
An MRI-Based Patient-Specific Computational Framework for the Calculation of Range of Motion of Total Hip Replacements

 ,
,
Abstract
1. Introduction
2. Materials and Methods
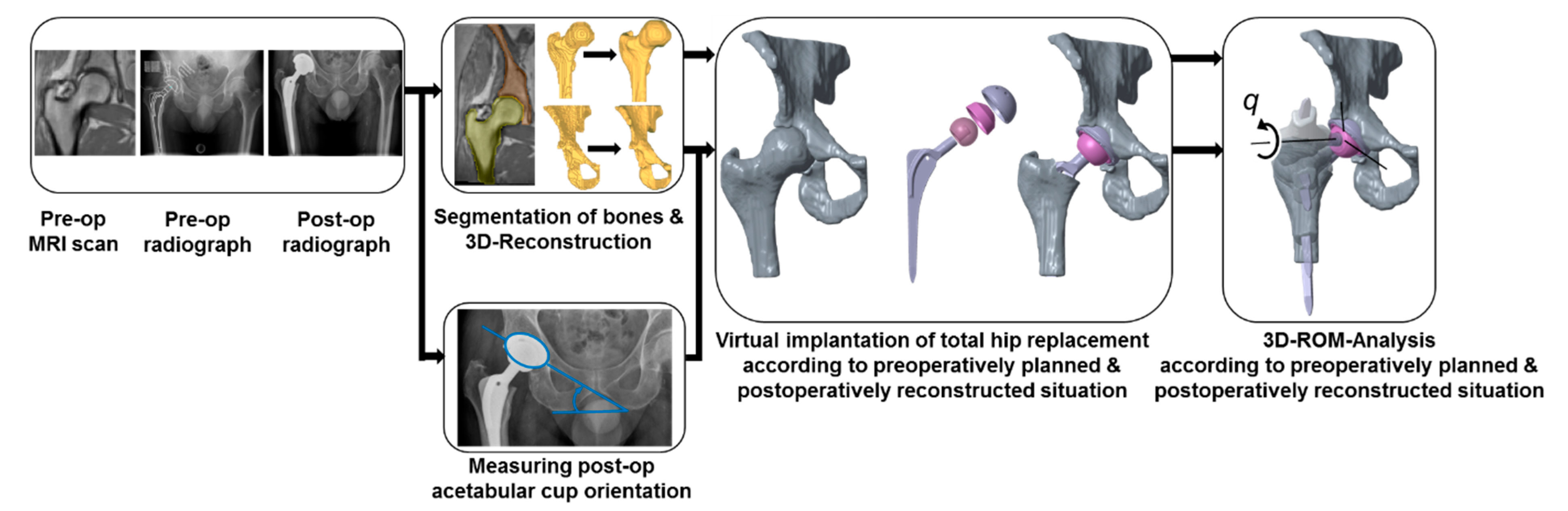
2.1. Overview of the Deployed Framework
2.2. Geometry Data Acquisition
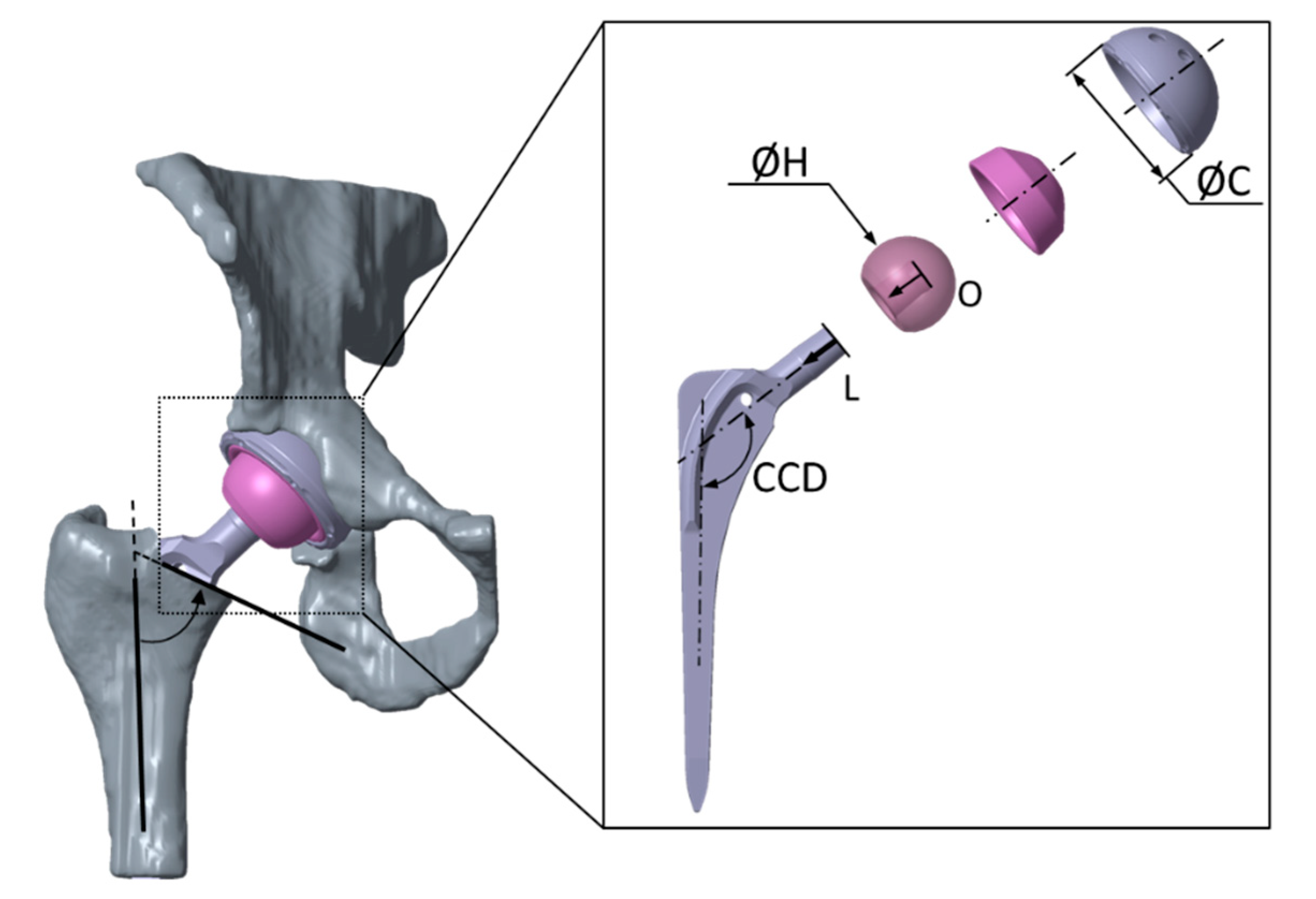
2.3. Preoperatively Planned Situation
2.4. Postoperatively Reconstructed Situation
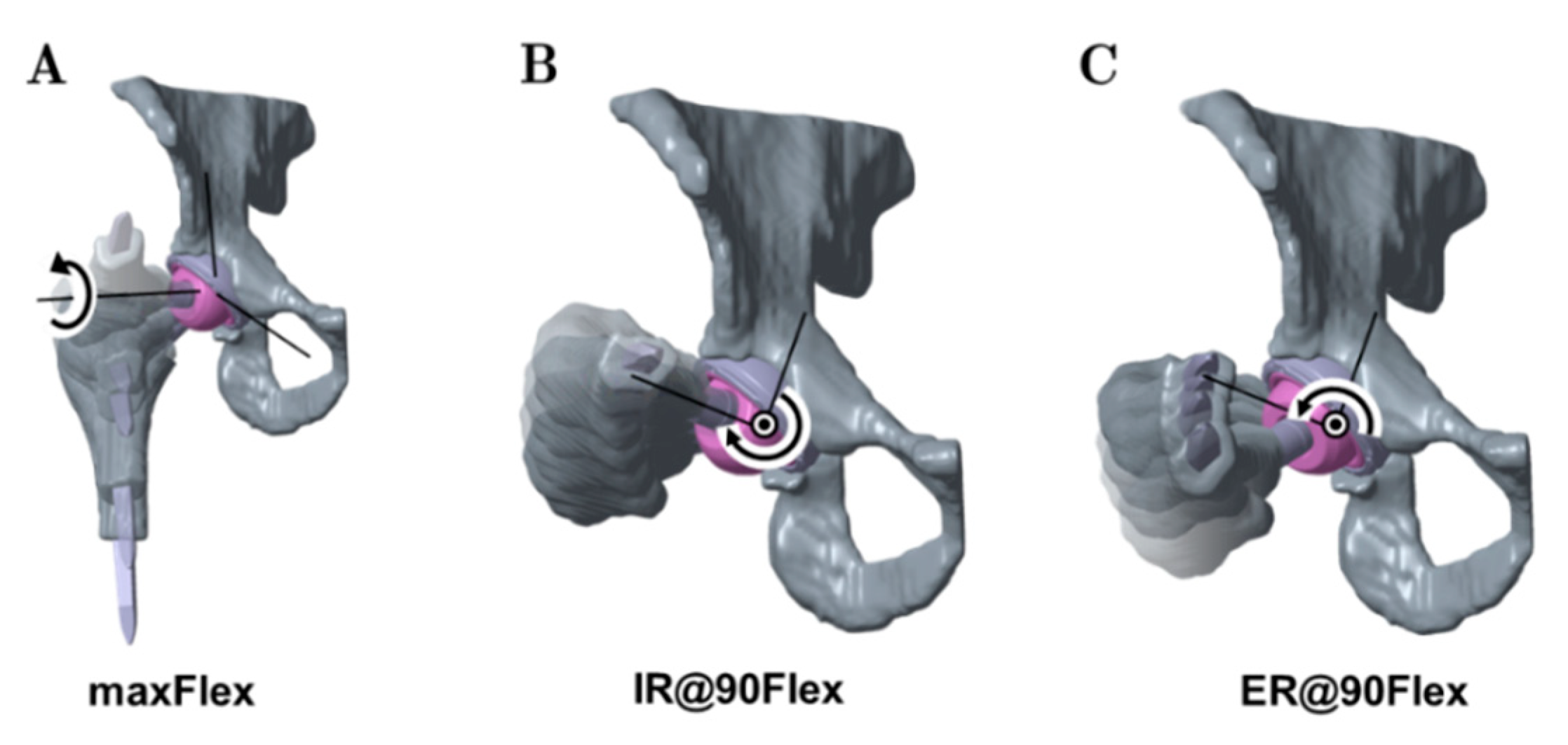
2.5. Analysis of Range of Motion
2.6. Analyzed Parameters
2.7. Statistical Metrics
3. Results
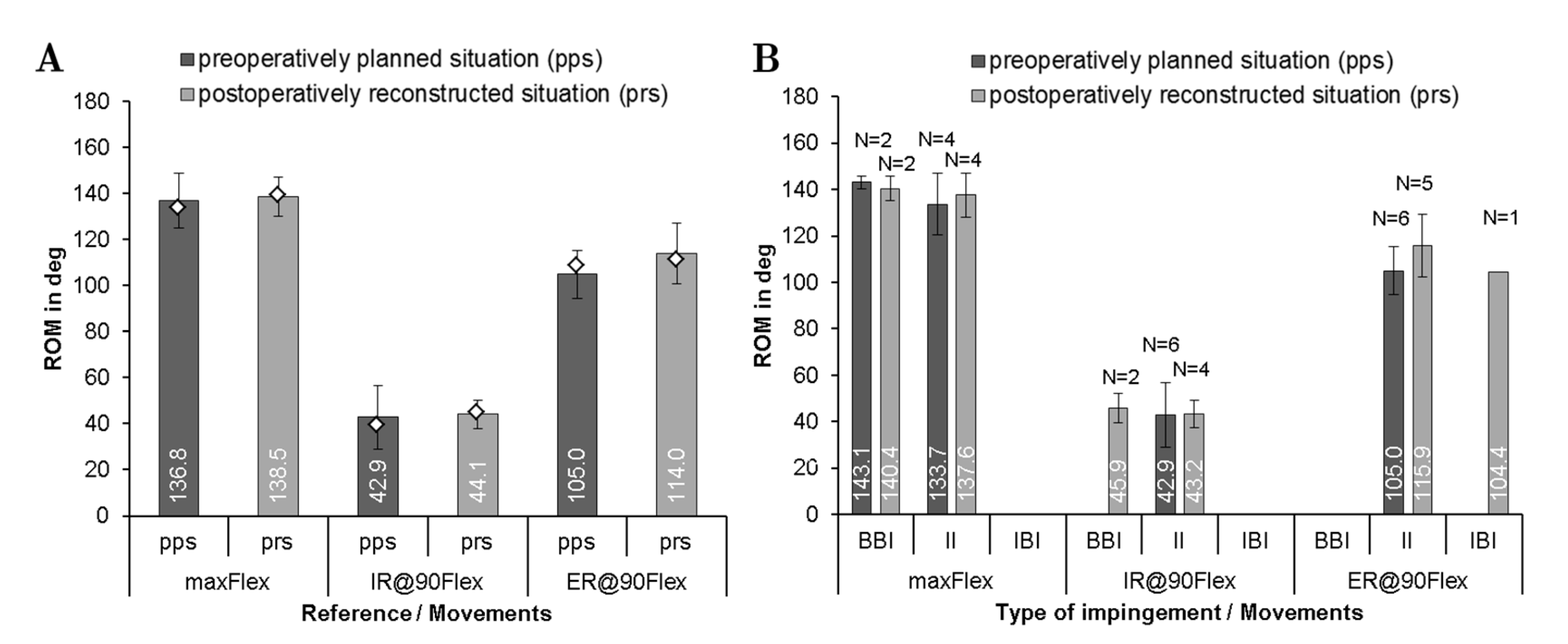
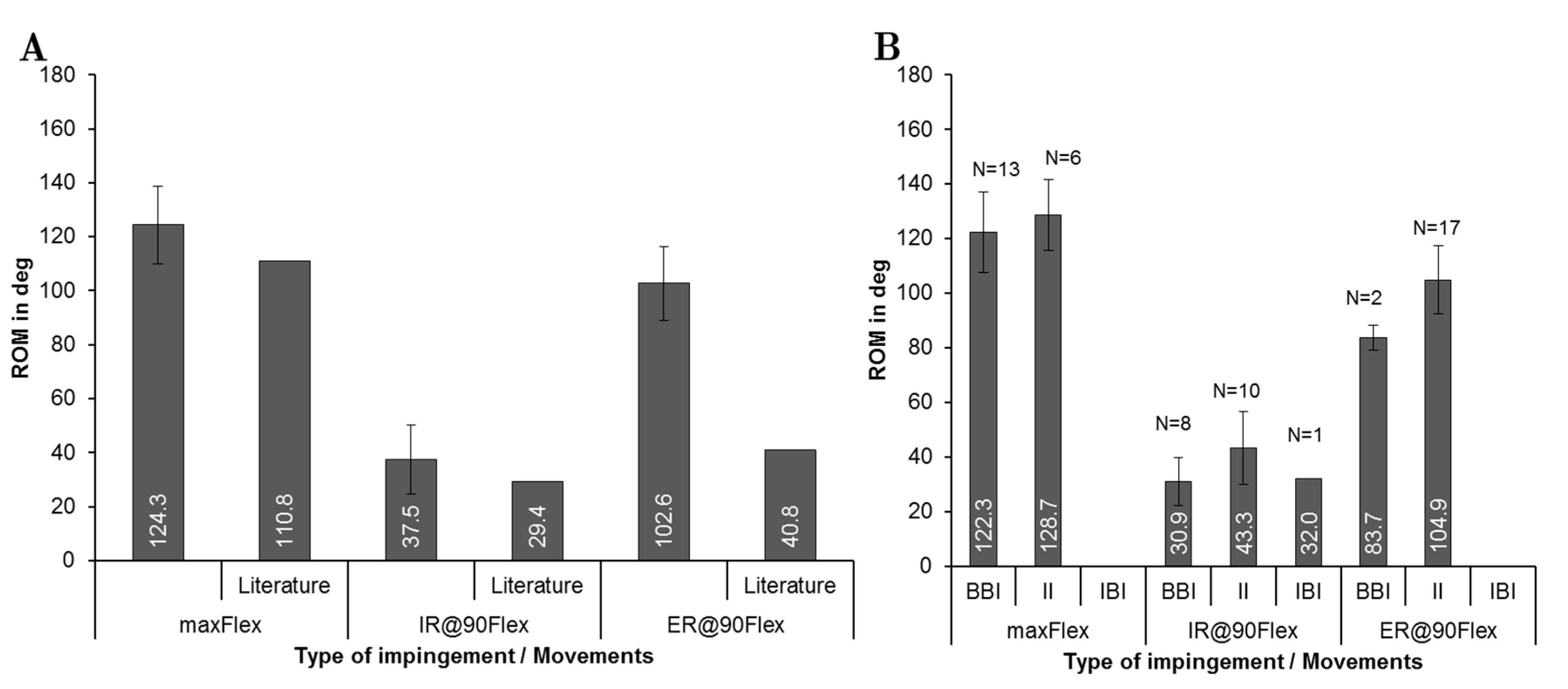
3.1. Comparison of ROM and Predominant Impingement Type between the Preoperatively Planned and Postoperatively Reconstructed Situation
3.2. Investigation of ROM and Predominant Impingement Type for the Preoperatively Planned Situation
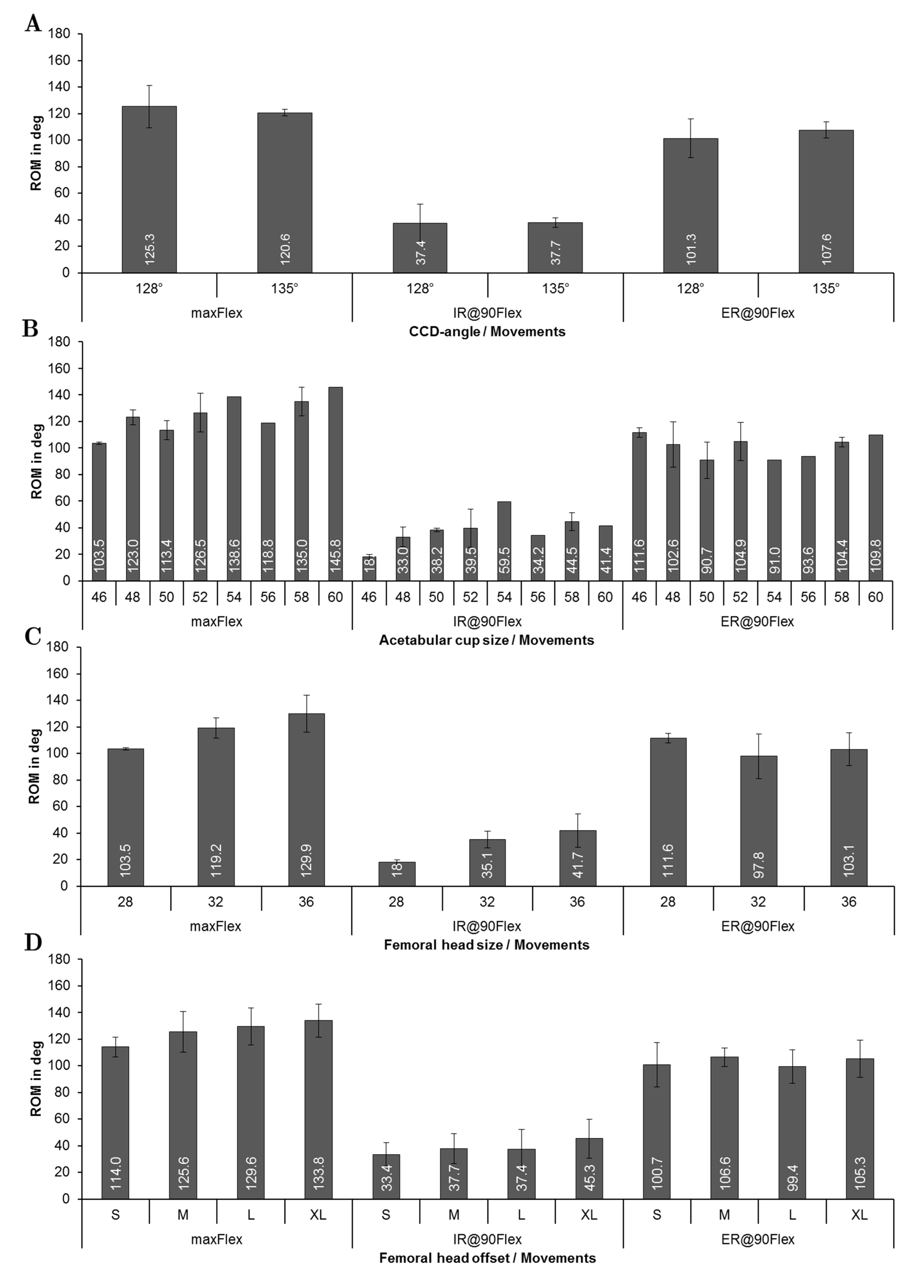
3.3. Influence of Implant Related Factors on ROM for the Preoperatively Planned Situation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brown, T.D.; Elkins, J.M.; Pedersen, D.R.; Callaghan, J.J. Impingement and Dislocation in Total HIP Arthroplasty: Mechanisms and Consequences. Iowa Orthop. J. 2014, 34, 1–15. [Google Scholar]
- Klauber, J.; Geraedts, M.; Friedrich, J.; Wasem, J. Krankenhaus-Report 2019; Springer: Berlin/Heidelberg, Germany, 2019; ISBN 978-3-662-58224-4. [Google Scholar]
- Organisation for Economic Co-operation and Development. Health at a Glance 2017: OECD Indicators; OECD Publishing: Paris, France, 2017; ISBN 9264280405. [Google Scholar]
- Maradit Kremers, H.; Larson, D.R.; Crowson, C.S.; Kremers, W.K.; Washington, R.E.; Steiner, C.A.; Jiranek, W.A.; Berry, D.J. Prevalence of Total Hip and Knee Replacement in the United States. J. Bone Jt. Surg. Am. 2015, 97, 1386–1397. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Ong, K.L.; Lau, E.; Bozic, K.J. Impact of the economic downturn on total joint replacement demand in the United States: Updated projections to 2021. J. Bone Jt. Surg. Am. 2014, 96, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Wolford, M.L.; Palso, K.; Bercovitz, A. Hospitalization for Total Hip Replacement Among Inpatients Aged 45 and Over: United States, 2000–2010; Data Brief; Centers for Disease Control & Prevention: Atlanta, GA, USA, 2015; pp. 1–8. [Google Scholar]
- Pilz, V.; Hanstein, T.; Skripitz, R. Projections of primary hip arthroplasty in Germany until 2040. Acta Orthop. 2018, 89, 308–313. [Google Scholar] [CrossRef]
- Gwam, C.U.; Mistry, J.B.; Mohamed, N.S.; Thomas, M.; Bigart, K.C.; Mont, M.A.; Delanois, R.E. Current Epidemiology of Revision Total Hip Arthroplasty in the United States: National Inpatient Sample 2009 to 2013. J. Arthroplast. 2017, 32, 2088–2092. [Google Scholar] [CrossRef] [PubMed]
