additional Movements | ||
|---|---|---|---|---|
| N | 30 | 30 | 30 | 30 |
| Mean | 0.8726 | 0.0878 | 11.97 | 4.6 |
| SD | 0.3169 | 0.1846 | 4.810 | 4.4225 |
| Visual Contact | Motor Activity | Expression of Gestures | Spontaneous Expression | Emotional Reactions | |
|---|---|---|---|---|---|
| N | 30 | 30 | 30 | 30 | 30 |
| Mean | 4.1333 | 2.0667 | 0.3333 | 0.6333 | 0.4667 |
| Visual Contact | Motor Activity | Expression of Gestures | Spontaneous Expression | Emotional Reactions | |
|---|---|---|---|---|---|
| N | 30 | 30 | 30 | 30 | 30 |
| Mean | 3.9333 | 3.3000 | 1.8667 | 0.8000 | 2.0667 |
References
- Frith, U. Autism: Explaining the Enigma; Blackwell Publishing: Hoboken, NJ, USA, 2003. [Google Scholar]
- Schopler, E.; Mesibov, G.B. Communication Problems in Autism; Springer Science & Business Media: Berlin/Heidelberg, Germany, 1985. [Google Scholar]
- Fletcher, P.; Happe, F.; Frith, U.; Baker, S.; Dolan, R.; Frackowiak, R.; Frith, C. Other minds in the brain: A functional imaging study of “theory of mind” in story comprehension. Cognition 1995, 57, 109–128. [Google Scholar] [CrossRef] [Green Version]
- Ochs, E.; Kremer-Sadlik, T.; Sirota, K.G.; Solomon, O. Autism and the social world: An anthropological perspective. Discourse Stud. 2004, 6, 147–183. [Google Scholar] [CrossRef]
- Eigsti, I.M.; Schuh, J.; Mencl, E.; Schultz, R.T.; Paul, R. The neural underpinnings of prosody in autism. Child Neuropsychol. 2012, 18, 600–617. [Google Scholar] [CrossRef]
- de Bildt, A.; Sytema, S.; Zander, E.; Bölte, S.; Sturm, H.; Yirmiya, N.; Yaari, M.; Charman, T.; Salomone, E.; LeCouteur, A.; et al. Autism Diagnostic Interview-Revised (ADI-R) Algorithms for Toddlers and Young Preschoolers: Application in a Non-US Sample of 1,104 Children. J. Autism Dev. Disord. 2015, 45, 2076–2091. [Google Scholar] [CrossRef] [Green Version]
- Kamio, Y.; Haraguchi, H.; Stickley, A.; Ogino, K.; Ishitobi, M.; Takahashi, H. Brief Report: Best Discriminators for Identifying Children with Autism Spectrum Disorder at an 18-Month Health Check-Up in Japan. J. Autism Dev. Disord. 2015, 45, 4147–4153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dix, L.; Fallows, R.; Murphy, G. Effectiveness of the ADEC as a Level 2 screening test for young children with suspected autism spectrum disorders in a clinical setting. J. Intellect. Dev. Disabil. 2015, 40, 179–188. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J. Autism Dev. Disord. 1994, 24, 659–685. [Google Scholar] [CrossRef]
- Robins, D.; Fein, D.; Barton, M. Follow-Up Interview for the Modified Checklist for Autism in Toddlers; (Self-Published). 1999. Available online: www.mchatscreen.com (accessed on 1 May 2022).
- Schopler, E.; Van Bourgondien, M.; Wellman, J.; Love, S. Childhood autism rating scale—Second edition (CARS2): Manual. In Los Angeles: Western Psychological Services; WPS: Torrance, CA, USA, 2010. [Google Scholar]
- Goldstein, S.; Naglieri, J.A. Autism Spectrum Rating Scales: ASRS; Multi-Health Systems: North Tonawanda, NY, USA, 2010. [Google Scholar]
- Lord, C.; Rutter, M.; DiLavore, P.; Risi, S.; Gotham, K.; Bishop, S. ADOS-2; Manual (Part I): Modules; Schedule ADOS Autism Diagnostic Observation: Abu Dhabi, United Arab Emirates, 2015; pp. 1–4. [Google Scholar]
- Scassellati, B. Quantitative metrics of social response for autism diagnosis. In Proceedings of the IEEE International Workshop on Robot and Human Interactive Communication (ROMAN), Nashville, TN, USA, 13–15 August 2005; pp. 585–590. [Google Scholar]
- Scassellati, B. How Social Robots Will Help Us to Diagnose, Treat, and Understand Autism. In Robotics Research; Thrun, S., Brooks, R., Durrant-Whyte, H., Eds.; Springer: Berlin/Heidelberg, Germany, 2007; pp. 552–563. [Google Scholar]
- Scassellati, B.; Admoni, H.; Matarić, M. Robots for Use in Autism Research. Annu. Rev. Biomed. Eng. 2012, 14, 275–294. [Google Scholar] [CrossRef] [Green Version]
- Petric, F. Robotic Autism Spectrum Disorder Diagnostic Protocol: Basis for Cognitive and Interactive Robotic Systems. 2014. Available online: https://www.fer.unizg.hr/_download/repository/KDI_Frano_Petric.pdf (accessed on 10 February 2018).
