
Current Trends in Orthognathic Surgery in Poland—A Retrospective Analysis of 124 Cases

 , , and
, , and
Abstract
:1. Introduction
1.1. Historical Development of Orthognathic Surgery
1.2. Contemporary Aspects of Orthognathic Surgery
1.3. Aim of the Study
2. Materials and Methods
Statistical Methods
- For all quantitative parameters (age, duration of surgery, etc.), the conformity of their distribution with the normal distribution was tested. The conformity was assessed with the Shapiro–Wilk test for normality. The assumed critical level of significance was p < 0.05.
- For quantitative parameters, mean values (M), standard deviations (SD) and extreme values, the lowest (Min) and the highest (Max) values were calculated.
- The significance of differences in mean values of parameters with a distribution close to the normal one was tested using the analysis of variance (ANOVA) and post-hoc Tukey tests.
- For nominal qualitative (e.g., sex) and ordinal (e.g., skeletal class) variables, frequencies (n) and percentages (%) were calculated and collected in multivariate contingency tables.
- The hypotheses that no correlations between qualitative traits existed were tested using the Pearson Chi-square test. When the test result was p < 0.05, it was assumed that a significant correlation between the variables existed.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Naini, F.B.; Moss, J.P.; Gill, D.S. The enigma of facial beauty: Esthetics, proportions, deformity, and controversy. Am. J. Orthod. Dentofacial Orthop. 2006, 130, 277–282. [Google Scholar] [CrossRef]
- Little, A.C.; Jones, B.C.; DeBruine, L.M. Facial attractiveness: Evolutionary based research. Philos. Trans. R. Soc. B Biol. Sci. 2011, 366, 1638–1659. [Google Scholar] [CrossRef] [Green Version]
- Hönn, M.; Göz, G. The ideal of facial beauty: A review. J. Orofac. Orthop. 2007, 68, 6–16. [Google Scholar] [CrossRef]
- Harrar, H.; Myers, S.; Ghanem, A.M. Art or Science? An Evidence-Based Approach to Human Facial Beauty a Quantitative Analysis Towards an Informed Clinical Aesthetic Practice. Aesthetic Plast. Surg. 2018, 42, 137–146. [Google Scholar] [CrossRef] [Green Version]