- Jamari, J.; Anwar, I.B.; Saputra, E.; van der Heide, E. Range of Motion Simulation of Hip Joint Movement during Salat Activity. J. Arthroplast. 2017, 32, 2898–2904. [Google Scholar] [CrossRef]
- Sugano, N.; Tsuda, K.; Miki, H.; Takao, M.; Suzuki, N.; Nakamura, N. Dynamic measurements of hip movement in deep bending activities after total hip arthroplasty using a 4-dimensional motion analysis system. J. Arthroplast. 2012, 27, 1562–1568. [Google Scholar] [CrossRef]
- Nakamura, N.; Maeda, Y.; Hamawaki, M.; Sakai, T.; Sugano, N. Effect of soft-tissue impingement on range of motion during posterior approach Total Hip Arthroplasty: An in vivo measurement study. Comput. Assist. Surg. 2016, 21, 132–136. [Google Scholar] [CrossRef]
- Amstutz, H.C.; Lodwig, R.M.; Schurman, D.J.; Hodgson, A.G. Range of motion studies for total hip replacements. A comparative study with a new experimental apparatus. Clin. Orthop. Relat. Res. 1975, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Scifert, C.F.; Brown, T.D.; Pedersen, D.R.; Callaghan, J.J. A finite element analysis of factors influencing total hip dislocation. Clin. Orthop. Relat. Res. 1998, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Miki, H.; Kyo, T.; Kuroda, Y.; Nakahara, I.; Sugano, N. Risk of edge-loading and prosthesis impingement due to posterior pelvic tilting after total hip arthroplasty. Clin. Biomech. 2014, 29, 607–613. [Google Scholar] [CrossRef]
- Zhang, J.; Wei, J.; Mao, Y.; Li, H.; Xie, Y.; Zhu, Z. Range of Hip Joint Motion in Developmental Dysplasia of the Hip Patients Following Total Hip Arthroplasty With the Surgical Technique Using the Concept of Combined Anteversion: A Study of Crowe I and II Patients. J. Arthroplast. 2015, 30, 2248–2255. [Google Scholar] [CrossRef]
- Malik, A.; Maheshwari, A.; Dorr, L.D. Impingement with total hip replacement. J. Bone Jt. Surg. Am. 2007, 89, 1832–1842. [Google Scholar] [CrossRef] [PubMed]
- Karachalios, T.; Komnos, G.; Koutalos, A. Total hip arthroplasty: Survival and modes of failure. EFORT Open Rev. 2018, 3, 232–239. [Google Scholar] [CrossRef]
- Kluess, D.; Zietz, C.; Lindner, T.; Mittelmeier, W.; Schmitz, K.-P.; Bader, R. Limited range of motion of hip resurfacing arthroplasty due to unfavorable ratio of prosthetic head size and femoral neck diameter. Acta Orthop. 2008, 79, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Scheerlinck, T. Cup positioning in total hip arthroplasty. Acta Orthop. Belg. 2014, 80, 336–347. [Google Scholar] [PubMed]
- Nadzadi, M.E.; Pedersen, D.R.; Yack, H.J.; Callaghan, J.J.; Brown, T.D. Kinematics, kinetics, and finite element analysis of commonplace maneuvers at risk for total hip dislocation. J. Biomech. 2003, 36, 577–591. [Google Scholar] [CrossRef]
- Kluess, D.; Martin, H.; Mittelmeier, W.; Schmitz, K.-P.; Bader, R. Influence of femoral head size on impingement, dislocation and stress distribution in total hip replacement. Med. Eng. Phys. 2007, 29, 465–471. [Google Scholar] [CrossRef]