- Petric, F.; Miklic, D.; Kovacic, Z. Robot-assisted Autism Spectrum Disorder Diagnostics Using POMDPs. In Proceedings of the Companion of the 2017 ACM/IEEE International Conference on Human-Robot Interaction, Vienna, Austria, 6–9 March 2017; ACM: New York, NY, USA, 2017; pp. 369–370. [Google Scholar] [CrossRef]
- Ramirez-Duque, A.A.; Frizera-Neto, A.; Bastes, T.F. Robot-Assisted Diagnosis for Children with Autism Spectrum Disorder Based on Automated Analysis of Nonverbal Cues. In Proceedings of the 2018 7th IEEE International Conference on Biomedical Robotics and Biomechatronics (Biorob), Enschede, The Netherlands, 26–29 August 2018; pp. 456–461. [Google Scholar] [CrossRef]
- Nomura, M.; Kucharek, N.; Zubrycki, I.; Granosik, G.; Morita, Y. Adjustability for Grasping Force of Patients with Autism by iWakka: A Pilot Study. In Proceedings of the 2019 12th International Workshop on Robot Motion and Control (RoMoCo), Poznan, Poland, 8–10 July 2019; pp. 50–55. [Google Scholar] [CrossRef]
- Dutta, V.; Zielińska, T. An Adversarial Explainable Artificial Intelligence (XAI) Based Approach for Action Forecasting. J. Autom. Mob. Robot. Intell. Syst. 2021, 14, 3–10. [Google Scholar] [CrossRef]
- Dautenhahn, K.; Werry, I. Towards interactive robots in autism therapy: Background, motivation and challenges. Pragmat. Cogn. 2004, 12, 1–35. [Google Scholar] [CrossRef]
- Robins, B.; Dautenhahn, K.; Ferrari, E.; Kronreif, G.; Prazak-Aram, B.; Marti, P.; Iacono, I.; Gelderblom, G.J.; Bernd, T.; Caprino, F.; et al. Scenarios of Robot Assisted Play for Children with Cognitive and Physical Disabilities. Interact. Stud. 2012, 13, 189. [Google Scholar] [CrossRef] [Green Version]
- Diehl, J.J.; Schmitt, L.M.; Villano, M.; Crowell, C.R. The clinical use of robots for individuals with Autism Spectrum Disorders: A critical review. Res. Autism Spectr. Disord. 2012, 6, 249–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esteban, P.G.; Baxter, P.; Belpaeme, T.; Billing, E.; Cai, H.; Cao, H.L.; Coeckelbergh, M.; Costescu, C.; David, D.; Beir, A.D.; et al. How to Build a Supervised Autonomous System for Robot-Enhanced Therapy for Children with Autism Spectrum Disorder. Paladyn, J. Behav. Robot. 2017, 8, 18–38. [Google Scholar] [CrossRef]
- Falconer, J. Nao Robot Goes to School to Help Kids with Autism; IEEE Spectrum: New York, NY, USA, 2013. [Google Scholar]
- Tapus, A.; Peca, A.; Aly, A.; Pop, C.; Jisa, L.; Pineta, S.; Rusu, A.S.; David, D.O. Children with Autism Social Engagement in Interaction with NAO, an Imitative Robot—A Series of Single Case Experiments. Interact. Stud. 2012, 13, 315–347. [Google Scholar] [CrossRef]
- Lytridis, C.; Vrochidou, E.; Chatzistamatis, S.; Kaburlasos, V. Social Engagement Interaction Games Between Children with Autism and Humanoid Robot NAO. In Proceedings of the 13th International Conference on Soft Computing Models in Industrial and Environmental Applications, San Sebastián, Spain, 6–8 June 2018; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar] [CrossRef]
- Robins, B.; Dautenhahn, K. Tactile Interactions with a Humanoid Robot: Novel Play Scenario Implementations with Children with Autism. Int. J. Soc. Robot. 2014, 6, 397–415. [Google Scholar] [CrossRef] [Green Version]
- Zorcec, T.; Robins, B.; Dautenhahn, K. Getting Engaged: Assisted Play with a Humanoid Robot Kaspar for Children with Severe Autism. In ICT Innovations 2018. Engineering and Life Sciences; Kalajdziski, S., Ackovska, N., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 198–207. [Google Scholar]