- Steinhäuser, E.W. Historical development of orthognatic surgery. J. Craniomaxillofac. Surg. 1996, 24, 195–204. [Google Scholar] [CrossRef]
- Proffit, W.R.; Turvey, T.A.; Phillips, C. Orthognathic surgery: A hierarchy of stability. Int. J. Adult Orthod. Orthognath. Surg. 1996, 3, 191–204. [Google Scholar]
- Nowak, R.M. Historical outline of orthognathic surgery Dent. Med. Probl. 2014, 51, 131–135. [Google Scholar]
- Panula, K. Correction of Dentofacial Deformities with Orthognatic Surgery. In Outcome of Treatment with Special Reference to Costs, Benefits and Risks; Department of Oral and Maxillofacial Surgery, Institute of Dentistry, University of Oulu: Oulu, Finland, 2003. [Google Scholar]
- Obwegeser, H.L. Surgical correction of small or retrodisplaced maxillae. Dish-Face Deform. Plast. Reconstr. Surg. 1969, 43, 351–365. [Google Scholar] [CrossRef]
- Obwegeser, H.L. Orthognathic Surgery and a Tale of How Three Procedures Came to Be: A Letter to the Next Generations of Surgeons. Clin. Plast. Surg. 2007, 34, 331–355. [Google Scholar] [CrossRef] [PubMed]
- Hunsuck, E.E. A modified intraoral sagittal splitting technique for correction of mandibular prognathism. J. Oral Surg. Anaesth. 1968, 2, 249–252. [Google Scholar]
- Epker, B.N. Modifications in the sagittal osteotomy of the mandible. J. Oral Surg. 1977, 35, 157–159. [Google Scholar]
- Klein, K.P.; Kaban, L.B.; Masoud, M.I. Orthognathic Surgery and Orthodontics: Inadequate Planning Leading to Complications or Unfavorable Results. Oral Maxillofac. Surg. Clin. N. Am. 2020, 32, 71–82. [Google Scholar] [CrossRef]
- Sato, F.R.; Mannarino, F.S.; Asprino, L.; de Moraes, M. Prevalence and treatment of dentofacial deformities on a multiethnic population: A retrospective study. Oral Maxillofac. Surg. 2014, 18, 173–179. [Google Scholar] [CrossRef]