- Shon, W.Y.; Baldini, T.; Peterson, M.G.; Wright, T.M.; Salvati, E.A. Impingement in total hip arthroplasty a study of retrieved acetabular components. J. Arthroplast. 2005, 20, 427–435. [Google Scholar] [CrossRef]
- Palit, A.; King, R.; Hart, Z.; Gu, Y.; Pierrepont, J.; Elliott, M.T.; Williams, M.A. Bone-to-Bone and Implant-to-Bone Impingement: A Novel Graphical Representation for Hip Replacement Planning. Ann. Biomed. Eng. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bader, R.; Scholz, R.; Steinhauser, E.; Busch, R.; Mittelmeier, W. Methode zur Evaluierung von Einflussfaktoren auf die Luxationsstabilität von künstlichen Hüftgelenken. Biomed. Tech. 2004, 49, 137–144. [Google Scholar] [CrossRef]
- Burroughs, B.R.; Hallstrom, B.; Golladay, G.J.; Hoeffel, D.; Harris, W.H. Range of motion and stability in total hip arthroplasty with 28-, 32-, 38-, and 44-mm femoral head sizes. J. Arthroplast. 2005, 20, 11–19. [Google Scholar] [CrossRef]
- Qurashi, S.; Parr, W.; Jang, B.; Walsh, W.R. Elevated lip liner positions improving stability in total hip arthroplasty. An experimental study. JISRF 2017, 7. [Google Scholar] [CrossRef]
- Geier, A.; Kluess, D.; Grawe, R.; Herrmann, S.; D’Lima, D.; Woernle, C.; Bader, R. Dynamical analysis of dislocation-associated factors in total hip replacements by hardware-in-the-loop simulation. J. Orthop. Res. 2017, 35, 2557–2566. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, S.; Kluess, D.; Kaehler, M.; Grawe, R.; Rachholz, R.; Souffrant, R.; Zierath, J.; Bader, R.; Woernle, C. A Novel Approach for Dynamic Testing of Total Hip Dislocation under Physiological Conditions. PLoS ONE 2015, 10, e0145798. [Google Scholar] [CrossRef] [PubMed]
- Bader, R.; Scholz, R.; Steinhauser, E.; Zimmermann, S.; Busch, R.; Mittelmeier, W. The influence of head and neck geometry on stability of total hip replacement: A mechanical test study. Acta Orthop. Scand. 2004, 75, 415–421. [Google Scholar] [CrossRef]
- Bader, R.; Steinhauser, E.; Gradinger, R.; Willmann, G.; Mittelmeier, W. Computergestützte Bewegungssimulation an Hüftendoprothesen mit Keramik-Keramik-Gleitpaarung. Analyse der Einflussparameter Implantat-Design und Position. Z. Orthop. Grenzgeb. 2002, 140, 310–316. [Google Scholar] [CrossRef]
- Pedersen, D.R.; Callaghan, J.J.; Brown, T.D. Activity-dependence of the “safe zone” for impingement versus dislocation avoidance. Med. Eng. Phys. 2005, 27, 323–328. [Google Scholar] [CrossRef]
- Putame, G.; Pascoletti, G.; Franceschini, G.; Dichio, G.; Terzini, M. Prosthetic Hip ROM from Multibody Software Simulation. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 5386–5389. [Google Scholar] [CrossRef]
- Zanetti, E.M.; Bignardi, C.; Terzini, M.; Putame, G.; Audenino, A.L. A multibody model for the optimization of hip arthroplasty in relation to range of movement. AMJ 2018, 11. [Google Scholar] [CrossRef]
