

The Sociology of Suicide After COVID-19: Assessment of the Spanish Case

 ,
,  ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Background: COVID-19 and the “New Normal”
3. Materials and Methods
4. Results and Analysis: Suicide in Spain During COVID-19
4.1. Findings from Official Data
4.2. Sociological and Theoretical Insights
5. Discussion: Suicide and the Pandemic—A Perfect Storm?
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
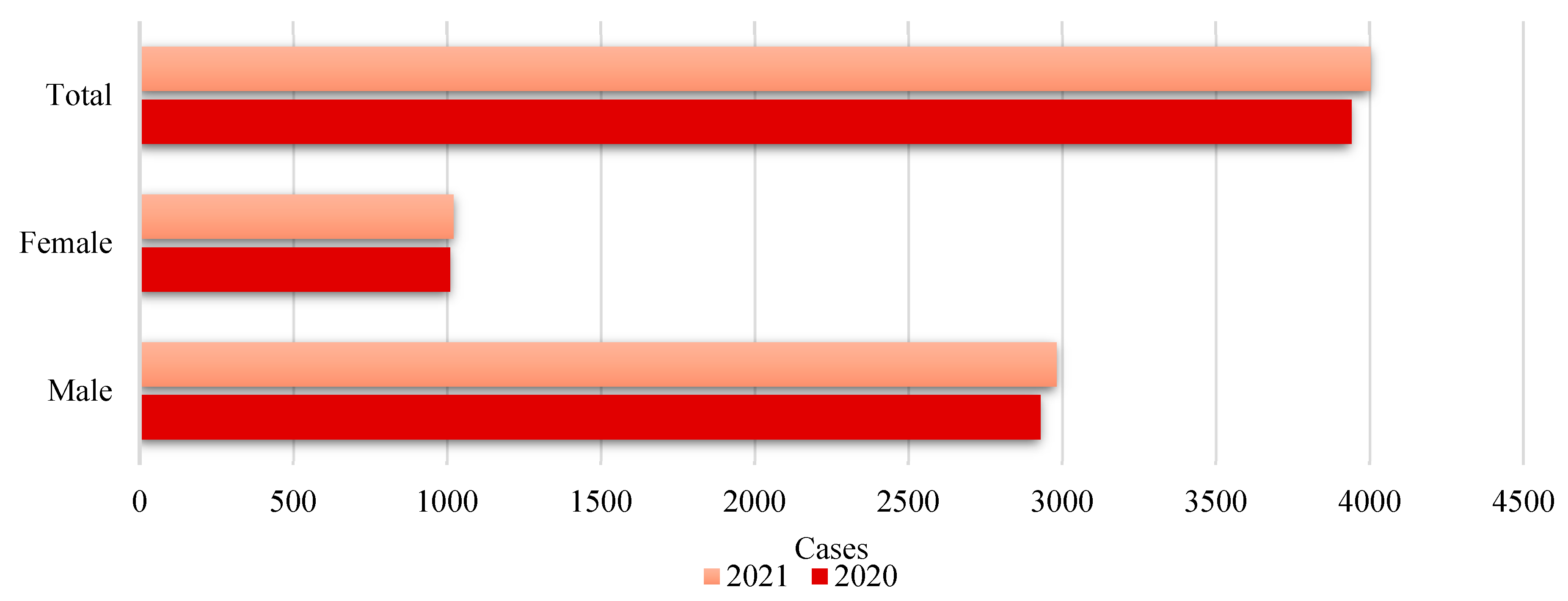
| 1 | The magnitude of the gender gap remains relatively constant from one year to the next (2020–2021), suggesting that gender-associated risk factors, such as social norms about the expression of distress and access to lethal means, may not have changed significantly between these two years. For example, according to data from the US Center for Disease Control and Prevention (CDC), in 2021, the suicide rate among men was approximately four times that of women, with 22.8 deaths per 100,000 men versus 5.7 per 100,000 women. Between 2020 and 2021, an increase in suicide rates was observed for both genders. For men, the rate increased from 21.9 to 22.8 per 100,000, while for women, it rose from 5.5 to 5.7 per 100,000. This increase may be related to several factors, including the late phases of the pandemic and the cumulative consequences of long periods of stress (Centers for Disease Control and Prevention, 2024; Substance Abuse and Mental Health Services Administration, 2023). |
| 2 |
References
- Abrams, D. S. (2021). COVID and crime: An early empirical look. Journal of Public Economics, 194, 104344. [Google Scholar] [CrossRef] [PubMed]
- Agnew, R. (1992). Foundation for a general strain theory of crime and delinquency. Criminology, 30(1), 47–88. [Google Scholar] [CrossRef]
- Ahmed, A., & Patil, P. S. (2024). Navigating the Shadows: A Comprehensive Review of Suicide in the Geriatric Population. Cureus, 16(1), e53352. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. (2021). Diversity and mental health. Available online: https://www.psychiatry.org/patients-families (accessed on 15 February 2025).