- Efanov, J.I.; Roy, A.A.; Huang, K.N.; Borsuk, D.E. Virtual Surgical Planning: The Pearls and Pitfalls. Plast. Reconstr. Surg. Glob. Open 2018, 17, e1443. [Google Scholar] [CrossRef]
- Steinhuber, T.; Brunold, S.; Gärtner, C.; Offermanns, V.; Ulmer, H.; Ploder, O. Is Virtual Surgical Planning in Orthognathic Surgery Faster Than Conventional Planning? A Time and Workflow Analysis of an Office-Based Workflow for Single- and Double-Jaw Surgery. J. Oral Maxillofac. Surg. 2018, 76, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Posnick, J.C.; Choi, E.; Chavda, A. Surgical Site Infections Following Bimaxillary Orthognathic, Osseous Genioplasty, and Intranasal Surgery: A Retrospective Cohort Study. J. Oral Maxillofac. Surg. 2017, 75, 584–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosola, S.; Marconcini, S.; Giammarinaro, E.; Poli, G.L.; Covani, U.; Barone, A. Oral health-related quality of life and clinical outcomes of immediately or delayed loaded implants in the rehabilitation of edentulous jaws: A retrospective comparative study. Minerva Stomatol. 2018, 67, 189–195. [Google Scholar] [CrossRef]
- Eslamipour, F.; Najimi, A.; Tadayonfard, A.; Azamian, Z. Impact of Orthognatic Surgery of Life in Patients with Dentofacial Deformities. Hindawi Int. J. Dent. 2017, 6, 4103905. [Google Scholar] [CrossRef]
- Boeck, E.M.; Lunardi, N.; Pinto Ados, S.; Pizzol, K.E.; Boeck, N.R.J. Occurrence of skeletal malocclusions in Brazilian patients with dentofacial deformities. Braz. Dent. J. 2011, 22, 340–345. [Google Scholar] [CrossRef]
- Nowak, R.; Rzepecka-Skupień, M.; Zawiślak, E. Complex orthodontic and surgical management of an adult patient with transverse maxillary deficiency and skeletal class III malocclusion: A case report. Dent. Med. Probl. 2020, 57, 103–109. [Google Scholar] [CrossRef]
- Ruslin, M.; Forouzanfar, T.; Astuti, I.A.; Soemantri, E.S.; Tuinzing, D.B. The epidemiology, treatment, and complication of dentofacial deformities in an Indonesian population: A 21-year analysis. J. Oral Maxillofac. Surg. Med. Pathol. 2015, 27, 601–607. [Google Scholar] [CrossRef]