- Chang, T.-C.; Kang, H.; Arata, L.; Zhao, W. A pre-operative approach of range of motion simulation and verification for femoroacetabular impingement. Int. J. Med. Robot. 2011, 7, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Miki, H.; Kyo, T.; Sugano, N. Anatomical hip range of motion after implantation during total hip arthroplasty with a large change in pelvic inclination. J. Arthroplast. 2012, 27, 1641–1650.e1. [Google Scholar] [CrossRef]
- Klingenstein, G.G.; Yeager, A.M.; Lipman, J.D.; Westrich, G.H. Computerized range of motion analysis following dual mobility total hip arthroplasty, traditional total hip arthroplasty, and hip resurfacing. J. Arthroplast. 2013, 28, 1173–1176. [Google Scholar] [CrossRef]
- Weber, M.; Woerner, M.; Craiovan, B.; Voellner, F.; Worlicek, M.; Springorum, H.-R.; Grifka, J.; Renkawitz, T. Current standard rules of combined anteversion prevent prosthetic impingement but ignore osseous contact in total hip arthroplasty. Int. Orthop. 2016, 40, 2495–2504. [Google Scholar] [CrossRef]
- Widmer, K.-H. Impingementfreie Bewegung nach Hüft-TEP—Wie realisieren? Z. Orthop. Unfallchir. 2016, 154, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Kummer, F.J.; Shah, S.; Iyer, S.; DiCesare, P.E. The effect of acetabular cup orientations on limiting hip rotation. J. Arthroplast. 1999, 14, 509–513. [Google Scholar] [CrossRef]
- Bader, R.; Willmann, G. Keramische Pfannen für Hüftendoprothesen. Teil 6: Pfannendesign, Inklinations- und Antetorsionswinkel beeinflussen Bewegungsumfang und Impingement. Biomed. Tech. 1999, 44, 212–219. [Google Scholar] [CrossRef]
- Widmer, K.-H. The Impingement-free, Prosthesis-specific, and Anatomy-adjusted Combined Target Zone for Component Positioning in THA Depends on Design and Implantation Parameters of both Components. Clin. Orthop. Relat. Res. 2020, 478, 1904–1918. [Google Scholar] [CrossRef]
- Fischer, M.C.M.; Tokunaga, K.; Okamoto, M.; Habor, J.; Radermacher, K. Preoperative factors improving the prediction of the postoperative sagittal orientation of the pelvis in standing position after total hip arthroplasty. Sci. Rep. 2020, 10, 15944. [Google Scholar] [CrossRef] [PubMed]
- Ezquerra, L.; Quilez, M.P.; Pérez, M.Á.; Albareda, J.; Seral, B. Range of Movement for Impingement and Dislocation Avoidance in Total Hip Replacement Predicted by Finite Element Model. J. Med. Biol. Eng. 2017, 37, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Kliewe, C.; Souffrant, R.; Kluess, D.; Woernle, C.; Brökel, K.; Bader, R. Analytisches Berechnungsmodell zur Bestimmung des Einflusses konstruktiver und operativer Faktoren auf den Bewegungsumfang von Hüftendoprothesen. Biomed. Tech. 2010, 55, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Yoshimine, F. The safe-zones for combined cup and neck anteversions that fulfill the essential range of motion and their optimum combination in total hip replacements. J. Biomech. 2006, 39, 1315–1323. [Google Scholar] [CrossRef]