- ANAR Foundation. (2021). Informe anual 2020: El teléfono/chat ANAR en tiempos de COVID-19. Available online: https://lc.cx/wz4n72 (accessed on 15 February 2025).
- Asmundson, G. J. G., & Taylor, S. (2020). How health anxiety influences responses to viral outbreaks like COVID-19: What all decision-makers, health authorities, and health care professionals need to know. Jornal Anxiety Disord, 71, 102211. [Google Scholar] [CrossRef]
- Aymerich, C., Pedruzo, B., Pérez, J. L., Laborda, M., Herrero, J., Blanco, J., Mancebo, G., Andrés, L., Estévez, O., Fernandez, M., Salazar de Pablo, G., Catalan, A., & González-Torres, M. A. (2022). COVID-19 pandemic effects on health worker’s mental health: Systematic review and meta-analysis. European Psychiatry, 65(1), e10. [Google Scholar] [CrossRef]
- Ayuso-Mateos, J. L., Morillo, D., Haro, J. M., Olaya, B., Lara, E., & Miret, M. (2023). Changes on depression and suicidal ideation under severe lockdown restrictions during the first wave of the COVID-19 pandemic in Spain: A longitudinal study in the general population. Epidemiology and Psychiatric Sciences, 32, e55. [Google Scholar] [CrossRef]
- Bacigalupe, A., Cabezas, A., Bueno, M. B., & Martín, U. (2020). Gender as a determinant of mental health and its medicalization. SESPAS Report 2020. Gaceta Sanitaria, 34(Suppl. S1), 61–67. [Google Scholar] [CrossRef]
- Bajos, N., Jusot, F., Pailhé, A., Spire, A., Martin, C., Meyer, L., Lydié, N., Franck, J. E., Zins, M., Carrat, F., & SAPRIS Study Group. (2021). When lockdown policies amplify social inequalities in COVID-19 infections: Evidence from a cross-sectional population-based survey in France. BMC Public Health-Springer Nature, 21, 705. [Google Scholar] [CrossRef]
- Barnett, P., Oshinowo, I., Cooper, C., Taylor, C., Smith, S., & Pilling, S. (2023). The association between social class and the impact of treatment for mental health problems: A systematic review and narrative synthesis. Social Psychiatry and Psychiatric Epidemiology, 58(4), 581–603. [Google Scholar] [CrossRef]
- Beck, U. (2009). World at risk. Polity. [Google Scholar]
- Bin Naeem, S., & Kamel Boulos, M. N. (2021). COVID-19 misinformation online and health literacy: A brief overview. International Journal of Environmental Research and Public Health, 18(15), 8091. [Google Scholar] [CrossRef]
- Bornheimer, L. A., Li, J., Im, V., Taylor, M., & Himle, J. A. (2020). The role of social isolation in the relationships between psychosis and suicidal ideation. Clinical Social Work Journal, 48, 54–62. [Google Scholar] [CrossRef]
- Bränström, R., van der Star, A., & Pachankis, J. E. (2020). Untethered lives: Barriers to societal integration as predictors of the sexual orientation disparity in suicidality. Social Psychiatry and Psychiatric Epidemiology, 55(1), 89–99. [Google Scholar] [CrossRef] [PubMed]
- Breet, E., Matooane, M., Tomlinson, M., & Bantjes, J. (2021). Systematic review and narrative synthesis of suicide prevention in high-schools and universities: A research agenda for evidence-based practice. BMC Public Health, 21(1), 1116. [Google Scholar] [CrossRef] [PubMed]
- Caceres, M. M., Sosa, J. P., Lawrence, J. A., Sestacovschi, C., Tidd-Johnson, A., Rasool, M. H. U., Gadamidi, V. K., Ozair, S., Pandav, K., Cuevas-Lou, C., Parrish, M., Rodriguez, I., & Fernandez, J. P. (2022). The impact of misinformation on the COVID-19 pandemic. AIMS Public Health, 9(2), 262–277. [Google Scholar] [CrossRef]
- Canetto, S. S., & Cleary, A. (2012). Men, masculinities and suicidal behaviour. Social Science & Medicine (1982), 74(4), 461–465. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. (2022a). Mental health. Available online: https://www.cdc.gov/mental-health/about/?CDC_AAref_Val= (accessed on 15 February 2025).