- Watanabe, M.; Suda, N.; Ohyama, K. Mandibular prognathism in Japanese families ascertained through orthognathically treated patients. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 466–470. [Google Scholar] [CrossRef] [PubMed]
- Chew, M.T. Spectrum and management of dentofacial deformities in a multiethnic Asian population. Angle Orthod. 2006, 76, 806–809. [Google Scholar] [CrossRef] [PubMed]
- Olkun, H.K.; Borzabadi-Farahani, A.; Uçkan, S. Orthognathic Surgery Treatment Need in a Turkish Adult Population: A Retrospective Study. Int. J. Environ. Res. Public Health 2019, 28, 1881. [Google Scholar] [CrossRef] [Green Version]
- Yu, D.; Wang, F.; Wang, X.; Fang, B.; Shen, S.G. Presurgical Motivations, Self-Esteem, and Oral Health of Orthognathic Surgery Patients. J. Craniofacial Surg. 2013, 24, 743–747. [Google Scholar] [CrossRef]
- Takatsuji, H.; Kobayashi, T.; Kojima, T.; Hasebe, D.; Izumi, N.; Saito, I.; Saito, C. Effects of orthognathic surgery on psychological status of patients with jaw deformities. Int. J. Oral Maxillofac. Surg. 2015, 44, 1125–1130. [Google Scholar] [CrossRef]
- Venugoplan, S.R.; Nanda, V.; Turkistani, K.; Desai, S.; Allareddy, V. Discharge patterns of orthognathic surgeries in the United States. J. Oral Maxillofac. Surg. 2012, 70, e77–e86. [Google Scholar] [CrossRef]
- Nancy, W.N.; Glover, K.; Major, P.; Varnhagen, C.; Grace, M. Age limitation on provision of orthopedic therapy and orthognathic surgery. Am. J. Orthod. Dentofac. Orthop. 1998, 113, 156–164. [Google Scholar] [CrossRef]
- Agrawal, M.; Agrawal, J.A.; Nanjannawar, L.; Fulari, S.; Kagi, V. Dentofacial Asymmetries: Challenging Diagnosis and Treatment Planning. J. Int. Oral Health 2015, 7, 128–131. [Google Scholar]
- Thiesen, G.; Gribel, B.F.; Freitas, M.P.M. Facial asymmetry: A current review. Dent. Press J. Orthod. 2015, 20, 110–125. [Google Scholar] [CrossRef]
- Eslamipour, F.; Borzabadi-Farahani, A.; Le, B.T.; Shahmoradi, M. A Retrospective Analysis of Dentofacial Deformities and Orthognathic Surgeries. Ann. Maxillofac. Surg. 2017, 7, 73–77. [Google Scholar] [CrossRef]