- Rodriguez-Elizalde, S.; Yeager, A.M.; Ravi, B.; Lipman, J.D.; Salvati, E.A.; Westrich, G.H. Computerized virtual surgery demonstrates where acetabular rim osteophytes most reduce range of motion following total hip arthroplasty. HSS J. 2013, 9, 223–228. [Google Scholar] [CrossRef]
- Shoji, T.; Yasunaga, Y.; Yamasaki, T.; Izumi, S.; Hachisuka, S.; Ochi, M. Low femoral antetorsion as a risk factor for bony impingement after bipolar hemiarthroplasty. J. Orthop. Surg. Res. 2015, 10, 105. [Google Scholar] [CrossRef]
- Brown, T.D.; Callaghan, J.J. Impingement in Total Hip Replacement: Mechanisms and Consequences. Curr. Orthop. 2008, 22, 376–391. [Google Scholar] [CrossRef] [PubMed]
- Hariri, S.; Chun, S.; Cowan, J.B.; Bragdon, C.; Malchau, H.; Rubash, H.E. Range of motion in a modular femoral stem system with a variety of neck options. J. Arthroplast. 2013, 28, 1625–1633. [Google Scholar] [CrossRef]
- Herrlin, K.; Selvik, G.; Pettersson, H.; Lidgren, L. Range of motion caused by design of the total hip prosthesis. Acta Radiologica 1988, 29, 701–704. [Google Scholar] [CrossRef] [PubMed]
- Widmer, K.-H.; Majewski, M. The impact of the CCD-angle on range of motion and cup positioning in total hip arthroplasty. Clin. Biomech. 2005, 20, 723–728. [Google Scholar] [CrossRef]
- Matsushita, A.; Nakashima, Y.; Jingushi, S.; Yamamoto, T.; Kuraoka, A.; Iwamoto, Y. Effects of the femoral offset and the head size on the safe range of motion in total hip arthroplasty. J. Arthroplast. 2009, 24, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Bader, R.; Klüss, D.; Gerdesmeyer, L.; Steinhauser, E. Biomechanische Aspekte zur Implantatverankerung und Kinematik von Oberflächenersatzhüftendoprothesen. Der Orthopäde 2008, 37, 634–643. [Google Scholar] [CrossRef]
- Han, S.; Owens, V.L.; Patel, R.V.; Ismaily, S.K.; Harrington, M.A.; Incavo, S.J.; Noble, P.C. The continuum of hip range of motion: From soft-tissue restriction to bony impingement. J. Orthop. Res. 2020, 38, 1779–1786. [Google Scholar] [CrossRef]
- Kouyoumdjian, P.; Coulomb, R.; Sanchez, T.; Asencio, G. Clinical evaluation of hip joint rotation range of motion in adults. Orthop. Traumatol. Surg. Res. 2012, 98, 17–23. [Google Scholar] [CrossRef]
- Wilson, J.J.; Furukawa, M. Evaluation of the patient with hip pain. Am. Fam. Physician 2014, 89, 27–34. [Google Scholar]
- Kataoka, T.; Oshima, Y.; Iizawa, N.; Majima, T.; Takai, S. Influence of Total Knee Arthroplasty on Hip Rotational Range of Motion. J. Nippon Med. Sch. 2020, 87, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Liaw, C.-K.; Yang, R.-S.; Hou, S.-M.; Wu, T.-Y.; Fuh, C.-S. Measurement of the acetabular cup anteversion on simulated radiographs. J. Arthroplast. 2009, 24, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Kluess, D.; Souffrant, R.; Mittelmeier, W.; Wree, A.; Schmitz, K.