- Centers for Disease Control and Prevention. (2022b). Suicide prevention. Available online: https://www.cdc.gov/suicide/risk-factors/?CDC_AAref_Val= (accessed on 17 February 2025).
- Centers for Disease Control and Prevention. (2024). Web-based Injury Statistics Query and Reporting System (WISQARS). Available online: https://www.cdc.gov/injury/wisqars/index.html (accessed on 14 February 2025).
- Chandler, A. (2020). Socioeconomic inequalities of suicide: Sociological and psychological intersections. European Journal of Social Theory, 23(1), 33–51. [Google Scholar] [CrossRef]
- Chang, S. S., Stuckler, D., Yip, P., & Gunnell, D. (2013). Impact of 2008 global economic crisis on suicide: Time trend study in 54 countries. BMJ (Clinical Research ed.), 347, f5239. [Google Scholar] [CrossRef]
- Chen, J. I., Roth, B., Dobscha, S. K., & Lowery, J. C. (2024). Implementation strategies in suicide prevention: A scoping review. Implementation Science: IS, 19(1), 20. [Google Scholar] [CrossRef]
- Clua-García, R., Casanova-Garrigós, G., & Moreno-Poyato, A. R. (2021). Suicide care from the nursing perspective: A meta-synthesis of qualitative studies. Journal of Advanced Nursing, 77(7), 2995–3007. [Google Scholar] [CrossRef]
- Cockerham, W. C. (2021). Sociology of mental disorder. Routledge. [Google Scholar]
- Cockerham, W. C. (2022). Medical sociology. Routledge. [Google Scholar]
- Cohen, L. E., & Felson, M. (1979). Social change and crime rate trends: A routine activity approach. American Sociological Review, 44(4), 588–608. [Google Scholar] [CrossRef]
- Coope, C., Gunnell, D., Hollingworth, W., Hawton, K., Kapur, N., Fearn, V., Wells, C., & Metcalfe, C. (2014). Suicide and the 2008 economic recession: Who is most at risk? Trends in suicide rates in England and Wales 2001–2011. Social Science & Medicine (1982), 117, 76–85. [Google Scholar] [CrossRef]
- Corcoran, P., Griffin, E., Arensman, E., Fitzgerald, A. P., & Perry, I. J. (2015). Impact of the economic recession and subsequent austerity on suicide and self-harm in Ireland: An interrupted time series analysis. International Journal of Epidemiology, 44(3), 969–977. [Google Scholar] [CrossRef] [PubMed]
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. (2020). The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nature Microbiology, 5(4), 536–544. [Google Scholar] [CrossRef] [PubMed]
- Da Cunha Varella, A. P., Griffin, E., Khashan, A., & Kabir, Z. (2024). Suicide rates before and during the COVID-19 pandemic: A systematic review and meta-analysis. Social Psychiatry and Psychiatric Epidemiology, 59(11), 1897–1905. [Google Scholar] [CrossRef]
- Daly, M., Sutin, A. R., & Robinson, E. (2022). Longitudinal changes in mental health and the COVID-19 pandemic: Evidence from the UK Household Longitudinal Study. Psychological Medicine, 52(13), 2549–2558. [Google Scholar] [CrossRef]
- De la Torre Luque, A. (2023). Evolución del suicidio en España en este milenio (2000–2021). Universidad Complutense de Madrid. [Google Scholar]
- De la Torre Luque, A., Perez-Diez, I., Pemau, A., Martinez-Ales, G., Borges, G., Perez-Sola, V., & Ayuso-Mateos, J. L. (2024). Suicide mortality in Spain during the COVID-19 pandemic: Longitudinal analysis of sociodemographic factors. European Neuropsychopharmacology, 82, 29–34. [Google Scholar] [CrossRef]
- Durkheim, E. (1951). Suicide: A study in sociology. Free Press. (originally in French 1897). [Google Scholar]
- Fair Health. (2022). Patients diagnosed with post-COVID conditions. An analysis of private healthcare claimsusing the OfficialICD-10 diagnostic code. Fair Health Inc. [Google Scholar]
- Favril, L., Yu, R., Uyar, A., Sharpe, M., & Fazel, S. (2022). Risk factors for suicide in adults: Systematic review and meta-analysis of psychological autopsy studies. Evidence-Based Mental Health, 25(4), 148–155. [Google Scholar] [CrossRef]
- Fiorillo, A., & Gorwood, P. (2020). The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. European Psychiatry, 63(1), e32. [Google Scholar] [CrossRef]