- Lee, C.H.; Park, H.H.; Seo, B.M.; Lee, S.J. Modern trends in Class III orthognathic treatment: A time series analysis. Angle Orthod. 2017, 87, 269–278. [Google Scholar] [CrossRef]
- Perez, D. Edward Ellis III: Sequencing Bimaxillary Surgery: Mandible First. J. Oral Maxillofac. Surg. 2011, 69, 2217–2224. [Google Scholar] [CrossRef]
- Turvey, T. Sequencing of Two-Jaw Surgery: The Case for Operating on the Maxilla First. J. Oral Maxillofac. Surg. 2011, 69, 2225. [Google Scholar] [CrossRef]
- Borba, A.M.; Borges, A.H.; Cé, P.S.; Venturi, B.A.; Naclério-Homem, M.G.; Miloro, M. Mandible-first sequence in bimaxillary orthognathic surgery: A systematic review. Int. J. Oral Maxillofac. Surg. 2016, 45, 472–475. [Google Scholar] [CrossRef]
- Liebregts, J.; Baan, F.; de Koning, M.; Ongkosuwito, E.; Bergé, S.; Maal, T.; Xi, T. Achievability of 3D planned bimaxillary osteotomies: Maxilla-first versus mandible-first surgery. Sci. Rep. 2017, 24, 9314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berlin, N.L.; Tuggle, C.T.; Steinbacher, D.M. Improved Short-Term Outcomes following Orthognathic Surgery Are Associated with High-Volume Centers. Plast. Reconstr. Surg. 2016, 138, 273e–281e. [Google Scholar] [CrossRef] [PubMed]
- Garg, M.; Cascarini, L.; Coombes, D.M.; Walsh, S.; Tsarouchi, D.; Bentley, R.; Brennan, P.A.; Dhariwal, D.K. Multicentre study of operating time and inpatient stay for orthognathic surgery. Br. J. Oral Maxillofac. Surg. 2010, 48, 363. [Google Scholar] [CrossRef]
- Andersen, K.; Thastum, M.; Nørholt, S.E.; Blomlöf, J. Relative blood loss and operative time can predict length of stay following orthognathic surgery. Int. J. Oral Maxillofac. Surg. 2016, 45, 1209–1212. [Google Scholar] [CrossRef] [PubMed]
- Bowe, C.M.; Gurney, B.; Sloane, J.; Johnson, P.; Newlands, C. Operative time, length of stay and reoperation rates for orthognatic surgery. Br. J. Oral Maxillofac. Surg. 2021, 59, 163–167. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Skeletal Groups and Other Skeletal Malocclusion | Skeletal Class I |