-P.; Bader, R. A convenient approach for finite-element-analyses of orthopaedic implants in bone contact: Modeling and experimental validation. Comput. Methods Programs Biomed. 2009, 95, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Murray, D.W. The definition and measurement of acetabular orientation. J. Bone Jt. Surg. Br. Vol. 1993, 75, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Widmer, K.-H. A simplified method to determine acetabular cup anteversion from plain radiographs. J. Arthroplast. 2004, 19, 387–390. [Google Scholar] [CrossRef] [PubMed]
- Dunlap, K.; Shands, A.R.; Hollister, L.C.; Gaul, J.S.; Streit, H.A. A new method for determination of torsion of the femur. J. Bone Jt. Surg. Am. 1953, 35, 289–311. [Google Scholar] [CrossRef]
- Bartz, R.L.; Nobel, P.C.; Kadakia, N.R.; Tullos, H.S. The effect of femoral component head size on posterior dislocation of the artificial hip joint. J. Bone Jt. Surg. Am. 2000, 82, 1300–1307. [Google Scholar] [CrossRef]
- Tannast, M.; Kubiak-Langer, M.; Langlotz, F.; Puls, M.; Murphy, S.B.; Siebenrock, K.A. Noninvasive three-dimensional assessment of femoroacetabular impingement. J. Orthop. Res. 2007, 25, 122–131. [Google Scholar] [CrossRef]
- Mulholland, S.J.; Wyss, U.P. Activities of daily living in non-Western cultures: Range of motion requirements for hip and knee joint implants. Int. J. Rehabil. Res. 2001, 24, 191–198. [Google Scholar] [CrossRef]
- Gilles, B.; Christophe, F.K.; Magnenat-Thalmann, N.; Becker, C.D.; Duc, S.R.; Menetrey, J.; Hoffmeyer, P. MRI-based assessment of hip joint translations. J. Biomech. 2009, 42, 1201–1205. [Google Scholar] [CrossRef]
- Zheng, G.; von Recum, J.; Nolte, L.-P.; Grützner, P.A.; Steppacher, S.D.; Franke, J. Validation of a statistical shape model-based 2D/3D reconstruction method for determination of cup orientation after THA. Int. J. Comput. Assist. Radiol. Surg. 2012, 7, 225–231. [Google Scholar] [CrossRef]
- Zheng, G. Statistical shape model-based reconstruction of a scaled, patient-specific surface model of the pelvis from a single standard AP x-ray radiograph. Med. Phys. 2010, 37, 1424–1439. [Google Scholar] [CrossRef] [PubMed]
- Shon, W.Y.; Gupta, S.; Biswal, S.; Hur, C.Y.; Jajodia, N.; Hong, S.J.; Myung, J.S. Validation of a simple radiographic method to determine variations in pelvic and acetabular cup sagittal plane alignment after total hip arthroplasty. Skelet. Radiol. 2008, 37, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Yun, H.; Murphy, W.S.; Ward, D.M.; Zheng, G.; Hayden, B.L.; Murphy, S.B. Effect of Pelvic Tilt and Rotation on Cup Orientation in Both Supine and Standing Positions. J. Arthroplast. 2018, 33, 1442–1448. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-H.; Lin, C.-C.; Lu, T.-W.; Hou, S.-M.; Hu, C.-C.; Yeh, L.-S. Evaluation of ranges of motion of a new constrained acetabular prosthesis for canine total hip replacement. Biomed. Eng. Online 2013, 12, 116. [Google Scholar] [CrossRef] [PubMed]