- Bernardo, B.; Alves-Oliveira, P.; Santos, M.G.; Melo, F.S.; Paiva, A. An Interactive Tangram Game for Children with Autism. In Proceedings of the 16th International Conference on Intelligent Virtual Agents, Los Angeles, CA, USA, 20–23 September 2016. [Google Scholar]
- Brok, J.C.J.; Barakova, E.I. Engaging Autistic Children in Imitation and Turn-Taking Games with Multiagent System of Interactive Lighting Blocks. In Entertainment Computing—ICEC 2010; Yang, H.S., Malaka, R., Hoshino, J., Han, J.H., Eds.; Springer: Berlin/Heidelberg, Germany, 2010; pp. 115–126. [Google Scholar]
- Kose-Bagci, H.; Dautenhahn, K.; Nehaniv, C.L. Emergent dynamics of turn-taking interaction in drumming games with a humanoid robot. In Proceedings of the RO-MAN 2008—The 17th IEEE International Symposium on Robot and Human Interactive Communication, Munich, Germany, 1–3 August 2008; pp. 346–353. [Google Scholar] [CrossRef] [Green Version]
- Iacono, I.; Lehmann, H.; Marti, P.; Robins, B.; Dautenhahn, K. Robots as social mediators for children with Autism—A preliminary analysis comparing two different robotic platforms. In Proceedings of the 2011 IEEE International Conference on Development and Learning (ICDL), Frankfurt am Main, Germany, 24–27 August 2011; Volume 2, pp. 1–6. [Google Scholar] [CrossRef]
- Kim, S.; Clarke, E. Case study: An iPad-based intervention on turn-taking behaviors in preschoolers with autism. Behav. Dev. Bull. 2015, 20, 253–264. [Google Scholar] [CrossRef] [Green Version]
- Wood, L.J.; Zaraki, A.; Robins, B.; Dautenhahn, K. Developing Kaspar: A Humanoid Robot for Children with Autism. Int. J. Soc. Robot. 2021, 13, 491–508. [Google Scholar] [CrossRef] [Green Version]
- Arent, K.; Kabała, M.; Wnuk, M. Towards the therapeutic spherical robot: Design, programming and control. In Proceedings of the Eighth International IFAC Symposium on Robot Control; Elsevier: Oxford, UK, 2006. [Google Scholar]
- Arent, K.; Wnuk, M. Remarks on Behaviours Programming of the Interactive Therapeutic Robot Koala Based on Fuzzy Logic Techniques. In Agent and Multi-Agent Systems: Technologies and Applications; Nguyen, N.T., Grzech, A., Howlett, R.J., Jain, L.C., Eds.; Springer: Berlin/Heidelberg, Germany, 2007; pp. 568–577. [Google Scholar]
- Arent, K.; Gakis, M.; Sobecki, J.; Szczepanowski, R. Toward emotion recognition embodied in social robots: Implementation of Laban movement analysis into NAO robot. J. Autom. Mob. Robot. Intell. Syst. 2017, 11, 3–6. [Google Scholar] [CrossRef]
- Czyżewska, B.I. Applications of NAO Robot in Therapy and Education of Children with Intellectual Disabilities and Autism. Master’s Thesis, Wroclaw University of Science and Technology, Wroclaw, Poland, 2016. (In Polish). [Google Scholar]
- Arent, K.; Kruk-Lasocka, J.; Niemiec, T.; Szczepanowski, R. Social robot in diagnosis of autism among preschool children. In Proceedings of the 24th International Conference on Methods and Models in Automation and Robotics, Miedzyzdroje, Poland, 26–29 August 2019. [Google Scholar]
- Goldstein, S.; Ozonoff, S. Assessment of Autism Spectrum Disorder; Guilford Publications: New York, NY, USA, 2018. [Google Scholar]
- DSM-5; Diagnostic and Statistical Manual of Mental Disorders. American Publishing Association: Chicago, IL, USA, 2013.