| Skeletal Class II | |
| Skeletal Class III | |
| Skeletal open bite | |
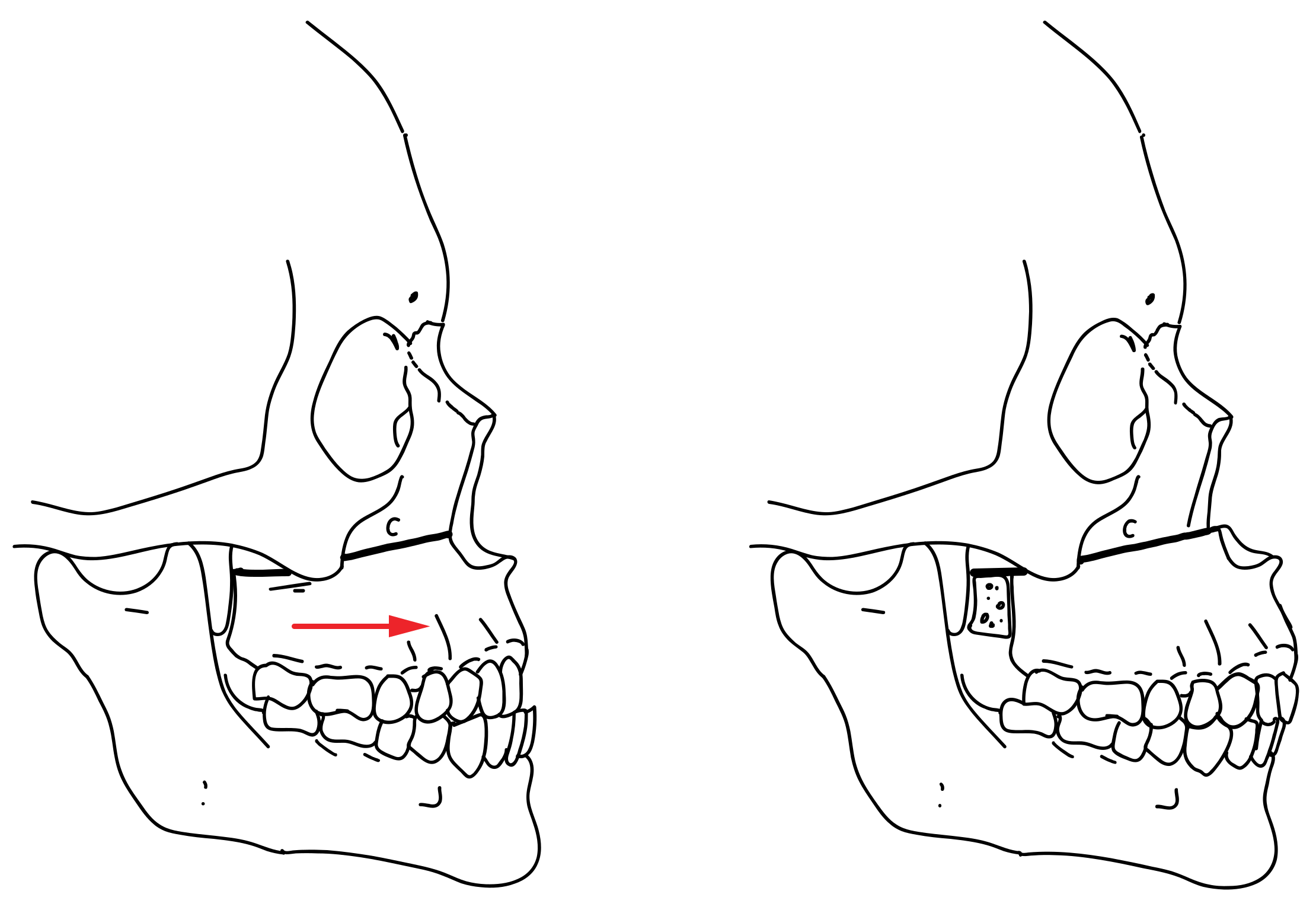
| Type of Osteotomy | Le Fort I |
| Le Fort I + segmentation | |
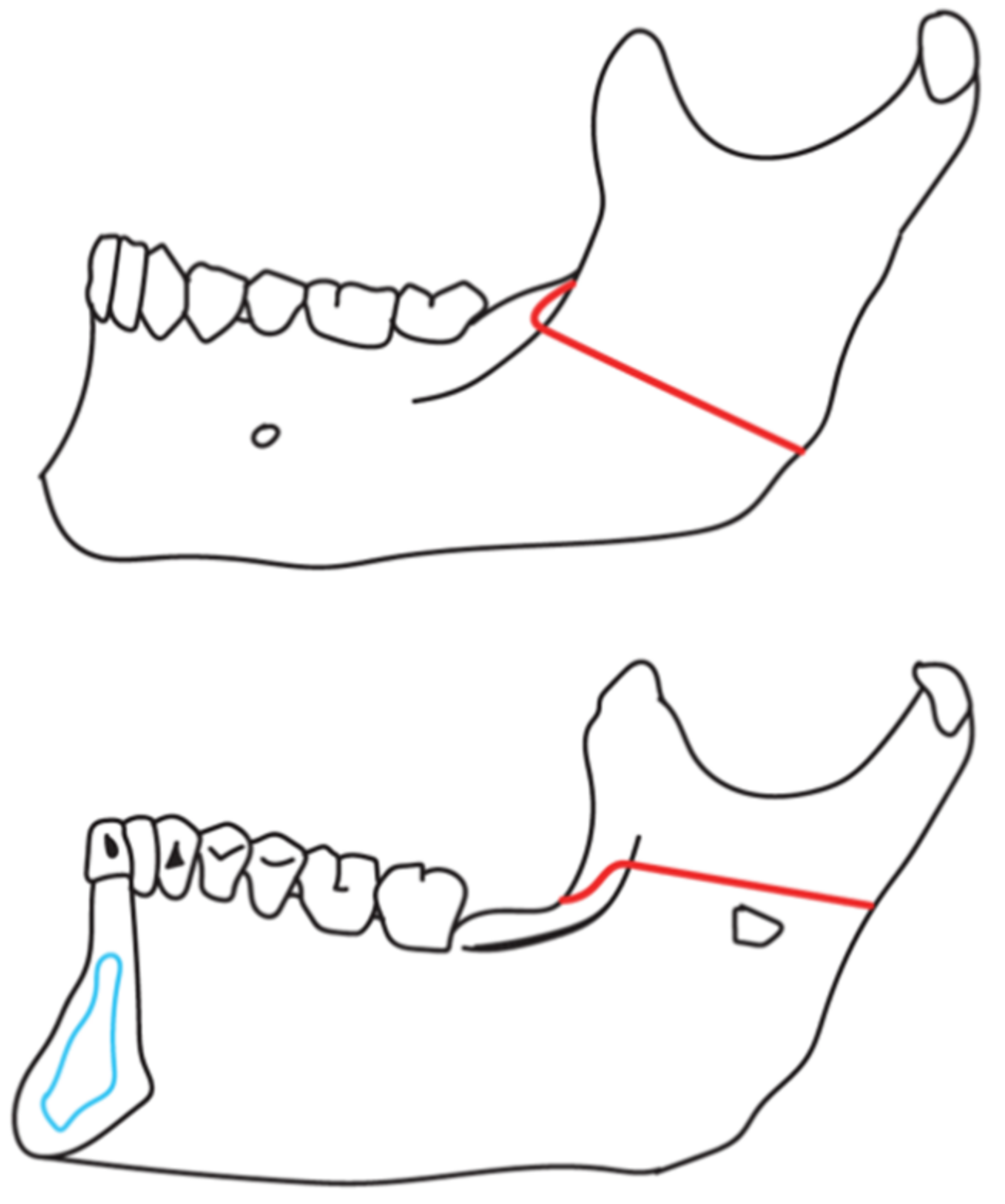
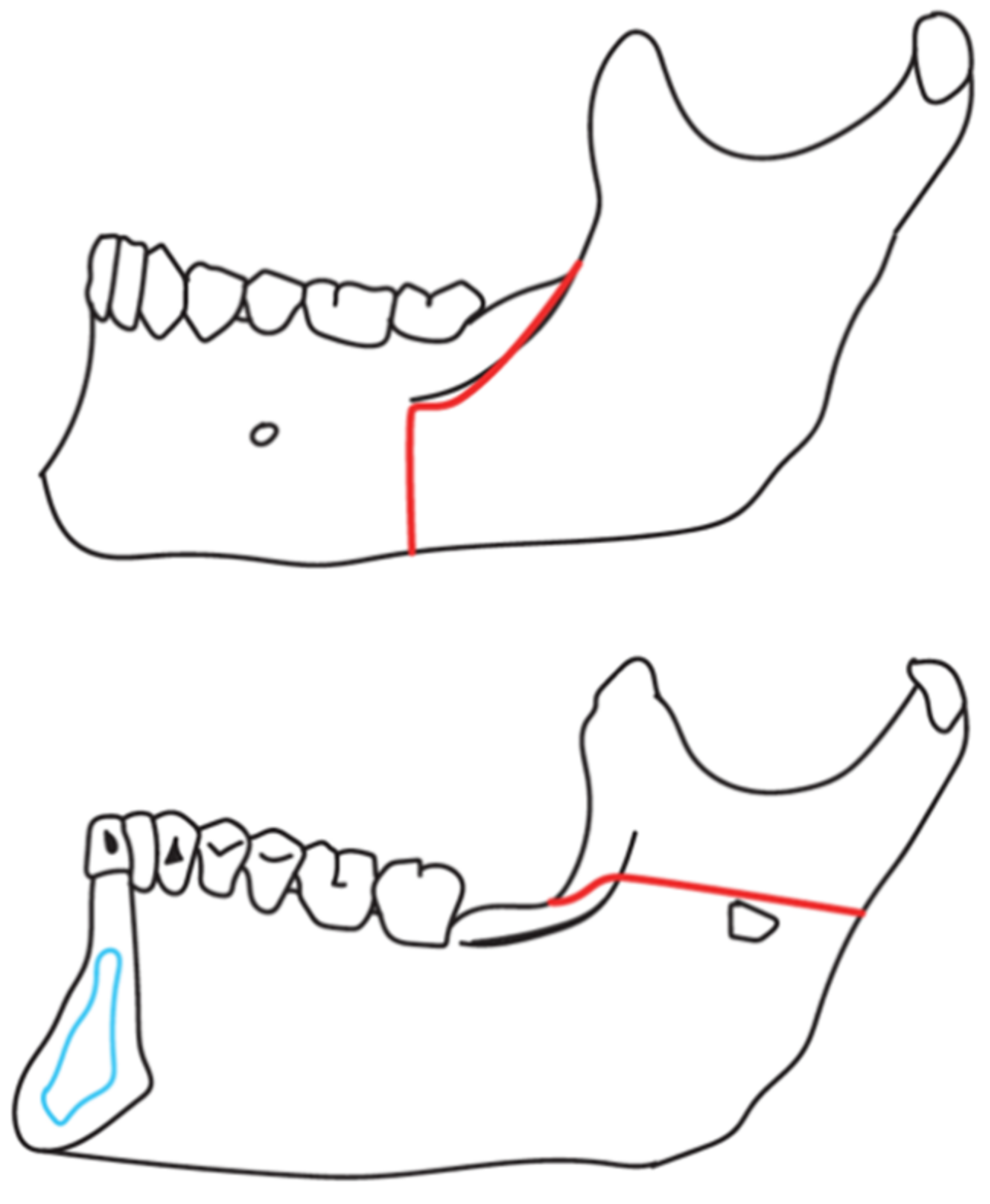
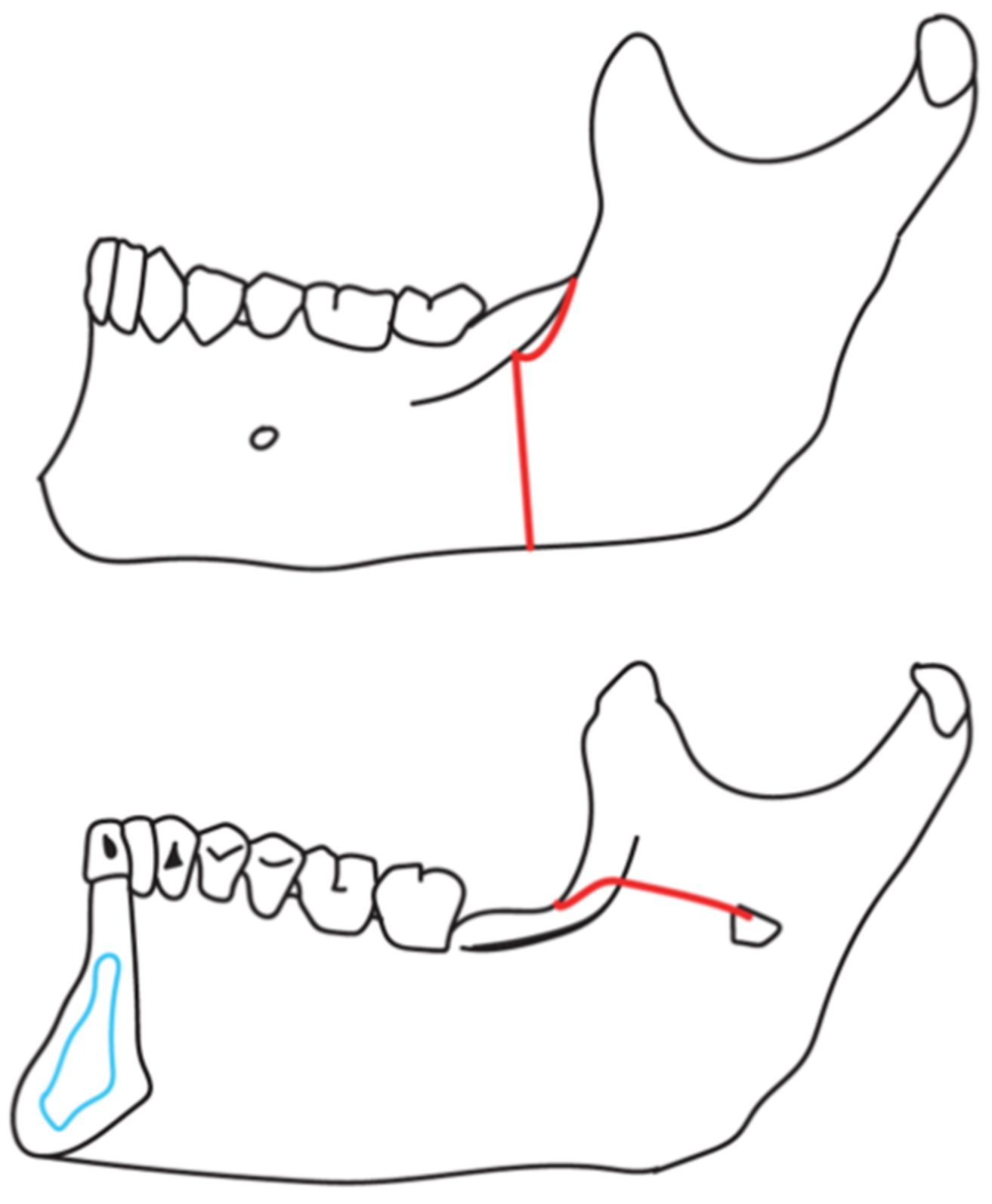
| BSSO—Obwegeser–Dal Pont | |
| BSSO—Obwegeser–Epker | |
| BSSO—Obwegeser–Epker + genioplasty | |
| Le Fort I + BSSO (Obwegeser-Epker) | |
| Le Fort I + BSSO (Obwegeser-Epker) + genioplasty | |
| Le Fort I + segmentation + BSSO (Obwegeser-Epker) | |
| Genioplasty | |
| Adjunctive Surgical Procedures | Bone graft |
| Bone graft + septoplasty | |
| Septoplasty | |
| Evacuation of osteosynthesis | |
| Assembly of skeletal anchorage | |
| No additional procedures |
| Age Range (years) | p Value | ||||
|---|---|---|---|---|---|
| 11–20 N = 25 | 21–30 N = 54 | 31–40 N = 37 | >40 N = 8 | ||
| Sex | 0.770 | ||||
| Females % (n) | 56.0 (14) | 57.4 (31) | 62.2 (23) | 75.0 (6) | |
| Males % (n) | 44.4 (11) | 42.6 (23) | 37.8 (14) | 25.0 (2) | |
| Skeletal Groups and Other Skeletal Malocclusion | ||||||
|---|---|---|---|---|---|---|
| Class I (n = 1) | Class II (n = 40) | Class III (n = 80) | Skeletal Open Bite (n = 3) | Total (n = 124) | p Value | |
| Age (mean. SD) | 33 | 30.5 (6.2) | 27.0 (7.6) | 27.7 (14.2) | 28 (7) | 0.099 |
| Sex | ||||||
| Females % (n) | 100.0 (1) | 55.0 (22) | 61.2 (49) | 66.7 (2) | 59.7 (74) | 0.757 |
| Males % (n) | 0.0 (0) | 45.0 (18) | 38.8 (31) | 33.3 (1) | 40.3 (50) | |
| Skeletal Groups and Other Skeletal Maloclusion | ||||||
|---|---|---|---|---|---|---|
| Class I (n = 1) | Class II (n = 40) | Class III (n = 80) | Skeletal Open Bite (n = 3) | Total (n = 124) | p Value | |
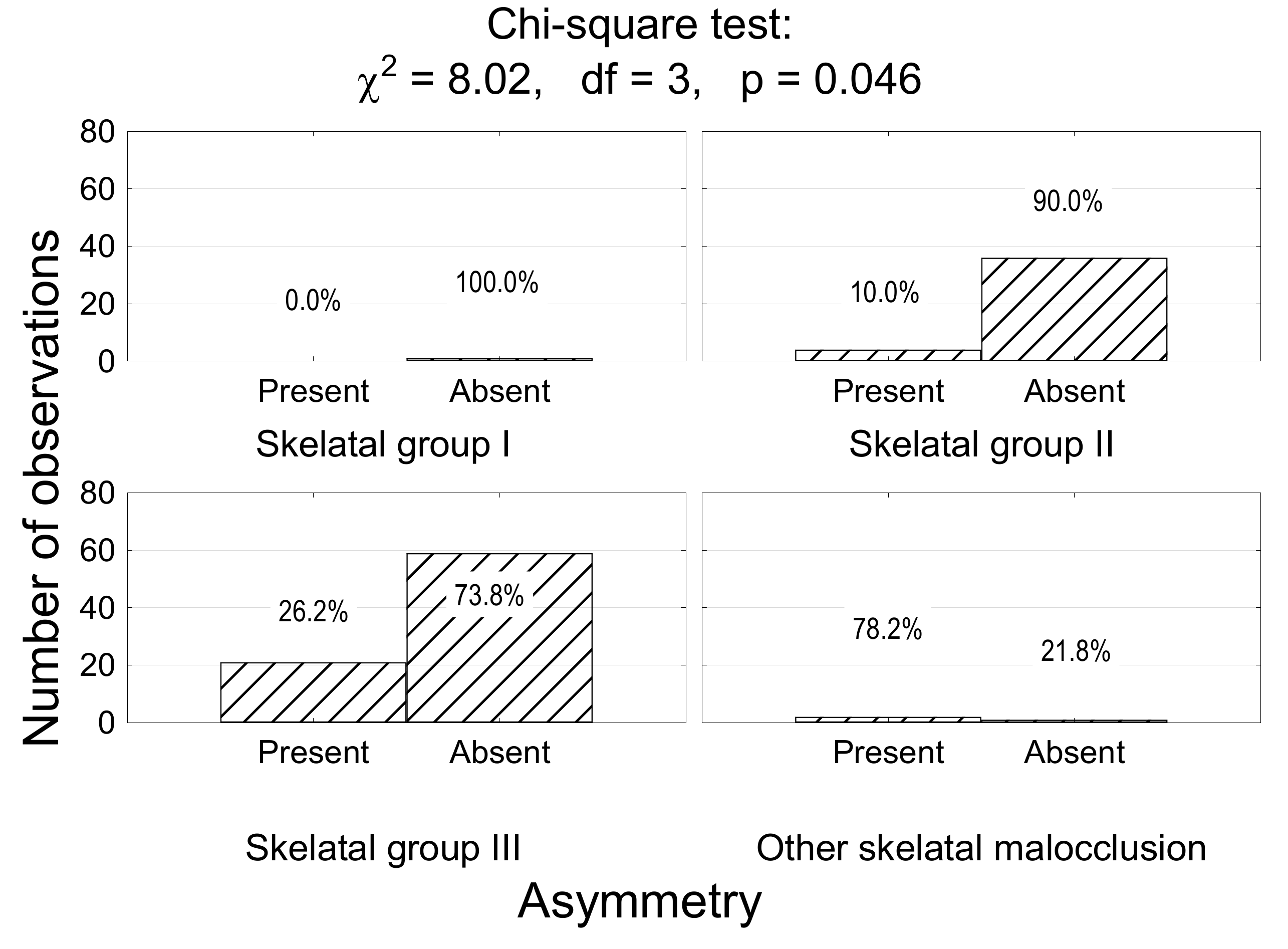
| Asymmetry | ||||||
| Present % (n) | 0.0 (0) | 10.0 (4) | 26.2 (21) | 66.7 (2) | 21.8 (27) | 0.046 |
| Absent % (n) | 100.0 (1) | 90.0 (36) | 73.8 (59) | 33.3 (1) | 78.2 (97) | |