- Freeman, A., Mergl, R., Kohls, E., Székely, A., Gusmao, R., Arensman, E., Koburger, N., Hegerl, U., & Rummel-Kluge, C. (2017). A cross-national study on gender differences in suicide intent. BMC Psychiatry, 17, 1–11. [Google Scholar] [CrossRef]
- González-Sanguino, C., Ausín, B., Castellanos, M. Á., Saiz, J., López-Gómez, A., Ugidos, C., & Muñoz, M. (2020). Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain, behavior, and Immunity, 87, 172–176. [Google Scholar] [CrossRef]
- Gunnell, D., Appleby, L., Arensman, E., Hawton, K., John, A., Kapur, N., Khan, M., O’Connor, R. C., Pirkis, J., & COVID-19 Suicide Prevention Research Collaboration. (2020). Suicide risk and prevention during the COVID-19 pandemic. The Lancet Psychiatry, 7(6), 468–471. [Google Scholar] [CrossRef] [PubMed]
- Harper, S., & Bruckner, T. A. (2017). Did the Great Recession increase suicides in the USA? Evidence from an interrupted time-series analysis. Annals of Epidemiology, 27(7), 409–414. [Google Scholar] [CrossRef] [PubMed]
- Haw, C., Hawton, K., Gunnell, D., & Platt, S. (2015). Economic recession and suicidal behaviour: Possible mechanisms and ameliorating factors. The International Journal of Social Psychiatry, 61(1), 73–81. [Google Scholar] [CrossRef]
- Hawton, K., Lascelles, K., Pitman, A., Gilbert, S., Bale, E., & Muniz, J. (2021). Self-harm and the COVID-19 pandemic: A study of factors contributing to self-harm during lockdown restrictions. Journal of Affective Disorders, 295, 441–449. [Google Scholar] [CrossRef]
- Hedegaard, H., & Warner, M. (2021). Suicide mortality in the United States, 1999–2019. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics. [Google Scholar]
- Holmes, E. A., O’Connor, R. C., Perry, V. H., Tracey, I., Wessely, S., Arseneault, L., Ballard, C., Christensen, H., Silver, R. C., Everall, I., & Ford, T. (2020). Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. The Lancet Psychiatry, 7(6), 547–560. [Google Scholar] [CrossRef]
- Holst, H., Fessler, A., & Niehoff, S. (2021). COVID-19, social class and work experience in Germany: Inequalities in work-related health and economic risks. European Societies, 23(Suppl. S1), S495–S512. [Google Scholar] [CrossRef]
- Hong, R., Cheng, W. H., Cheng, L. J., Lau, Y., & Lau, S. T. (2023). Global prevalence of social isolation among community-dwelling older adults: A systematic review and meta-analysis. Archives of Gerontology and Geriatrics, 107, 104904. [Google Scholar]
- Houle, J., Mishara, B. L., & Chagnon, F. (2008). An empirical test of a mediation model of the impact of the traditional male gender role on suicidal behavior in men. Journal of Affective Disorders, 107(1–3), 37–43. [Google Scholar] [CrossRef]
- Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., Zhang, L., Fan, G., Xu, J., Gu, X., & Cheng, Z. (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet, 395(10223), 497–506. [Google Scholar] [CrossRef]
- Husain, M. O., Gratzer, D., Husain, M. I., & Naeem, F. (2021). Mental Illness in the Post-pandemic World: Digital Psychiatry and the Future. Frontiers in Psychology, 12, 567426. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística. (2020). Defunciones por suicidio. Año 2019 [dataset]. Spanish Statistical Office Database. Available online: https://www.ine.es/jaxi/Datos.htm?tpx=48293 (accessed on 27 January 2025).
- Instituto Nacional de Estadística. (2021). Defunciones por suicidio. Año 2020 [dataset]. Spanish Statistical Office Database. Available online: https://www.ine.es/jaxi/Datos.htm?tpx=49948 (accessed on 27 January 2025).
- Instituto Nacional de Estadística. (2023). Estadísticas de suicidio en España. Spanish Statistical Office Database. Available online: https://n9.cl/kml7b (accessed on 14 February 2025).
- Instituto Nacional de Estadística. (2024). Estadística de defunciones según causa de muerte [dataset]. Spanish Statistical Office Database. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176780&menu=ultiDatos&idp=1254735573175 (accessed on 14 February 2025).