- Cross, M.B.; Nam, D.; Mayman, D.J. Ideal femoral head size in total hip arthroplasty balances stability and volumetric wear. HSS J. 2012, 8, 270–274. [Google Scholar] [CrossRef]
- Howie, D.W.; Holubowycz, O.T.; Middleton, R. Large femoral heads decrease the incidence of dislocation after total hip arthroplasty: A randomized controlled trial. J. Bone Jt. Surg. Am. 2012, 94, 1095–1102. [Google Scholar] [CrossRef]
- Hummel, M.T.; Malkani, A.L.; Yakkanti, M.R.; Baker, D.L. Decreased dislocation after revision total hip arthroplasty using larger femoral head size and posterior capsular repair. J. Arthroplast. 2009, 24, 73–76. [Google Scholar] [CrossRef]
- Scifert, C.F.; Noble, P.C.; Brown, T.D.; Bartz, R.L.; Kadakia, N.; Sugano, N.; Johnston, R.C.; Pedersen, D.R.; Callaghan, J.J. Experimental and computational simulation of total hip arthroplasty dislocation. Orthop. Clin. N. Am. 2001, 32, 553–567. [Google Scholar] [CrossRef]
- Hettich, G.; Schierjott, R.A.; Ramm, H.; Graichen, H.; Jansson, V.; Rudert, M.; Traina, F.; Grupp, T.M. Method for quantitative assessment of acetabular bone defects. J. Orthop. Res. 2019, 37, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Schierjott, R.A.; Hettich, G.; Ringkamp, A.; Baxmann, M.; Morosato, F.; Damm, P.; Grupp, T.M. A method to assess primary stability of acetabular components in association with bone defects. J. Orthop. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Pierrepont, J.; Stambouzou, C.; Li, Q.; Baré, J. A Preoperative Analytical Model for Patient-Specific Impingement Analysis in Total Hip Arthroplasty. Adv. Orthop. 2019, 2019, 6293916. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, T.J.; Weber, M.; Renkawitz, T.; Greimel, F.; Leiss, F.; Grifka, J.; Schaumburger, J. Diskrepanz zwischen radiographischer und tatsächlicher Pfannenstellung bei der Hüft-TEP-Versorgung: Interpretieren wir unsere radiologischen Qualitätsindikatoren richtig? Videobeitrag. Der Orthopäde 2020, 49, 226–229. [Google Scholar] [CrossRef]
- Visser, J.D.; Konings, J.G. A new method for measuring angles after total hip arthroplasty. A study of the acetabular cup and femoral component. J. Bone Jt. Surg. Br. Vol. 1981, 63B, 556–559. [Google Scholar] [CrossRef]
- Kebbach, M.; Grawe, R.; Geier, A.; Winter, E.; Bergschmidt, P.; Kluess, D.; D’Lima, D.; Woernle, C.; Bader, R. Effect of surgical parameters on the biomechanical behaviour of bicondylar total knee endoprostheses—A robot-assisted test method based on a musculoskeletal model. Sci. Rep. 2019, 9, 14504. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient No. | Preoperatively Planned Situation | Postoperatively Reconstructed Situation | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Liner (Inner-Ø in mm) | Cup (Outer-Ø in mm) | Stem (CCD in °) | Head (Ø in mm; Head Offset Type) | Head-to-Neck Ratio | Liner (Inner-Ø in mm) | Cup (Outer-Ø in mm) | Stem (CCD in °) | Head (Ø in mm; Head Offset Type) | Head-to-Neck Ratio | |