| Type of Surgical Treatment | Skeletal Groups and Other Skeletal Maloclusion | |||||
|---|---|---|---|---|---|---|
| Class I (n = 1) | Class II (n = 40) | Class III (n = 80) | Skeletal Open Bite (n = 3) | Total (n = 124) | p Value | |
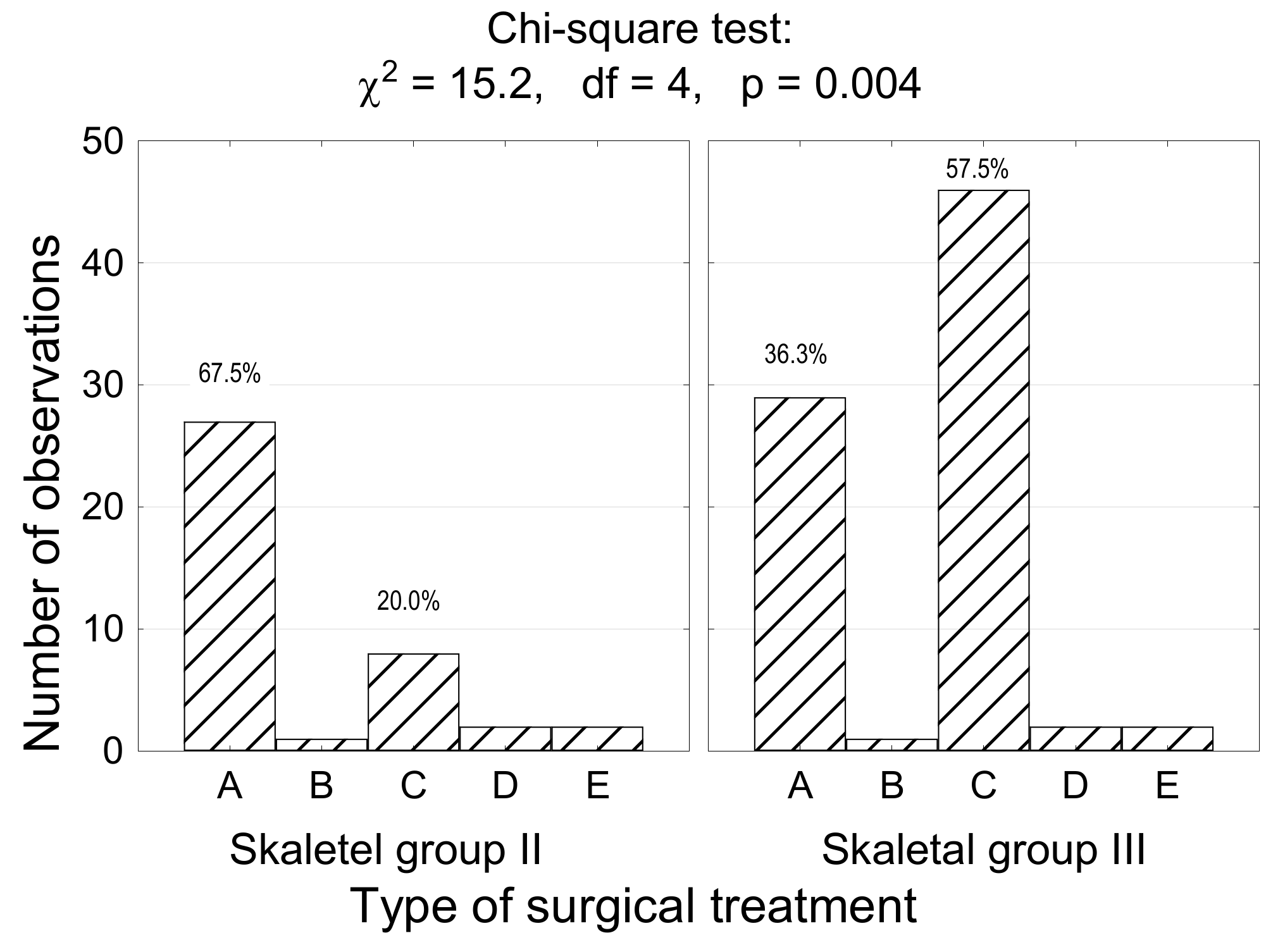
| A. One jaw surgery | 0.0 (0) | 67.5 (27) | 36.2 (29) | 0.0 (0) | 45.2 (56) | <0.001 |
| B. One jaw + genioplasty | 0.0 (0) | 2.5 (1) | 1.3 (1) | 0.0 (0) | 1.6 (2) | |
| C. Bimaxillary surgery | 0.0 (0) | 20.0 (8) | 57.5 (46) | 33.3 (1) | 44.4 (55) | |
| D. Bimaxillary surgery + genioplasty | 0.0 (0) | 5.0 (2) | 2.5 (2) | 66.7 (2) | 4.8 (6) | |
| E. No jaw (genioplasty) | 100.0 (1) | 5.0 (2) | 2.5 (2) | 0.0 (0) | 4.0 (5) | |
| Type of Osteotomy | Frequency | |
|---|---|---|
| % | n | |
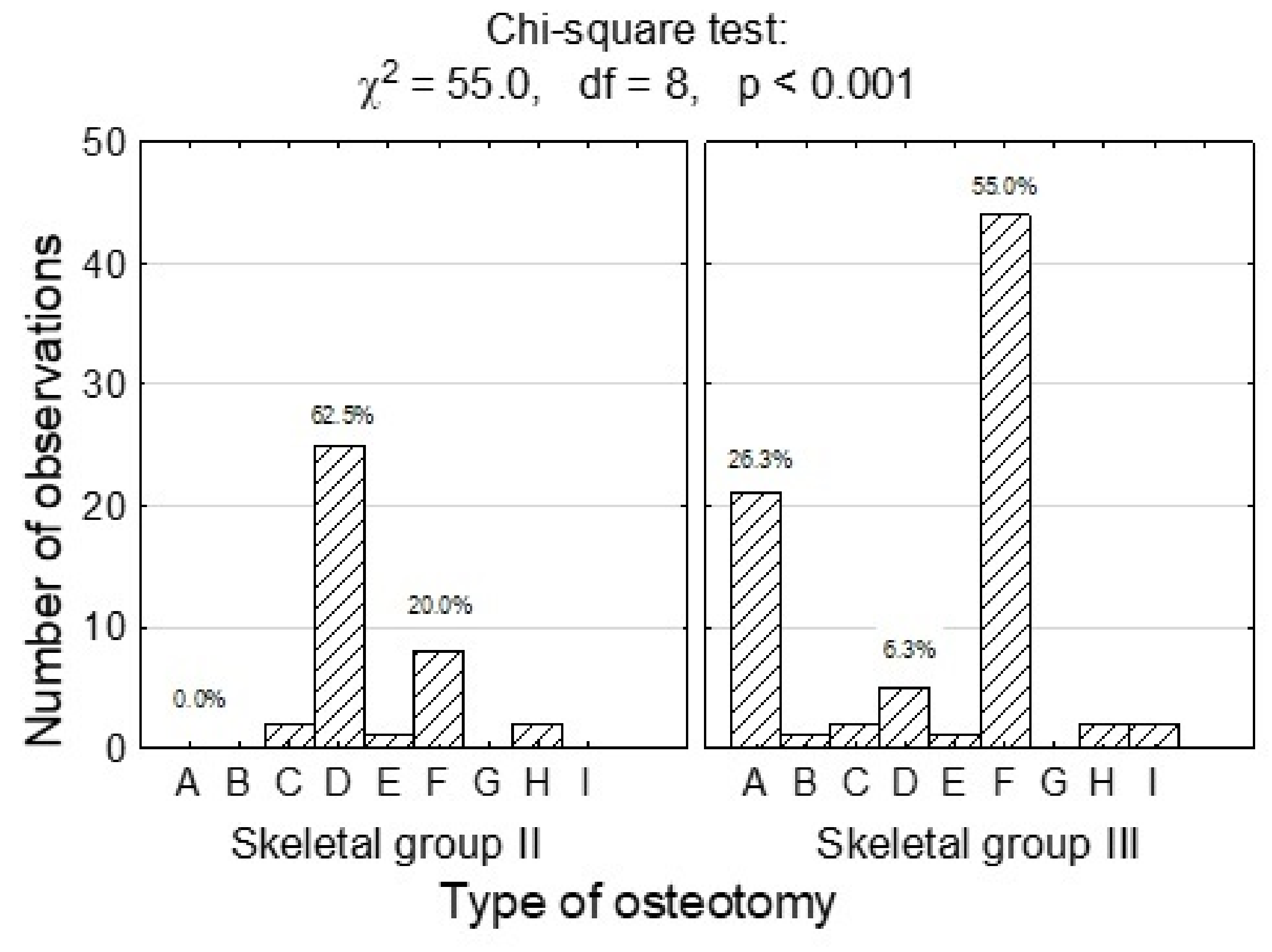
| A. Le Fort I | 16.9 | 21 |
| B. Le Fort I + segmentation | 0.8 | 1 |
| C. BSSO—Obwegeser–Dal Pont | 3.2 | 4 |
| D. BSSO—Obwegeser–Epker | 24.2 | 30 |
| E. BSSO—Obwegeser–Epker + genioplasty | 1.6 | 2 |
| F. Le Fort I + BSSO (Obwegeser–Epker) | 42.7 | 53 |
| G. Le Fort I + BSSO (Obwegeser–Epker) + genioplasty | 4.8 | 6 |
| H. Le Fort I + segmentation + BSSO (Obwegeser–Epker) | 1.6 | 2 |
| I. Genioplasty | 4.0 | 5 |
| Total | 100 | 124 |
| Type | Skeletal Groups and Other Skeletal Maloclusion | |||
|---|---|---|---|---|
| Class II (n = 10) | Class III (n = 49) | Skeletal Open Bite (n = 3) | p Value | |
| Maxilla first | 30.0 (3) | 38.8 (19) | 66.7 (2) | 0.727 |
| Mandible first | 70.0 (7) | 61.2 (30) | 33.3 (1) | |
| Total | 16.1 (10) | 79.0 (49) | 4.8 (3) | |
| Variables | Frequency | |
|---|---|---|
| % | n | |
| A—bone graft | 8.1 | 10 |
| B—bone graft + septoplasty | 2.4 | 3 |
| C—septoplasty | 13.7 | 17 |
| D—evacuation of osteosynthesis | 2.4 | 3 |
| E—assembly of skeletal anchorage | 0.8 | 1 |
| F—no additional procedures | 72.6 | 90 |
| Total | 100% | 124 |
| Adjunctive Surgical Procedures | Skeletal Groups and Other Skeletal Maloclusion | |||||
|---|---|---|---|---|---|---|