- Ji, X., Zhan, T., & Zhu, T. (2024). Impact of COVID-19 on negative body image: Evidence based on social media data. Social Science & Medicine, 340, 116461. [Google Scholar] [CrossRef]
- Johns Hopkins University. (2023). COVID-19 dashboard. Available online: https://n9.cl/gj7w (accessed on 27 January 2025).
- Kasal, A., Táborská, R., Juríková, L., Grabenhofer-Eggerth, A., Pichler, M., Gruber, B., Tomášková, H., & Niederkrotenthaler, T. (2023). Facilitators and barriers to implementation of suicide prevention interventions: Scoping review. Global Mental Health, 10, e15. [Google Scholar] [CrossRef] [PubMed]
- Kawohl, W., & Nordt, C. (2020). COVID-19, unemployment, and suicide. The Lancet Psychiatry, 7(5), 389–390. [Google Scholar] [CrossRef] [PubMed]
- Keohane, A., & Richardson, N. (2018). Negotiating Gender Norms to Support Men in Psychological Distress. American Journal of Men’s Health, 12(1), 160–171. [Google Scholar] [CrossRef]
- Kim, A. M. (2022). The impact of the COVID-19 pandemic on suicides: A population study. Psychiatry Research, 314, 114663. [Google Scholar] [CrossRef]
- Krishnamoorthy, S., Mathieu, S., Armstrong, G., Ross, V., Francis, J., Reifels, L., & Kõlves, K. (2024). Implementation of complex suicide prevention interventions: Insights into barriers, facilitators and lessons learned. Archives of Suicide Research: Official Journal of the International Academy for Suicide Research, 9, 1–24. [Google Scholar] [CrossRef]
- Kwon, J. W., Chun, H., & Cho, S. I. (2009). A closer look at the increase in suicide rates in South Korea from 1986–2005. BMC Public Health, 9, 1–9. [Google Scholar] [CrossRef]
- Kwong, A. S. F., Pearson, R. M., Adams, M. J., Northstone, K., Tilling, K., Smith, D., Fawns-Ritchie, C., Bould, H., Warne, N., Zammit, S., Gunnell, D., Moran, P., Micali, N., & Timpson, N. J. (2021). Mental health before and during the COVID-19 pandemic in two longitudinal UK population cohorts. The British Journal of Psychiatry, 218(6), 334–343. [Google Scholar] [CrossRef]
- Lee, H., & Singh, G. K. (2021). Monthly trends in self-reported health status and depression by race/ethnicity and socioeconomic status during the COVID-19 Pandemic, United States, April 2020–May 2021. Annals of Epidemiology, 63, 52–62. [Google Scholar] [CrossRef]
- Lopes, J., Damasceno, A. B. P., da Costa, G. S., Silva, V. D. O., Filho, V. A. D. B., & De Lima, J. C. M. G. (2022). A Influência da Pandemia da COVID-19 na Pronunciação de Sinais Neurológicos e Cognitivos de Crianças e Adolescentes com TDAH: Uma Revisão Integrativa. Brazilian Medical Students, 7(10), 1–11. [Google Scholar] [CrossRef]
- Manchia, M., Gathier, A. W., Yapici-Eser, H., Schmidt, M. V., de Quervain, D., van Amelsvoort, T., Bisson, J. I., Cryan, J. F., Howes, O. D., Pinto, L., van der Wee, N. J., Domschke, K., Branchi, I., & Vinkers, C. H. (2022). The impact of the prolonged COVID-19 pandemic on stress resilience and mental health: A critical review across waves. European Neuropsychopharmacology: The Journal of the European College of Neuropsychopharmacology, 55, 22–83. [Google Scholar] [CrossRef] [PubMed]
- Martini, M., da Fonseca, R. C., de Sousa, M. H., de Azambuja Farias, C., Cardoso, T. A., Kunz, M., Longaray, V. K., & Magalhães, P. V. D. S. (2019). Age and sex trends for suicide in Brazil between 2000 and 2016. Social Psychiatry and Psychiatric Epidemiology, 54(7), 857–860. [Google Scholar] [CrossRef] [PubMed]
- Mauss, M. (1990). The gift: Forms and functions of exchange in archaic societies. Routledge. (originally in French 1925). [Google Scholar]
- Mayo Clinic. (2023). Mental illness. Symptoms and causes. Available online: https://www.mayoclinic.org/diseases-conditions/mental-illness/in-depth/mental-health/art-20046477 (accessed on 20 February 2025).