| 210 | 36 | 52 | NK113T (128) | 36S | 2.67 | − | − | − | − | − |
| 212 | 32 | 50 | NK510T (135) | 32S | 2.37 | − | − | − | − | − |
| 216 | 32 | 48 | NK110T (128) | 32S | 2.37 | − | − | − | − | − |
| 219 | 28 | 46 | NK111T (128) | 28M | 2.07 | − | − | − | − | − |
| 253 | 36 | 52 | NK112T (128) | 36L | 2.67 | − | − | − | − | − |
| 256 | 36 | 52 | NK512T (135) | 36M | 2.67 | − | − | − | − | − |
| 259 | 36 | 52 | NK112T (128) | 36XL | 2.67 | − | − | − | − | − |
| 260 | 28 | 46 | NK110T (128) | 28S | 2.07 | − | − | − | − | − |
| 208 | 36 | 52 | NK112T (128) | 36L | 2.67 | 36 | 52 | NK112T (128) | 36XL | 2.67 |
| 213 | 32 | 48 | NK110T (128) | 32L | 2.37 | 32 | 48 | NK112T (128) | 32L | 2.37 |
| 214 | 36 | 52 | NK113T (128) | 36M | 2.67 | 36 | 52 | NK112T (128) | 36M | 2.67 |
| 217 | 36 | 60 | NK114T (128) | 36M | 2.67 | 36 | 56 | NK114T (128) | 36S | 2.67 |
| 252 | 36 | 58 | NK516T (135) | 36S | 2.67 | 36 | 56 | NK516T (135) | 36M | 2.67 |
| 254 | 32 | 48 | NK113T (128) | 32L | 2.37 | 32 | 50 | NK112T (128) | 32L | 2.37 |
| 106 | 32 | 50 | NK511T (135) | 32S | 2.37 | − | − | − | − | − |
| 107 | 36 | 52 | NK512T (135) | 36M | 2.67 | − | − | − | − | − |
| 108 | 36 | 56 | NK114T (128) | 36L | 2.67 | − | − | − | − | − |
| 109 | 36 | 58 | NK114T (128) | 36XL | 2.67 | − | − | − | − | − |
| 110 | 36 | 54 | NK112T (128) | 36XL | 2.67 | − | − | − | − | − |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kebbach, M.; Schulze, C.; Meyenburg, C.; Kluess, D.; Sungu, M.; Hartmann, A.; Günther, K.-P.; Bader, R. An MRI-Based Patient-Specific Computational Framework for the Calculation of Range of Motion of Total Hip Replacements. Appl. Sci. 2021, 11, 2852. https://doi.org/10.3390/app11062852
Kebbach M, Schulze C, Meyenburg C, Kluess D, Sungu M, Hartmann A, Günther K-P, Bader R. An MRI-Based Patient-Specific Computational Framework for the Calculation of Range of Motion of Total Hip Replacements. Applied Sciences. 2021; 11(6):2852. https://doi.org/10.3390/app11062852
Chicago/Turabian StyleKebbach, Maeruan, Christian Schulze, Christian Meyenburg, Daniel Kluess, Mevluet Sungu, Albrecht Hartmann, Klaus-Peter Günther, and Rainer Bader. 2021. "An MRI-Based Patient-Specific Computational Framework for the Calculation of Range of Motion of Total Hip Replacements" Applied Sciences 11, no. 6: 2852. https://doi.org/10.3390/app11062852
APA StyleKebbach, M., Schulze, C., Meyenburg, C., Kluess, D., Sungu, M., Hartmann, A., Günther, K.-P., & Bader, R. (2021). An MRI-Based Patient-Specific Computational Framework for the Calculation of Range of Motion of Total Hip Replacements. Applied Sciences, 11(6), 2852. https://doi.org/10.3390/app11062852