| Class I (n = 1) | Class II (n = 40) | Class III (n = 80) | Skeletal Open Bite (n = 3) | Total (n = 124) | p Value | |
| A—bone graft | 0.0 (0) | 0.0 (0) | 11.2 (9) | 33.3 (1) | 8.1 (10) | <0.001 |
| B—bone graft + septoplasty | 0.0 (0) | 0.0 (0) | 2.5 (2) | 33.3 (1) | 2.4 (3) | |
| C—septoplasty | 0.0 (0) | 7.5 (3) | 17.5 (14) | 0.0 (0) | 13.7 (17) | |
| D—evacuation of osteosynthesis | 100.0 (1) | 0.0 (0) | 2.5 (2) | 0.0 (0) | 2.4 (3) | |
| E—assembly of skeletal anchorage | 0.0 (0) | 0.0 (0) | 1.3 (1) | 0.0 (0) | 0.8 (1) | |
| F—no additional procedures | 0.0 (0) | 92.5 (37) | 65.0 (52) | 33.3 (1) | 72.6 (90) | |
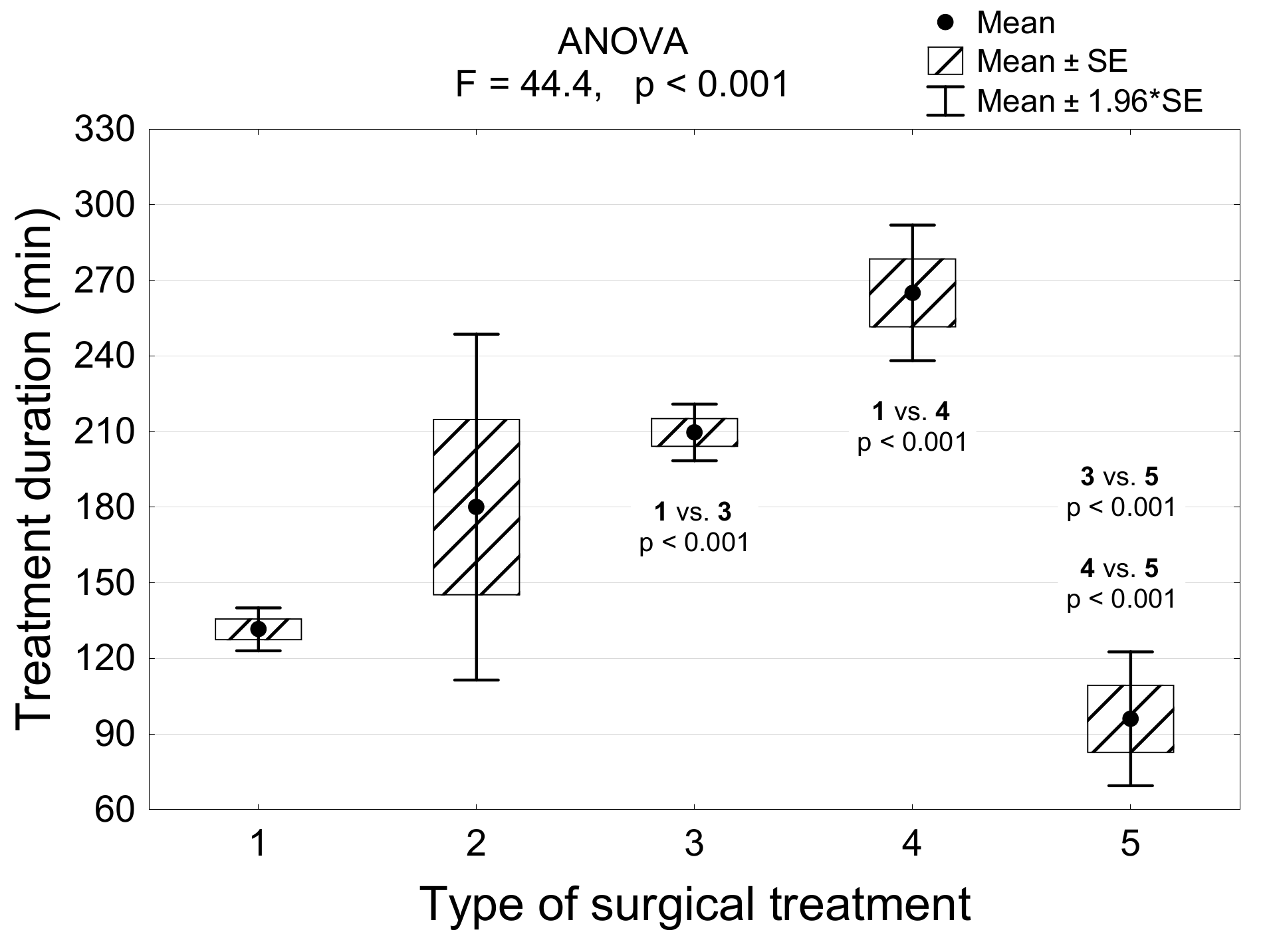
| Type of Surgical Treatment | Duration (min) | |
|---|---|---|
| Min–Max | Mean (SD) | |
| One jaw surgery | 75–210 | 132 (33) |
| One jaw + genioplasty | 145–215 | 180 (49) |
| Bimaxillary surgery | 135–385 | 210 (43) |
| Bimaxillary surgery + genioplasty | 215–305 | 265 (34) |
| No jaw (genioplasty) | 60–140 | 96 (30) |
| All | 60–385 | 172 (58) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zawiślak, E.; Przywitowski, S.; Olejnik, A.; Gerber, H.; Golusiński, P.; Nowak, R. Current Trends in Orthognathic Surgery in Poland—A Retrospective Analysis of 124 Cases. Appl. Sci. 2021, 11, 6439. https://doi.org/10.3390/app11146439
Zawiślak E, Przywitowski S, Olejnik A, Gerber H, Golusiński P, Nowak R. Current Trends in Orthognathic Surgery in Poland—A Retrospective Analysis of 124 Cases. Applied Sciences. 2021; 11(14):6439. https://doi.org/10.3390/app11146439
Chicago/Turabian StyleZawiślak, Ewa, Szymon Przywitowski, Anna Olejnik, Hanna Gerber, Paweł Golusiński, and Rafał Nowak. 2021. "Current Trends in Orthognathic Surgery in Poland—A Retrospective Analysis of 124 Cases" Applied Sciences 11, no. 14: 6439. https://doi.org/10.3390/app11146439
APA StyleZawiślak, E., Przywitowski, S., Olejnik, A., Gerber, H., Golusiński, P., & Nowak, R. (2021). Current Trends in Orthognathic Surgery in Poland—A Retrospective Analysis of 124 Cases. Applied Sciences, 11(14), 6439. https://doi.org/10.3390/app11146439