- Meltzer, H., Bebbington, P., Brugha, T., Jenkins, R., McManus, S., & Dennis, M. S. (2011). Personal debt and suicidal ideation. Psychological Medicine, 41(4), 771–778. [Google Scholar] [CrossRef] [PubMed]
- Mental Health and Substance Use. (2013). Mental health action plan 2013–2020. World Health Organization. [Google Scholar]
- Mental Health and Substance Use. (2021). Suicide worldwide in 2019. Global Health Estimates. World Health Organization. [Google Scholar]
- Merayo-Cano, J. M., Porras-Segovia, A. A., & Baca-García, E. (2023). COVID-19 impact vs. suicide impact in Spain. Spanish Journal of Psychiatry and Mental Health, 16(2), 129–130. [Google Scholar] [CrossRef]
- Minian, N., Gayapersad, A., Coroiu, A., Dragonetti, R., Zawertailo, L., Zaheer, J., O’Neill, B., Lange, S., Thomson, N., Crawford, A., Kennedy, S. H., & Selby, P. (2024). Prototyping the implementation of a suicide prevention protocol in primary care settings using PDSA cycles: A mixed method study. Frontiers in Psychiatry, 15, 1286078. [Google Scholar] [CrossRef]
- Ministerio de Sanidad. (2024). Defunciones por suicidio en España, 2022–2024. Available online: https://www.sanidad.gob.es/estadEstudios/estadisticas/estadisticas/estMinisterio/mortalidad/docs/DefunSuicidio2022-2024_NOTA__TEC.pdf (accessed on 20 February 2025).
- Mościcki, E. K. (1994). Gender differences in completed and attempted suicides. Annals of Epidemiology, 4(2), 152–158. [Google Scholar] [CrossRef]
- Motillon-Toudic, C., Walter, M., Séguin, M., Carrier, J. D., Berrouiguet, S., & Lemey, C. (2022). Social isolation and suicide risk: Literature review and perspectives. European psychiatry: The journal of the Association of European Psychiatrists, 65(1), e65. [Google Scholar] [CrossRef]
- Möller-Leimkühler, A. M. (2003). The gender gap in suicide and premature death or: Why are men so vulnerable? European Archives of Psychiatry and Clinical Neuroscience, 253(1), 1–8. [Google Scholar] [CrossRef]
- Mueller, A. S., Abrutyn, S., Pescosolido, B., & Diefendorf, S. (2021). The social roots of suicide: Theorizing how the external social world matters to suicide and suicide prevention. Frontiers in Psychology, 12, 621569. [Google Scholar] [CrossRef]
- National Institutes of Health. (2023). Suicide prevention. Available online: https://www.nimh.nih.gov/health/topics/suicide-prevention (accessed on 20 February 2025).
- Nettleton, S. (2021). The sociology of health and illness. Polity. [Google Scholar]
- Nicolini, H. (2020). Depression and anxiety during COVID-19 pandemic. Cirugía y Cirujanos, 88(5), 542–547. [Google Scholar] [CrossRef]
- Niedzwiedz, C. L., Green, M. J., Benzeval, M., Campbell, D., Craig, P., Demou, E., Leyland, A. H., Pearce, A., Thomson, R., & Whitley, E. (2021). Mental health and health behaviours before and during the initial phase of the COVID-19 lockdown: Longitudinal analyses of the UK Household Longitudinal Study. Journal of Epidemiology & Community Health, 75(3), 224–231. [Google Scholar] [CrossRef]
- O’Connor, R. C., Wetherall, K., Cleare, S., McClelland, H., Melson, A. J., Niedzwiedz, C. L., O’Carroll, R. E., O’Connor, D. B., Platt, S., Scowcroft, E., Watson, B., Zortea, T., Ferguson, E., & Robb, K. A. (2021). Mental health and well-being during the COVID-19 pandemic: Longitudinal analyses of adults in the UK COVID-19 Mental Health & Wellbeing study. The British Journal of Psychiatry: The Journal of Mental Science, 218(6), 326–333. [Google Scholar] [CrossRef] [PubMed]
- Pappa, S., Ntella, V., Giannakas, T., Giannakoulis, V. G., Papoutsi, E., & Katsaounou, P. (2020). Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain, Behavior, and Immunity, 88, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Paricio del Castillo, R., del Sol-Calderón, P., García-Murillo, L., Mallol-Castaño, L., Pascual-Aranda, A., & Palanca-Maresca, I. (2024). Suicidio infanto-juvenil tras la pandemia de COVID-19: Análisis de un fenómeno trágico. Revista de la Asociación Española de Neuropsiquiatría, 44(145), 19–45. [Google Scholar]