- Wing, L.; Leekam, S.R.; Libby, S.J.; Gould, J.; Larcombe, M. The diagnostic interview for social and communication disorders: Background, inter-rater reliability and clinical use. J. Child Psychol. Psychiatry 2002, 43, 307–325. [Google Scholar] [CrossRef] [Green Version]
- Marvin, A.R.; Marvin, D.J.; Lipkin, P.H.; Law, J.K. Analysis of Social Communication Questionnaire (SCQ) screening for children less than age 4. Curr. Dev. Disord. Rep. 2017, 4, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Watson, L.R.; Baranek, G.T.; Crais, E.R.; Reznick, J.S.; Dykstra, J.; Perryman, T. The first year inventory: Retrospective parent responses to a questionnaire designed to identify one-year-olds at risk for autism. J. Autism Dev. Disord. 2007, 37, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.H.; Rodgers, J.; McConachie, H. Restricted and Repetitive Behaviours, Sensory Processing and Cognitive Style in Children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2009, 39, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, R.A.; Siemann, J.K.; Schneider, B.C.; Eberly, H.E.; Woynaroski, T.G.; Camarata, S.M.; Wallace, M.T. Multisensory Temporal Integration in Autism Spectrum Disorders. J. Neurosci. 2014, 34, 691–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Rater No | Me (Touch me) | Me (Dance with me) | H(2) | p |
|---|---|---|---|---|
| 1 | 1.056 | 0.005 | 13.377 | 0.0003 |
| 2 | 1.000 | 0.066 | 14.925 | 0.0001 |
| 3 | 0.955 | 0.041 | 14.004 | 0.0002 |
| 4 | 0.955 | 0.036 | 14.560 | 0.0001 |
| 5 | 1.100 | 0.020 | 13.418 | 0.0002 |
| 6 | 0.838 | 0.071 | 13.866 | 0.0002 |
| Child’s Diagnosis | ||
|---|---|---|
| Typical Development | Autism | |
| commands executed | 29 | 7 |
| commands not executed | 1 | 23 |
| Child’s Diagnosis | ||
|---|---|---|
| Typically Developing | Autism | |
| commands executed | 23 | 7 |
| commands not executed | 7 | 23 |
| Measure | Diagnosis | Me | Comparison Results |
|---|---|---|---|
| Interest in the robot | Autism | 13 | Mann–Whitney , |
| Typically developing | 7 | ||
| Additional movements | Autism | 4 | Mann–Whitney , |
| Typical development | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arent, K.; Brown, D.J.; Kruk-Lasocka, J.; Niemiec, T.L.; Pasieczna, A.H.; Standen, P.J.; Szczepanowski, R. The Use of Social Robots in the Diagnosis of Autism in Preschool Children. Appl. Sci. 2022, 12, 8399. https://doi.org/10.3390/app12178399
Arent K, Brown DJ, Kruk-Lasocka J, Niemiec TL, Pasieczna AH, Standen PJ, Szczepanowski R. The Use of Social Robots in the Diagnosis of Autism in Preschool Children. Applied Sciences. 2022; 12(17):8399. https://doi.org/10.3390/app12178399
Chicago/Turabian StyleArent, Krzysztof, David J. Brown, Joanna Kruk-Lasocka, Tomasz Lukasz Niemiec, Aleksandra Helena Pasieczna, Penny J. Standen, and Remigiusz Szczepanowski. 2022. "The Use of Social Robots in the Diagnosis of Autism in Preschool Children" Applied Sciences 12, no. 17: 8399. https://doi.org/10.3390/app12178399
APA StyleArent, K., Brown, D. J., Kruk-Lasocka, J., Niemiec, T. L., Pasieczna, A. H., Standen, P. J., & Szczepanowski, R. (2022). The Use of Social Robots in the Diagnosis of Autism in Preschool Children. Applied Sciences, 12(17), 8399. https://doi.org/10.3390/app12178399