- Pathirathna, M. L., Nandasena, H. M. R. K. G., Atapattu, A. M. M. P., & Weerasekara, I. (2022). Impact of the COVID-19 pandemic on suicidal attempts and death rates: A systematic review. BMC Psychiatry, 22(1), 506. [Google Scholar] [CrossRef]
- Patwa, P., Sharma, S., Pykl, S., Guptha, V., Kumari, G., Akhtar, M. S., Ekbal, A., Das, A., & Chakraborty, T. (2021). Fighting an infodemic: COVID-19 fake news dataset. In combating online hostile posts in regional languages during emergency situation: First international workshop, constraint 2021, collocated with AAAI 2021, virtual event, 8 February 2021, revised selected papers 1 (pp. 21–29). Springer International Publishing. [Google Scholar]
- Pearman, A., Hughes, M. L., Smith, E. L., & Neupert, S. D. (2020). Mental health challenges of United States healthcare professionals during COVID-19. Frontiers in Psychology, 11, 2065. [Google Scholar] [CrossRef]
- Pierce, M., Hope, H., Ford, T., Hatch, S., Hotopf, M., John, A., Kontopantelis, E., Webb, R., Wessely, S., McManus, S., & Abel, K. M. (2020). Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. The Lancet Psychiatry, 7(10), 883–892. [Google Scholar] [CrossRef]
- Radhakrishnan, R., & Andrade, C. (2012). Suicide: An Indian perspective. Indian Journal of Psychiatry, 54(4), 304–319. [Google Scholar] [CrossRef]
- Reger, M. A., Stanley, I. H., & Joiner, T. E. (2020). Suicide Mortality and Coronavirus Disease 2019-A Perfect Storm? JAMA Psychiatry, 77(11), 1093–1094. [Google Scholar] [CrossRef]
- Schnitzer, P. G., Dykstra, H., & Collier, A. (2023). The COVID-19 Pandemic and Youth Suicide: 2020–2021. Pediatrics, 151(3), e2022058716. [Google Scholar] [CrossRef]
- Schrijvers, D. L., Bollen, J., & Sabbe, B. G. (2012). The gender paradox in suicidal behavior and its impact on the suicidal process. Journal of Affective Disorders, 138(1–2), 19–26. [Google Scholar] [CrossRef] [PubMed]
- Sher, L. (2020). The impact of the COVID-19 pandemic on suicide rates. QJM: Monthly Journal of the Association of Physicians, 113(10), 707–712. [Google Scholar] [CrossRef] [PubMed]
- Shi, P., Yang, A., Zhao, Q., Chen, Z., Ren, X., & Dai, Q. (2021). A Hypothesis of Gender Differences in Self-Reporting Symptom of Depression: Implications to Solve Under-Diagnosis and Under-Treatment of Depression in Males. Frontiers in Psychiatry, 12, 589687. [Google Scholar] [CrossRef] [PubMed]
- Shidhaye, R. (2023). Global priorities for improving access to mental health services for adolescents in the post-pandemic world. Current Opinion in Psychology, 53, 101661. [Google Scholar] [CrossRef]
- Shinn, A. K., & Viron, M. (2020). Perspectives on the COVID-19 pandemic and individuals with serious mental illness. The Journal of Clinical Psychiatry, 81(3), 20com13412. [Google Scholar] [CrossRef]
- Sohn, M., Koo, H., Choi, H., Cho, H., & Han, E. (2022). Collateral impact of the COVID−19 pandemic on the use of healthcare resources among people with disabilities. Frontiers Public Health, 10, 922043. [Google Scholar] [CrossRef]
- Solomonov, N., Green, J., Quintana, A., Lin, J., Ognyanova, K., Santillana, M., Druckman, J. N., Baum, M. A., Lazer, D., Gunning, F. M., & Perlis, R. H. (2023). A 50-state survey study of thoughts of suicide and social isolation among older adults in the United States. Journal of Affective Disorders, 334, 43–49. [Google Scholar] [CrossRef]
- Soria, K. M., & Horgos, B. (2020). Social class differences in students’ experiences during the COVID-19 pandemic. University of California-Berkeley and University of Minnesota. [Google Scholar]
- Substance Abuse and Mental Health Services Administration. (2023). Key substance use and mental health indicators in the United States: Results from the 2022 national survey on drug use and health. Available online: https://www.samhsa.gov/data/report/2022-nsduh-annual-national-report (accessed on 15 February 2025).
- Tanaka, T., & Okamoto, S. (2021). Increase in suicide following an initial decline during the COVID-19 pandemic in Japan. Nature Human Behaviour, 5(2), 229–238. [Google Scholar] [CrossRef]
- Toribio-Caballero, S., Cardenal, V., Ávila, A., & Ovejero, M. (2022). Gender roles and women’s mental health: Their influence on the demand for psychological care. Anales de Psicología, 38(1), 7–16. [Google Scholar] [CrossRef]
- Vadivel, R., Shoib, S., El Halabi, S., El Hayek, S., Essam, L., Gashi Bytyçi, D., Karaliuniene, R., Schuh Teixeira, A. L., Nagendrappa, S., Ramalho, R., Ransing, R., Pereira-Sanchez, V., Jatchavala, C., Adiukwu, F. N., & Kudva Kundadak, G. (2021). Mental health in the post-COVID-19 era: Challenges and the way forward. General Psychiatry, 34(1), e100424. [Google Scholar] [CrossRef]
- van Bavel, J. J., Baicker, K., Boggio, P. S., Capraro, V., Cichocka, A., Cikara, M., Crockett, M. J., Crum, A. J., Douglas, K. M., Druckman, J. N., Drury, J., Dube, O., Ellemers, N., Finkel, E. J., Fowler, J. H., Gelfand, M., Han, S., Haslam, S. A., Jetten, J., … Willer, R. (2020). Using social and behavioural science to support COVID-19 pandemic response. Nature Human Behaviour, 4(5), 460–471. [Google Scholar] [CrossRef] [PubMed]
- Werdin, S., & Wyss, K. (2024). Challenges in the evaluation of suicide prevention measures and quality of suicide data in Germany, Austria, and Switzerland: Findings from qualitative expert interviews. BMC Public Health, 24(1), 2209. [Google Scholar] [CrossRef] [PubMed]
- Wetherall, K., & O’Connor, R. (2023). Suicide prevention targeting middle-aged males: The role of primary care. The British Journal of General Practice: The Journal of the Royal College of General Practitioners, 73(732), 292–294. [Google Scholar] [CrossRef]
- Winkler, P., Formanek, T., Mlada, K., Kagstrom, A., Mohrova, Z., Mohr, P., & Csemy, L. (2020). Prevalence of depressive symptoms during the COVID-19 pandemic in the Czech Republic: A cross-sectional survey. Journal of Affective Disorders, 277, 251–257. [Google Scholar] [CrossRef]
- World Health Organization. (2021). Live life: An implementation guide for suicide prevention in countries. Available online: https://n9.cl/9ygqy (accessed on 14 February 2025).
- World Health Organization. (2023a). Digital health. Available online: https://www.who.int/health-topics/digital-health#tab=tab_1 (accessed on 20 February 2025).
- World Health Organization. (2023b). Fact sheets: Suicide. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 14 February 2025).
- World Health Organization. (2023c). With the international public health emergency ending, WHO/Europe launches its transition plan for COVID-19. Available online: https://n9.cl/sb0t1 (accessed on 20 February 2025).
- Wu, C., & Qian, Y. (2022). The gender peak effect: Women are most vulnerable to infections during COVID-19 peaks. Frontiers Public Health, 10, 937179. [Google Scholar] [CrossRef]
- Yan, Y., Hou, J., Li, Q., & Yu, N. X. (2023). Suicide before and during the COVID-19 pandemic: A systematic review with meta-analysis. International Journal of Environmental Research and Public Health, 20(4), 3346. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Vilas, E.; Coca, J.R.; Labora González, J.J.; Iglesias Carrera, M. The Sociology of Suicide After COVID-19: Assessment of the Spanish Case. Behav. Sci. 2025, 15, 606. https://doi.org/10.3390/bs15050606
Fernández-Vilas E, Coca JR, Labora González JJ, Iglesias Carrera M. The Sociology of Suicide After COVID-19: Assessment of the Spanish Case. Behavioral Sciences. 2025; 15(5):606. https://doi.org/10.3390/bs15050606
Chicago/Turabian StyleFernández-Vilas, Enrique, Juan R. Coca, Juan José Labora González, and Marcos Iglesias Carrera. 2025. "The Sociology of Suicide After COVID-19: Assessment of the Spanish Case" Behavioral Sciences 15, no. 5: 606. https://doi.org/10.3390/bs15050606
APA StyleFernández-Vilas, E., Coca, J. R., Labora González, J. J., & Iglesias Carrera, M. (2025). The Sociology of Suicide After COVID-19: Assessment of the Spanish Case. Behavioral Sciences, 15(5), 606. https://doi.org/10.3390/bs15050606